Breed-Specific Variations in Vertebral Right Heart Index (VRHi): Implications for Detection of True and False Right Heart Enlargement (RHE) in Dogs


Simple Summary
Abstract
1. Introduction
- (a)
- Investigate breed-specific variations in VRHi among dogs with apparent radiographic RHE but a normal cardiac anatomy;
- (b)
- Compare the VRHi values between dogs with and without RHE in the NBC and brachycephalic breeds;
- (c)
- Establish VRHi cutoff values to differentiate true RHE from false-positive cases;
- (d)
- Examine factors contributing to false-positive RHE diagnoses, including echocardiographic parameters and thoracic conformation.
2. Materials and Methods
2.1. Data Recording Analysis
2.2. Data Collection and Thoracic Radiography Evaluation
2.3. Data Collection and Echocardiographic Evaluation
2.4. Statistical Analysis
3. Results
3.1. Study Population
3.2. Imaging and Statistical Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bahr, R.J. Canine and feline cardiovascular system. In Textbook of Veterinary Diagnostic Radiology; Thrall, D.E., Ed.; Saunders Elsevier: Philadelphia, PA, USA, 2018; pp. 684–709. [Google Scholar]
- Jepsen-Grant, K.; Pollard, R.E.; Johnson, L.R. Vertebral heart scores in eight dog breeds. Vet. Radiol. Ultrasound 2013, 54, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Puccinelli, C.; Vezzosi, T.; Grosso, G.; Citi, S.; Della Santa, D.; Buralli, C.; Marchetti, V.; Tognetti, R. The vertebral right heart index: A new radiographic method to assess right heart enlargement in dogs. Vet. Radiol. Ultrasound 2024, 65, 596–602. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, C.; Häggström, J.; Eriksson, A.; Järvinen, A.-K.; Kvart, C.; Lord, P. Size and Shape of Right Heart Chambers in Mitral Valve Regurgitation in Small-Breed Dogs. J. Vet. Intern. Med. 2009, 23, 1013–1020. [Google Scholar] [CrossRef]
- Reinero, C.; Visser, L.C.; Kellihan, H.B.; Masseau, I.; Rozanski, E.; Clercx, C.; Williams, K.; Abbott, J.; Borgarelli, M.; Scansen, B.A. ACVIM consensus statement guidelines for the diagnosis, classification, treatment, and monitoring of pulmonary hypertension in dogs. J. Vet. Intern. Med. 2020, 34, 549–573. [Google Scholar] [CrossRef]
- Buchanan, J.W.; Bücheler, J. Vertebral scale system to measure canine heart size in radiographs. J. Am. Vet. Med. Assoc. 1995, 206, 194–199. [Google Scholar] [CrossRef]
- Corcoran, B.M. Static respiratory compliance in normal dogs. J. Small Anim. Pract. 1991, 32, 438–442. [Google Scholar] [CrossRef]
