Prognostic Factors and Life Expectancy in Canine Leishmaniosis

 ,
,  , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Case Selection
2.3. Medical Records Evaluation
2.3.1. Dog Signalment
2.3.2. Establishment of CanL Diagnosis
2.3.3. Confirmation of Other Infectious Diseases
2.3.4. Anti-Leishmania Treatment
2.3.5. Veterinary Follow-Ups
2.4. Statistical Analysis
3. Results
3.1. Anemia and Hyperproteinemia Are Frequent Clinicopathological Findings in CanL
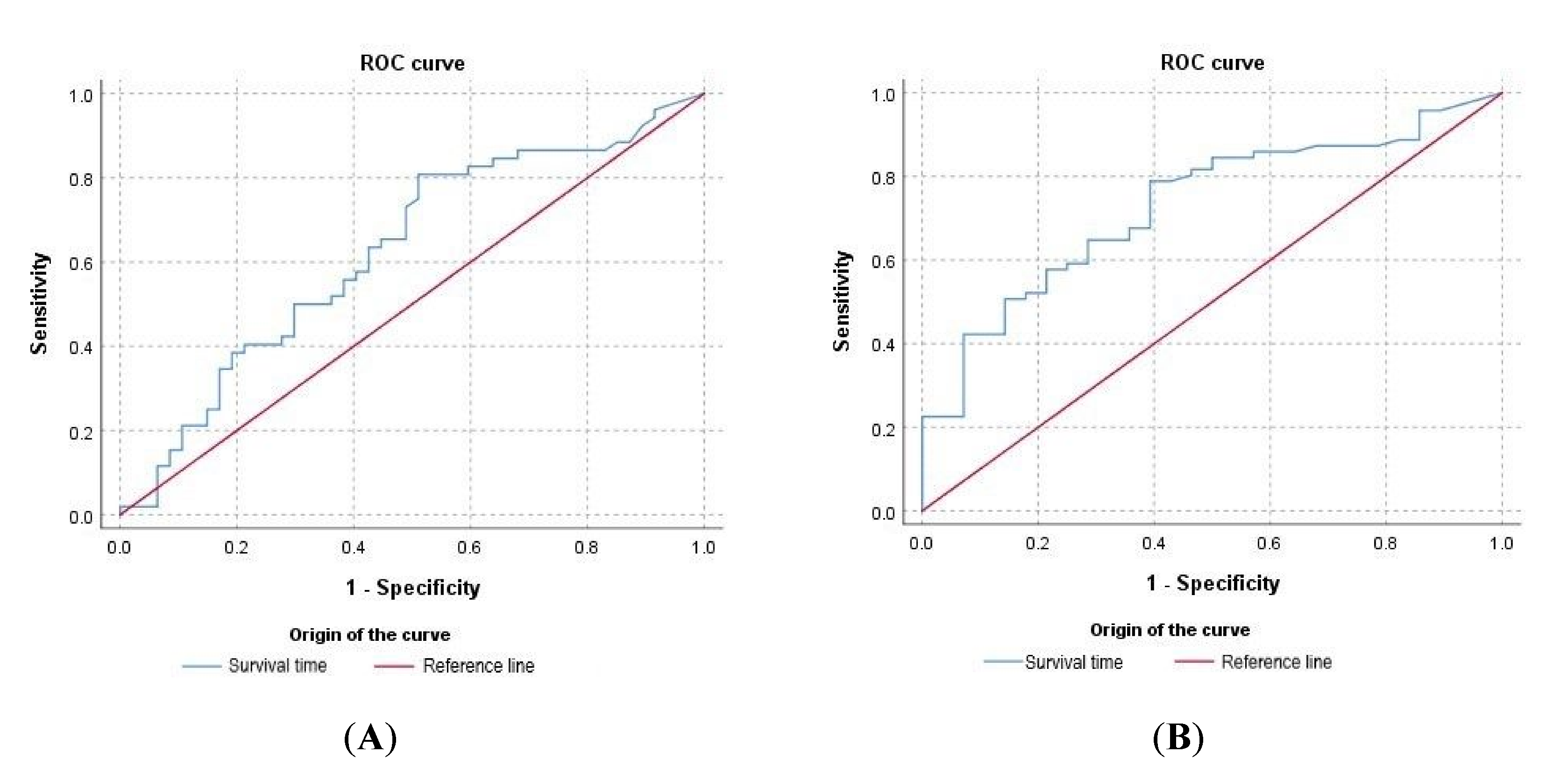
3.2. Clinicopathological Abnormalities Observed at the Time of Diagnosis Can Be Useful to Predict Prognosis
3.3. The Presence of Coinfections at the Time of Diagnosis Compromised Dog Survival
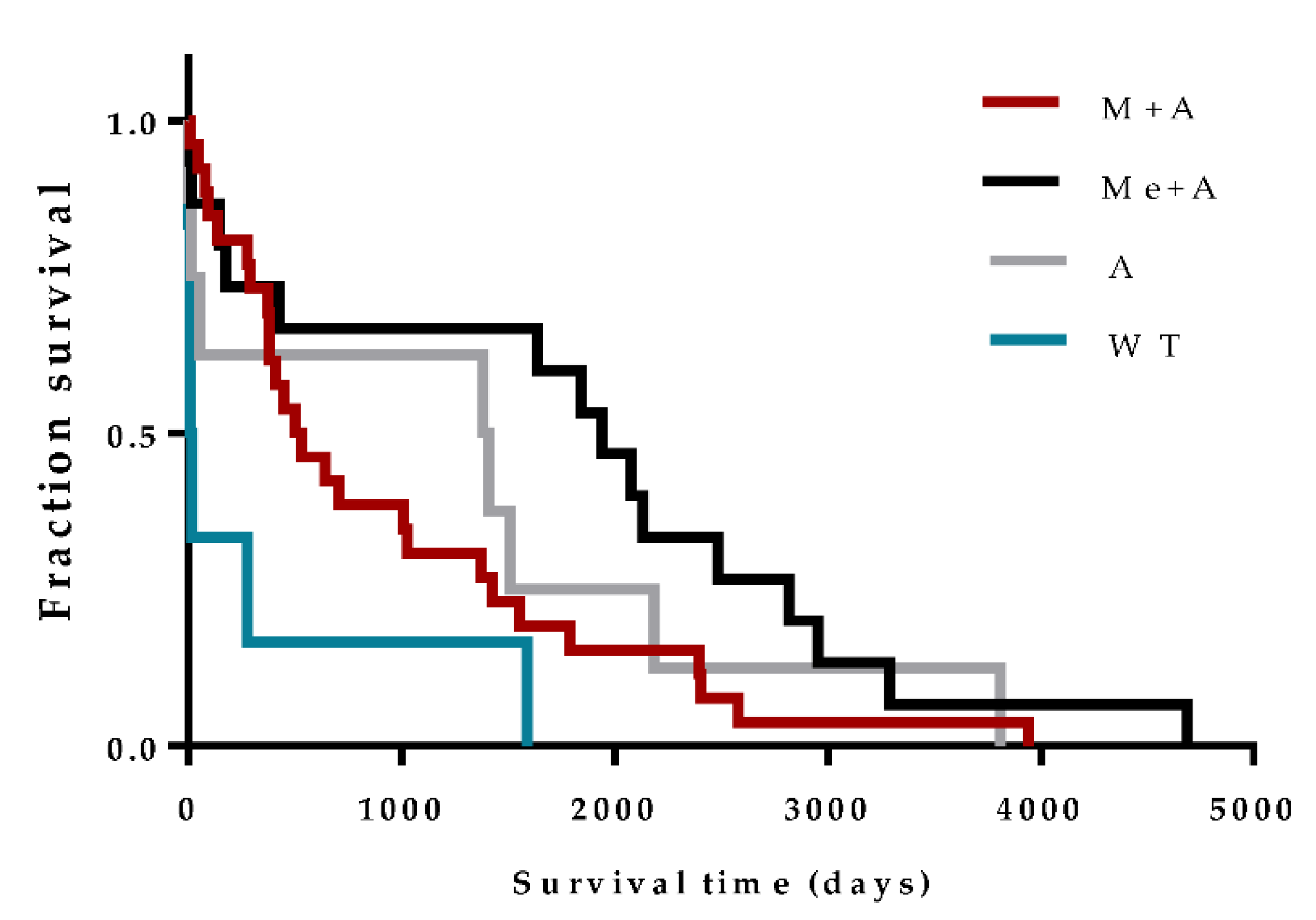
3.4. Anti-Leishmania Therapy Can Influence Prognosis
3.5. The Improvement in Renal Function Is a Rare Event during the Course of CanL Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Alvar, J.; Cañavate, C. Canine leishmaniasis. Adv. Parasitol. 2004, 57, 1–88. [Google Scholar] [CrossRef] [PubMed]
- Baneth, G.; Koutinas, A.F. Canine leishmaniosis—New concepts and insights on an expanding zoonosis: Part one. Trends Parasitol. 2008, 24, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Solano-Gallego, L.; Koutinas, A. Directions for the diagnosis, clinical staging, treatment and prevention of canine leishmaniosis. Vet. Parasitol. 2009, 165, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Moreno, J.; Alvar, J. Canine leishmaniasis: Epidemiological risk and the experimental model. Trends Parasitol. 2002, 18, 399–405. [Google Scholar] [CrossRef]
- Amusategui, I.; Sainz, A. Seroprevalence of Leishmania infantum in northwestern Spain, an area traditionally considered free of leishmaniasis. Ann. N. Y. Acad. Sci. 2004, 1026, 154–157. [Google Scholar] [CrossRef]
- Morosetti, G.; Bongiorno, G. Risk assessment for canine leishmaniasis spreading in the north of Italy. Geospat. Health 2009, 4, 115–127. [Google Scholar] [CrossRef]
- Chamaillé, L.; Tran, A. Environmental risk mapping of canine leishmaniasis in France. Parasites Vectors 2010, 3, 31. [Google Scholar] [CrossRef]
- Baldelli, R.; Piva, S. Canine leishmaniasis surveillance in a northern Italy kennel. Vet. Parasitol. 2011, 179, 57–61. [Google Scholar] [CrossRef]
- Menn, B.; Lorentz, S. Imported and travelling dogs as carriers of canine vector-borne pathogens in Germany. Parasites Vectors 2010, 3, 34. [Google Scholar] [CrossRef]
