


Transcutaneous Auricular Vagal Nerve Stimulation in Healthy Non-Sedated Horses: A Feasibility Study
 , , , ,
, , , ,  and
and
Abstract
Simple Summary
Abstract
1. Introduction
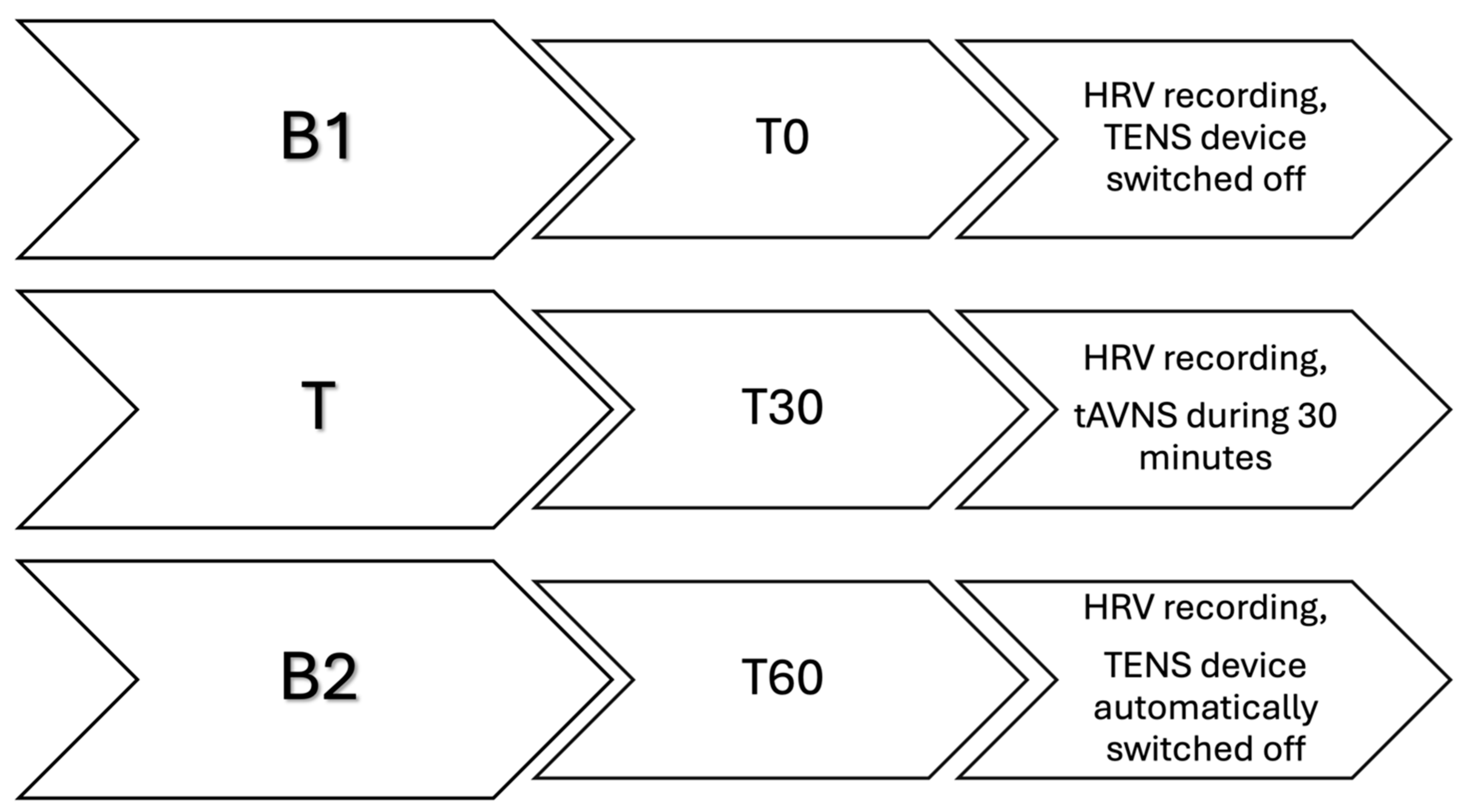
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| Ach | acetylcholine |
| ABVN | auricular branch of the vagal nerve |
| fMRI | functional magnetic resonance imaging |
| GI | gastrointestinal |
| HF | high frequency |
| HR | heart rate |
| HRV | heart rate variability |
| LF | low frequency |
| PNSi | parasympathetic nervous system index |
| POI | post-operative ileus |
| RMSSD | root mean square of successive |
| SDRR | standard deviation of R–R intervals |
| SD1 | standard deviation 1 of Poincaré plot |
| SD2 | standard deviation 2 of Poincaré plot |
| SNSi | sympathetic nervous system index |
| STi | stress index |
| tAVNS | transcutaneous auricular vagal nerve stimulation |
| TENS | transcutaneous electrical nerve stimulation |
References
- Lisowski, Z.M.; Pirie, R.S.; Blikslager, A.T.; Lefebvre, D.; Hume, D.A.; Hudson, N.P.H. An update on equine post-operative ileus: Definitions, pathophysiology and management. Equine Vet. J. 2018, 2, 292–303. [Google Scholar] [CrossRef] [PubMed]
- Vather, R.; O’Grady, G.; Bissett, I.P.; Dinning, P.G. Postoperative ileus: Mechanisms and future directions for research. Clin. Exp. Pharmacol. Physiol. 2014, 2, 358–370. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, H.; Tsuchida, D.; Koda, K.; Miyazaki, M.; Pappas, T.N.; Takahashi, T. Inhibition of sympathetic pathways restores postoperative ileus in the upper and lower gastrointestinal tract. J. Gastroenterol. Hepatol. 2007, 2, 1293–1299. [Google Scholar] [CrossRef] [PubMed]
- Hellstrom, E.A.; Ziegler, A.L.; Blikslager, A.T. Postoperative Ileus: Comparative Pathophysiology and Future Therapies. Front. Vet. Sci. 2021, 8, 714800. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lefebvre, D.; Hudson, N.P.H.; Elce, Y.A.; Blikslager, A.; Divers, T.J.; Handel, I.G.; Tremaine, W.H.; Pirie, R.S. Clinical features and management of equine post operative ileus (POI): Survey of Diplomates of the American Colleges of Veterinary Internal Medicine (ACVIM), Veterinary Surgeons (ACVS) and Veterinary Emergency and Critical Care (ACVECC). Equine Vet. J. 2016, 2, 714–719. [Google Scholar] [CrossRef] [PubMed]