- Asorey, I.; Pellegrini, L.; Canfrán, S.; Ortiz-Díez, G.; Aguado, D. Factors affecting respiratory system compliance in anaesthetised mechanically ventilated healthy dogs: A retrospective study. J. Small Anim. Pract. 2020, 61, 617–623. [Google Scholar] [CrossRef]
- Phansangiemjit, A.; Kasemjiwat, K.; Patchanee, K.; Panninvong, Y.; Sunisarud, A.; Choisunirachon, N.; Thanaboonnipat, C. The Differences in Radiographic Vertebral Size in Dogs with Different Chest and Skull Types. Animals 2024, 14, 470. [Google Scholar] [CrossRef]
- Thomas, W.P.; Gaber, C.E.; Jacobs, G.J.; Kaplan, P.M.; Lombard, C.W.; Moise, N.S.; Moses, B.L. Recommendations for standards in transthoracic two-dimensional echocardiography in the dog and cat. Vet. Rad. Ultrasound 1994, 35, 173–178. [Google Scholar] [CrossRef]
- Gentile-Solomon, J.M.; Abbott, J.A. Conventional Echocardiographic Assessment of the Canine Right Heart: Reference Intervals and Repeatability. J. Vet. Cardiol. 2016, 18, 234–247. [Google Scholar] [CrossRef]
- Visser, L.C.; Scansen, B.A.; Schober, K.E.; Bonagura, J.D. Echocardiographic assessment of right ventricular systolic function in conscious healthy dogs: Repeatability and reference intervals. J. Vet. Cardiol. 2015, 17, 83–96. [Google Scholar] [CrossRef] [PubMed]
- Vezzosi, T.; Domenech, O.; Costa, G.; Marchesotti, F.; Venco, L.; Zini, E.; Del Palacio, M.J.F.; Tognetti, R. Echocardiographic evaluation of the right ventricular dimension and systolic function in dogs with pulmonary hypertension. J. Vet. Intern. Med. 2018, 32, 1541–1548. [Google Scholar] [CrossRef] [PubMed]
- Vezzosi, T.; Domenech, O.; Iacona, M.; Marchesotti, F.; Zini, E.; Venco, L.; Tognetti, R. Echocardiographic evaluation of the right atrial area index in dogs with pulmonary hypertension. J. Vet. Intern. Med. 2018, 32, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Visser, L.C.; Im, M.K.; Johnson, L.R.; Stern, J.A. Diagnostic value of right pulmonary artery distensibility index in dogs with pulmonary hypertension: Comparison with doppler echocardiographic estimates of pulmonary arterial pressure. J. Vet. Intern. Med. 2016, 30, 543–552. [Google Scholar] [CrossRef]
- Feldhütter, E.K.; Domenech, O.; Vezzosi, T.; Bussadori, C.; Zini, E.; Marchesotti, F.; Venco, L.; Tognetti, R. Echocardiographic reference intervals for right ventricular indices, including 3-dimensional volume and 2-dimensional strain measurements in healthy dogs. J. Vet. Intern. Med. 2022, 36, 8–19. [Google Scholar] [CrossRef]