- Teske, E.; van Knapen, F. Risk of infection with Leishmania spp. in the canine population in the Netherlands. Acta Vet. Scand. 2002, 43, 195–201. [Google Scholar] [CrossRef]
- Kaszak, I.; Planellas, M. Canine leishmaniosis—An emerging disease. Ann. Parasitol. 2015, 61, 69–76. [Google Scholar] [PubMed]
- Schäfer, I.; Volkmann, M. Retrospective evaluation of vector-borne infections in dogs imported from the Mediterranean region and southeastern Europe (2007–2015). Parasites Vectors 2019, 12, 30. [Google Scholar] [CrossRef] [PubMed]
- Paltrinieri, S.; Solano-Gallego, L. Guidelines for diagnosis and clinical classification of leishmaniasis in dogs. J. Am. Vet. Med. Assoc. 2010, 236, 1184–1191. [Google Scholar] [CrossRef]
- Ciaramella, P.; Oliva, G. A retrospective clinical study of canine leishmaniasis in 150 dogs naturally infected by Leishmania infantum. Vet. Rec. 1997, 141, 539–543. [Google Scholar] [CrossRef] [PubMed]
- Saridomichelakis, M.N. Advances in the pathogenesis of canine leishmaniosis: Epidemiologic and diagnostic implications. Vet. Dermatol. 2009, 20, 471–489. [Google Scholar] [CrossRef]
- Koutinas, A.F.; Koutinas, C.K. Pathologic mechanisms underlying the clinical findings in canine leishmaniasis due to Leishmania infantum/chagasi. Vet. Pathol. 2014, 51, 527–538. [Google Scholar] [CrossRef] [PubMed]
- Momo, C.; Jacintho, A.P. Morphological changes in the bone marrow of the dogs with visceral leishmaniasis. Vet. Med. Int. 2014, 2014, 150582. [Google Scholar] [CrossRef]
- Costa, F.A.; Goto, H. Histopathologic patterns of nephropathy in naturally acquired canine visceral leishmaniasis. Vet. Pathol. 2003, 40, 677–684. [Google Scholar] [CrossRef]
- Poli, A.; Abramo, F. Renal involvement in canine leishmaniasis. A light-microscopic, immunohistochemical and electron-microscopic study. Nephron 1991, 57, 444–452. [Google Scholar] [CrossRef]
- Plevraki, K.; Koutinas, A.F. Effects of allopurinol treatment on the progression of chronic nephritis in Canine leishmaniosis (Leishmania infantum). J. Vet. Intern. Med. 2006, 20, 228–233. [Google Scholar] [CrossRef]
- Gill, T.M. The central role of prognosis in clinical decision making. JAMA 2012, 307, 199–200. [Google Scholar] [CrossRef] [PubMed]
