
Prospective Case Series of Clinical Signs and Adrenocorticotrophin (ACTH) Concentrations in Seven Horses Transitioning to Pituitary Pars Intermedia Dysfunction (PPID)


Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Blood Sample Collection and Analysis
2.3. Data Analysis
3. Results
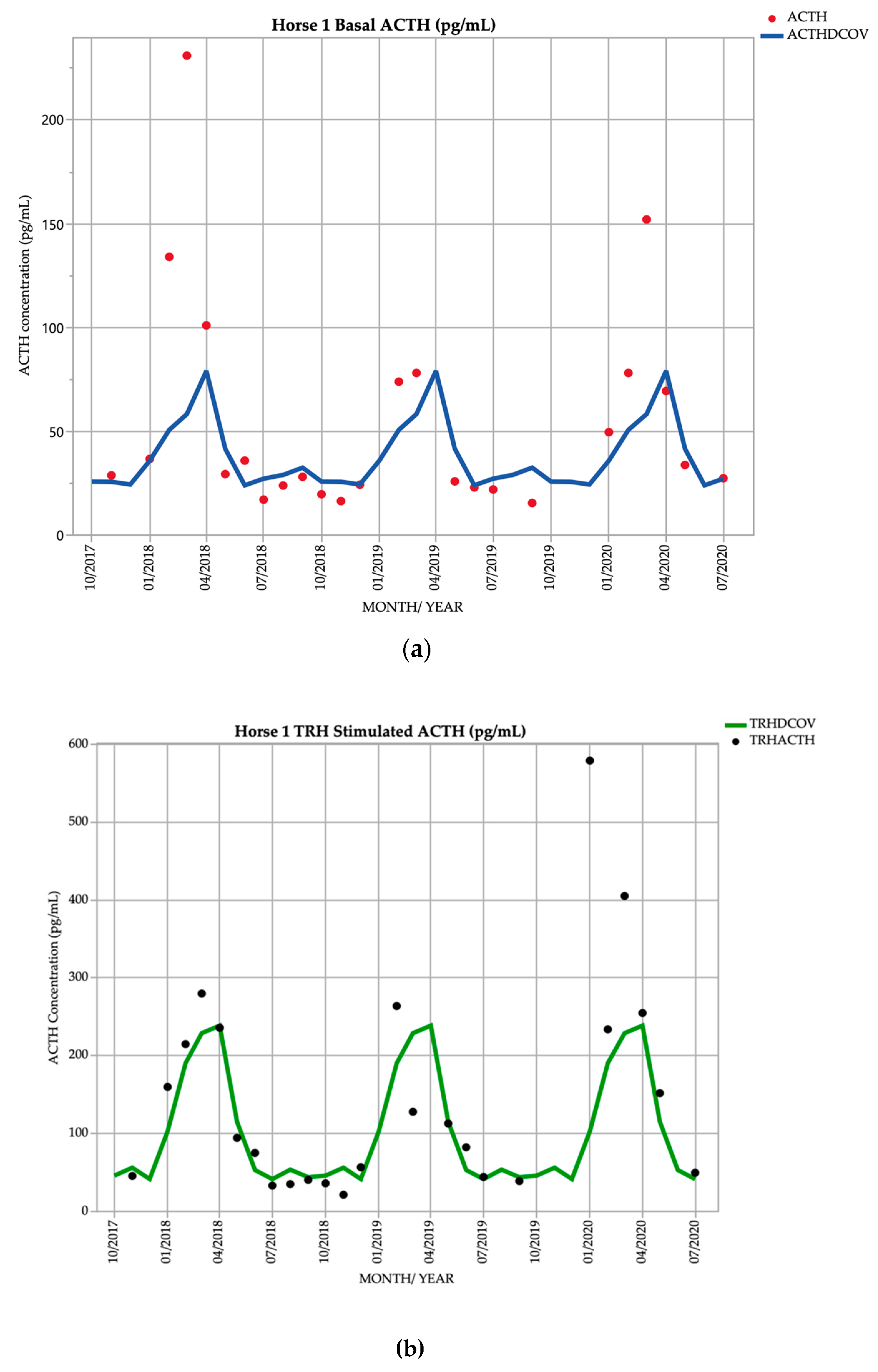
3.1. Horse 1
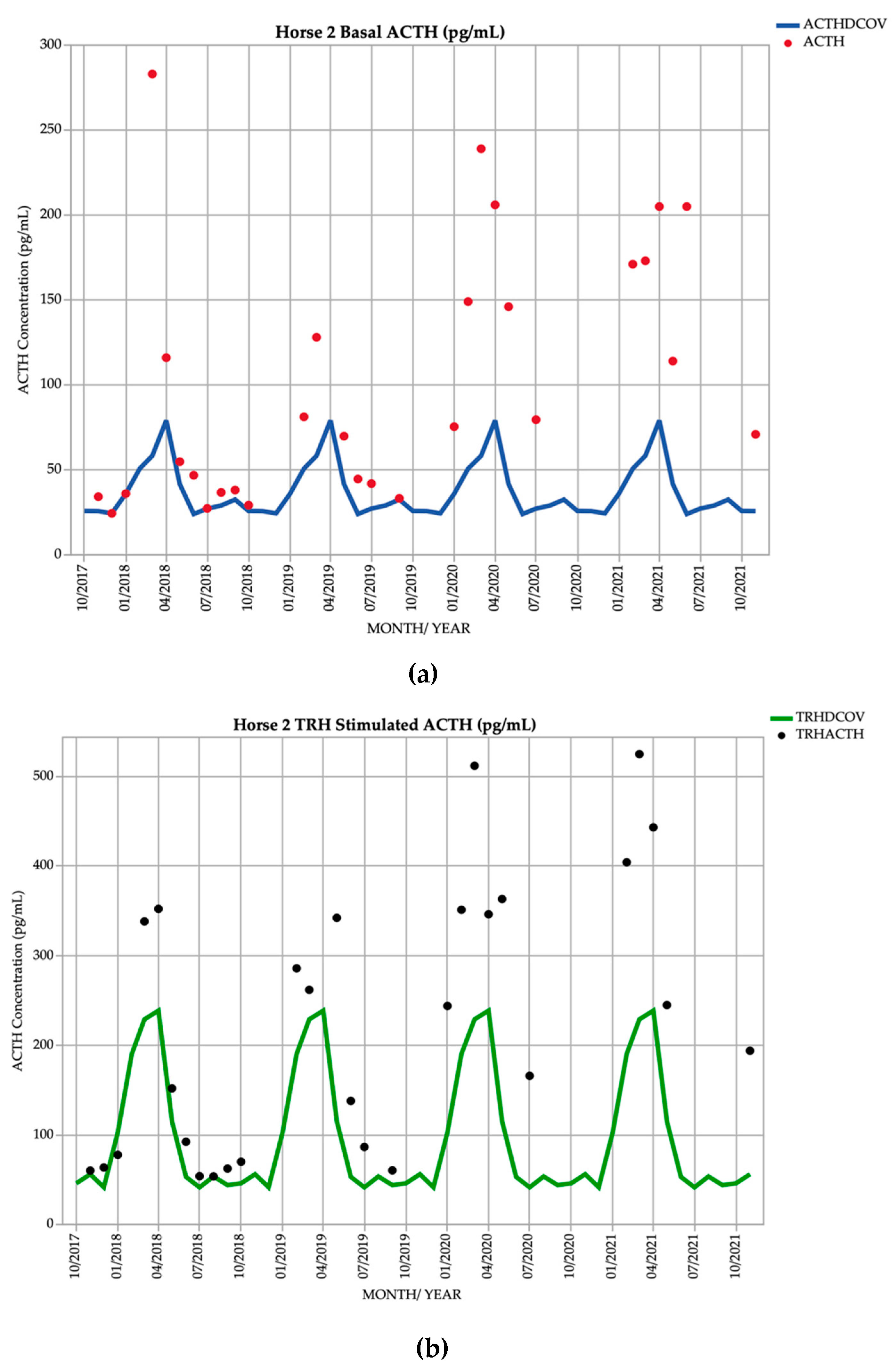
3.2. Horse 2
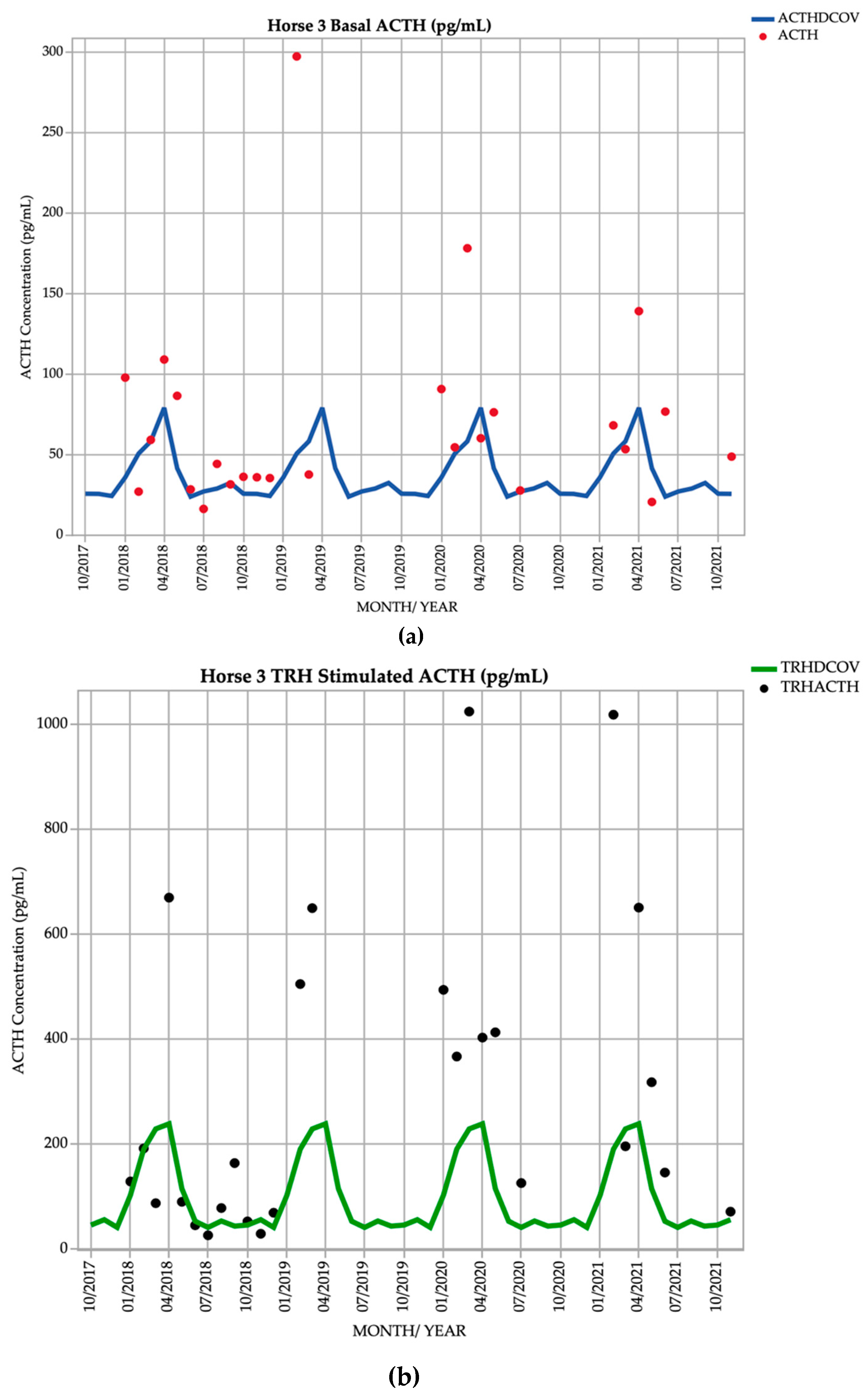
3.3. Horse 3
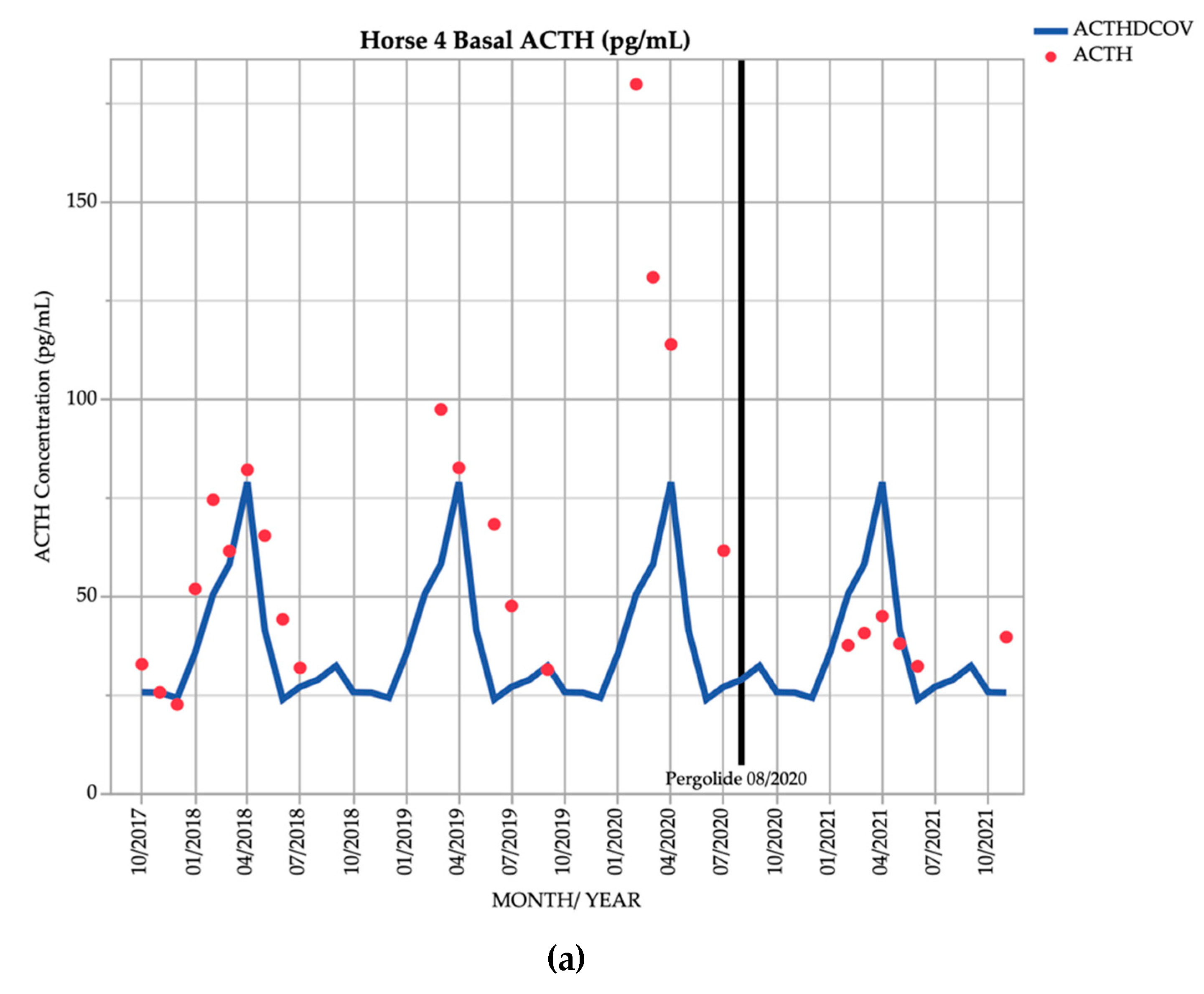
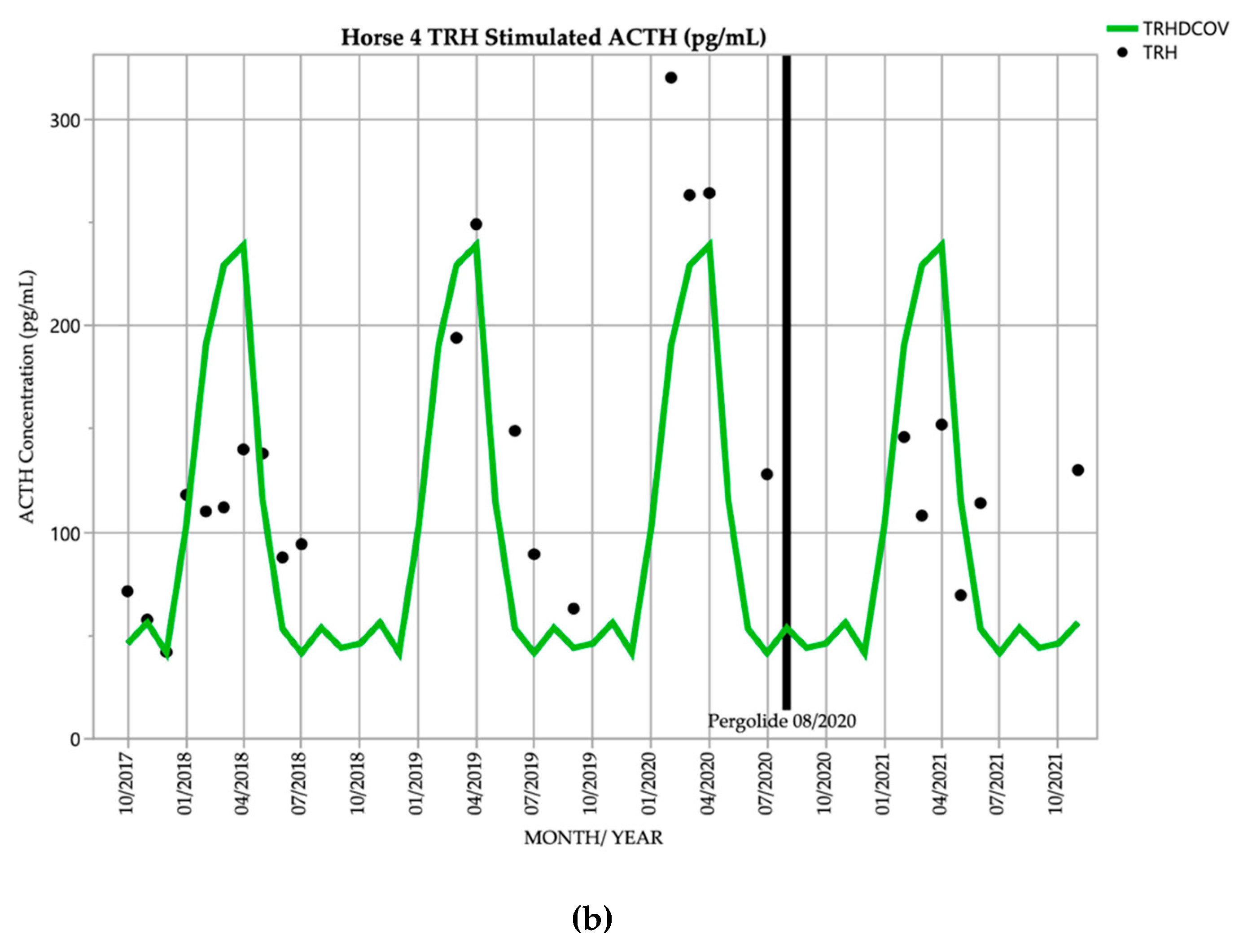
3.4. Horse 4
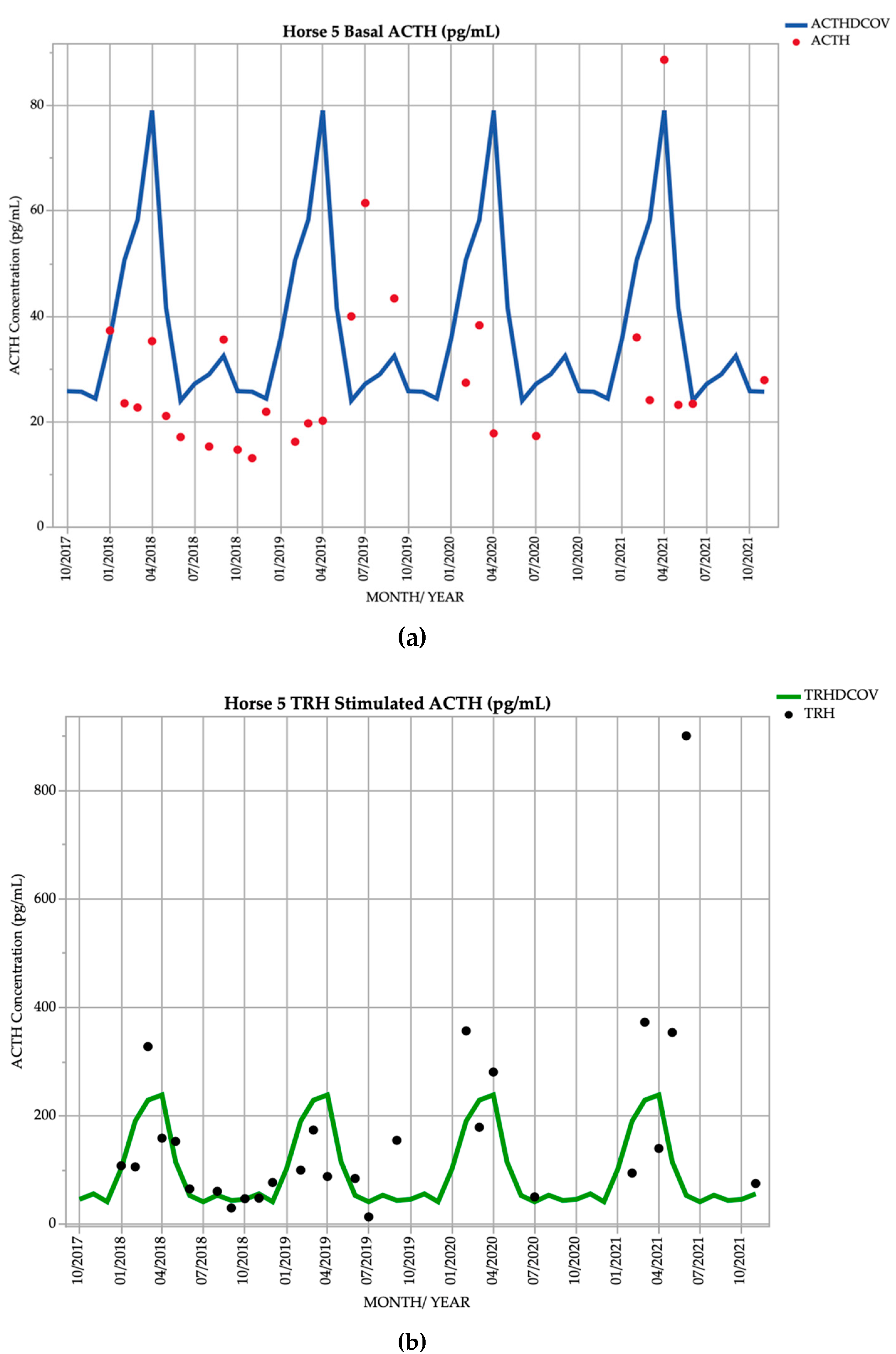
3.5. Horse 5
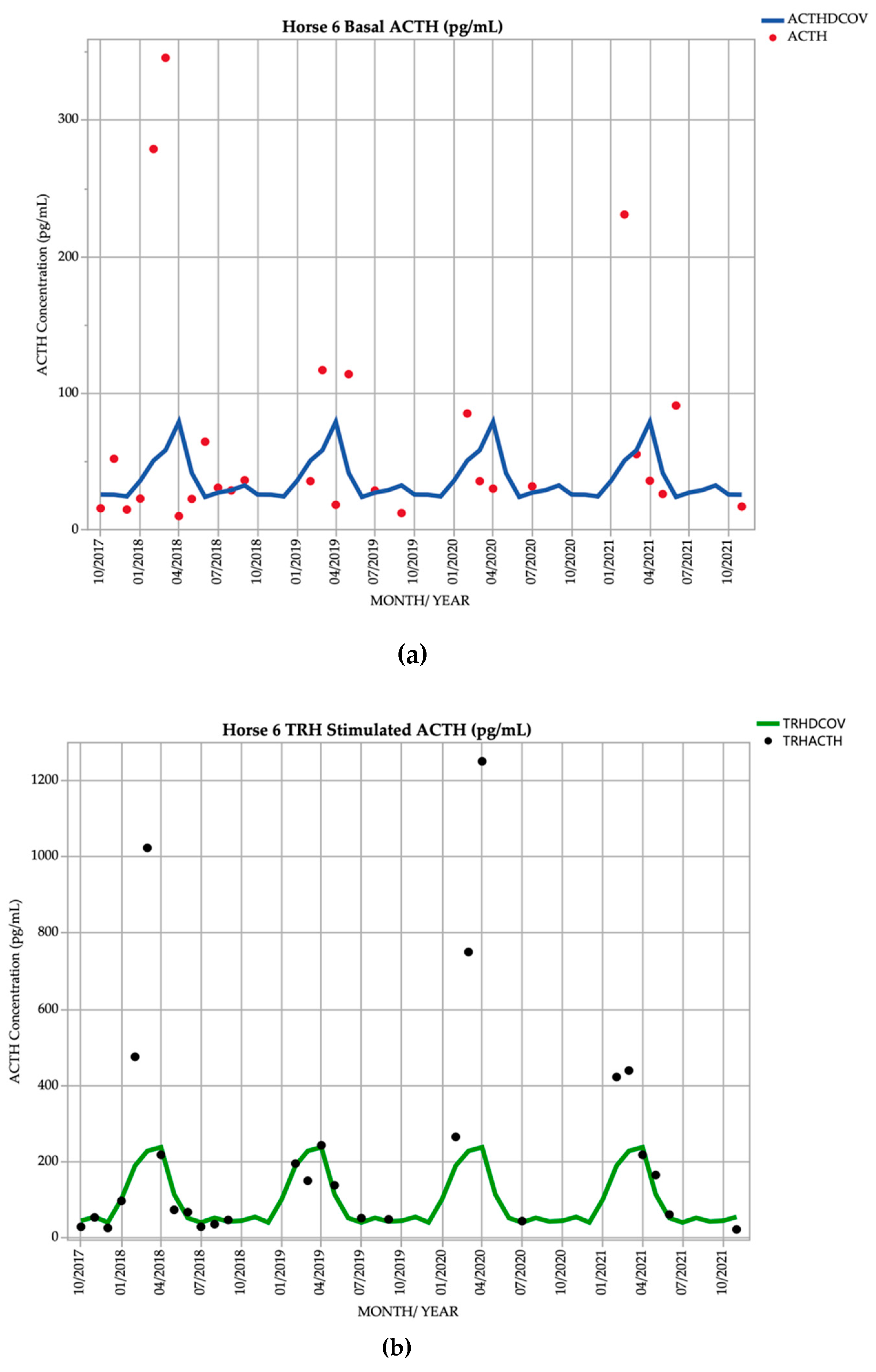
3.6. Horse 6
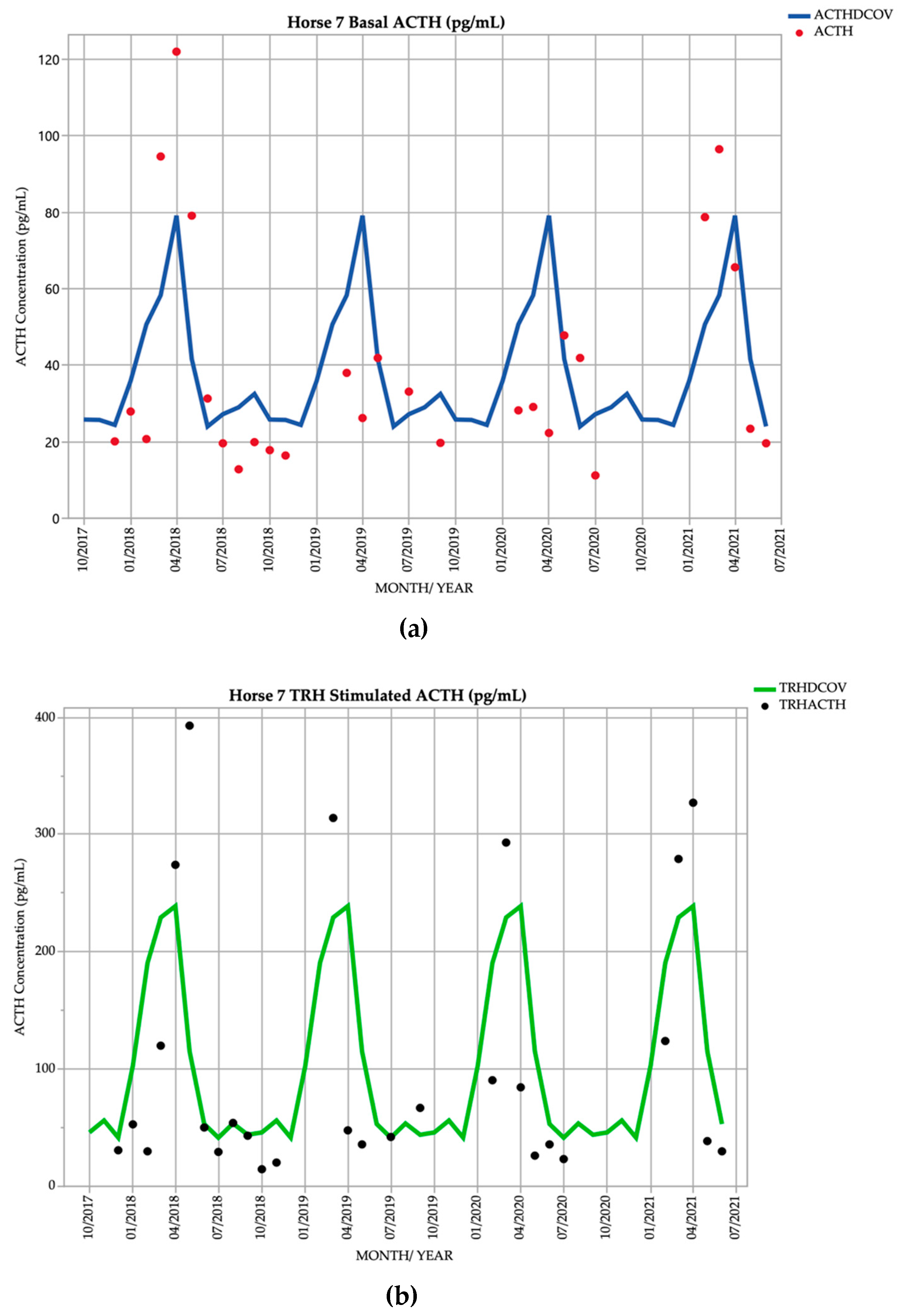
3.7. Horse 7
4. Discussion
5. Study Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Durham, A.; McGowan, C.; Fey, K.; Tamzali, Y.; Van der Kolk, J. Pituitary pars intermedia dysfunction: Diagnosis and treatment. Equine Vet. Educ. 2014, 26, 216–223. [Google Scholar] [CrossRef]
- Horn, R.; Stewart, A.J.; Jackson, K.V.; Dryburgh, E.L.; Medina-Torres, C.E.; Bertin, F.R. Clinical implications of using adrenocorticotropic hormone diagnostic cutoffs or reference intervals to diagnose pituitary pars intermedia dysfunction in mature horses. J. Vet. Intern. Med. 2021, 35, 560–570. [Google Scholar] [CrossRef] [PubMed]
