Data Quality: A Negotiator between Paper-Based and Digital Records in Pakistan’s TB Control Program

 ,
,  ,
,
Abstract
1. Introduction
2. Methods
2.1. Sample Description
2.2. Data Collection
2.3. Data Quality Assessment Method
2.4. Data Analysis
2.5. Ethical Considerations
2.6. Study Findings
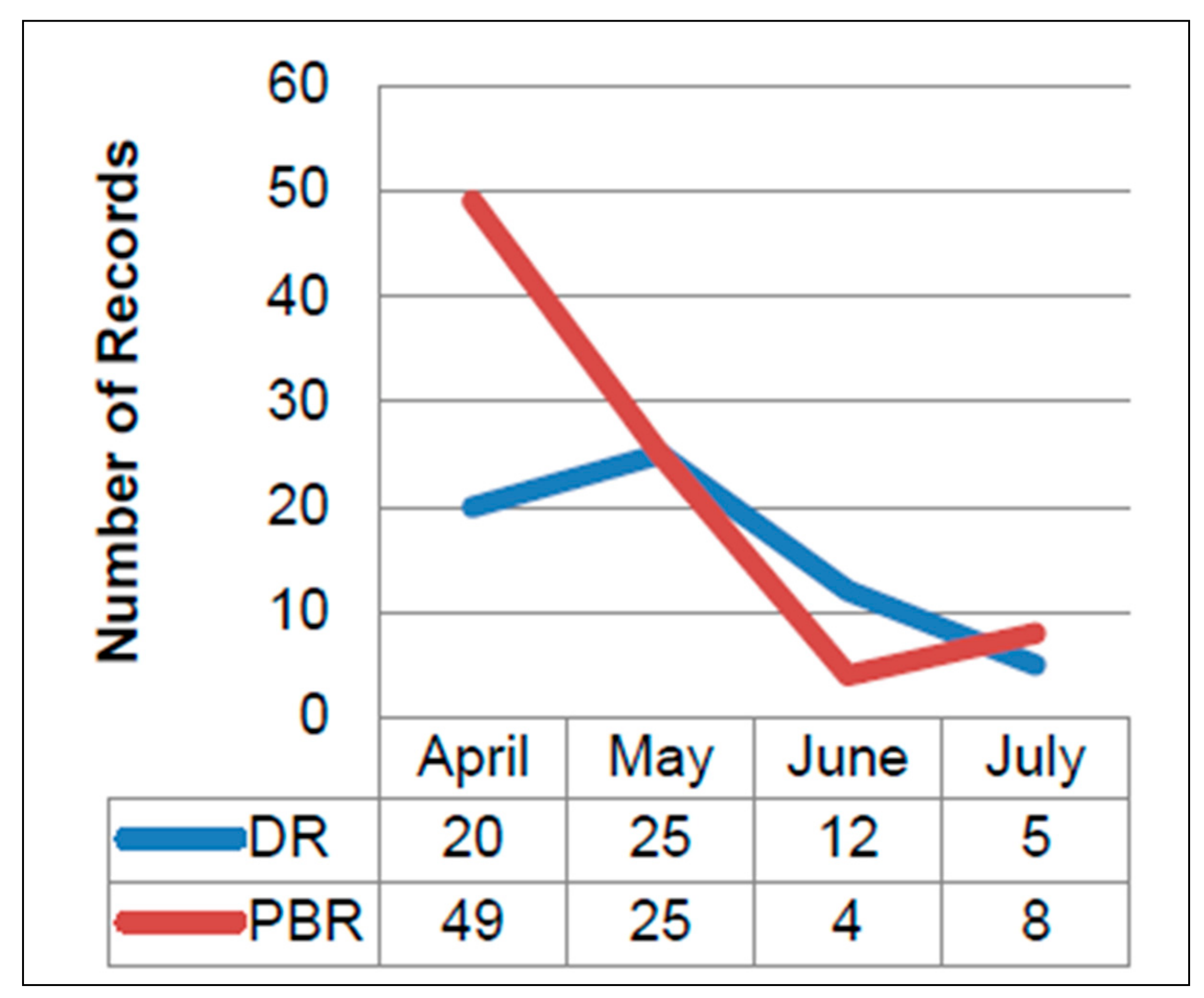
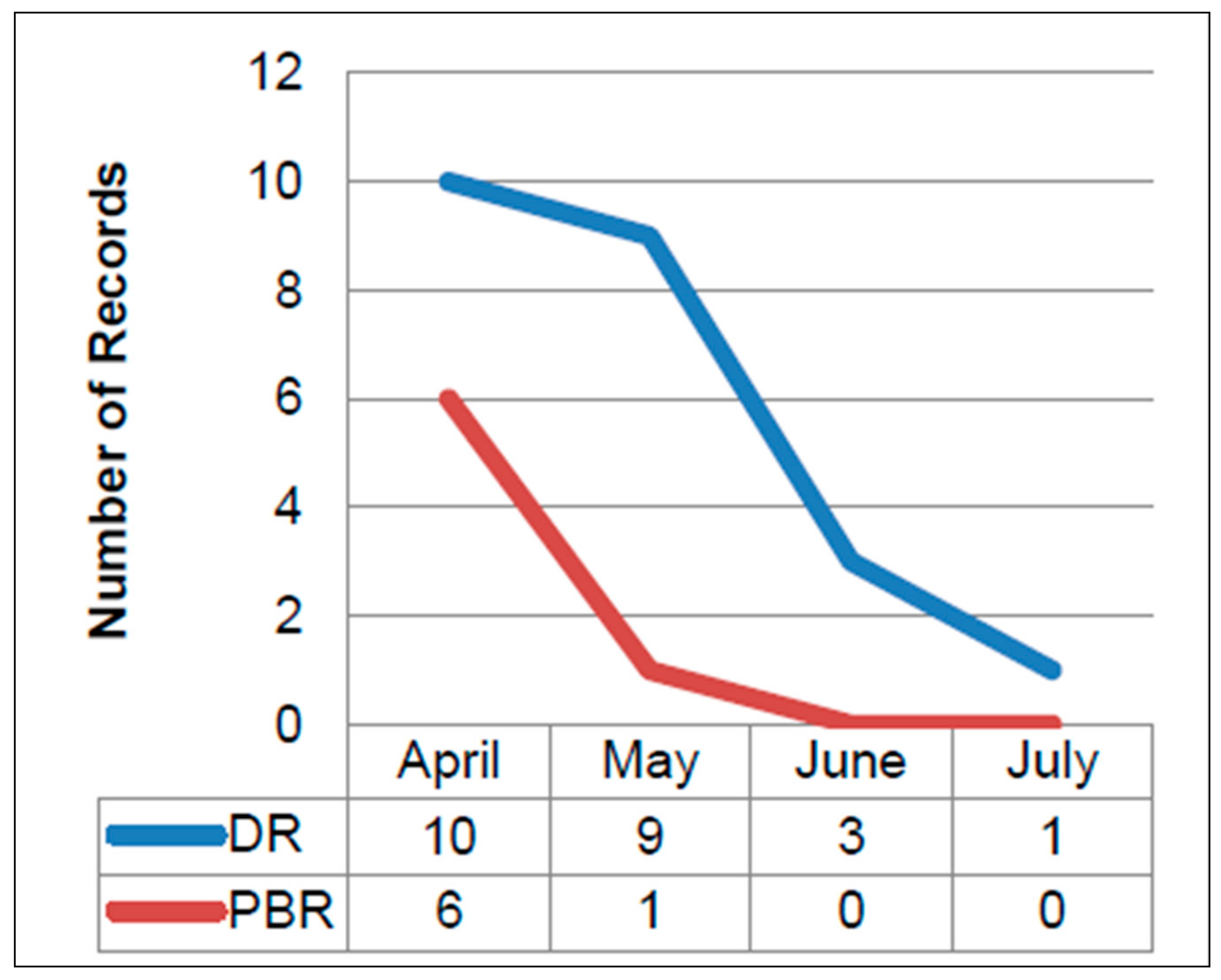