- Lefebvre, D.; Pirie, R.S.; Handel, I.G.; Tremaine, W.H.; Hudson, N.P. Clinical features and management of equine post operative ileus: Survey of diplomates of the European Colleges of Equine Internal Medicine (ECEIM) and Veterinary Surgeons (ECVS). Equine Vet. J. 2016, 2, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Berghmans, T.M.; Hulsewé, K.W.; Buurman, W.A.; Luyer, M.D. Stimulation of the autonomic nervous system in colorectal surgery: A study protocol for a randomized controlled trial. Trials 2012, 13, 93. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Helman, C.A. Chewing gum is as effective as food in stimulating cephalic phase gastric secretion. Am. J. Gastroenterol. 1988, 2, 640–642. [Google Scholar] [PubMed]
- Giusto, G.; Pagliara, E.; Gandini, M. Effects of Bit Chewing on Right Upper Quadrant Intestinal Sound Frequency in Adult Horses. J. Equine Vet. Sci. 2014, 2, 520–523. [Google Scholar] [CrossRef]
- Butt, M.F.; Albusoda, A.; Farmer, A.D.; Aziz, Q. The anatomical basis for transcutaneous auricular vagus nerve stimulation. J. Anat. 2020, 2, 588–611. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- He, W.; Wang, X.; Shi, H.; Shang, H.; Li, L.; Jing, X.; Zhu, B. Auricular acupuncture and vagal regulation. Evid. Based Complement. Alternat Med. 2012, 2012, 786839. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Asher, G.N.; Jonas, D.E.; Coeytaux, R.R.; Reilly, A.C.; Loh, Y.L.; Motsinger-Reif, A.A.; Winham, S.J. Auriculotherapy for pain management: A systematic review and meta-analysis of randomized controlled trials. J. Altern. Complement. Med. 2010, 2, 1097–1108. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Usichenko, T.; Hacker, H.; Lotze, M. Transcutaneous auricular vagal nerve stimulation (taVNS) might be a mechanism behind the analgesic effects of auricular acupuncture. Brain Stimul. 2017, 2, 1042–1044. [Google Scholar] [CrossRef] [PubMed]