- Geisweid, K.; Mueller, R. Prognostic analytes in dogs with Leishmania infantum infection living in a non-endemic area. Vet. Rec. 2012, 171, 399. [Google Scholar] [CrossRef] [PubMed]
- Roura, X.; Fondati, A. Prognosis and monitoring of leishmaniasis in dogs: A working group report. Vet. J. 2013, 198, 43–47. [Google Scholar] [CrossRef] [PubMed]
- IRIS Staging of CKD (Modified 2019). International Renal Interest Society, 2019. Available online: http://iris-kidney.com/ (accessed on 16 August 2020).
- Pierantozzi, M.; Roura, X. Variation of proteinuria in dogs with leishmaniasis treated with meglumine antimoniate and allopurinol: A retrospective study. J. Am. Anim. Hosp. Assoc. 2013, 49, 231–236. [Google Scholar] [CrossRef]
- Proverbio, D.; Spada, E. Proteinuria reduction after treatment with miltefosine and allopurinol in dogs naturally infected with leishmaniasis. Vet. World 2016, 9, 904–908. [Google Scholar] [CrossRef]
- Cringoli, G.; Rinaldi, L. Serological survey of Neospora caninum and Leishmania infantum co-infection in dogs. Vet. Parasitol. 2002, 106, 307–313. [Google Scholar] [CrossRef]
- Attipa, C.; Solano-Gallego, L. Association between canine leishmaniosis and Ehrlichia canis co-infection: A prospective case-control study. Parasites Vectors 2018, 11, 184. [Google Scholar] [CrossRef]
- Baxarias, M.; Álvarez-Fernández, A. Does co-infection with vector-borne pathogens play a role in clinical canine leishmaniosis? Parasites Vectors 2018, 11, 135. [Google Scholar] [CrossRef]
- Otranto, D.; Dantas-Torres, F. Managing canine vector-borne diseases of zoonotic concern: Part one. Trends Parasitol. 2009, 25, 157–163. [Google Scholar] [CrossRef]
- Tabar, M.D.; Francino, O. PCR survey of vectorborne pathogens in dogs living in and around Barcelona, an area endemic for leishmaniasis. Vet. Rec. 2009, 164, 112–116. [Google Scholar] [CrossRef]
- De Tommasi, A.S.; Otranto, D. Are vector-borne pathogen co-infections complicating the clinical presentation in dogs? Parasites Vectors 2013, 6, 97. [Google Scholar] [CrossRef] [PubMed]
- Mekuzas, Y.; Gradoni, L. Ehrlichia canis and Leishmania infantum co-infection: A 3-year longitudinal study in naturally exposed dogs. Clin. Microbiol. Infect. 2009, 15 (Suppl. 2), 30–31. [Google Scholar] [CrossRef]
