
Ventricular and Atrial Pressure—Volume Loops: Analysis of the Effects Induced by Right Centrifugal Pump Assistance

 , and
, and
Abstract
:
1. Introduction
- ✓
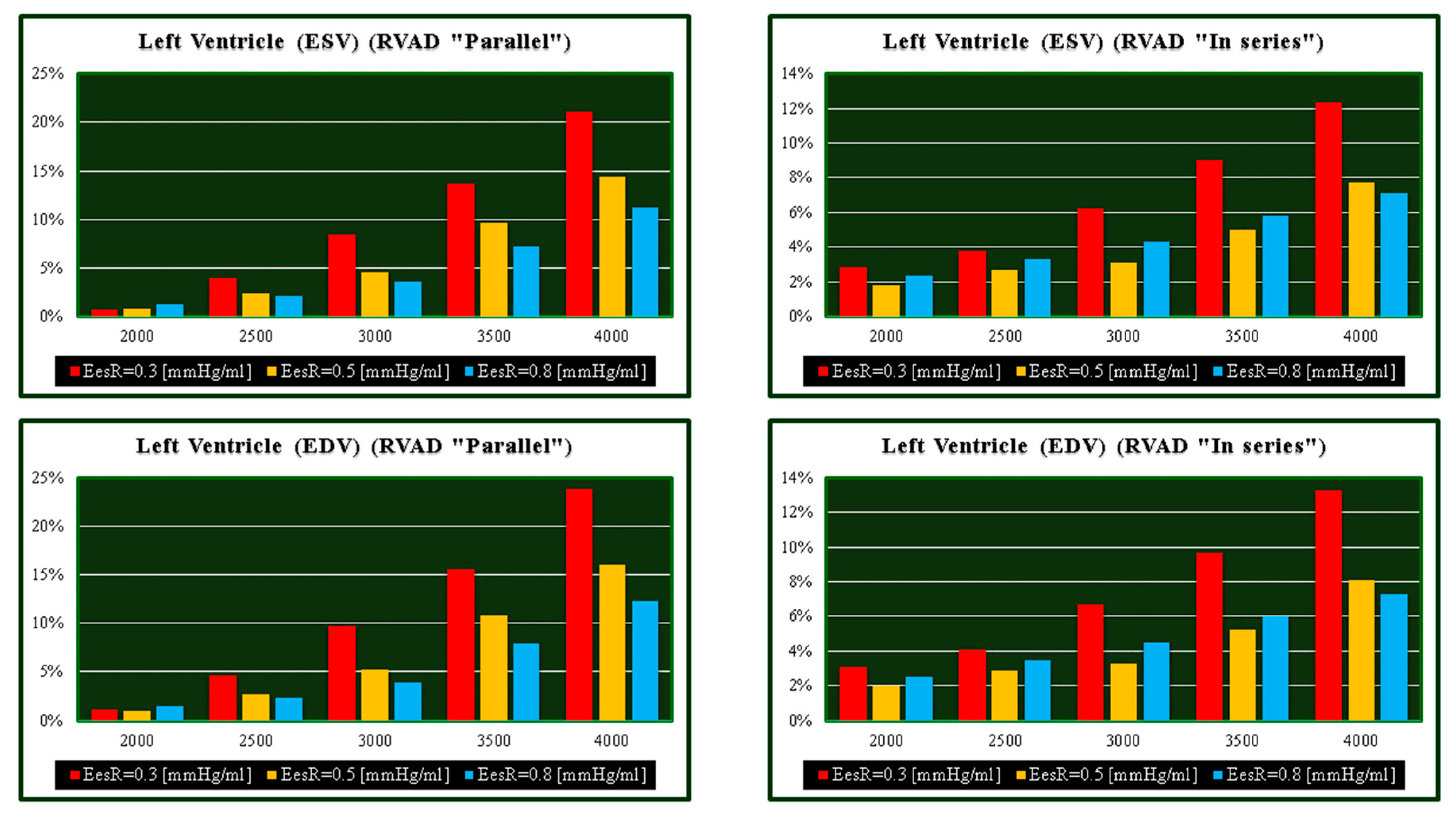
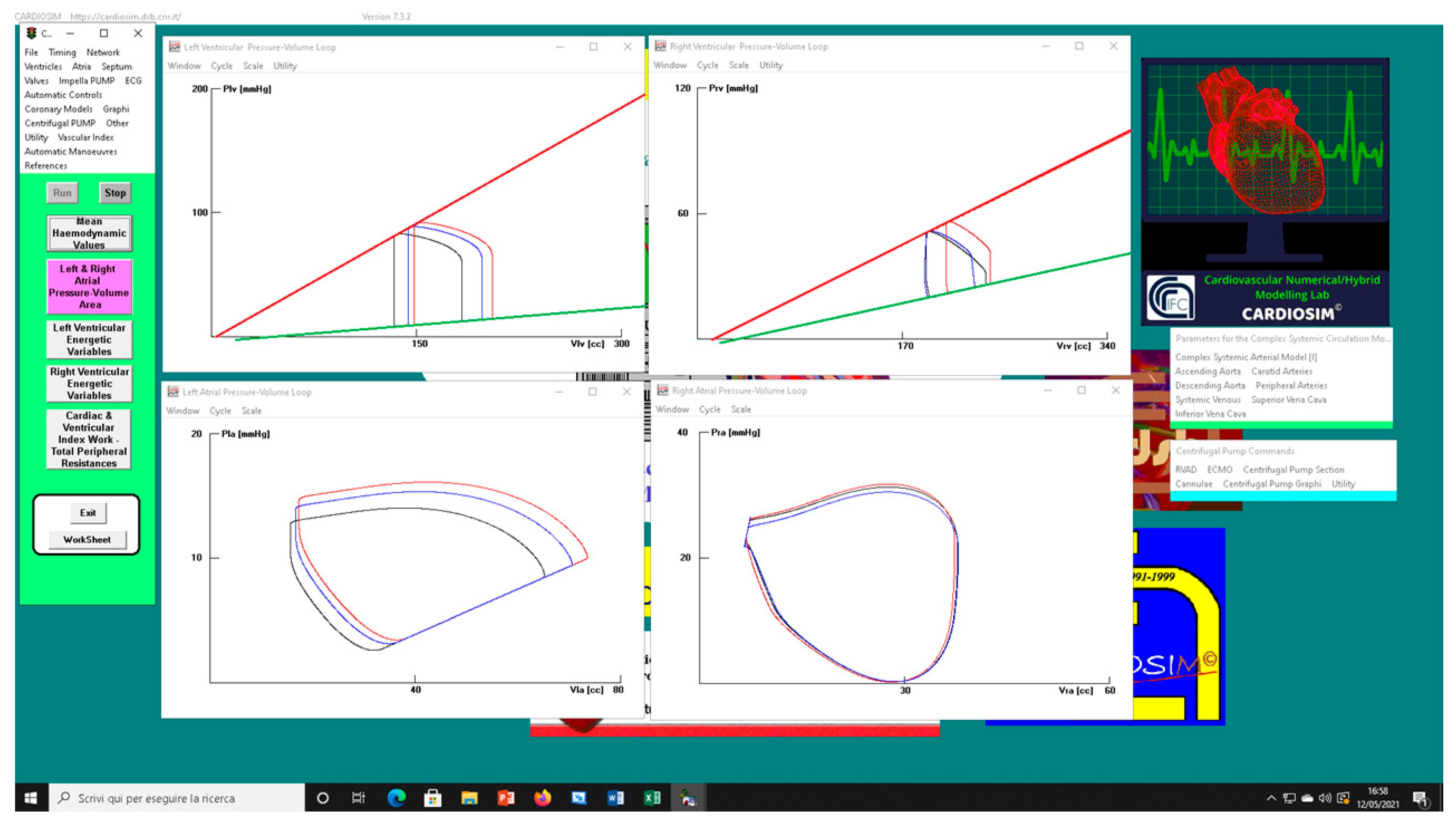
- Right and left ventricular end-systolic volume (ESVR-V and ESVL-V);
- ✓
- Right and left ventricular end-diastolic volume (EDVR-V and EDVL-V);
- ✓
- Stroke volume (SV);
- ✓
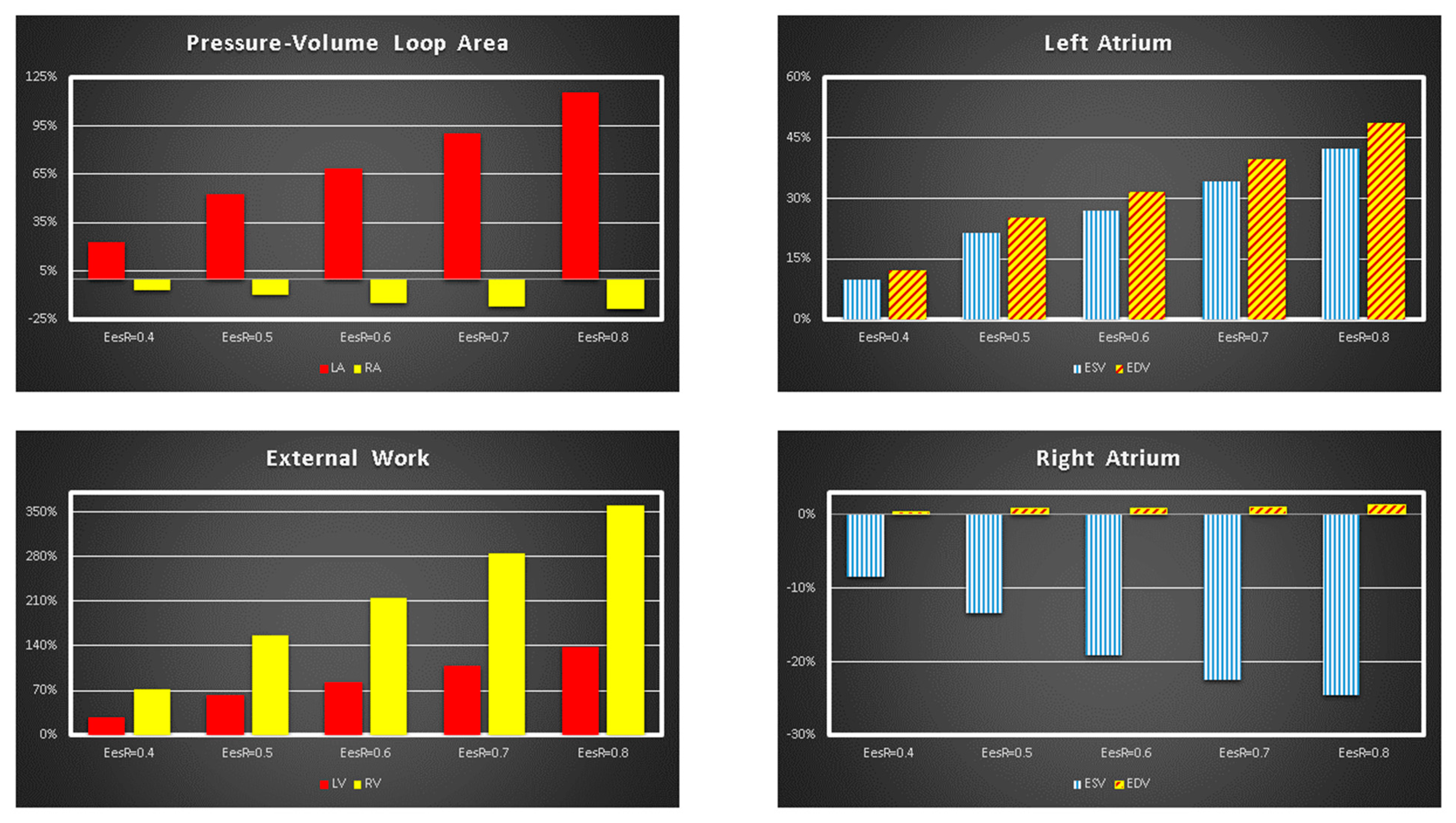
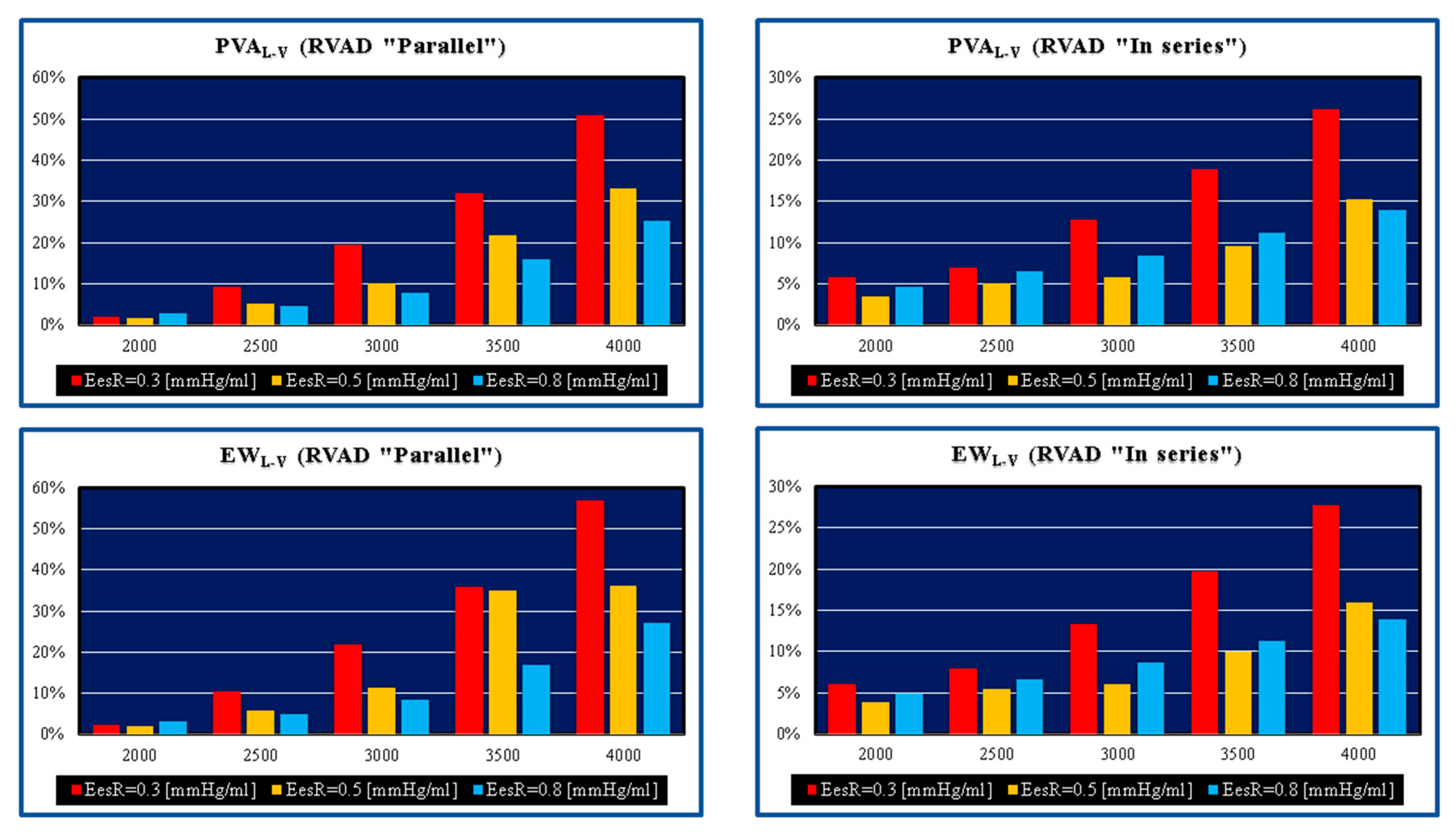
- Right and left ventricular external work (EWR-V and EWL-V) and pressure-volume area (PVAR-V and PVAL-V);