- Ru, O.; Jin, X.; Qu, L.; Long, D.; Liu, M.; Cheng, L.; Jiang, Y. Low-intensity transcutaneous auricular vagus nerve stimulation reduces postoperative ileus after laparoscopic radical resection of colorectal cancer: A randomized controlled trial. Minerva Anestesiol. 2023, 2, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Xu, F.; Lu, D.; Rong, P.; Cheng, J.; Li, M.; Gong, Y.; Sun, C.; Wei, W.; Lin, L.; et al. Transcutaneous auricular vagal nerve stimulation improves functional dyspepsia by enhancing vagal efferent activity. Am. J. Physiol. Gastrointest. Liver Physiol. 2021, 2, G700–G711. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Vitale, V.; Balocchi, R.; Varanini, M.; Sgorbini, M.; Macerata, A.; Sighieri, C.; Baragli, P. The effects of restriction of movement on the reliability of heart rate variability measurements in the horse (Equus caballus). J. Vet. Behavior. 2013, 2, 400–403. [Google Scholar] [CrossRef]
- Tarvainen, M.P.; Niskanen, J.P.; Lipponen, J.A.; Ranta-Aho, P.O.; Karjalainen, P.A. Kubios HRV--heart rate variability analysis software. Comput. Methods Programs Biomed. 2014, 2, 210–220. [Google Scholar] [CrossRef] [PubMed]
- Mouchtouri, E.-T.; Lekkas, P.; Delis, F.; Pantelakis, E.; Mourouzis, I.; Pantos, C.; Kolettis, T.M. Sympathetic and Vagal Responses Elicited by Acute Stress in Rats. Cureus 2020, 2, e11602. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rietmann, T.; Stuart, A.; Bernasconi, P.; Stauffacher, M.; Auer, J.A.; Weishaupt, M.A. Assessment of mental stress in warmblood horses: Heart rate variability in comparison to heart rate and selected behavioural parameters. Appl. Anim. Behav. Sci. 2004, 88, 121–136. [Google Scholar] [CrossRef]
- Tekdemir, I.; Aslan, A.; Elhan, A. A clinico-anatomic study of the auricular branch of the vagus nerve and Arnold’s ear-cough reflex. Surg. Radiol. Anat. 1998, 2, 253–257. [Google Scholar] [PubMed]
- Yu, L.; Scherlag, B.J.; Li, S.; Fan, Y.; Dyer, J.; Male, S.; Varma, V.; Sha, Y.; Stavrakis, S.; Po, S.S. Low-level transcutaneous electrical stimulation of the auricular branch of the vagus nerve: A noninvasive approach to treat the initial phase of atrial fibrillation. Heart Rhythm. 2013, 2, 428–435. [Google Scholar] [CrossRef] [PubMed]