- Ikeda-Garcia, F.A.; Lopes, R.S. Clinical and parasitological evaluation of dogs naturally infected by Leishmania (Leishmania) chagasi submitted to treatment with meglumine antimoniate. Vet. Parasitol. 2007, 143, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, R.R.; Michalick, M. Canine Leishmaniasis: An Overview of the Current Status and Strategies for Control. BioMed Res. Int. 2018, 2018, 3296893. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.F.; Alexandre-Pires, G. Meglumine Antimoniate and Miltefosine Combined with Allopurinol Sustain Pro-inflammatory Immune Environments During Canine Leishmaniosis Treatment. Front. Vet. Sci. 2019, 6, 362. [Google Scholar] [CrossRef]
- Gradoni, L.; Maroli, M. Leishmania infantum infection rates in Phlebotomus perniciosus fed on naturally infected dogs under antimonial treatment. Med. Vet. Entomol. 1987, 1, 339–342. [Google Scholar] [CrossRef]
- Alvar, J.; Molina, R. Canine leishmaniasis: Clinical, parasitological and entomological follow-up after chemotherapy. Ann. Trop. Med. Parasitol. 1994, 88, 371–378. [Google Scholar] [CrossRef]
- Guarga, J.L.; Moreno, J. Evaluation of a specific immunochemotherapy for the treatment of canine visceral leishmaniasis. Vet. Immunol. Immunopathol. 2002, 88, 13–20. [Google Scholar] [CrossRef]
- Miró, G.; Gálvez, R. Infectivity to Phlebotomus perniciosus of dogs naturally parasitized with Leishmania infantum after different treatments. Parasites Vectors 2011, 4, 52. [Google Scholar] [CrossRef]
- da Silva, S.M.; Amorim, I.F. Efficacy of combined therapy with liposome-encapsulated meglumine antimoniate and allopurinol in treatment of canine visceral leishmaniasis. Antimicrob. Agents Chemother. 2012, 56, 2858–2867. [Google Scholar] [CrossRef]
- Travi, B.L.; Tabares, C.J. Canine visceral leishmaniasis in Colombia: Relationship between clinical and parasitologic status and infectivity for sand flies. Am. J. Trop. Med. Hyg. 2001, 64, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Noli, C.; Auxilia, S.T. Treatment of canine Old World visceral leishmaniasis: A systematic review. Vet. Dermatol. 2005, 16, 213–232. [Google Scholar] [CrossRef] [PubMed]
- Reguera, R.M.; Morán, M. Current status on prevention and treatment of canine leishmaniasis. Vet. Parasitol. 2016, 227, 98–114. [Google Scholar] [CrossRef] [PubMed]
- Manna, L.; Vitale, F. Study of efficacy of miltefosine and allopurinol in dogs with leishmaniosis. Vet. J. 2009, 182, 441–445. [Google Scholar] [CrossRef]