- ✓
- Right and left atrial end-systolic volume (ESVR-A and ESVL-A);
- ✓
- Right and left atrial end-diastolic volume (EDVR-A and EDVL-A);
- ✓
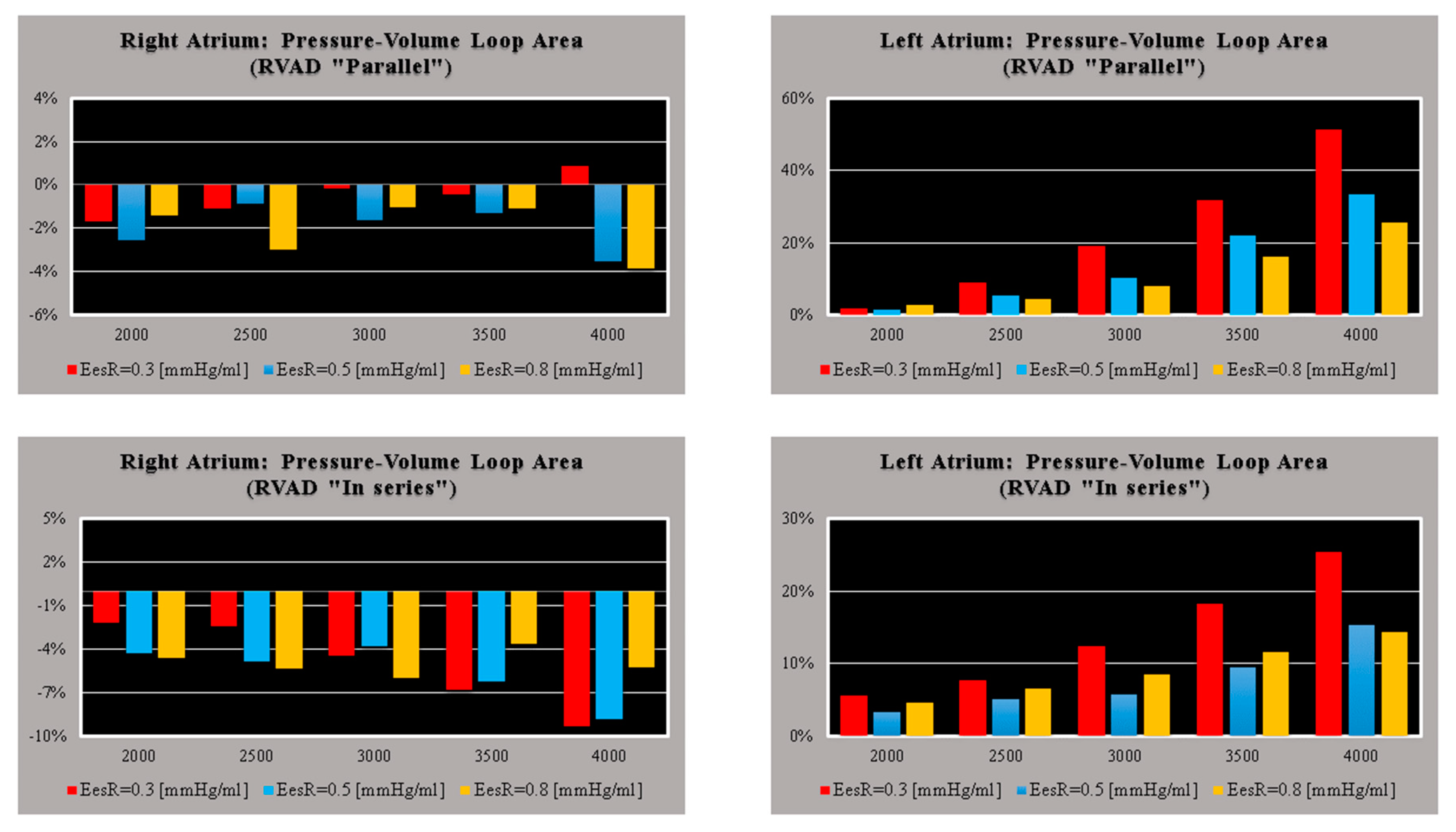
- Right and left atrial pressure-volume loop area (PVLAR-A and PVLAL-A);
- ✓
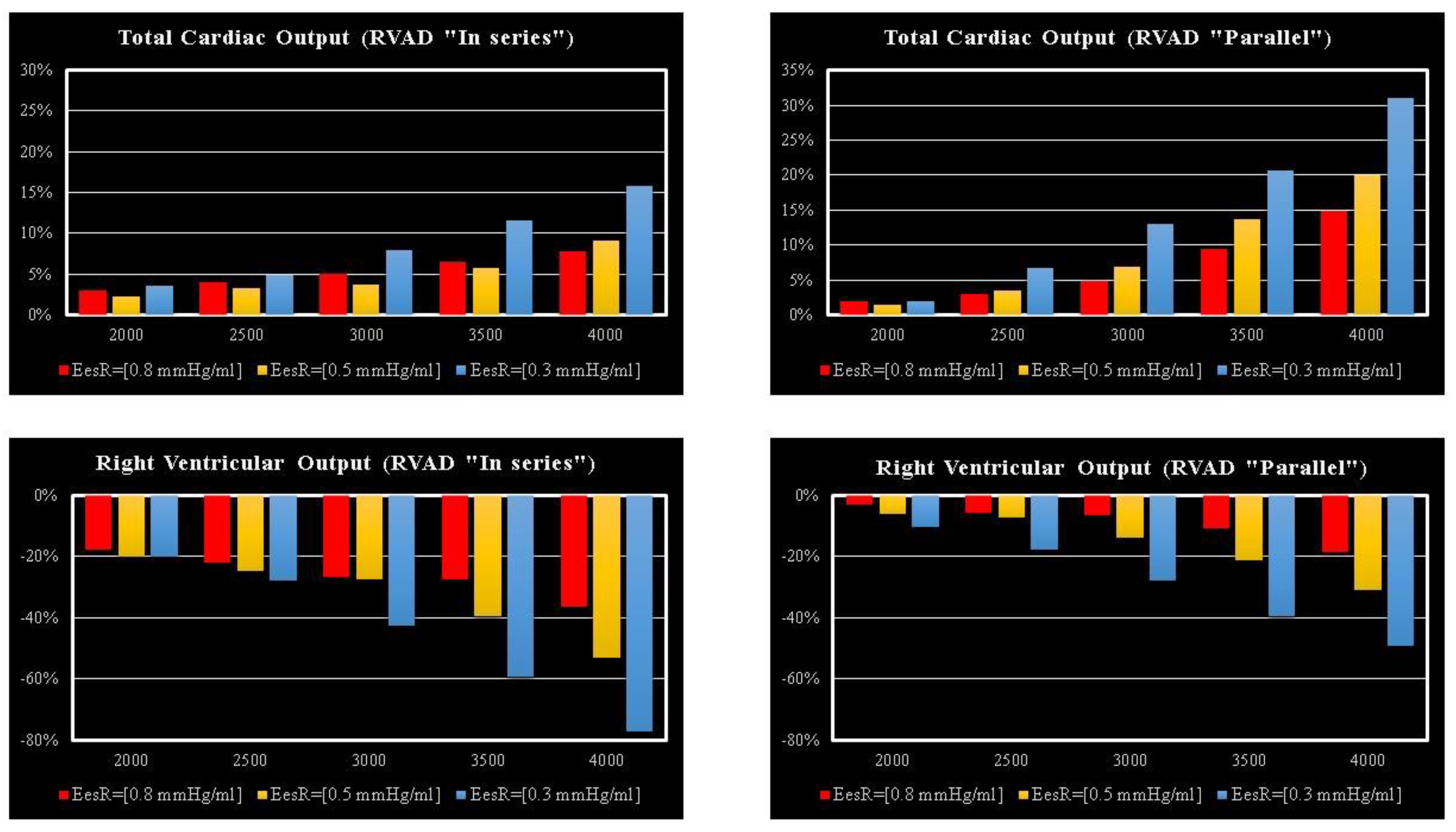
- Cardiac output (CO);
- ✓
- Systolic, diastolic, and mean systemic aortic pressure (AoP);
- ✓
- Systolic, diastolic, and mean pulmonary arterial pressure (PAP);
- ✓
- Pulmonary capillary wedge pressure (PCWP);
- ✓
- Right and left atrial pressure (RAP and LAP).
2. Materials and Methods