- Malcolm, E.L.; Visser, L.C.; Phillips, K.L.; Johnson, L.R. Diagnostic value of vertebral left atrial size as determined from thoracic radiographs for assessment of left atrial size in dogs with myxomatous mitral valve disease. J. Am. Vet. Med. Assoc. 2018, 253, 1038–1045. [Google Scholar] [CrossRef]
- Sánchez Salguero, X.; Prandi, D.; Llabrés-Díaz, F.; Manzanilla, E.G.; Bussadori, C. A radiographic measurement of left atrial size in dogs. Ir. Vet. J. 2018, 71, 25. [Google Scholar] [CrossRef]
- Lamb, C.R.; Tyler, M.; Boswood, A.; Skelly, B.J.; Cain, M. Assessment of the value of the vertebral heart scale in the radiographic diagnosis of cardiac disease in dogs. Vet. Rec. 2000, 146, 687–690. [Google Scholar] [CrossRef]
- Stepien, R.L.; Rak, M.B.; Blume, L.M. Use of radiographic measurements to diagnose stage B2 preclinical myxomatous mitral valve disease in dogs. J. Am. Vet. Med. Assoc. 2020, 256, 1129–1136. [Google Scholar] [CrossRef]
- Vezzosi, T.; Puccinelli, C.; Citi, S.; Tognetti, R. Two radiographic methods for assessing left atrial enlargement and cardiac remodeling in dogs with myxomatous mitral valve disease. J. Vet. Cardiol. 2021, 34, 55–63. [Google Scholar] [CrossRef]
- Adams, D.S.; Marolf, A.J.; Valdés-Martínez, A.; Randall, E.K.; Bachand, A.M. Associations between thoracic radiographic changes and severity of pulmonary arterial hypertension diagnosed in 60 dogs via Doppler echocardiography: A retrospective study. Vet. Radiol. Ultrasound 2017, 58, 454–462. [Google Scholar] [CrossRef] [PubMed]
- Schad, N.; Stark, P. The radiologic features of cardiac rotation: A pictorial essay. J. Thorac. Imaging 1992, 7, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Manheimer, E. Chest Roentgenography for Cardiovascular Evaluation. In Clinical Methods: The History, Physical, and Laboratory Examinations, 3rd ed.; Walker, H.K., Hall, W.D., Hurst, J.W., Eds.; Butterworths: Boston, MA, USA, 1990; pp. 186–190. [Google Scholar]
- Genovese, D.; Mor-Avi, V.; Palermo, C.; Muraru, D.; Volpato, V.; Kruse, E.; Yamat, M.; Aruta, P.; Addetia, K.; Badano, L.P.; et al. Comparison Between Four-Chamber and Right Ventricular-Focused Views for the Quantitative Evaluation of Right Ventricular Size and Function. J. Am. Soc. Echocardiogr. 2019, 32, 484–494. [Google Scholar] [CrossRef] [PubMed]