- Ireland, J.; McGowan, C. Epidemiology of pituitary pars intermedia dysfunction: A systematic literature review of clinical presentation, disease prevalence and risk factors. Vet. J. 2018, 235, 22–33. [Google Scholar] [CrossRef] [PubMed]
- McGowan, T.W.; Pinchbeck, G.P.; McGowan, C.M. Prevalence, risk factors and clinical signs predictive for equine pituitary pars intermedia dysfunction in aged horses. Equine Vet. J. 2013, 45, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Kirkwood, N.C.; Hughes, K.J.; Stewart, A.J. Review Article: Pituitary Pars Intermedia Dysfunction (PPID) in Horses. Vet. Sci. 2022, 9, 556. [Google Scholar] [CrossRef]
- Fortin, J.S.; Hetak, A.A.; Duggan, K.E.; Burglass, C.M.; Penticoff, H.B.; Schott, H.C., 2nd. Equine pituitary pars intermedia dysfunction: A spontaneous model of synucleinopathy. Sci. Rep. 2021, 11, 16036. [Google Scholar] [CrossRef]
- McFarlane, D.; Cribb, A.E. Systemic and pituitary pars intermedia antioxidant capacity associated with pars intermedia oxidative stress and dysfunction in horses. Am. J. Vet. Res. 2005, 66, 2065–2072. [Google Scholar] [CrossRef]
- Huang, L.; Palmieri, C.; Bertin, F.-R. Correlation of pituitary histomorphometry with dopamine and dopamine D2 receptor expression in horses with pituitary pars intermedia dysfunction. Res. Vet. Sci. 2022, 152, 427–433. [Google Scholar] [CrossRef]