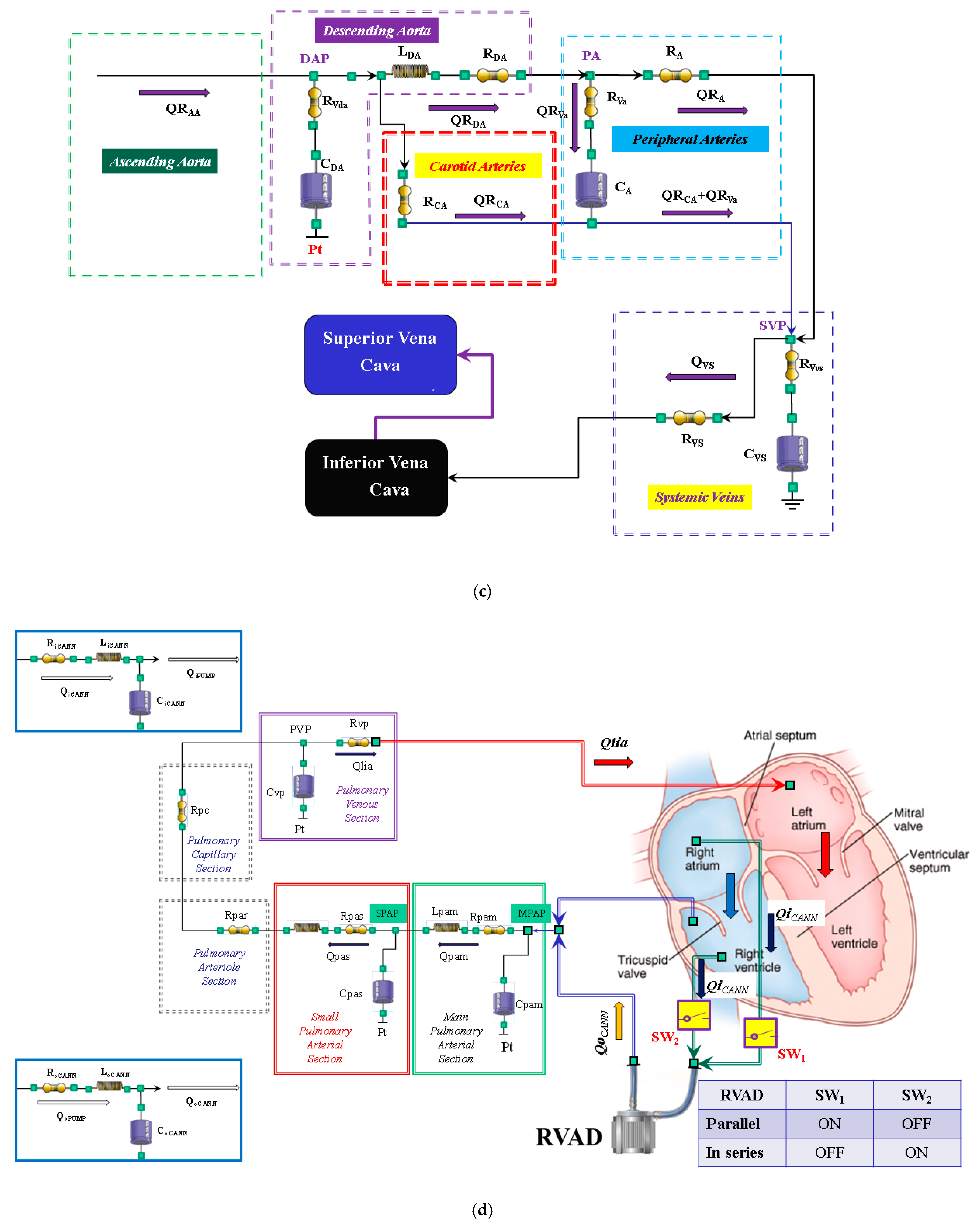
2.1. The Heart and Circulatory Numerical Network

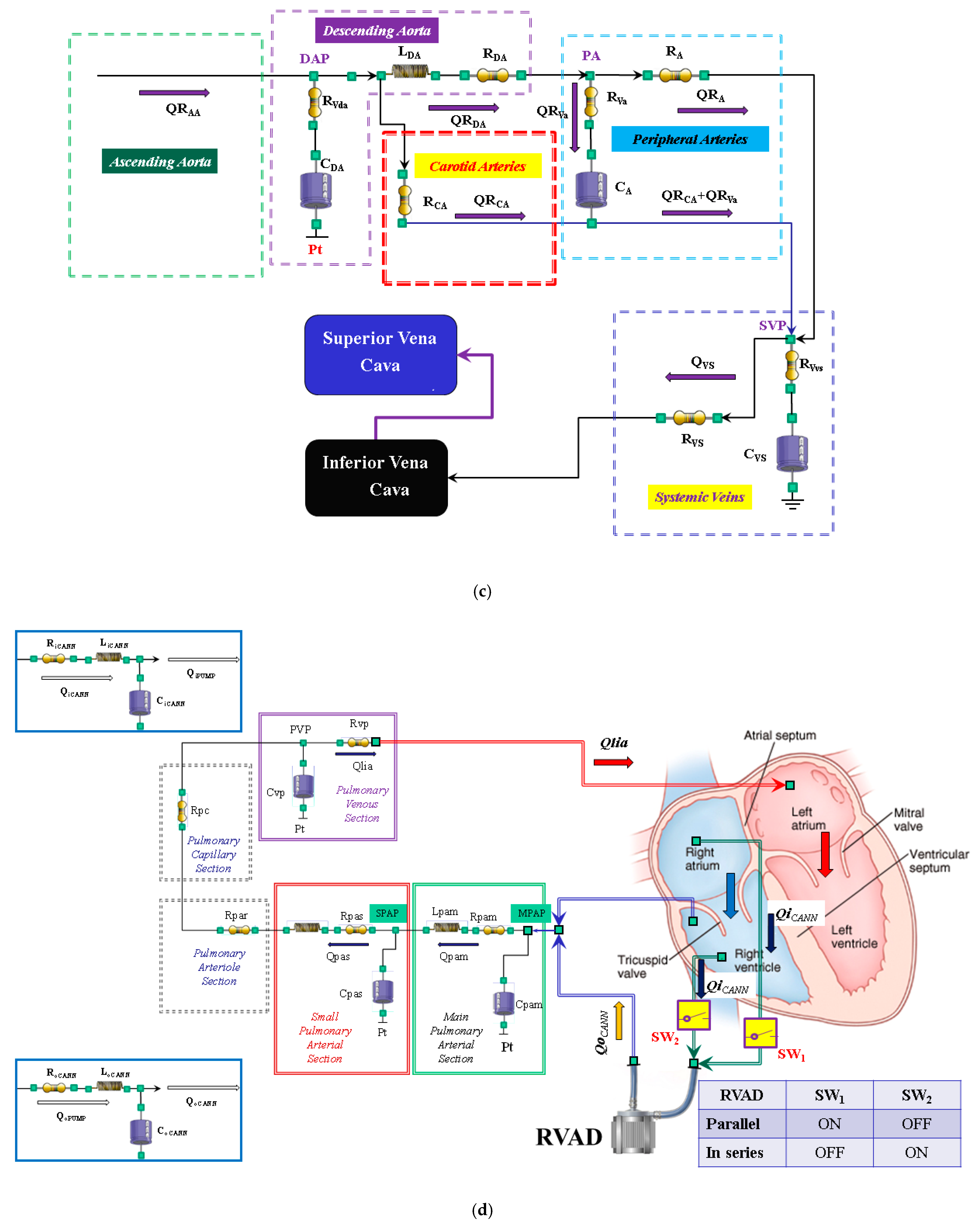
2.2. New Lumped-Parameter Model of the Systemic Circulation
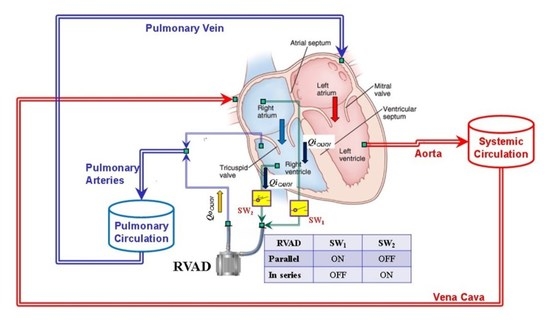
2.3. Right Ventricular Assist Device (RVAD)
2.4. Simulation Protocol
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mandawat, A.; Rao, S.V. Percutaneous Mechanical Circulatory Support Devices in Cardiogenic Shock. Circ. Cardiovasc. Interv. 2017, 10, e004337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vullaganti, S.; Tibrewala, A.; Rich, J.D.; Pham, D.T.; Rich, S. The use of a durable right ventricular assist device for isolated right ventricular failure due to combined pre- and postcapillary pulmonary hypertension. Pulm. Circ. 2019, 9, 1–3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaul, T.K.; Fields, B.L. Postoperative acute refractory right ventricular failure: Incidence, pathogenesis, management and prognosis. Cardiovasc. Surg. 2000, 8, 1–9. [Google Scholar] [CrossRef]
- Matthews, J.C.; Koelling, T.M.; Pagani, F.D.; Aaronson, K.D. The right ventricular failure risk score a pre-operative tool for assessing the risk of right ventricular failure in left ventricular assist device candidates. J. Am. Coll. Cardiol. 2008, 51, 2163–2172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frankfurter, C.; Molinero, M.; Vishram-Nielsen, J.K.K.; Foroutan, F.; Mak, S.; Rao, V.; Billia, F.; Orchanian-Cheff, A.; Alba, A.C. Predicting the Risk of Right Ventricular Failure in Patients Undergoing Left Ventricular Assist Device Implantation. A Systematic Review. Circ. Heart Fail. 2020, 13, e006994. [Google Scholar] [CrossRef]
- SAGE Journals. Available online: https://doi.org/10.1177/02676591211024817 (accessed on 6 April 2022).