2.6.1. Comparison of the Paper-Based and Digital Records
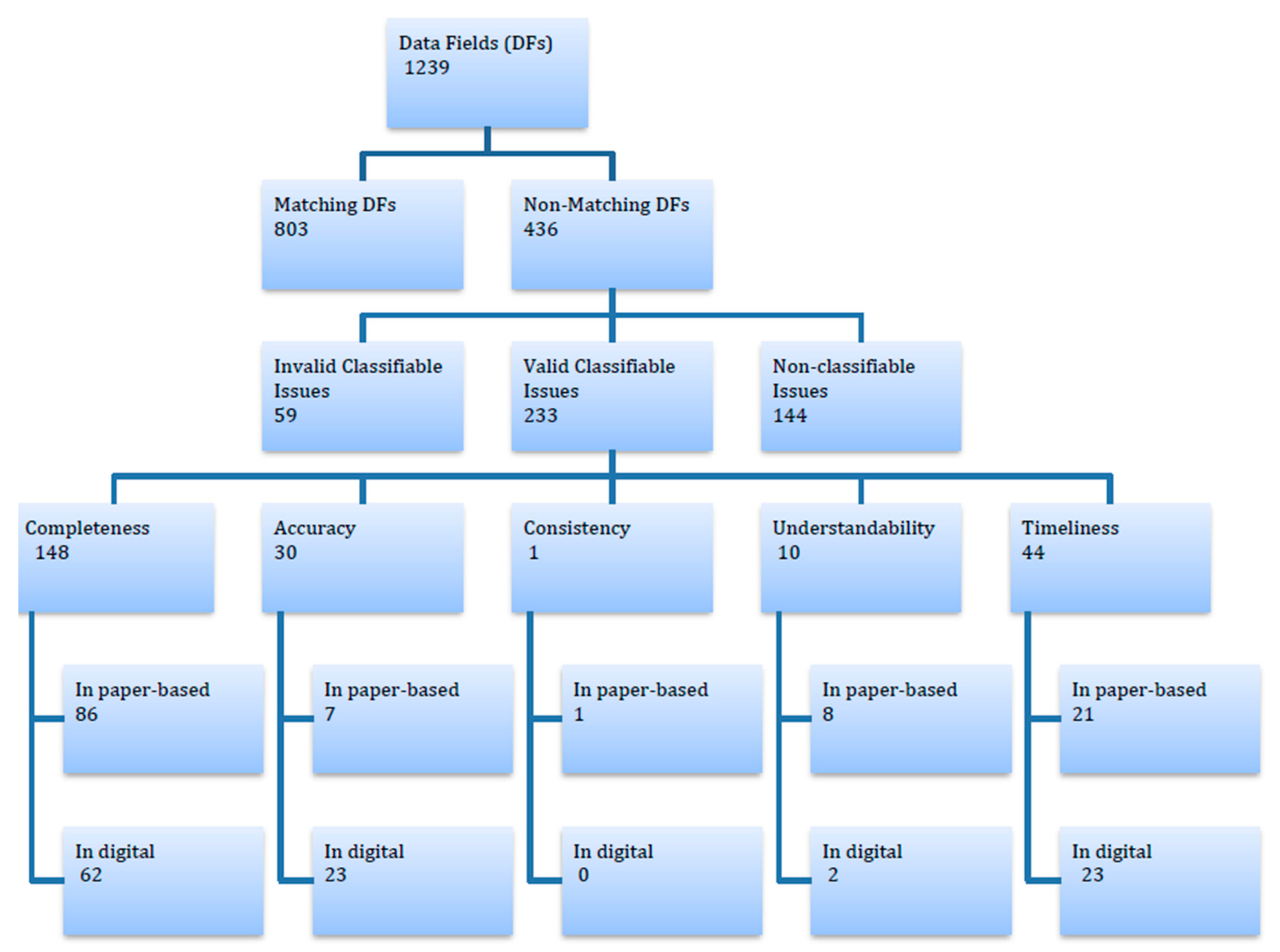
2.6.2. Analysis of Non-Classifiable Issues
2.6.3. Analysis of Classifiable Issues
Classifier 1: Completeness
Classifier 2: Accuracy
Classifier 3: Consistency
Classifier 4: Understandability
Classifier 5: Timeliness
3. Discussion
3.1. User Adoption and Acceptance Issues of Digital Data Collection
3.2. Novel Contribution, Replicability and Generalizability of the Work beyond the Six Study Locales
3.3. Follow-Up on Current Work
3.4. Research Implications
4. Strengths and Limitations of the Study
- The scope of study included a comprehensive review and comparison of paper-based and digital data to identify quality issues and to categorize the identified issues into classifiable and non-classifiable ones.