- Vitale, V.; Viu, J.; Armengou, L.; Ríos, J.; Jose-Cunilleras, E. Prognostic value of measuring heart rate variability at the time of hospital admission in horses with colic. Am. J. Vet. Res. 2020, 2, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Hong, G.-S.; Pintea, B.; Lingohr, P.; Coch, C.; Randau, T.; Schaefer, N.; Wehner, S.; Kalff, J.C.; Pantelis, D. Effect of transcutaneous vagus nerve stimulation on muscle activity in the gastrointestinal tract (transVaGa): A prospective clinical trial. Int. J. Color. Dis. 2019, 2, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Badran, B.; Glusman, C.; Badran, A.; Austelle, C.; DeVries, W.; Borckhardt, J.; George, M. The physiological and neurobiological effects of transcutaneous auricular vagus nerve stimulation (taVNS). Brain Stimul. 2017, 2, 378. [Google Scholar] [CrossRef]
- Clancy, J.A.; Mary, D.A.; Witte, K.K.; Greenwood, J.P.; Deuchars, S.A.; Deuchars, J. Non-invasive vagus nerve stimulation in healthy humans reduces sympathetic nerve activity. Brain Stimul. 2014, 2, 871–877. [Google Scholar] [CrossRef] [PubMed]
- Groves, D.A.; Brown, V.J. Vagal nerve stimulation: A review of its applications and potential mechanisms that mediate its clinical effects. Neurosci. Biobehav. Rev. 2005, 2, 493–500. [Google Scholar] [CrossRef] [PubMed]
- Castoro, M.A.; Yoo, P.B.; Hincapie, J.G.; Hamann, J.J.; Ruble, S.B.; Wolf, P.D.; Grill, W.M. Excitation properties of the right cervical vagus nerve in adult dogs. Exp. Neurol. 2011, 2, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Sluka, K.A.; Walsh, D. Transcutaneous electrical nerve stimulation: Basic science mechanisms and clinical effectiveness. J. Pain. 2003, 2, 109–121. [Google Scholar] [CrossRef] [PubMed]
- Safi, S.; Ellrich, J.; Neuhuber, W. Myelinated Axons in the Auricular Branch of the Human Vagus Nerve. Anat. Rec. 2016, 2, 1184–1191. [Google Scholar] [CrossRef] [PubMed]
- Thor, P.J.; Furgała, A.; Mazur, M.; Pośnik-Urbańska, A.; Kolasińska-Kloch, W.; Czarnecka, D.; Kawecka-Jaszcz, K. Comparison of cardiac and gastric responses to vagal stimulation in hypertensive women. Med. Sci. Monit. 2009, 2, Cr504–Cr511. [Google Scholar] [PubMed]
- Sanders, K.M.; Ward, S.M. Interstitial cells of Cajal: A new perspective on smooth muscle function. J. Physiol. 2006, 576 Pt 3, 721–726. [Google Scholar] [CrossRef] [PubMed]