- Kiernan, M.S.; Grandin, E.W.; Brinkley, M., Jr.; Kapur, N.K.; Pham, D.T.; Ruthazer, R.; Rame, J.E.; Atluri, P.; Birati, E.Y.; Oliveira, G.H.; et al. Early Right Ventricular Assist Device Use in Patients Undergoing Continuous-Flow Left Ventricular Assist Device Implantation. Incidence and Risk Factors from the Interagency Registry for Mechanically Assisted Circulatory Support. Circ. Heart Fail. 2017, 10, e003863. [Google Scholar] [CrossRef]
- Arrigo, M.; Huber, L.C.; Winnik, S.; Mikulicic, F.; Guidetti, F.; Frank, M.; Flammer, A.J.; Ruschitzka, F. Right Ventricular Failure: Pathophysiology, Diagnosis and Treatment. Card. Fail. Rev. 2019, 5, 140–146. [Google Scholar] [CrossRef] [Green Version]
- Naeije, R.; Brimioulle, S.; Dewachter, L. Biomechanics of the right ventriclein health and disease (2013 Grover Conference series). Pulm. Circ. 2014, 4, 395–406. [Google Scholar] [CrossRef] [Green Version]
- Tello, K.; Dalmer, A.; Axmann, J.; Vanderpoo, R.; Ghofrani, H.A.; Naeije, R.; Roller, F.; Seeger, W.; Sommer, N.; Wilhelm, J.; et al. Reserve of Right Ventricular—Arterial Coupling in the Setting of Chronic Overload. Circ. Heart Fail. 2019, 12, e005512. [Google Scholar] [CrossRef]
- Stevenson, L.W.; Hoffman, J.R.H.; Menachem, J.N. The Other Ventricle with Left Ventricular Assist Devices. J. Am. Coll. Cardiol. 2021, 78, 2309–2311. [Google Scholar] [CrossRef]
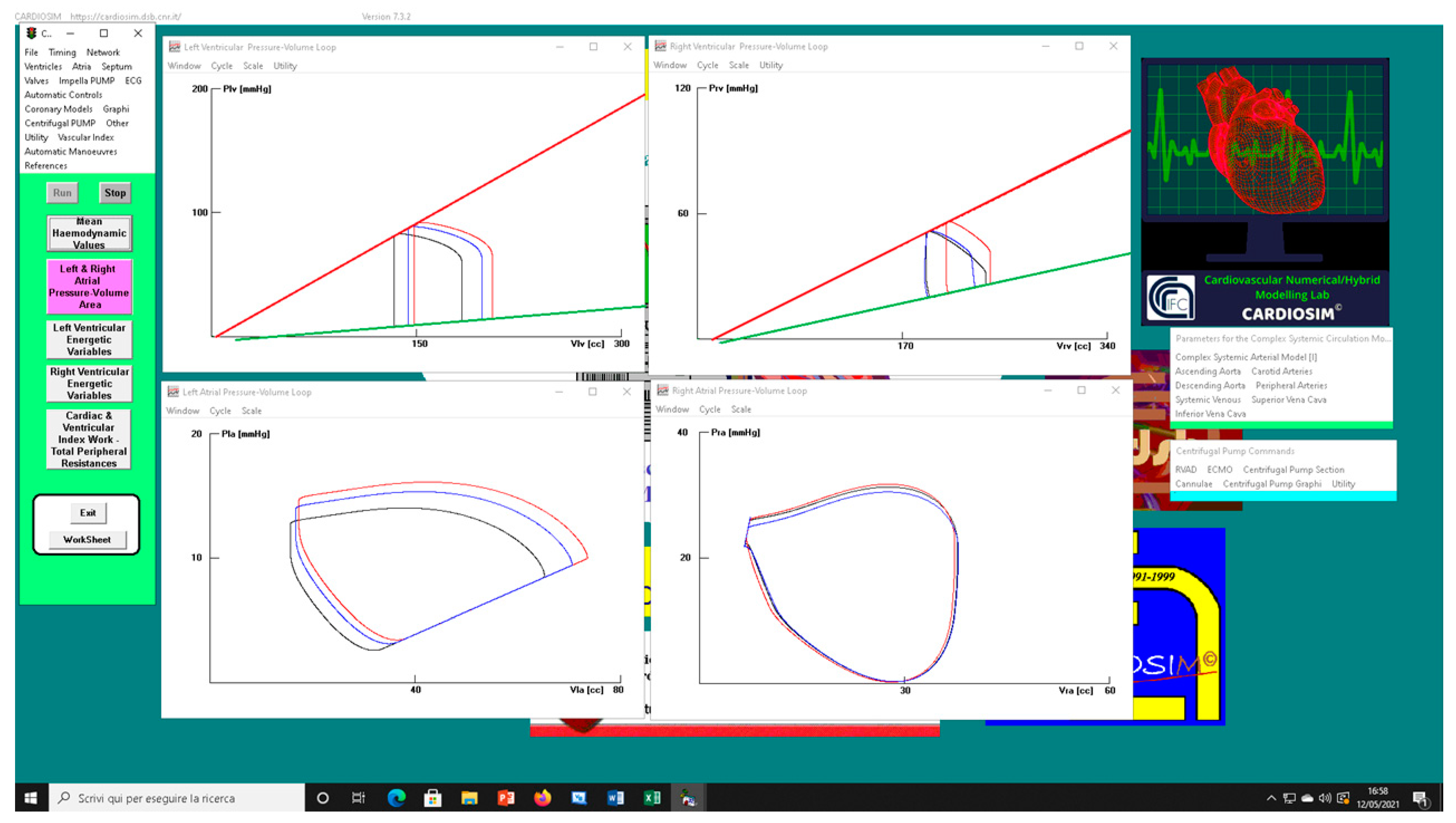
- De Lazzari, C.; Stalteri, D. 2011–2019, CARDIOSIM© Website. Original Website Platform Regarding the Implementation of the Cardiovascular Software Simulator CARDIOSIM©. Available online: https://cardiosim.dsb.cnr.it/ (accessed on 6 April 2022).
- De Lazzari, C.; Genuini, I.; Pisanelli, D.M.; D’Ambrosi, A.; Fedele, F. Interactive simulator for e-Learning environments: A teaching software for health care professionals. BioMed Eng. OnLine 2014, 13, 172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Lazzari, C.; Marconi, S.; Capoccia, M. Physiology of ventricular interdependence. In Concepts, Mathematical Modelling and Applications in Hart Failure, 1st ed.; Capoccia, M., De Lazzari, C., Eds.; Nova Science Publisher: New York, NY, USA, 2019; pp. 77–118. [Google Scholar]
- Capoccia, M.; Marconi, S.; Singh, S.A.; Pisanelli, D.M.; De Lazzari, C. Simulation as a preoperative planning approach in advanced heart failure patients. A retrospective clinical analysis. BioMed Eng. OnLine 2018, 17, 52. [Google Scholar] [CrossRef] [PubMed]
- De Lazzari, B.; Iacovoni, A.; Mottaghy, K.; Capoccia, M.; Badagliacca, R.; Vizza, C.D.; De Lazzari, C. ECMO Assistance During Mechanical Ventilation: Effects Induced on Energetic and Haemodynamic Variables. Comput. Methods Programs. Biomed. 2021, 202, 106003. [Google Scholar] [CrossRef] [PubMed]
- De Lazzari, C.; De Lazzari, B.; Iacovoni, A.; Marconi, S.; Papa, S.; Capoccia, M.; Badagliacca, R.; Vizza, C.D. Intra-Aortic Balloon Counterpulsation Timing: A New Numerical Model for Programming and Training in the Clinical Environment. Comput. Methods Programs Biomed. 2020, 194, 105537. [Google Scholar] [CrossRef]
- Marconi, S.; Capoccia, M.; De Lazzari, C. Mathematical Modelling of the Cardiovascular System. In Concepts, Mathematical Modelling and Applications in Hart Failure, 1st ed.; Capoccia, M., De Lazzari, C., Eds.; Nova Science Publisher: New York, NY, USA, 2019; pp. 119–158. [Google Scholar]
- De Lazzari, C. Interaction between the septum and the left (right) ventricular free wall in order to evaluate the effects on coronary blood flow: Numerical simulation. Comput. Methods Biomech. Biomed. Eng. 2012, 15, 1359–1368. [Google Scholar] [CrossRef] [Green Version]
- Capoccia, M.; Marconi, S.; De Lazzari, C. Decision-making in advanced heart failure patients requiring LVAD insertion: Can preoperative simulation become the way forward? A case study. J. Biomed. Eng. Inform. 2018, 4, 8–20. [Google Scholar] [CrossRef]
- De Lazzari, C.; Stalteri, D. 2011–2019, CARDIOSIM© Website. Available online: https://cardiosim.dsb.cnr.it/CirculationModels/pci4 (accessed on 6 April 2022).