- The strength of the present work is its usefulness in developing a case for implementation agencies for expanding their digital health initiatives, particularly for data collection.
- As a result of patients’ information confidentiality concerns and provisions (researchers had no access to or contact with the patients), the researchers were unable to categorize non-classifiable issues (those data that would have required contacting the patient to verify them), which can be considered as a limitation of the current study. Nonetheless, we demonstrated the need for putting in place an adequate data quality improvement strategy so that reliability and sanity of healthcare data can be fully achieved.
- With the limited human and other resources in the enrolled clinics, running two systems (paper-based and digital) in parallel during the study period might have caused frustration among clinic staff. Overburdening the data collection workflows of the involved staff might have also been a reason for the relatively low (50.4%) overall use of MAPPLE in data collection. With sufficient incentives in place and a complete switch to a digital format (following any necessary tweaking and optimization of MAPPLE), digital data collection rates can greatly improve in the future.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- St-Maurice, J.; Burns, C.M. A method for developing data quality measures and metrics for primary health care. In Proceedings of the International Symposium on Human Factors and Ergonomics in Health Care: Improving the Outcomes; Sage Publications: New Delhi, India, 2016. [Google Scholar] [CrossRef]
- Ndabarora, E.; Chipps, J.A.; Uys, L. Systematic review of health data quality management and best practices at community and district levels in LMIC. Inf. Dev. 2013, 30, 1–18. [Google Scholar] [CrossRef]
- Kerr, K.A.; Norris, T.; Stockdale, R. The strategic management of data quality in healthcare. Health Inform. J. 2008, 14, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Haux, R. Health information systems past, present, future. Int. J. Med. Inform. 2006, 75, 268–281. [Google Scholar] [CrossRef] [PubMed]
- Walker, R. Health information and public health. Health Inf. Manag. J. 2008, 37, 4–5. [Google Scholar] [CrossRef] [PubMed]
- Even, A.; Shankaranarayanan, G. Dual assessment of data quality in customer databases. ACM J. Data Inf. Qual. 2009, 1, 1–29. [Google Scholar] [CrossRef]
- Redman, T.C. Data: An unfolding quality disaster. DM Rev. 2004, 14, 21–23. [Google Scholar]
- Cappiello, C.; Francalanci, C.; Pernici, B. Data quality assessment from the user’s perspective. In Proceedings of the 2004 International Workshop on Information Quality in Information Systems, Paris, France, 18 June 2004; pp. 68–73. [Google Scholar] [CrossRef]
- Madnick, S.E.; Wang, R.Y.; Lee, Y.W.; Zhu, H. Overview and framework for data and information quality research. ACM J. Data Inf. Qual. 2009, 1, 1–22. [Google Scholar] [CrossRef]
- Glowalla, P.; Sunyaev, A. Process-driven data quality management: A critical review on the application of process modeling languages. ACM J. Data Inf. Qual. 2014, 5, 1–30. [Google Scholar] [CrossRef]
- Agyeman-Duah, J.N.A.; Theurer, A.; Munthali, C.; Alide, N.; Neuhann, F. Understanding the barriers to setting up a healthcare quality improvement process in resource-limited settings: A situational analysis at the medical department of Kamuzu Central Hospital in Lilongwe, Malawi. BMC Health Serv. Res. 2014, 14, 1. [Google Scholar] [CrossRef] [PubMed]