- Carmalt, J.L.; Mortazavi, S.; McOnie, R.C.; Allen, A.L.; Unniappan, S. Profiles of pro-opiomelanocortin and encoded peptides, and their processing enzymes in equine pituitary pars intermedia dysfunction. PLoS One 2018, 13, e0190796. [Google Scholar] [CrossRef]
- Heinrichs, M.; Baumgärtner, W.; Capen, C. Immunocytochemical demonstration of proopiomelanocortin-derived peptides in pituitary adenomas of the pars intermedia in horses. Vet. Pathol. 1990, 27, 419–425. [Google Scholar] [CrossRef]
- Orth, D.N.; Holscher, M.A.; Wilson, M.G.; Nicholson, W.E.; Plue, R.E.; Mount, C.D. Equine Cushing’s disease: Plasma immunoreactive proopiolipomelanocortin peptide and cortisol levels basally and in response to diagnostic tests. Endocrinology 1982, 110, 1430–1441. [Google Scholar] [CrossRef]
- Wilson, M.G.; Nicholson, W.E.; Holscher, M.A.; Sherrell, B.J.; Mount, C.D.; Orth, D.N. Proopiolipomelanocortin peptides in normal pituitary, pituitary tumor, and plasma of normal and Cushing’s horses. Endocrinology 1982, 110, 941–954. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, H.; Oishi, H.; Sumi, A.; Ueki, H.; Oyamada, T.; Yoshikawa, T. Spontaneous Pituitary Adenomas of the Pars Intermedia in 5 Aged Horses: Histopathological, Immunohistochemical and Ultrastructural Studies. J. Equine Sci. 2001, 12, 119–126. [Google Scholar] [CrossRef]