- Tracey, K.J. The inflammatory reflex. Nature 2002, 2, 853–859. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| B1 | T | B2 | Statistical Significance | |
|---|---|---|---|---|
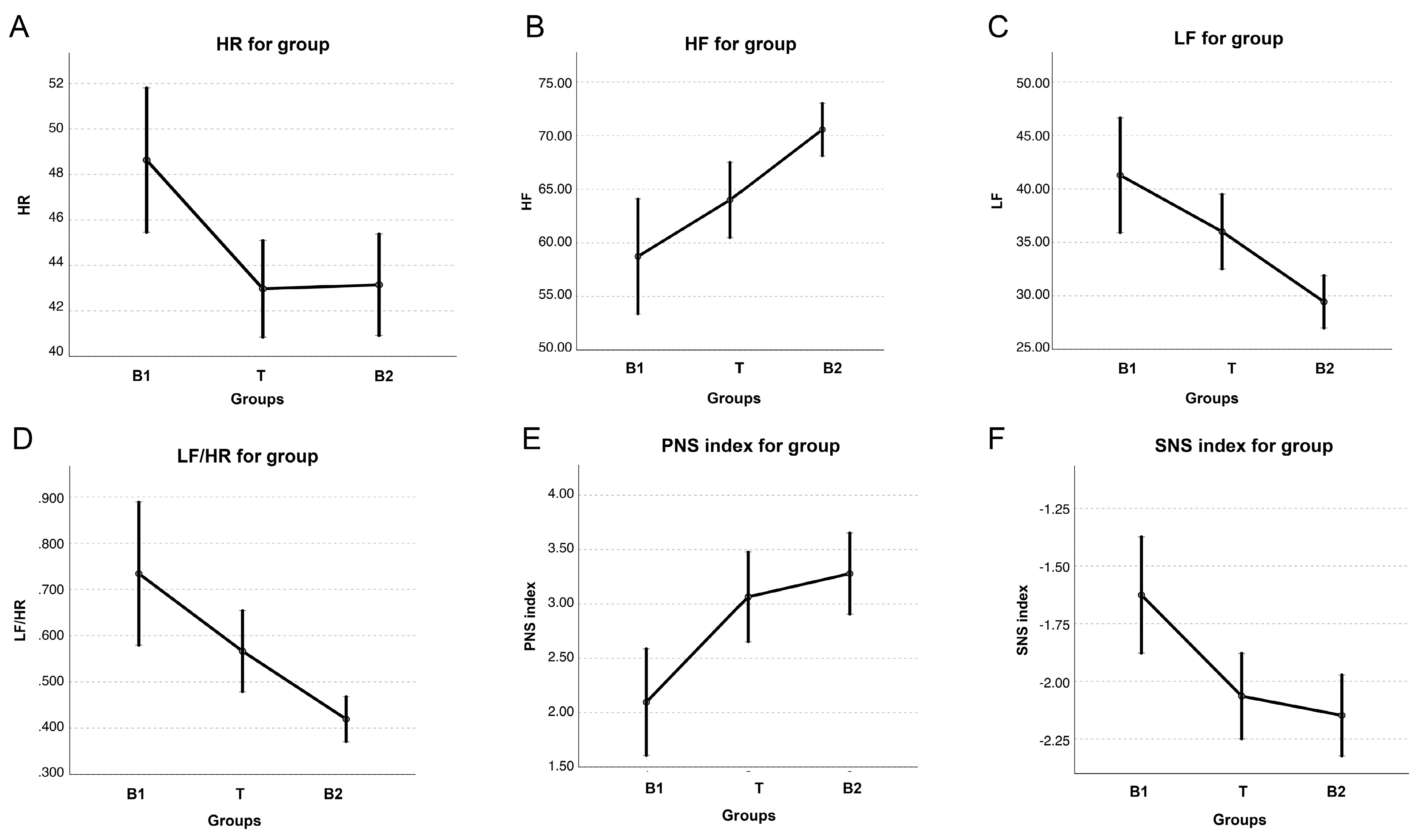
| HR (bpm) | 40.5 (38.7–53.0) a | 41.0 (38.0–43.0) a,b | 40.0 (35.0–43.0) b | p = 0.012 |
| SDRR (ms) | 60.2 (52.7–88.8) a | 67.7 (54.7–83.8) a | 55.6 (44.7–67.6) b | p = 0.009 |
| RMSSD (ms) | 68.5 (52.5–94.1) | 72.5 (62.8–89.4) | 71.4 (58.3–82.5) | NS |
| SD1 (ms) | 48.5 (37.2–66.7) | 51.4 (44.5–63.4) | 50.6 (41.4–58.5) | p = 0.014 |
| SD2 (ms) | 73.6 (60.1–108.4) a | 78.4 (61.3–100.6) a | 61.0 (45.3–75.9) b | NS |
| HF (n.u.) | 61.1 (51.7–74.1) a | 63.6 (55.9–74.8) a | 71.4 (65.8–80.6) b | p = 0.004 |
| LF (n.u.) | 38.9 (25.9–48.3) a | 36.4 (25.2–44.1) a | 28.6 (19.4–34.1) b | p = 0.004 |
| LF/HF | 0.6 (0.3–0.9) a | 0.6 (0.3–0.8) a | 0.4 (0.2–0.5) b | p = 0.014 |
| PNSi | 2.9 (2.3–3.7) a | 3.1 (2.6–4.0) a,b | 3.5 (2.9–4.3) b | p = 0.009 |
| SNSi | −2.0 (−2.4–−1.6) a | −2.2 (−2.4–−1.9) a,b | −2.3 (−2.5–−2.1) b | p = 0.004 |
| STi | 5.8 (4.0–6.8) | 5.3 (4.4–6.4) | 6.1 (5.5–6.8) | NS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vitale, V.; Bindi, F.; Velloso Alvarez, A.; de la Cuesta-Torrado, M.; Sala, G.; Sgorbini, M. Transcutaneous Auricular Vagal Nerve Stimulation in Healthy Non-Sedated Horses: A Feasibility Study. Vet. Sci. 2024, 11, 241. https://doi.org/10.3390/vetsci11060241
Vitale V, Bindi F, Velloso Alvarez A, de la Cuesta-Torrado M, Sala G, Sgorbini M. Transcutaneous Auricular Vagal Nerve Stimulation in Healthy Non-Sedated Horses: A Feasibility Study. Veterinary Sciences. 2024; 11(6):241. https://doi.org/10.3390/vetsci11060241
Chicago/Turabian StyleVitale, Valentina, Francesca Bindi, Ana Velloso Alvarez, María de la Cuesta-Torrado, Giulia Sala, and Micaela Sgorbini. 2024. "Transcutaneous Auricular Vagal Nerve Stimulation in Healthy Non-Sedated Horses: A Feasibility Study" Veterinary Sciences 11, no. 6: 241. https://doi.org/10.3390/vetsci11060241
APA StyleVitale, V., Bindi, F., Velloso Alvarez, A., de la Cuesta-Torrado, M., Sala, G., & Sgorbini, M. (2024). Transcutaneous Auricular Vagal Nerve Stimulation in Healthy Non-Sedated Horses: A Feasibility Study. Veterinary Sciences, 11(6), 241. https://doi.org/10.3390/vetsci11060241