- Ogunsola, O.O.; Aburogbola, F.; Olajide, O.; Ladi-Akinyemi, B. Clinical documentation and doctor: Is it a challenge in HIV care? Experience of four new comprehensive HIV sites in Oyo State, Nigeria. Adv. Trop. Med. Public Health Int. 2015, 5, 77–89. [Google Scholar]
- Lium, J.T.; Tjora, A.; Faxvaag, A. No paper, but the same routines: A qualitative exploration of experiences in two Norwegian hospitals deprived of the paper based medical records. BMC Med. Inform. Decis. Mak. 2008, 8, 2. [Google Scholar] [CrossRef] [PubMed]
- Pourasghar, F.; Malekafzali, H.; Koch, S.; Fors, U. Factors influencing the quality of medical documentation when a paper-based medical records system is replaced with an electronic medical records system: An Iranian case study. Int. J. Technol. Assess. Health Care 2008, 24, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Wager, K.A.; Lee, F.W.; White, A.W.; Ward, D.M.; Ornstein, S.M. Impact of an electronic medical record system on community-based primary care practices. J. Am. Board Fam. Pract. 2000, 13, 338–348. [Google Scholar] [PubMed]
- Makoul, G.; Curry, R.H.; Tang, P.C. The use of electronic medical records: Communication patterns in outpatient encounters. J. Am. Med. Inf. Assoc. 2001, 8, 610–615. [Google Scholar] [CrossRef]
- Ammenwerth, E.; Eichstadter, R.; Haux, R.; Pohl, U.; Rebel, S.; Ziegler, S. A randomized evaluation of a computer-based nursing documentation system. Method Inf. Med. 2001, 40, 61–68. [Google Scholar]
- Ozair, F.F.; Jamshed, N.; Sharma, A.; Aggarwal, P. Ethical issues in electronic health records: A general overview. Perspect. Clin. Res. 2015, 6, 73–76. [Google Scholar] [PubMed]
- Van Velthoven, M.H.; Car, J.; Zhang, Y.; Marušić, A. mHealth series: New ideas for mHealth data collection implementation in low– and middle–income countries. J. Glob. Health 2013, 3, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Sebastian-Coleman, L. Measuring Data Quality for Ongoing Improvement: A Data Quality Assessment Framework; Morgan Kaufmann Elsevier: Waltham, MA, USA, 2013. [Google Scholar]
- Pringle, M.; Wilson, T.; Grol, R. Measuring ‘goodness’ in individuals and healthcare systems. BMJ 2002, 325, 704–707. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.M.; Anjum, N.; Boulos, M.N.K.; Ishaq, M.; Aamir, J.; Haider, G.R. Measuring management’s perspective of data quality in Pakistan’s tuberculosis control programme: A test-based approach to identify data quality dimensions. BMC Res. Notes 2018, 11, 40. [Google Scholar] [CrossRef] [PubMed]
- Bovee, M.; Srivastava, R.; Mak, B. A conceptual framework and belief-function approach to assessing overall information quality. Int. J. Intell. Syst. 2001, 18, 51–74. [Google Scholar] [CrossRef]
- DAMA. The Six Primary Dimensions for Data Quality Assessment: Defining Data Quality Dimensions. DAMA UK Working Group on Data Quality Dimensions. Available online: https://www.whitepapers.em360tech.com/wp-content/files_mf/1407250286DAMAUKDQ DimensionsWhitePaperR37.pdf (accessed on 5 May 2016).
- Almutiry, O.; Wills, G.; Alwabel, A.; Crowder, R.; Walters, R. Toward a framework for data quality in cloud-based health information system. In Proceedings of the International Conference on Information Society (i-Society 2013), Toronto, ON, Canada, 24–26 June 2013; Available online: http://ieeexplore.ieee.org/document/6636362/ (accessed on 3 July 2016).