- Horn, R.; Bamford, N.; Afonso, T.; Sutherland, M.; Buckerfield, J.; Tan, R.; Secombe, C.; Stewart, A.; Bertin, F. Factors associated with survival, laminitis and insulin dysregulation in horses diagnosed with equine pituitary pars intermedia dysfunction. Equine Vet. J. 2019, 51, 440–445. [Google Scholar] [CrossRef] [PubMed]
- Rohrbach, B.; Stafford, J.; Clermont, R.; Reed, S.; Schott, H.; Andrews, F. Diagnostic frequency, response to therapy, and long-term prognosis among horses and ponies with pituitary par intermedia dysfunction, 1993–2004. J. Vet. Intern. Med. 2012, 26, 1027–1034. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.A.; Pardo, I.D.; Jackson, L.P.; Moore, G.E.; Sojka, J.E. Correlation of pituitary histomorphometry with adrenocorticotrophic hormone response to domperidone administration in the diagnosis of equine pituitary pars intermedia dysfunction. Vet. Pathol. 2008, 45, 26–38. [Google Scholar] [CrossRef]
- Beech, J.; Boston, R.; Lindborg, S.; Russell, G.E. Adrenocorticotropin concentration following administration of thyrotropin-releasing hormone in healthy horses and those with pituitary pars intermedia dysfunction and pituitary gland hyperplasia. J. Am. Vet. Med. Assoc. 2007, 231, 417–426. [Google Scholar] [CrossRef]