- Andrade, H.M.; Toledo, V.P. Evaluation of miltefosine for the treatment of dogs naturally infected with L. infantum (=L. chagasi) in Brazil. Vet. Parasitol. 2011, 181, 83–90. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Gonçalves, A.A.M.; Leite, J.C. An Overview of Immunotherapeutic Approaches Against Canine Visceral Leishmaniasis: What Has Been Tested on Dogs and a New Perspective on Improving Treatment Efficacy. Front. Cell Infect. Microbiol. 2019, 9, 427. [Google Scholar] [CrossRef]
- Baneth, G.; Shaw, S.E. Chemotherapy of canine leishmaniosis. Vet. Parasitol. 2002, 106, 315–324. [Google Scholar] [CrossRef]
- Manna, L.; Corso, R. Long-term follow-up of dogs with leishmaniosis treated with meglumine antimoniate plus allopurinol versus miltefosine plus allopurinol. Parasites Vectors 2015, 8, 289. [Google Scholar] [CrossRef]
- Soares, M.R.; de Mendonça, I.L. Canine visceral leishmaniasis in Teresina, Brazil: Relationship between clinical features and infectivity for sand flies. Acta Trop. 2011, 117, 6–9. [Google Scholar] [CrossRef]
- Paltrinieri, S.; Gradoni, L. Laboratory tests for diagnosing and monitoring canine leishmaniasis. Vet. Clin. Pathol. 2016, 45, 552–578. [Google Scholar] [CrossRef]
- Fawcett, T. An introduction to ROC analysis. Pattern Recognit. Lett. 2006, 27, 861–874. [Google Scholar] [CrossRef]
- Cortes, S.; Vaz, Y. Risk factors for canine leishmaniasis in an endemic Mediterranean region. Vet. Parasitol. 2012, 189, 189–196. [Google Scholar] [CrossRef]
- Schallig, H.D.; Cardoso, L. Seroepidemiology of canine leishmaniosis in Évora (southern Portugal): 20-year trends. Parasites Vectors 2013, 6, 100. [Google Scholar] [CrossRef] [PubMed]
- Viegas, C.; Requicha, J. Tongue nodules in canine leishmaniosis—A case report. Parasites Vectors 2012, 5, 120. [Google Scholar] [CrossRef] [PubMed]
- Márquez, M.; Pedregosa, J.R. Leishmania amastigotes in the central nervous system of a naturally infected dog. J. Vet. Diagn. Investig. 2013, 25, 142–146. [Google Scholar] [CrossRef]
- Wallborn, F.; Söffler, C. Leishmania-infantum-bedingte Knochenläsionen bei einem Hund [Leishmania infantum induced bone lesions in a dog]. Tierarztl Prax Ausg K Kleintiere Heimtiere 2016, 44, 278–282. [Google Scholar] [CrossRef]
- Abranches, P.; Silva-Pereira, M.C. Canine leishmaniasis: Pathological and ecological factors influencing transmission of infection. J. Parasitol. 1991, 77, 557–561. [Google Scholar] [CrossRef]