- Roberts, T.; McGreevy, P.; Valenzuela, M. Human Induced Rotation and Reorganization of the Brain of Domestic Dogs. PLoS ONE 2010, 5, e11946. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | M/F (N) | Age (Years) (Mean ± SD, Range) | Weight (kg) (Mean ± SD) |
|---|---|---|---|
| Brachycephalic breeds | |||
| Without RHE | 32/39 | 10.5 ± 3.7 (1–19) | 5.6 ± 2.3 |
| With RHE | 23/24 | 11.4 ± 3.5 (1–17) | 5.4 ± 2.7 |
| NBC breeds | |||
| Without RHE | 34/30 | 10.3 ± 2.9 (1–14) | 7.3 ± 6.2 |
| With RHE | 14/9 | 7.0 ± 3.8 (1–15) | 10.3 ± 7.4 |
| Schnauzers | 19/12 | 12.0 ± 2.5 (8–18) | 7.4 ± 2.4 |
| Dachshunds | 18/13 | 10.5 ± 3.7 (2–18) | 7.4 ± 2.2 |
| Pomeranians | 8/22 | 10.5 ± 3.4 (5–18) | 3.5 ± 1.2 |
| Yorkshire Terriers | 10/20 | 11.6 ± 3.0 (3–17) | 3.5 ± 1.7 |
| Miniature Pinschers | 13/19 | 11.0 ± 2.5 (6–15) | 5.1 ± 1.3 |
| Group | RL VRHi (Mean ± SD, v) | VD VRHi (Mean ± SD, v) | p Value (Breed vs. NBC) * | |
|---|---|---|---|---|
| RL VRHi | VD VRHi | |||
| NBC | 3.07 ± 0.24 | 2.32 ± 0.36 | - | - |
| Brachycephalic breeds | 3.29 ± 0.33 | 2.43 ± 0.43 | <0.001 | 0.133 |
| Schnauzer | 3.55 ± 0.32 | 2.80 ± 0.40 | <0.001 | <0.001 |
| Dachshund | 3.34 ± 0.33 | 2.34 ± 0.37 | <0.001 | 0.802 |
| Pomeranian | 3.48 ± 0.33 | 2.71 ± 0.42 | <0.001 | <0.001 |
| Yorkshire Terrier | 3.32 ± 0.35 | 2.67 ± 0.35 | <0.001 | <0.001 |
| Miniature Pinscher | 3.48 ± 0.34 | 2.66 ± 0.34 | <0.001 | <0.001 |
| Group | RVWTd Index (Mean ± SD) (cm/kg0.250) (N) | RVEDA Index (Mean ± SD) (cm2/kg0.624) (N) | RAA Index (Mean ± SD) (cm2/kg0.714) (N) | p Value (Breed vs. NBC) * | ||
|---|---|---|---|---|---|---|
| RVWTd Index | RVEDA Index | RAA Index | ||||
| NBC | 0.301 ± 0.059 (57) | 0.593 ± 0.182 (46) | 0.433 ± 0.130 (63) | - | - | - |
| Brachycephalic breeds | 0.313 ± 0.040 (67) | 0.539 ± 0.202 (54) | 0.430 ± 0.150 (69) | 0.205 | 0.164 | 0.894 |
| Schnauzer | 0.288 ± 0.053 (29) | 0.618 ± 0.164 (28) | 0.441 ± 0.136 (31) | 0.314 | 0.564 | 0.803 |
| Dachshund | 0.280 ± 0.055 (27) | 0.628 ± 0.178 (26) | 0.400 ± 0.101 (31) | 0.122 | 0.439 | 0.210 |
| Pomeranian | 0.283 ± 0.043 (26) | 0.590 ± 0.149 (25) | 0.443 ± 0.125 (30) | 0.151 | 0.937 | 0.744 |
| Yorkshire Terrier | 0.295 ± 0.042 (24) | 0.616 ± 0.098 (22) | 0.462 ± 0.096 (29) | 0.641 | 0.583 | 0.299 |
| Miniature Pinscher | 0.284 ± 0.055 (22) | 0.604 ± 0.140 (22) | 0.435 ± 0.119 (32) | 0.237 | 0.812 | 0.943 |