- Carmalt, J.L.; Waldner, C.L.; Allen, A.L. Equine pituitary pars intermedia dysfunction: An international survey of veterinarians’ approach to diagnosis, management, and estimated prevalence. Can. J. Vet. Res. 2017, 81, 261–269. [Google Scholar]
- Toribio, R.E. Diagnosing equine pars intermedia dysfunction: Are we there yet? J. Vet. Intern. Med. 2005, 19, 145–146. [Google Scholar] [CrossRef]
- Frank, N.; Andrews, F.M.; Sommardahl, C.S.; Eiler, H.; Rohrbach, B.W.; Donnell, R.L. Evaluation of the combined dexamethasone suppression/ thyrotropin-releasing hormone stimulation test for detection of pars intermedia pituitary adenomas in horses. J. Vet. Intern. Med. 2006, 20, 987–993. [Google Scholar] [CrossRef]
- Van der Kolk, J.; Wensing, T.; Kalsbeek, H.; Breukink, H. Laboratory diagnosis of equine pituitary pars intermedia adenoma. Domest. Anim. Endocrinol. 1995, 12, 35–39. [Google Scholar] [CrossRef]
- Hart, K.; Durham, A.; Frank, N.; McGowan, C.; Schott, H.; Stewart, A.J. EEG Recommendations on Diagnosis and Management of Pituitary Pars Intermedia Dysfunction (PPID). Available online: https://sites.tufts.edu/equineendogroup/files/2021/12/2021-PPID-Recommendations-V11-wo-insert.pdf (accessed on 11 November 2021).