- Cardoso, L.; Schallig, H.D. Serological survey of Leishmania infection in dogs from the municipality of Peso da Régua (Alto Douro, Portugal) using the direct agglutination test (DAT) and fast agglutination screening test (FAST). Acta Trop. 2004, 91, 95–100. [Google Scholar] [CrossRef]
- Oliva, G.; Scalone, A. Incidence and time course of Leishmania infantum infections examined by parasitological, serologic, and nested-PCR techniques in a cohort of naive dogs exposed to three consecutive transmission seasons. J. Clin. Microbiol. 2006, 44, 1318–1322. [Google Scholar] [CrossRef]
- Miranda, S.; Roura, X. Characterization of sex, age, and breed for a population of canine leishmaniosis diseased dogs. Res. Vet. Sci. 2008, 85, 35–38. [Google Scholar] [CrossRef]
- Barati, M.; Mohebali, M. Canine visceral leishmaniasis: Seroprevalence survey of asymptomatic dogs in an endemic area of northwestern Iran. J. Parasites Dis. 2015, 39, 221–224. [Google Scholar] [CrossRef] [PubMed]
- Reis, A.B.; Teixeira-Carvalho, A. Isotype patterns of immunoglobulins: Hallmarks for clinical status and tissue parasite density in Brazilian dogs naturally infected by Leishmania (Leishmania) chagasi. Vet. Immunol. Immunopathol. 2006, 112, 102–116. [Google Scholar] [CrossRef] [PubMed]
- Athanasiou, L.V.; Petanides, T.A. Comparison of two commercial rapid in-clinic serological tests for detection of antibodies against Leishmania spp. in dogs. J. Vet. Diagn. Investig. 2014, 26, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Herrera, G.; Castillo, A. Evaluation of four rapid diagnostic tests for canine and human visceral Leishmaniasis in Colombia. BMC Infect. Dis. 2019, 19, 747. [Google Scholar] [CrossRef]
- Nicolato Rde, C.; de Abreu, R.T. Clinical forms of canine visceral Leishmaniasis in naturally Leishmania infantum-infected dogs and related myelogram and hemogram changes. PLoS ONE 2013, 8, e82947. [Google Scholar] [CrossRef]
- Meléndez-Lazo, A.; Ordeix, L. Clinicopathological findings in sick dogs naturally infected with Leishmania infantum: Comparison of five different clinical classification systems. Res. Vet. Sci. 2018, 117, 18–27. [Google Scholar] [CrossRef]
- Trópia de Abreu, R.; Carvalho, M. Influence of Clinical Status and Parasite Load on Erythropoiesis and Leucopoiesis in Dogs Naturally Infected with Leishmania (Leishmania) chagasi. PLoS ONE 2011, 6, e18873. [Google Scholar] [CrossRef]