- De Lazzari, C.; Stalteri, D. 2011–2019, CARDIOSIM© Website. Available online: https://cardiosim.dsb.cnr.it/CirculationModels/ncm2 (accessed on 6 April 2022).
- Ottesen, J.T.; Danielsen, M. Mathematical Modelling in Medicine, 1st ed.; IOS Press: Amsterdam, The Netherlands, 2000; pp. 1–235. [Google Scholar]
- Dell’Italia, L.J.; Walsh, R.A. Application of a time varying elastance model to right ventricular performance in man. Cardiovasc. Res. 1988, 22, 864–874. [Google Scholar] [CrossRef]
- Brimioulle, S.; Wauthy, P.; Ewalenko, P.; Rondelet, B.; Vermeulen, F.; Kerbaul, F.; Naeije, R.R. Single-beat estimation of right ventricular end-systolic pressure-volume relationship. Am. J. Physiol. Heart Circ. Physiol. 2003, 284, H1625–H1630. [Google Scholar] [CrossRef]
- Starling, M.R. Left ventricular-arterial coupling relations in the normal human heart. Am. Heart J. 1993, 125, 1659–1666. [Google Scholar] [CrossRef] [Green Version]
- Kiani, A.; Gilani Shakibi, J. Normal Values of Left Ventricular End-Systolic Elastance in Infants and Children. Iran J. Med. Sci. 2003, 28, 169–172. [Google Scholar]
- Donker, D.W.; Sallismani, M.; Bromé, M. Right–Left Ventricular Interaction in Left-Sided Heart Failure with and Without Venoarterial Extracorporeal Membrane Oxygenation Support—A Simulation Study. ASAIO J. 2021, 67, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Kocica, M.J.; Corno, A.F.; Carreras-Costa, F.; Ballester-Rodes, M.; Moghbel, M.C.; Cueva, C.N.; Lackovis, V.; Kanjuh, V.I.; Torrent-Guasp, F. The helical ventricular myocardial band: Global, three-dimensional, functional architecture of the ventricular myocardium. Eur. J. Cardiothorac. Surg. 2006, 29, S21–S40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buckberg, G.; Hoffman, J.I.E.; Mahajan, A.; Saleh, S.; Coghlan, C. Cardiac mechanics revisited: The relationship of cardiac architecture to ventricular function. Circulation 2008, 118, 2571–2587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buckberg, G.; Hoffman, J.I.E. Right ventricular architecture responsible for mechanical performance: Unifying the role of ventricular septum. J. Thorac. Cardiovasc. Surg. 2014, 148, 3166–3171. [Google Scholar] [CrossRef] [Green Version]
- James, T.N. Anatomy of the Crista Supraventricularis: Its Importance for Understanding Right Ventricular Function, Right Ventricular Infarction and Related Conditions. J. Am. Coll. Cardiol. 1985, 6, 1083–1095. [Google Scholar] [CrossRef] [Green Version]
- Raina, A.; Vaidya, A.; Gertz, Z.M.; Chambers, S.; Forfia, P.R. Marked changes in right ventricular contractile pattern after cardiothoracic surgery: Implications for post-surgical assessment of right ventricular function. J. Heart Lung Transpl. 2013, 32, 777–783. [Google Scholar] [CrossRef]
- Brown, S.B.; Raina, A.; Katz, D.; Szerlip, M.; Wiegers, S.E.; Forfia, P.R. Longitudinal Shortening Accounts for the Majority of Right Ventricular Contraction and Improves After Pulmonary Vasodilator Therapy in Normal Subjects and Patients with Pulmonary Arterial Hypertension. Chest 2011, 140, 27–33. [Google Scholar] [CrossRef]
- Sanz, J.; Sánchez-Quintana, D.; Bossone, E.; Bogaard, H.I.; Naeije, R. Anatomy, Function and Dysfunction of the Right Ventricle. J. Am. Coll. Cardiol. 2019, 73, 1463–1482. [Google Scholar] [CrossRef]
- Konstam, M.A.; Kiernan, M.S.; Bernstein, D.; Bozkurt, B.; Jacob, M.; Kapur, N.K.; Kociol, R.D.; Lewis, E.F.; Mehra, M.R.; Pagani, F.D.; et al. On behalf of the American Heart Association Council on Clinical Cardiology; Council on Cardiovascular Disease in the Young; and Council on Cardiovascular Surgery and Anaesthesia. Evaluation and Management of Right-Sided Heart Failure. A Scientific Statement from the American Heart Association. Circulation 2018, 137, e578–e622. [Google Scholar]
- Haddad, F.; Hunt, S.A.; Rosenthal, D.N.; Murphy, D.J. Right Ventricular Function in Cardiovascular Disease, Part I. Anatomy, Physiology, Aging and Functional Assessment of the Right Ventricle. Circulation 2008, 117, 1436–1448. [Google Scholar] [CrossRef]
- Kuehne, T.; Yilmaz, S.; Steendijk, P.; Moore, P.; Groenink, M.; Saaed, M.; Weber, O.; Higgins, C.B.; Ewert, P.; Fleck, E.; et al. Magnetic Resonance Imaging Analysis of Right Ventricular Pressure-Volume Loops. In Vivo Validation and Clinical Application in Patients with Pulmonary Hypertension. Circulation 2004, 110, 2010–2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzpatrick, J.R.; Frederick, J.R.; Hiesinger, W.; Hsu, V.M.; McCormick, R.C.; Kozin, E.D.; Laporte, C.M.; O’Hara, M.L.; Howell, E.; Dougherty, D.; et al. Early planned institution of biventricular mechanical circulatory support results in improved outcomes compared with delayed conversion of a left ventricular assist device to a biventricular assist device. J. Thorac. Cardiovasc. Surg. 2009, 137, 971–977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischer, Q.; Kirsch, M. Liberal Right Ventricular Assist Device Extracorporeal Membrane Oxygenation Support for Right Ventricular Failure after Implantable Left Ventricular Assist Device Placement. ASAIO J. 2018, 64, 741–747. [Google Scholar] [CrossRef] [PubMed]