- Schreiber, C.M.; Stewart, A.J.; Kwessi, E.; Behrend, E.N.; Wright, J.C.; Kemppainen, R.J.; Busch, K.A. Seasonal variation in results of diagnostic tests for pituitary pars intermedia dysfunction in older, clinically normal geldings. J. Am. Vet. Med. Assoc. 2012, 241, 241–248. [Google Scholar] [CrossRef]
- Mc Gowan, T.W.; Pinchbeck, G.P.; Mc Gowan, C.M. Evaluation of basal plasma α-melanocyte-stimulating hormone and adrenocorticotrophic hormone concentrations for the diagnosis of pituitary pars intermedia dysfunction from a population of aged horses. Equine Vet. J. 2013, 45, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Durham, A.E.; Clarke, B.R.; Potier, J.F.N.; Hammarstrand, R.; Malone, G.L. Clinically and temporally specific diagnostic thresholds for plasma ACTH in the horse. Equine Vet. J. 2021, 53, 250–260. [Google Scholar] [CrossRef]
- Horn, R.; Bertin, F.R. Evaluation of combined testing to simultaneously diagnose pituitary pars intermedia dysfunction and insulin dysregulation in horses. J. Vet. Intern. Med. 2019, 33, 2249–2256. [Google Scholar] [CrossRef] [PubMed]
- Frank, N. Pituitary pars intermedia dysfunction. In Robinson’s Current Therapy in Equine Medicine, 7th ed.; Robinson, N.E., Sprayberry, K.A., Eds.; Elsevier Inc.: Maryland Heights, MO, USA, 2015; pp. 574–577. [Google Scholar]
- Funk, R.; Stewart, A.; Wooldridge, A.; Kwessi, E.; Kemppainen, R.; Behrend, E.; Zhong, Q.; Johnson, A. Seasonal changes in plasma adrenocorticotropic hormone and α-melanocyte-stimulating hormone in response to thyrotropin-releasing hormone in normal, aged horses. J. Vet. Intern. Med. 2011, 25, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Copas, V.E.; Durham, A.E. Circannual variation in plasma adrenocorticotropic hormone concentrations in the UK in normal horses and ponies, and those with pituitary pars intermedia dysfunction. Equine Vet. J. 2012, 44, 440–443. [Google Scholar] [CrossRef] [PubMed]
- Secombe, C.; Bailey, S.; de Laat, M.; Hughes, K.; Stewart, A.; Sonis, J.; Tan, R. Equine pituitary pars intermedia dysfunction: Current understanding and recommendations from the Australian and New Zealand Equine Endocrine Group. Aust. Vet. J. 2018, 96, 233–242. [Google Scholar] [CrossRef]
- Alexander, S.; Irvine, C. The effect of social stress on adrenal axis activity in horses: The importance of monitoring corticosteroid-binding globulin capacity. J. Endocrinol. 1998, 157, 425–432. [Google Scholar] [CrossRef]
- Alexander, S.; Irvine, C.; Livesey, J.; Donald, R. Effect of isolation stress on concentrations of arginine vasopressin, α-melanocyte-stimulating hormone and ACTH in the pituitary venous effluent of the normal horse. J. Endocrinol. 1988, 116, 325–334. [Google Scholar] [CrossRef]
- Alexander, S.; Irvine, C.; Ellis, M.; Donald, R. The effect of acute exercise on the secretion of corticotropin-releasing factor, arginine vasopressin, and adrenocorticotropin as measured in pituitary venous blood from the horse. Endocrinology 1991, 128, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Jacob, S.; Geor, R.; Weber, P.; Harris, P.; McCue, M. Effect of dietary carbohydrates and time of year on ACTH and cortisol concentrations in adult and aged horses. Domest. Anim. Endocrinol. 2018, 63, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Stewart, A.J.; Hackett, E.; Bertin, F.R.; Towns, T.J. Cortisol and adrenocorticotropic hormone concentrations in horses with systemic inflammatory response syndrome. J. Vet. Intern. Med. 2019, 33, 2257–2266. [Google Scholar] [CrossRef] [PubMed]
- Friedrichs, K.R.; Harr, K.E.; Freeman, K.P.; Szladovits, B.; Walton, R.M.; Barnhart, K.F.; Blanco-Chavez, J. ASVCP reference interval guidelines: Determination of de novo reference intervals in veterinary species and other related topics. Vet. Clin. Pathol. 2012, 41, 441–453. [Google Scholar] [CrossRef] [PubMed]
- Diez de Castro, E.; Lopez, I.; Cortes, B.; Pineda, C.; Garfia, B.; Aguilera-Tejero, E. Influence of feeding status, time of the day, and season on baseline adrenocorticotropic hormone and the response to thyrotropin releasing hormone-stimulation test in healthy horses. Domest. Anim. Endocrinol. 2014, 48, 77–83. [Google Scholar] [CrossRef]
- Hu, K.; Stewart, A.J.; Yuen, K.Y.; Hinrichsen, S.; Dryburgh, E.L.; Bertin, F.R. The effect of freeze-thaw cycles on determination of immunoreactive plasma adrenocorticotrophic hormone concentrations in horses. J. Vet. Intern. Med. 2020, 34, 1350–1356. [Google Scholar] [CrossRef]
- Kam, Y.N.; McKenzie, K.; Coyle, M.; Bertin, F.R. Repeatability of a thyrotropin-releasing hormone stimulation test for diagnosis of pituitary pars intermedia dysfunction in mature horses. J. Vet. Intern. Med. 2021, 35, 2885–2890. [Google Scholar] [CrossRef]
- Hinrichsen, S.L.; Yuen, K.Y.; Dryburgh, E.L.; Bertin, F.R.; Stewart, A.J. Short-Term Effects of Temperature and Thyrotropin-Releasing Hormone Stimulation on Adrenocorticotropin Stability in Horses. Animals 2022, 12, 324. [Google Scholar] [CrossRef]
- Byrne, D.P.; Secombe, C.J.; Tan, R.H.H.; Perera, D.I.; Watts, S.P.; Wearn, J.G. Circannual variability in adrenocorticotropic hormone responses to administration of thyrotropin-releasing hormone in clinically normal horses in Australia. Vet. J. 2018, 238, 58–62. [Google Scholar] [CrossRef]
- Frank, N.; Elliott, S.; Chameroy, K.; Toth, F.; Chumbler, N.; McClamroch, R. Association of season and pasture grazing with blood hormone and metabolite concentrations in horses with presumed pituitary pars intermedia dysfunction. J. Vet. Intern. Med. 2010, 24, 1167–1175. [Google Scholar] [CrossRef]