| Group | RL VRHi (Mean ± SD) (v) | VD VRHi (Mean ± SD) (v) | p Value * | RVWTd Index (Mean ± SD) (cm/kg0.250) (N) | RVEDA Index (Mean ± SD) (cm2/kg0.624) (N) | RAA Index (Mean ± SD) (cm2/kg0.714) (N) | ||
|---|---|---|---|---|---|---|---|---|
| RL VRHi | VD VRHi | |||||||
| NBC | Without RHE | 3.07 ± 0.24 | 2.32 ± 0.36 | <0.001 | <0.001 | 0.301 ± 0.059 (57) | 0.593 ± 0.182 (46) | 0.433 ± 0.130 (63) |
| With RHE | 3.77 ± 0.50 | 2.65 ± 0.47 | 0.348 ± 0.053 (23) | 1.292 ± 0.340 (23) | 1.140 ± 0.485 (23) | |||
| Brachycephalic | Without RHE | 3.29 ± 0.33 | 2.43 ± 0.43 | <0.001 | <0.001 | 0.313 ± 0.040 (67) | 0.539 ± 0.202 (54) | 0.430 ± 0.150 (69) |
| With RHE | 3.74 ± 0.42 | 3.0 ± 0.46 | 0.354 ± 0.067 (47) | 1.163 ± 0.343 (47) | 1.115 ± 0.367 (47) | |||
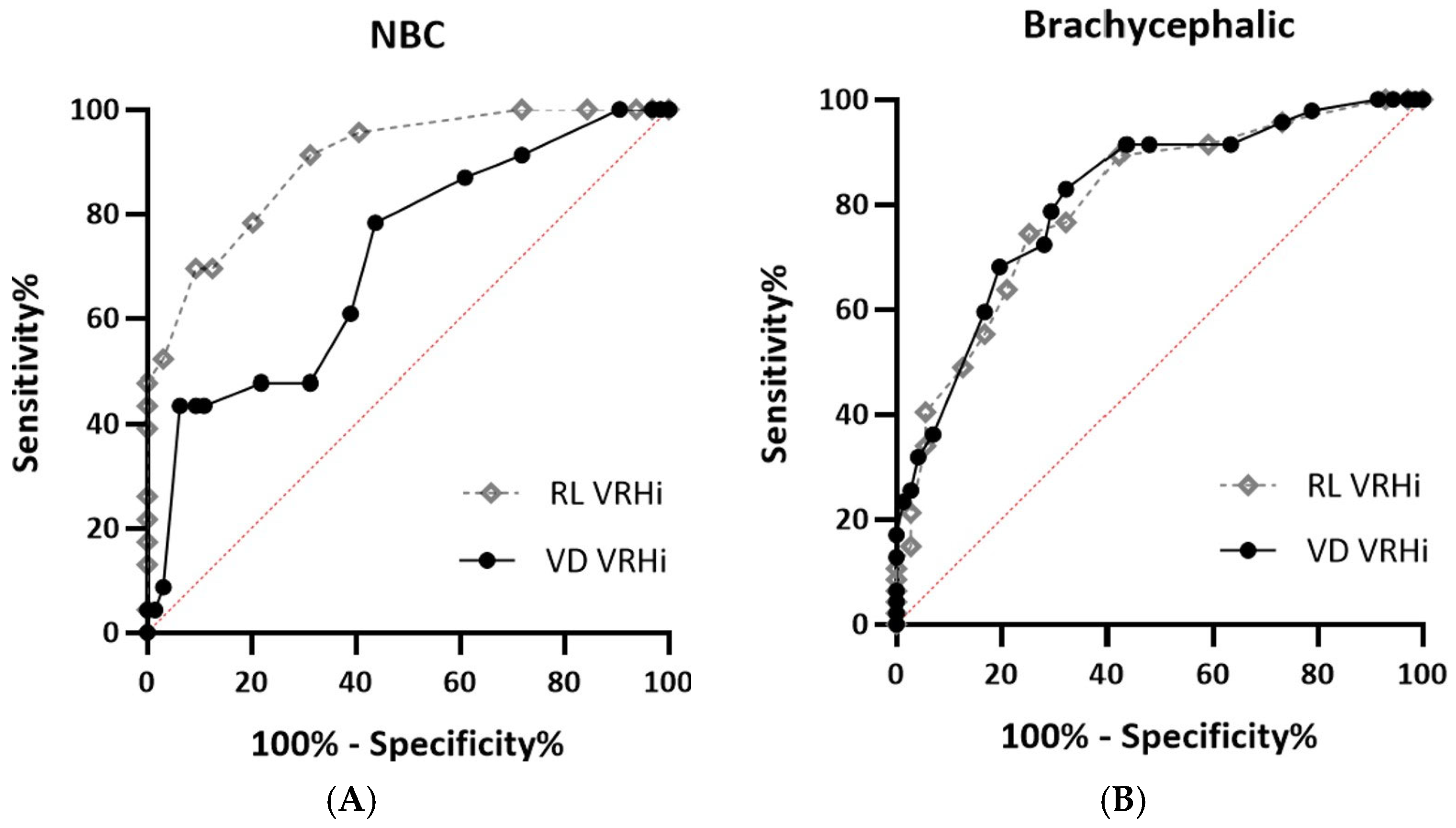
| Group | AUC | 95% CI | Cutoff (v) | Sn (%) | Sp (%) | |
|---|---|---|---|---|---|---|
| Brachycephalic | RL VRHi | 0.80 | 0.72–0.88 | ≥3.45 | 75 | 75 |
| ≥2.95 | 100 | 7 | ||||
| ≥4.25 | 11 | 100 | ||||
| VD VRHi | 0.81 | 0.74–0.89 | ≥2.75 | 72 | 72 | |
| ≥1.95 | 100 | 8 | ||||
| ≥3.45 | 17 | 100 | ||||
| NBC | RL VRHi | 0.90 | 0.83–0.97 | ≥3.25 | 78 | 80 |
| ≥2.95 | 100 | 28 | ||||
| ≥3.80 | 48 | 100 | ||||
| VD VRHi | 0.71 | 0.59–0.84 | ≥2.4 | 61 | 61 | |
| ≥1.95 | 100 | 9 | ||||
| ≥3.6 | 4 | 100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, K.; Kim, J.; Eom, K.; Koo, J.; Jeong, I.; Park, C. Breed-Specific Variations in Vertebral Right Heart Index (VRHi): Implications for Detection of True and False Right Heart Enlargement (RHE) in Dogs. Vet. Sci. 2025, 12, 300. https://doi.org/10.3390/vetsci12040300
Choi K, Kim J, Eom K, Koo J, Jeong I, Park C. Breed-Specific Variations in Vertebral Right Heart Index (VRHi): Implications for Detection of True and False Right Heart Enlargement (RHE) in Dogs. Veterinary Sciences. 2025; 12(4):300. https://doi.org/10.3390/vetsci12040300
Chicago/Turabian StyleChoi, Kawon, Jaehwan Kim, Kidong Eom, Jongwon Koo, Inseong Jeong, and Chul Park. 2025. "Breed-Specific Variations in Vertebral Right Heart Index (VRHi): Implications for Detection of True and False Right Heart Enlargement (RHE) in Dogs" Veterinary Sciences 12, no. 4: 300. https://doi.org/10.3390/vetsci12040300
APA StyleChoi, K., Kim, J., Eom, K., Koo, J., Jeong, I., & Park, C. (2025). Breed-Specific Variations in Vertebral Right Heart Index (VRHi): Implications for Detection of True and False Right Heart Enlargement (RHE) in Dogs. Veterinary Sciences, 12(4), 300. https://doi.org/10.3390/vetsci12040300