Investigation of the Theragnostic Role of KIT Expression for the Treatment of Canine Mast Cell Tumors with Tyrosine Kinase Inhibitors

 ,
,  , ,
, ,  ,
, 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Overview and Case Inclusion Criteria
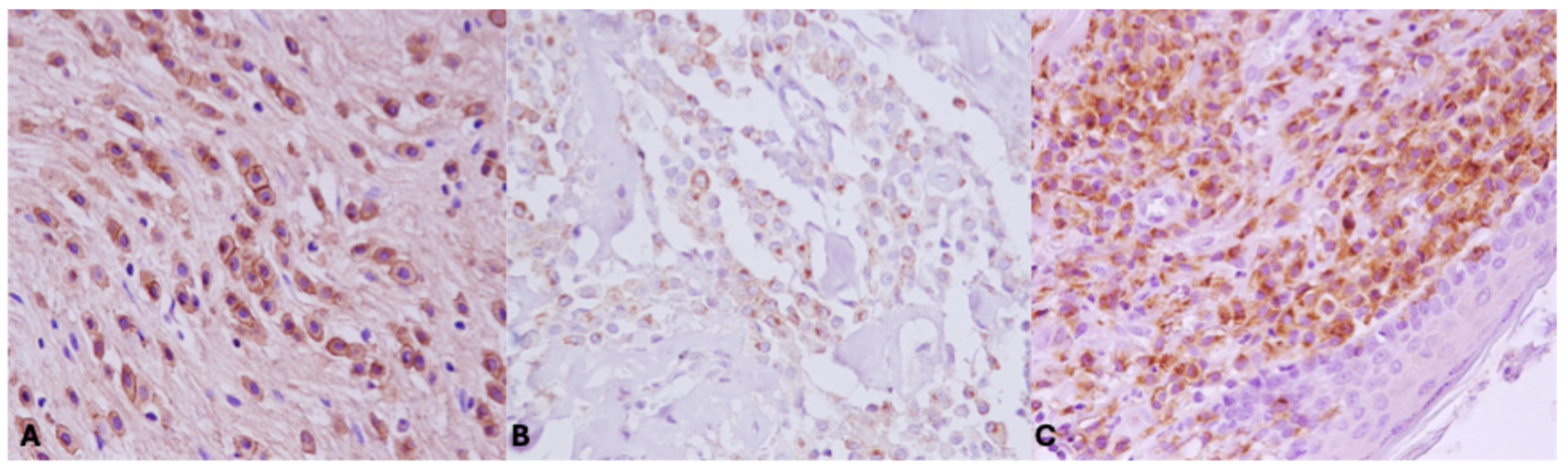
2.2. Immunohistochemistry and Evaluation of KIT Staining Patterns
2.3. Statistical Analysis
3. Results
3.1. Dogs’ Demographics and Clinical Background
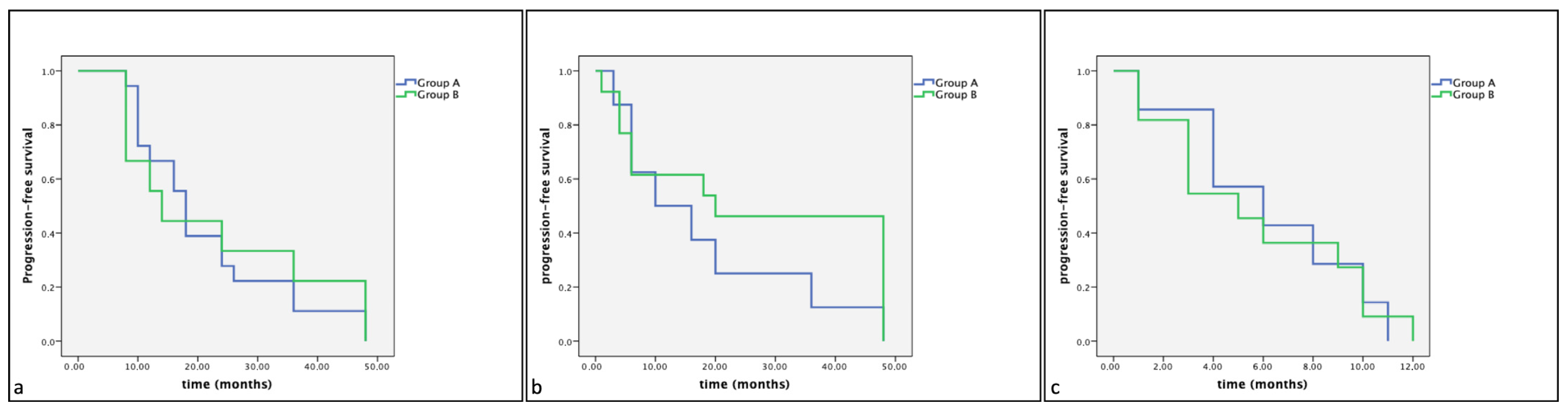
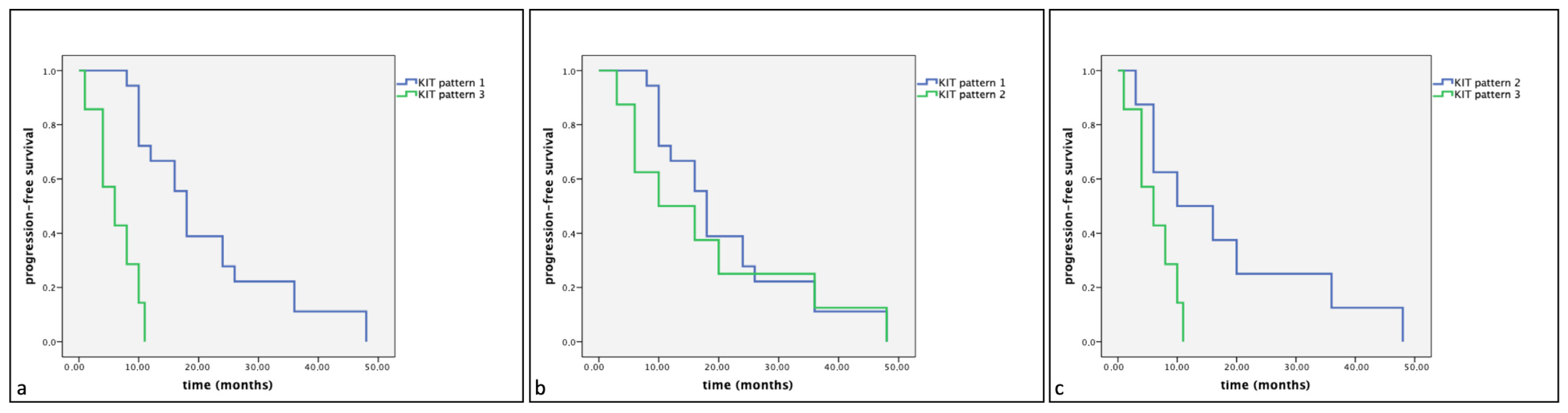
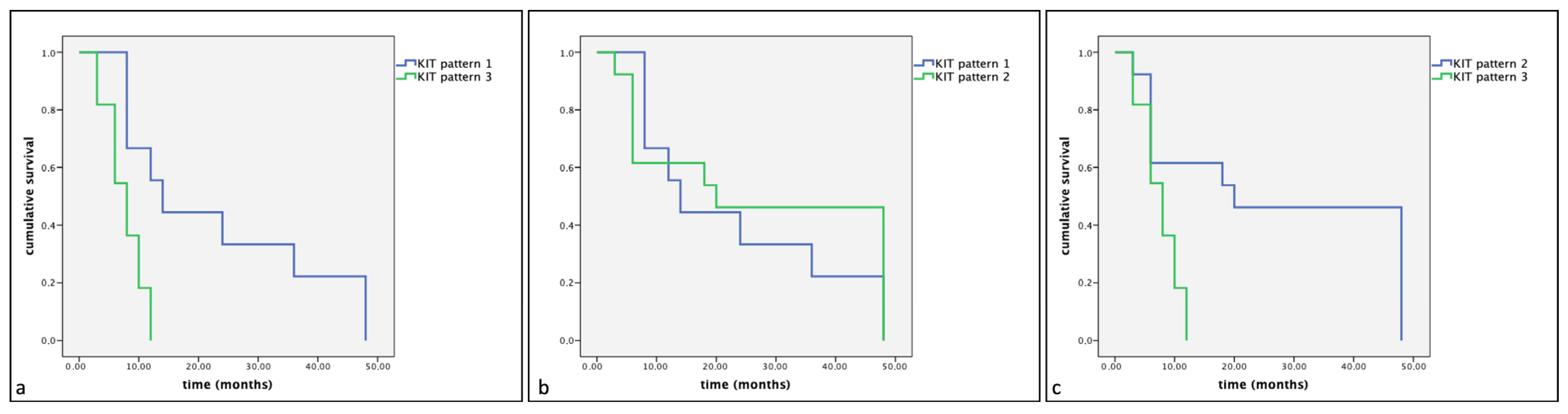
3.2. KIT Staining Patterns and Dogs’ Survival Status
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kiupel, M. Mast cell tumors. In Tumors in Domestic Animals, 5th ed.; Meuten, D.J., Ed.; Wiley-Blackwell: Ames, IA, USA, 2017; pp. 176–202. [Google Scholar] [CrossRef]
- Blackwood, L.; Murphy, S.; Buracco, P.; De Vos, J.P.; De Fornel-Thibaud, P.; Hirschberger, J.; Kessler, M.; Pastor, J.; Ponce, F.; Savary-Bataille, K.; et al. European consensus document on mast cell tumours in dogs and cats. Vet. Comp. Oncol. 2012, 10, 1–29. [Google Scholar] [CrossRef] [PubMed]
- Welle, M.M.; Bley, C.R.; Howard, J.; Rüfenacht, S. Canine mast cell tumours: A review of the pathogenesis, clinical features, pathology and treatment. Vet. Dermatol. 2008, 19, 321–339. [Google Scholar] [CrossRef] [PubMed]
- Webster, J.D.; Yuzbasiyan-Gurkan, V.; Miller, R.A.; Kaneene, J.B.; Kiupel, M. Cellular proliferation in canine cutaneous mast cell tumors: Associations with c-KIT and its role in prognostication. Vet. Pathol. 2007, 44, 298–308. [Google Scholar] [CrossRef] [PubMed]
- Webster, J.D.; Yuzbasiyan-Gurkan, V.; Kaneene, J.B.; Miller, R.; Resau, J.H.; Kiupel, M. The role of c-KIT in tumorigenesis: Evaluation in canine cutaneous mast cell tumors. Neoplasia 2006, 8, 104–111. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Letard, S.; Yang, Y.; Hanssens, K.; Palmérini, F.; Leventhal, P.S.; Guéry, S.; Moussy, A.; Kinet, J.P.; Hermine, O.; Dubreuil, P. Gain-of-function mutations in the extracellular domain of KIT are common in canine mast cell tumors. Mol. Cancer Res. 2008, 6, 1137–1145. [Google Scholar] [CrossRef] [PubMed]