- Irvine, K.L.; Burt, K.; Hill, A.J.; Shaw, S.; Papasouliotis, K. Initial analytic quality assessment and method comparison of an immunoassay for adrenocorticotropic hormone measurement in equine samples. Vet. Clin. Pathol. 2016, 45, 154–163. [Google Scholar] [CrossRef] [PubMed]
- McFarlane, D. Equine Pituitary Pars Intermedia Dysfunction. Vet. Clin. North. Am. Equine Pract. 2011, 27, 93–113. [Google Scholar] [CrossRef] [PubMed]
- Couëtil, L.; Paradis, M.R.; Knoll, J. Plasma adrenocorticotropin concentration in healthy horses and in horses with clinical signs of hyperadrenocorticism. J. Vet. Intern. Med. 1996, 10, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Innerå, M.; Petersen, A.D.; Desjardins, D.R.; Steficek, B.A.; Rosser Jr, E.J.; Schott, H.C. Comparison of hair follicle histology between horses with pituitary pars intermedia dysfunction and excessive hair growth and normal aged horses. Vet. Dermatol. 2013, 24, 212-e247. [Google Scholar] [CrossRef]
- Brosnahan, M.M.; Paradis, M.R. Demographic and clinical characteristics of geriatric horses: 467 cases (1989–1999). J. Am. Vet. Med. Assoc. 2003, 223, 93–98. [Google Scholar] [CrossRef]
- Mellor, D.; Reid, S.; Love, S.; Walker, R.; Gettinby, G. Sentinel practice-based survey of the management and health of horses in northern Britain. Vet. Rec. 2001, 149, 417–423. [Google Scholar] [CrossRef] [PubMed]
- McFarlane, D.; Hill, K.; Anton, J. Neutrophil function in healthy aged horses and horses with pituitary dysfunction. Vet. Immunol. Immunopathol. 2015, 165, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Hart, K.A.; Kitchings, K.M.; Kimura, S.; Norton, N.A.; Myrna, K.E. Measurement of cortisol concentration in the tears of horses and ponies with pituitary pars intermedia dysfunction. Am. J. Vet. Res. 2016, 77, 1236–1244. [Google Scholar] [CrossRef]
- Spelta, C.; Axon, J. Case series of equine pituitary pars intermedia dysfunction in a tropical climate. Aust. Vet. J. 2012, 90, 451–456. [Google Scholar] [CrossRef]
- Schott, H.C. Pituitary pars intermedia dysfunction: Equine Cushing’s disease. Vet. Clin. North. Am. Equine Pract. 2002, 18, 237–270. [Google Scholar] [CrossRef]
- McFarlane, D. Pathophysiology and clinical features of pituitary pars intermedia dysfunction. Equine Vet. Educ. 2014, 26, 592–598. [Google Scholar] [CrossRef]
- Miller, A.B.; Loynachan, A.T.; Barker, V.D.; Adams, A.A. Investigation of innate immune function in adult and geriatric horses. Vet. Immunol. Immunopathol. 2021, 235, 110207. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.B.; Loynachan, A.T.; Bush, H.M.; Hart, K.A.; Barker, V.D.; Campana-Emard, A.G.; Grubbs, S.T.; Adams, A.A. Effects of pituitary pars intermedia dysfunction and Prascend (pergolide tablets) treatment on endocrine and immune function in horses. Domest. Anim. Endocrinol. 2021, 74, 106531. [Google Scholar] [CrossRef]
- Miller, C.; Utter, M.L.; Beech, J. Evaluation of the effects of age and pituitary pars intermedia dysfunction on corneal sensitivity in horses. Am. J. Vet. Res. 2013, 74, 1030–1035. [Google Scholar] [CrossRef]
- Miller, M.; Moore, G.; Bertin, F.; Kritchevsky, J. What’s new in old horses? Postmortem diagnoses in mature and aged equids. Vet. Pathol. 2016, 53, 390–398. [Google Scholar] [CrossRef]
- Beech, J.; Boston, R.; Lindborg, S. Comparison of cortisol and ACTH responses after administration of thyrotropin releasing hormone in normal horses and those with pituitary pars intermedia dysfunction. J. Vet. Intern. Med. 2011, 25, 1431–1438. [Google Scholar] [CrossRef]
- Thane, K.; Uricchio, C.; Frank, N. Effect of early or late blood sampling on thyrotropin releasing hormone stimulation test results in horses. J. Vet. Intern. Med. 2022, 36, 770–777. [Google Scholar] [CrossRef] [PubMed]
- McGowan, C. Hyperadrenocorticism (Pituitary Pars Intermedia Dysfunction) in Horses, 1st ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2013; pp. 100–114. [Google Scholar]
- Tatum, R.C.; McGowan, C.M.; Ireland, J.L. Efficacy of pergolide for the management of equine pituitary pars intermedia dysfunction: A systematic review. Vet. J. 2020, 266, 105562. [Google Scholar] [CrossRef]
- Donaldson, M.T.; LaMonte, B.H.; Morresey, P.; Smith, G.; Beech, J. Treatment with pergolide or cyproheptadine of pituitary pars intermedia dysfunction (equine Cushing’s disease). J. Vet. Intern. Med. 2002, 16, 742–746. [Google Scholar] [CrossRef]
- Perkins, G.; Lamb, S.; Erb, H.; Schanbacher, B.; Nydam, D.; Divers, T. Plasma adrenocorticotropin (ACTH) concentrations and clinical response in horses treated for equine Cushing’s disease with cyproheptadine or pergolide. Equine Vet. J. 2002, 34, 679–685. [Google Scholar] [CrossRef]
- Banse, H.E.; Whitehead, A.E.; McFarlane, D.; Chelikani, P.K. Markers of muscle atrophy and impact of treatment with pergolide in horses with pituitary pars intermedia dysfunction and muscle atrophy. Domest. Anim. Endocrinol. 2021, 76, 106620. [Google Scholar] [CrossRef] [PubMed]
- Beech, J.; McFarlane, D.; Lindborg, S.; Sojka, J.E.; Boston, R.C. α-Melanocyte—stimulating hormone and adrenocorticotropin concentrations in response to thyrotropin-releasing hormone and comparison with adrenocorticotropin concentration after domperidone administration in healthy horses and horses with pituitary pars intermedia dysfunction. J. Am. Vet. Med. Assoc. 2011, 238, 1305–1315. [Google Scholar] [CrossRef] [PubMed]
- McFarlane, D.; Beech, J.; Cribb, A. Alpha-melanocyte stimulating hormone release in response to thyrotropin releasing hormone in healthy horses, horses with pituitary pars intermedia dysfunction and equine pars intermedia explants. Domest. Anim. Endocrinol. 2006, 30, 276–288. [Google Scholar] [CrossRef] [PubMed]