- Orfanidis, L.; Bamidis, P.D.; Eaglestone, B. Data quality issues in Electronic Health Records: An adaptation framework for the Greek health system. Health Inform. J. 2004, 10, 23–36. [Google Scholar] [CrossRef]
- Chaudhry, B.; Wang, J.; Wu, S.; Maglione, M.; Mojica, W.; Roth, E.; Morton, S.C.; Shekelle, P.G. Systematic review: Impact of health information technology on quality, efficacy, and costs of medical care. Ann. Intern. Med. 2006, 144, 742–752. [Google Scholar] [CrossRef] [PubMed]
- Kalogriopoulos, N.A.; Baran, J.; Nimunkar, A.J.; Webster, J.G. Electronic medical record systems for developing countries: Review. In Proceedings of the Annual International Conference of IEEE in Engineering in Medicine and Biology Society, Mineapolis, MN, USA, 3–6 September 2009; pp. 1730–1733. [Google Scholar]
- Kahn, M.G.; Raebel, M.A.; Glanz, J.M.; Riedlinger, K.; Steiner, J.F. A pragmatic framework for single-site and multisite data quality assessment in electronic health record-based clinical research. Med. Care 2012, 50, S21–S29. [Google Scholar] [CrossRef] [PubMed]
- Divorski, S.; Scheirer, M.A. Improving data quality for performance measures: Results from a GAO study of verification and validation. Eval. Program Plan. 2001, 24, 83–94. [Google Scholar] [CrossRef]
- Chen, H.; Hailey, D.; Wang, N.; Yu, P. A review of data quality assessment methods for public health information systems. Int. J. Environ. Res. Public Health 2014, 11, 5170–5207. [Google Scholar] [CrossRef] [PubMed]
- Tsai, J.; Bond, G. A comparison of electronic records to paper records in mental health centers. Int. J. Qual. Health Care 2008, 20, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Ward, M.; Brandsema, P.; van Straten, E.; Bosman, A. Electronic reporting improves timeliness and completeness of infectious disease notification, The Netherlands, 2003. Euro Surveill. 2005, 10, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Shovlin, A.; Ghen, M.; Simpson, P.; Mehta, K. Challenges facing medical data digitization in low-resource contexts. In Proceedings of the IEEE 2013 Global Humantarian Technology Conference, San Jose, CA, USA, 2 July 2013; pp. 365–371. [Google Scholar]
- Bram, J.T.; Warwick-Clark, B.; Obeysekare, E.; Mehta, K. Utilization and monetization of healthcare data in developing countries. Big Data 2015, 3, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Duhm, J.; Fleischmann, R.; Schmidt, S.; Hupperts, H.; Brandt, S.A. Mobile electronic medical records promote workflow: Physicians’ perspective from a survey. JMIR MHealth UHealth 2016, 4, e70. [Google Scholar] [CrossRef] [PubMed]
- Despont-Gros, C.; Rutschmann, O.; Geissbuhler, A.; Lovis, C. Acceptance and cognitive load in a clinical setting of a novel device allowing natural real-time data acquisition. Int. J. Med. Inform. 2007, 76, 850–855. [Google Scholar] [CrossRef] [PubMed]
- Bassi, J.; Lau, F.; Lesperance, M. Perceived impact of electronic medical records in physician office practices: A review of survey-based research. Interact. J. Med. Res. 2012, 1, e3. [Google Scholar] [CrossRef] [PubMed]
- Wand, Y.; Wang, R.Y. Anchoring data quality dimensions in ontological foundations. Commun. ACM 1996, 39, 86–89. [Google Scholar] [CrossRef]
- Wang, R.Y.; Strong, D.M. Beyond accuracy: What data quality means to data consumers. J. Manag. Inf. Syst. 1996, 12, 5–33. [Google Scholar] [CrossRef]
- National Health Service. Executive Summary of the First National Data Quality Review. Quality Information Committee of the National Health Service. Available online: https://www.england.nhs.uk/wp-content/uploads/2013/04/1ndqr-exec-sum.pdf (accessed on 25 February 2017).
- Nishtar, S. The Gateway Paper on Health System in Pakistan—A Way Forward. Pakistan’s Health Policy Forum and Heartfile, Islamabad, Pakistan. Available online: http://www.heartfile.org/pdf/phpf-GWP.pdf (accessed on 25 February 2017).