- Kiupel, M.; Webster, J.D.; Kaneene, J.B.; Miller, R.; Yuzbasiyan-Gurkan, V. The use of KIT and tryptase expression patterns as prognostic tools for canine cutaneous mast cell tumors. Vet. Pathol. 2004, 41, 371–377, Erratum in Vet. Pathol. 2004, 41, 543. [Google Scholar] [CrossRef] [PubMed]
- Preziosi, R.; Morini, M.; Sarli, G. Expression of the KIT protein (CD117) in primary cutaneous mast cell tumors of the dog. J. Vet. Diagn. Investig. 2004, 16, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Morini, M.; Bettini, G.; Preziosi, R.; Mandrioli, L. C-kit gene product (CD117) immunoreactivity in canine and feline paraffin sections. J. Histochem. Cytochem. 2004, 52, 705–708. [Google Scholar] [CrossRef]
- da Costa, R.M.G. C-kit as a prognostic and therapeutic marker in canine cutaneous mast cell tumours: From laboratory to clinic. Vet. J. 2015, 205, 5–10. [Google Scholar] [CrossRef]
- De Nardi, A.B.; Dos Santos Horta, R.; Fonseca-Alves, C.E.; de Paiva, F.N.; Linhares, L.C.M.; Firmo, B.F.; Sueiro, F.A.R.; de Oliveira, K.D.; Lourenço, S.V.; Strefezzi, R.D.F.; et al. Diagnosis, Prognosis and Treatment of Canine Cutaneous and Subcutaneous Mast Cell Tumors. Cells 2022, 11, 618. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Oliveira, M.T.; Campos, M.; Lamego, L.; Magalhães, D.; Menezes, R.; Oliveira, R.; Patanita, F.; Ferreira, D.A. Canine and Feline Cutaneous Mast Cell Tumor: A Comprehensive Review of Treatments and Outcomes. Top. Companion Anim. Med. 2020, 41, 100472. [Google Scholar] [CrossRef] [PubMed]
- Govier, S.M. Principles of treatment for mast cell tumors. Clin. Tech. Small Anim. Pract. 2003, 18, 103–106. [Google Scholar] [CrossRef] [PubMed]
- Maeda, S. Second era of molecular-targeted cancer therapies in dogs. J. Vet. Med. Sci. 2023, 85, 790–798. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- London, C.A. Tyrosine kinase inhibitors in veterinary medicine. Top. Companion Anim. Med. 2009, 24, 106–112. [Google Scholar] [CrossRef] [PubMed]