- McFarlane, D.; Miller, L.M.; Craig, L.E.; Dybdal, N.O.; Habecker, P.L.; Miller, M.A.; Patterson, J.S.; Cribb, A.E. Agreement in histologic assessments of the pituitary pars intermedia in aged horses. Am. J. Vet. Res. 2005, 66, 2055–2059. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hypertrichosis Scoring System (0–5) | ||
|---|---|---|
| Score | Photographic Representation | Description |
| 0/5 |  | No hypertrichosis present |
| 1/5 |  | Mild hypertrichosis present, usually persistent along the ventral abdomen, palmar or plantar aspect of distal limbs, mandible and over the semimembranosus and semitendinosus muscles. Often accompanied by delayed shedding. |
| 2/5 |  | Generalized mild hypertrichosis over the entire body, accompanied by delayed shedding. |
| 3/5 |  | Moderate generalized hypertrichosis present over the entire body and most severe along the ventral abdomen and semimembranosus and semitendinosus muscles. Always accompanied by delayed shedding. |
| 4/5 |  | Severe generalized hypertrichosis, always accompanied by delayed shedding. |
| 5/5 |  | Extreme generalized hypertrichosis. Always accompanied by delayed shedding and often accompanied by difficulty thermoregulating in warmer months. |
| Horse | Month/Year | Hypertrichosis Score | Basal ACTH (Likely Positive or Negative for PPID) * | TRH-Stimulated ACTH (Likely Positive or Negative for PPID) * |
|---|---|---|---|---|
| Horse 1 | February 2019 | 0/5 | Positive | Positive |
| September 2019 | 1/5 | Negative | Negative | |
| January 2020 | 0/5 | Positive | Positive | |
| March 2020 | 0/5 | Positive | Positive | |
| Horse 2 | February 2019 | 0/5 | Positive | Positive |
| September 2019 | 5/5 | Positive | Positive | |
| January 2020 | 1/5 | Positive | Positive | |
| March 2020 | 2/5 | Positive | Positive | |
| September 2020 | 5/5 | − | − | |
| February 2021 | 2/5 | Positive | Positive | |
| March 2021 | 3/5 | Positive | Positive | |
| April 2021 | 3/5 | Positive | Positive | |
| May 2021 | 3/5 | Positive | Positive | |
| June 2021 | 4/5 | Positive | − | |
| November 2021 | 2/5 | Positive | Positive | |
| Horse 3 | February 2019 | 0/5 | Positive | Positive |
| March 2019 | 1/5 | Negative | Positive | |
| January 2020 | 0/5 | Positive | Positive | |
| September 2020 | 1/5 | − | − | |
| March 2021 | 0/5 | Negative | Negative | |
| April 2021 | 0/5 | Positive | Positive | |
| May 2021 | 0/5 | Negative | Positive | |
| June 2021 | 0/5 | Positive | Positive | |
| October 2021 | 1/5 | Positive | Positive | |
| Horse 4 | February 2019 | 0/5 | − | − |
| September 2019 | 2/5 | Negative | Positive | |
| January 2020 | 0/5 | - | - | |
| March 2020 | 0/5 | Positive | Positive | |
| September 2020 1 | 5/51 | − | − | |
| February 2021 1 | 0/5 1 | Negative 1 | Negative 1 | |
| March 2021 1 | 1/5 1 | Negative 1 | Negative 1 | |
| April 2021 1 | 1/5 1 | Negative 1 | Negative 1 | |
| June 2021 1 | 2/5 | Negative 1 | Positive 1 | |
| September 2021 1 | 3/5 | − | − | |
| November 2021 1 | 2/5 | Positive 1 | Positive 1 | |
| Horse 5 | February 2019 | 0/5 | Negative | Negative |
| March 2019 | 0/5 | Negative | Negative | |
| September 2019 | 0/5 | Positive | Positive | |
| January 2020 | 0/5 | − | − | |
| March 2020 | 0/5 | Negative | Negative | |
| September 2020 | 0/5 | − | − | |
| February 2021 | 0/5 | Negative | Negative | |
| March 2021 | 0/5 | Negative | Positive | |
| April 2021 | 0/5 | Positive | Negative | |
| May 2021 | 0/5 | Negative | Positive | |
| June 2021 | 0/5 | Negative | Positive | |
| November 2021 | 0/5 | Positive | Positive | |
| Horse 6 | February 2019 | 0/5 | Negative | Positive |
| September 2019 | 0/5 | Negative | Positive | |
| March 2020 | 0/5 | Negative | Positive | |
| February 2021 | 0/5 | Positive | Positive | |
| March 2021 | 0/5 | Negative | Positive | |
| April 2021 | 0/5 | Negative | Negative | |
| May 2021 | 0/5 | Negative | Positive | |
| September 2021 | 1/5 | − | − | |
| November 2021 | 0/5 | Negative | Negative | |
| Horse 7 | March 2019 | 0/5 | Negative | Positive |
| September 2019 | 1/5 | Negative | Positive | |
| March 2020 | 0/5 | Negative | Positive | |
| February 2021 | 0/5 | Positive | Negative | |
| March 2021 | 0/5 | Positive | Positive | |
| April 2021 | 0/5 | Negative | Positive | |
| May 2021 | 0/5 | Negative | Negative | |
| June 2021 | 0/5 | Negative | Negative | |
| July 2021 2 | − 2 | − 2 | − 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kirkwood, N.C.; Hughes, K.J.; Stewart, A.J. Prospective Case Series of Clinical Signs and Adrenocorticotrophin (ACTH) Concentrations in Seven Horses Transitioning to Pituitary Pars Intermedia Dysfunction (PPID). Vet. Sci. 2022, 9, 572. https://doi.org/10.3390/vetsci9100572
Kirkwood NC, Hughes KJ, Stewart AJ. Prospective Case Series of Clinical Signs and Adrenocorticotrophin (ACTH) Concentrations in Seven Horses Transitioning to Pituitary Pars Intermedia Dysfunction (PPID). Veterinary Sciences. 2022; 9(10):572. https://doi.org/10.3390/vetsci9100572
Chicago/Turabian StyleKirkwood, Naomi C., Kristopher J. Hughes, and Allison J. Stewart. 2022. "Prospective Case Series of Clinical Signs and Adrenocorticotrophin (ACTH) Concentrations in Seven Horses Transitioning to Pituitary Pars Intermedia Dysfunction (PPID)" Veterinary Sciences 9, no. 10: 572. https://doi.org/10.3390/vetsci9100572
APA StyleKirkwood, N. C., Hughes, K. J., & Stewart, A. J. (2022). Prospective Case Series of Clinical Signs and Adrenocorticotrophin (ACTH) Concentrations in Seven Horses Transitioning to Pituitary Pars Intermedia Dysfunction (PPID). Veterinary Sciences, 9(10), 572. https://doi.org/10.3390/vetsci9100572