- Harrus, S.; Kass, P.H. Canine monocytic ehrlichiosis: A retrospective study of 100 cases, and an epidemiological investigation of prognostic indicators for the disease. Vet. Rec. 1997, 141, 360–363. [Google Scholar] [CrossRef]
- Yu, I.B.; Huang, H.P. Prevalence and Prognosis of Anemia in Dogs with Degenerative Mitral Valve Disease. BioMed Res. Int. 2016, 2016, 4727054. [Google Scholar] [CrossRef]
- Eichenberger, R.M.; Riond, B. Prognostic Markers in Acute Babesia canis Infections. J. Vet. Intern. Med. 2016, 30, 174–182. [Google Scholar] [CrossRef]
- Zatelli, A.; Borgarelli, M. Glomerular lesions in dogs infected with Leishmania organisms. Am. J. Vet. Res. 2003, 64, 558–561. [Google Scholar] [CrossRef] [PubMed]
- Solano-Gallego, L.; Rodriguez-Cortes, A. Detection of Leishmania infantum DNA by fret-based real-time PCR in urine from dogs with natural clinical leishmaniosis. Vet. Parasitol. 2007, 147, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Alves, C.F.; de Amorim, I.F. Expression of IFN-gamma, TNF-alpha, IL-10 and TGF-beta in lymph nodes associates with parasite load and clinical form of disease in dogs naturally infected with Leishmania (Leishmania) chagasi. Vet. Immunol. Immunopathol. 2009, 128, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Bianciardi, P.; Brovida, C. Administration of miltefosine and meglumine antimoniate in healthy dogs: Clinicophatological evaluation of the impact on the Kidney. Toxicol. Pathol. 2009, 37, 770–775. [Google Scholar] [CrossRef]
- Koutinas, A.F.; Saridomichelakis, M.N. A randomised, blinded, placebo-controlled clinical trial with allopurinol in canine leishmaniosis. Vet. Parasitol. 2001, 98, 247–261. [Google Scholar] [CrossRef]
- Nascimento, L.F.M.; Miranda, D.F.H. Allopurinol therapy provides long term clinical improvement, but additional immunotherapy is required for sustained parasite clearance, in L. infantum-infected dogs. Vaccine X 2019, 4, 100048. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients (%) | ||
|---|---|---|
| Sex | Male | 59.6 |
| Female | 40.4 | |
| Breed | Mixed-breed | 47.5 |
| Labrador retriever | 16.2 | |
| Boxer | 5.0 | |
| Epagneul Breton | 4.0 | |
| German Shepherd | 3.0 | |
| Other breeds | 24.3 | |
| Age at diagnosis (years) | Young (<1) | 1.0 |
| Young adult (1–3) | 18.2 | |
| Adult (4–8) | 53.5 | |