- London, C.A.; Malpas, P.B.; Wood-Follis, S.L.; Boucher, J.F.; Rusk, A.W.; Rosenberg, M.P.; Henry, C.J.; Mitchener, K.L.; Klein, M.K.; Hintermeister, J.G.; et al. Multi-center, placebo-controlled, double-blind, randomized study of oral toceranib phosphate (SU11654), a receptor tyrosine kinase inhibitor, for the treatment of dogs with recurrent (either local or distant) mast cell tumor following surgical excision. Clin. Cancer Res. 2009, 15, 3856–3865. [Google Scholar] [CrossRef] [PubMed]
- Bertola, L.; Pellizzoni, B.; Giudice, C.; Grieco, V.; Ferrari, R.; Chiti, L.E.; Stefanello, D.; Manfredi, M.; De Zani, D.; Recordati, C. Tumor-associated macrophages and tumor-infiltrating lymphocytes in canine cutaneous and subcutaneous mast cell tumors. Vet. Pathol. 2024, 22, 3009858241244851. [Google Scholar] [CrossRef] [PubMed]
- De Biase, D.; Prisco, F.; Piegari, G.; Ilsami, A.; d’Aquino, I.; Baldassarre, V.; Zito Marino, F.; Franco, R.; Papparella, S.; Paciello, O. RNAScope in situ Hybridization as a Novel Technique for the Assessment of c-KIT mRNA Expression in Canine Mast Cell Tumor. Front. Vet. Sci. 2021, 8, 591961. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kiupel, M.; Webster, J.D.; Bailey, K.L.; Best, S.; DeLay, J.; Detrisac, C.J.; Fitzgerald, S.D.; Gamble, D.; Ginn, P.E.; Goldschmidt, M.H.; et al. Proposal of a 2-tier histologic grading system for canine cutaneous mast cell tumors to more accurately predict biological behavior. Vet. Pathol. 2011, 48, 147–155. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Webster, J.D.; Yuzbasiyan-Gurkan, V.; Thamm, D.H.; Hamilton, E.; Kiupel, M. Evaluation of prognostic markers for canine mast cell tumors treated with vinblastine and prednisone. BMC Vet. Res. 2008, 4, 32–40. [Google Scholar] [CrossRef]
- Horta, R.D.S.; Giuliano, A.; Lavalle, G.E.; Costa, M.D.P.; De Araujo, R.B.; Constantino-Casas, F.; Dobson, J.M. Clinical, histological, immunohistochemical and genetic factors associated with measurable response of high-risk canine mast cell tumours to tyrosine kinase inhibitors. Oncol. Lett. 2018, 15, 129–136. [Google Scholar] [CrossRef]