- Shaikh, B.T. Private sector in health care delivery: A reality and a challenge in Pakistan. J. Ayub Med. Coll. Abbottabad 2015, 27, 496–498. [Google Scholar] [PubMed]
- Tweya, H.; Feldacker, C.; Gadabu, O.J.; Ng’ambi, W.; Mumba, S.L.; Phiri, D.; Kamvazine, L.; Mwakilama, S.; Kanyerere, H.; Keiser, O.; et al. Developing a point-f-care electronic medical record system for TB/HIV co-infected patients: Experiences from Lighthouse Trust, Lilongwe, Malawi. BMC Res. Notes 2016, 9, 146. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category of Data | Data Fields | Type of Data | |||
|---|---|---|---|---|---|
| Number | Text | Alpha-Numeric | Selection | ||
| Profile | 17 | 5 | 9 | 1 | 2 |
| Clinical | 7 | 3 | 1 | − | 3 |
| Diagnostic | 6 | 4 | 1 | − | 1 |
| Category of Data | Comparable Data Fields |
|---|---|
| Profile | 12 |
| Clinical | 6 |
| Diagnostic | 3 |
| Total | 21 |
| Data Category | Data Field | # of Issues | Total (n = 59) | Data Quality Dimension |
|---|---|---|---|---|
| Patient Profile | Father/Spouse Name | 25 | 37 | Completeness (missing responses) |
| Type of Referral | 12 | |||
| Clinical | Treatment Start Date | 5 | 22 | |
| Disease Category | 3 | |||
| Type of Patient | 12 | |||
| Disease Site | 2 |
| Month | Total Comparable Records | No. of Issues in DR | No. of Issues in DR (Design Concern) | No. of Valid Issues in DR | No. of Issues Per DR | No. of Issues in PBR | No. of Issues Per PBR | Test |
|---|---|---|---|---|---|---|---|---|
| n | x | x1 | xv = x − x1 | d = xv/n | y | p = y/n | p-Value | |
| April | 31 | 85 | 40 | 45 | 1.5 | 67 | 2.2 | 0.0287 |
| May | 10 | 50 | 8 | 42 | 4.2 | 34 | 3.4 | 0.3124 |
| June | 10 | 24 | 7 | 17 | 1.7 | 11 | 1.1 | 0.2411 |
| July | 8 | 10 | 4 | 6 | 0.7 | 11 | 1.4 | 0.2138 |
| Total | 59 | 169 | 59 | 110 | 1.9 | 123 | 2.1 | 0.3711 |
| Name of Data Fields | April | May | June | July | Total |
|---|---|---|---|---|---|
| Name | 0 | 0 | 2 | 0 | 2 |
| Age | 25 | 12 | 8 | 2 | 47 |
| Weight | 12 | 2 | 6 | 2 | 22 |
| Patient Identifier Code | 3 | 9 | 4 | 4 | 20 |
| National Identity Number | 6 | 3 | 1 | 1 | 11 |
| Address | 1 | 0 | 0 | 1 | 2 |
| Phone Number | 6 | 1 | 1 | 1 | 9 |
| Father/Spouse Name | 0 | 2 | 0 | 0 | 2 |
| Supporter Name | 1 | 0 | 0 | 0 | 1 |
| Type of Referral | 6 | 11 | 3 | 2 | 22 |
| Lab Number | 2 | 0 | 1 | 0 | 3 |
| Disease Site | 0 | 2 | 0 | 0 | 2 |
| Lab Result | 1 | 0 | 0 | 0 | 1 |
| Total | 63 | 42 | 26 | 13 | 144 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ali, S.M.; Naureen, F.; Noor, A.; Kamel Boulos, M.N.; Aamir, J.; Ishaq, M.; Anjum, N.; Ainsworth, J.; Rashid, A.; Majidulla, A.; et al. Data Quality: A Negotiator between Paper-Based and Digital Records in Pakistan’s TB Control Program. Data 2018, 3, 27. https://doi.org/10.3390/data3030027
Ali SM, Naureen F, Noor A, Kamel Boulos MN, Aamir J, Ishaq M, Anjum N, Ainsworth J, Rashid A, Majidulla A, et al. Data Quality: A Negotiator between Paper-Based and Digital Records in Pakistan’s TB Control Program. Data. 2018; 3(3):27. https://doi.org/10.3390/data3030027
Chicago/Turabian StyleAli, Syed Mustafa, Farah Naureen, Arif Noor, Maged N. Kamel Boulos, Javariya Aamir, Muhammad Ishaq, Naveed Anjum, John Ainsworth, Aamna Rashid, Arman Majidulla, and et al. 2018. "Data Quality: A Negotiator between Paper-Based and Digital Records in Pakistan’s TB Control Program" Data 3, no. 3: 27. https://doi.org/10.3390/data3030027
APA StyleAli, S. M., Naureen, F., Noor, A., Kamel Boulos, M. N., Aamir, J., Ishaq, M., Anjum, N., Ainsworth, J., Rashid, A., Majidulla, A., & Fatima, I. (2018). Data Quality: A Negotiator between Paper-Based and Digital Records in Pakistan’s TB Control Program. Data, 3(3), 27. https://doi.org/10.3390/data3030027