| Mature (> 8) | 27.3 |
| Clinical Signs | Patients (%) |
| Dermatological signs | 67.4 |
| Weight loss | 40.0 |
| Lymphadenomegaly | 21.0 |
| Osteoarticular pathology and muscle atrophy | 18.9 |
| Ocular pathology | 14.7 |
| Splenomegaly | 10.5 |
| Gastrointestinal signs | 10.5 |
| Anorexia | 10.5 |
| Epistaxis | 4.2 |
| Fever | 2.1 |
| Others | 21.0 |
| Analytic Panel | Abnormalities | Reference Range | Patients (%) |
|---|---|---|---|
| Erythrogram | Anemia | Ht 37–55% | 60.4 |
| Mild anemia | Ht 30–37% | 44.8 | |
| Moderate anemia | Ht 20–30% | 51.7 | |
| Severe anemia | Ht < 20% | 3.4 | |
| Leucogram | Leukocytosis | 6.0–17.0 (×109/L) | 9.6 |
| Leukopenia | 6.0–17.0 (×109/L) | 7.4 | |
| Lymphocytosis | 0.8–5.1 (×109/L) | 9.6 | |
| Lymphopenia | 0.8–5.1 (×109/L) | 2.1 | |
| Monocytosis | 0.0–1.8 (×109/L) | 18.0 | |
| Neutrophilia | 4.0–12.6 (×109/L) | 7.3 | |
| Neutropenia | 4.0–12.6 (×109/L) | 10.4 | |
| Platelet count | Thrombocytopenia | 117–460 (×109/μL) | 18.3 |
| Biochemical profile | Hyperproteinemia | 5.5–7.5 g/dL | 52.8 |
| Hypoproteinemia | 5.5–7.5 g/dL | 8.8 | |
| Creatinemia | 0.4–1.2 mg/dL | 18.3 | |
| Uremia | 6–24 mg/dL | 43.2 | |
| Elevated ALP | 0–85 UI/L | 12.0 | |
| Elevated GPT | 13–92 UI/L | 10.4 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pereira, M.A.; Santos, R.; Oliveira, R.; Costa, L.; Prata, A.; Gonçalves, V.; Roquette, M.; Vala, H.; Santos-Gomes, G. Prognostic Factors and Life Expectancy in Canine Leishmaniosis. Vet. Sci. 2020, 7, 128. https://doi.org/10.3390/vetsci7030128
Pereira MA, Santos R, Oliveira R, Costa L, Prata A, Gonçalves V, Roquette M, Vala H, Santos-Gomes G. Prognostic Factors and Life Expectancy in Canine Leishmaniosis. Veterinary Sciences. 2020; 7(3):128. https://doi.org/10.3390/vetsci7030128
Chicago/Turabian StylePereira, Maria Aires, Rute Santos, Ricardo Oliveira, Lina Costa, Ana Prata, Vânia Gonçalves, Madalena Roquette, Helena Vala, and Gabriela Santos-Gomes. 2020. "Prognostic Factors and Life Expectancy in Canine Leishmaniosis" Veterinary Sciences 7, no. 3: 128. https://doi.org/10.3390/vetsci7030128
APA StylePereira, M. A., Santos, R., Oliveira, R., Costa, L., Prata, A., Gonçalves, V., Roquette, M., Vala, H., & Santos-Gomes, G. (2020). Prognostic Factors and Life Expectancy in Canine Leishmaniosis. Veterinary Sciences, 7(3), 128. https://doi.org/10.3390/vetsci7030128