- Aupperle-Lellbach, H.; Kehl, A.; de Brot, S.; van der Weyden, L. Clinical Use of Molecular Biomarkers in Canine and Feline Oncology: Current and Future. Vet. Sci. 2024, 11, 199. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, E.; Tran, T.; Vranic, S.; Levy, A.; Bonfil, R.D. Role and significance of c-KIT receptor tyrosine kinase in cancer: A review. Bosn. J. Basic Med. Sci. 2022, 16, 683–698. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Coelho, Y.N.B.; Soldi, L.R.; Silva, P.H.R.D.; Mesquita, C.M.; Paranhos, L.R.; Santos, T.R.D.; Silva, M.J.B. Tyrosine kinase inhibitors as an alternative treatment in canine mast cell tumor. Front. Vet. Sci. 2023, 10, 1188795. [Google Scholar] [CrossRef] [PubMed]
- Halsey, C.H.; Gustafson, D.L.; Rose, B.J.; Wolf-Ringwall, A.; Burnett, R.C.; Duval, D.L.; Avery, A.C.; Thamm, D.H. Development of an in vitro model of acquired resistance to toceranib phosphate (Palladia®) in canine mast cell tumor. BMC Vet. Res. 2014, 6, 105–117. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Verstovsek, S.; Akin, C.; Manshouri, T.; Quintàs-Cardama, A.; Huynh, L.; Manley, P.; Tefferi, A.; Cortes, J.; Giles, F.J.; Kantarjian, H. Effects of AMN107, a novel aminopyrimidine tyrosine kinase inhibitor, on human mast cells bearing wild-type or mutated codon 816 c-kit. Leuk. Res. 2006, 30, 1365–1370. [Google Scholar] [CrossRef]
- Longley, B.J.; Reguera, M.J.; Ma, Y. Classes of c-KIT activating mutations: Proposed mechanisms of action and implications for disease classification and therapy. Leuk. Res. 2001, 25, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Nakano, Y.; Kobayashi, M.; Bonkobara, M.; Takanosu, M. Identification of a secondary mutation in the KIT kinase domain correlated with imatinib-resistance in a canine mast cell tumor. Vet. Immunol. Immunopathol. 2017, 188, 84–88. [Google Scholar] [CrossRef]
- Kobayashi, M.; Kuroki, S.; Tanaka, Y.; Moriya, Y.; Kozutumi, Y.; Uehara, Y.; Ono, K.; Tamura, K.; Washizu, T.; Bonkobara, M. Molecular changes associated with the development of resistance to imatinib in an imatinib-sensitive canine neoplastic mast cell line carrying a KIT c.1523A>T mutation. Eur. J. Haematol. 2015, 95, 524–531. [Google Scholar] [CrossRef]
- Gentilini, F.; Turba, M.E.; Dally, C.; Takanosu, M.; Kurita, S.; Bonkobara, M. The secondary KIT mutation p.Ala510Val in a cutaneous mast cell tumour carrying the activating mutation p.Asn508Ile confers resistance to masitinib in dogs. BMC Vet. Res. 2020, 16, 64–73. [Google Scholar] [CrossRef]
- Gil da Costa, R.M.; Matos, E.; Rema, A.; Lopes, C.; Pires, M.A.; Gärtner, F. CD117 immunoexpression in canine mast cell tumours: Correlations with pathological variables and proliferation markers. BMC Vet. Res. 2007, 21, 19–26. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tamborini, E.; Bonadiman, L.; Greco, A.; Albertini, V.; Negri, T.; Gronchi, A.; Bertulli, R.; Maurizio, C.; Paolo, G.C.; Marco, A.P.; et al. A new mutation in the KIT ATP pocket causes acquired resistance to imatinib in a gastrointestinal stromal tumor patient. Gastroenterology 2004, 127, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Tamborini, E.; Pricl, S.; Negri, T.; Lagonigro, M.S.; Miselli, F.; Greco, A.; Gronchi, A.; Casali, P.G.; Ferrone, M.; Fermeglia, M.; et al. Functional analyses and molecular modeling of two c-Kit mutations responsible for imatinib secondary resistance in GIST patients. Oncogene 2006, 25, 6140–6146. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.L.; Trent, J.C.; Wu, E.F.; Fuller, G.N.; Ramdas, L.; Zhang, W.; Austin, K.R.; Victor, G.P.; Caroline, O.O.; Kelly, K.H.; et al. A missense mutation in KIT kinase domain 1 correlates with imatinib resistance in gastrointestinal stromal tumors. Cancer Res. 2004, 64, 5913–5919. [Google Scholar] [CrossRef] [PubMed]
- Wardelmann, E.; Thomas, N.; Merkelbach-Bruse, S.; Pauls, K.; Speidel, N.; Büttner, R.; Bihl, H.; Leutner, C.C.; Heinicke, T.; Hohenberger, P. Acquired resistance to imatinib in gastrointestinal stromal tumours caused by multiple KIT mutations. Lancet Oncol. 2005, 6, 249–251. [Google Scholar] [CrossRef] [PubMed]
- Sledge, D.G.; Webster, J.; Kiupel, M. Canine cutaneous mast cell tumors: A combined clinical and pathologic approach to diagnosis, prognosis, and treatment selection. Vet. J. 2016, 215, 43–54. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cases Characteristics | Value |
|---|---|
| Total participants | 66 |
| Median age at presentation (years) | 8 (range 1–14) |
| Gender | |
| Female spayed | 17 |
| Female intact | 17 |
| Male neutered | 10 |
| Male intact | 22 |
| Breed | |
| Mixed breeds | 29 |
| Labrador retriever | 10 |
| Sharpei | 3 |
| Boxer | 3 |
| Setter | 5 |
| Maltese | 3 |
| Other breeds | 13 |
| Histologic grade (by Kiupel) | |
| Low | 34 |
| High | 22 |
| Number of metastatic diseases | |
| Group A (TKI) | 3 |
| Group B (Surgery alone) | 4 |
| Number of recurrences | |
| Group A (TKI) | 1 |
| Group B (Surgery alone) | 3 |
| Variable | KIT Staining Pattern 1 | KIT Staining Pattern 2 | KIT Staining Pattern 3 | Value |
|---|---|---|---|---|
| Immunohistochemistry | 27 | 21 | 18 | 66 |
| Grade | ||||
| High grade | 6 | 7 | 9 | 22 |
| Low grade | 21 | 14 | 9 | 44 |
| Treatment | ||||
| Group A (Toceranib phosphate) | 2 | 5 | 4 | 11 |
| Group A (Masitinib mesylate) | 7 | 8 | 7 | 22 |
| Group B (Surgery alone) | 18 | 8 | 7 | 33 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Biase, D.; De Leo, M.; Piegari, G.; d’Aquino, I.; Di Napoli, E.; Mercogliano, C.; Calabria, A.; Pula, A.; Navas, L.; Russo, V.; et al. Investigation of the Theragnostic Role of KIT Expression for the Treatment of Canine Mast Cell Tumors with Tyrosine Kinase Inhibitors. Vet. Sci. 2024, 11, 492. https://doi.org/10.3390/vetsci11100492
De Biase D, De Leo M, Piegari G, d’Aquino I, Di Napoli E, Mercogliano C, Calabria A, Pula A, Navas L, Russo V, et al. Investigation of the Theragnostic Role of KIT Expression for the Treatment of Canine Mast Cell Tumors with Tyrosine Kinase Inhibitors. Veterinary Sciences. 2024; 11(10):492. https://doi.org/10.3390/vetsci11100492
Chicago/Turabian StyleDe Biase, Davide, Marcello De Leo, Giuseppe Piegari, Ilaria d’Aquino, Evaristo Di Napoli, Carmela Mercogliano, Alfonso Calabria, Agata Pula, Luigi Navas, Valeria Russo, and et al. 2024. "Investigation of the Theragnostic Role of KIT Expression for the Treatment of Canine Mast Cell Tumors with Tyrosine Kinase Inhibitors" Veterinary Sciences 11, no. 10: 492. https://doi.org/10.3390/vetsci11100492
APA StyleDe Biase, D., De Leo, M., Piegari, G., d’Aquino, I., Di Napoli, E., Mercogliano, C., Calabria, A., Pula, A., Navas, L., Russo, V., & Paciello, O. (2024). Investigation of the Theragnostic Role of KIT Expression for the Treatment of Canine Mast Cell Tumors with Tyrosine Kinase Inhibitors. Veterinary Sciences, 11(10), 492. https://doi.org/10.3390/vetsci11100492