- Beller, J.P.; Mehaffey, J.H.; Wegermann, Z.K.; Grau-Sepulveda, M.; O’Brien, S.M.; Brennan, J.M.; Thourani, V.; Badhwar, V.; Pagani, F.D.; Ailawadi, G.; et al. Strategies for Mechanical Right Ventricular Support during Left Ventricular Assist Device Implant. Ann. Thorac. Surg. 2021, in press. [CrossRef]
- Rame, J.E.; Pagani, F.D.; Kiernan, M.S.; Oliveira, G.H.; Birati, E.Y.; Atluri, P.; Gaffey, A.; Grandin, E.W.; Myers, S.L.; Collum, C.; et al. Evolution of Late Right Heart Failure with Left Ventricular Assist Devices and Association with Outcomes. J. Am. Coll. Cardiol. 2021, 78, 2294–2308. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Symbol | Description | Unit |
|---|---|---|
| Plv(t) [Prv(t)] | Instantaneous left (right) ventricular pressure | mmHg |
| Plv,0 [Prv,0] | Resting left (right) ventricular pressure | mmHg |
| Vlv(t) [Vrv(t)] | Instantaneous left (right) ventricular volume | mL |
| Vlv,0 [Vrv,0] | Resting left (right) ventricular volume | mL |
| elv(t) [erv(t)] | Left (right) ventricular elastance | mmHg·mL−1 |
| eVsp(t) | Inter-ventricular septum elastance | mmHg·mL−1 |
| Pla(t) [Pra(t)] | Instantaneous left (right) atrial pressure | mmHg |
| Pla,0 [Pra,0] | Resting left (right) atrial pressure | mmHg |
| Vla(t) [Vra(t)] | Instantaneous left (right) atrial volume | mL |
| Vla,0 [Vra,0] | Resting left (right) atrial volume | mL |
| ela(t) [era(t)] | Left (right) atrial elastance | mmHg·mL−1 |
| eAsp(t) | Inter-atrial septum elastance | mmHg·mL−1 |
| Rpam (Rpas) | Main (small) pulmonary arterial resistance [mmHg·cm−3·s] |
| Lpam (Lpas) | Main (small) pulmonary arterial inertance [mmHg·cm−3·s2] |
| Cpam (Cpas) | Main (small) pulmonary arterial compliance [mmHg−1·cm−3] |
| MPAP (SPAP) | Main (small) pulmonary arterial pressure [mmHg] |
| Rpar (Rpc) | Pulmonary arteriole (capillary) resistance [mmHg·cm−3·s] |
| Wedge | Pulmonary capillary wedge pressure [mmHg] |
| Cvp | Pulmonary venous compliance [mmHg−1·cm−3] |
| Rvp | Pulmonary venous resistance [mmHg·cm−3·s] |
| PVP | Pulmonary venous pressure [mmHg] |
| Rro (Rri) | Pulmonary (tricuspid) valve resistance [mmHg·cm−3·s] |
| SVP | Systemic veins pressure [mmHg] |
| CVS | Systemic veins compliance [mmHg−1·cm−3] |
| RVS | Systemic veins resistance [mmHg·cm−3·s] |
| RVvs | Resistor accounting viscous losses of the systemic veins wall [mmHg·cm−3·s] |
| RSVC_I | First Superior vena cava resistance [mmHg·cm−3·s] |
| CSVC | Superior vena cava compliance [mmHg−1·cm−3] |
| LSVC | Superior vena cava inertance [mmHg·cm−3·s2] |
| RSVC_II | Second superior vena cava resistance [mmHg·cm−3·s] |
| SVCP | Superior vena cava pressure [mmHg] |
| LAP(RAP) | Left (right) atrial pressure [mmHg] |
| LVP(RVP) | Left (right) ventricular pressure [mmHg] |
| RAA | Ascending aorta resistance [mmHg·cm−3·s] |
| RVaa | Resistor accounting viscous losses of the ascending aorta wall [mmHg·cm−3·s] |
| LAA | Ascending aorta inertance [mmHg·cm−3·s2] |
| CAA | Ascending aorta compliance [mmHg−1·cm−3] |
| AoP | Aortic Pressure [mmHg] |
| RDA | Descending aorta resistance [mmHg·cm−3·s] |
| RVda | Resistor accounting viscous losses of the descending aorta wall [mmHg·cm−3·s] |
| LDA | Descending aorta inertance [mmHg·cm−3·s2] |
| CDA | Descending aorta compliance [mmHg−1·cm−3] |
| DPA | Descending aortic pressure [mmHg] |
| RCA | Carotid arteries resistance [mmHg·cm−3·s] |
| RA | Peripheral arteries resistance [mmHg·cm−3·s] |
| RVa | Resistor accounting viscous losses of the peripheral arteries wall [mmHg·cm−3·s] |
| CA | Peripheral arteries compliance [mmHg−1·cm−3] |
| PA | Peripheral arteries pressure [mmHg] |
| RIVC, RIVC_I, RIVC_II | Inferior vena cava resistances [mmHg·cm−3·s] |
| LIVC | Inferior vena cava inertance [mmHg·cm−3·s2] |
| CIVC | Inferior vena cava compliance [mmHg−1·cm−3] |
| Pt | Mean intrathoracic pressure [mmHg] |
| ela (era) | Left (right) atrial elastance [mmHg/mL] |
| elv (erv) | Left (right) ventricular elastance [mmHg/mL] |
| eAspt (eVspt) | Inter-atrial (-ventricular) septal elastance [mmHg/mL] |
| Qartery (Qvenous) | Coronary arterial (venous) flow [mL/s] |
| RoCANN (RiCANN) | RVAD output (input) cannula resistance [mmHg·cm−3·s] |
| LoCANN (LiCANN) | RVAD output (input) cannula inertance [mmHg·cm−3·s2] |
| CoCANN (CiCANN) | RVAD output (input) cannula compliance [mmHg−1·cm−3] |
| Qli (Qlo) | Left ventricular input (output) flow [mL/s] |
| Qri (Qro) | Right ventricular input (output) flow [mL/s] |
| Qlia (Qria) | Left (right) atrial input flow [mL/s] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Lazzari, B.; Iacovoni, A.; Capoccia, M.; Papa, S.; Badagliacca, R.; Filomena, D.; De Lazzari, C. Ventricular and Atrial Pressure—Volume Loops: Analysis of the Effects Induced by Right Centrifugal Pump Assistance. Bioengineering 2022, 9, 181. https://doi.org/10.3390/bioengineering9050181
De Lazzari B, Iacovoni A, Capoccia M, Papa S, Badagliacca R, Filomena D, De Lazzari C. Ventricular and Atrial Pressure—Volume Loops: Analysis of the Effects Induced by Right Centrifugal Pump Assistance. Bioengineering. 2022; 9(5):181. https://doi.org/10.3390/bioengineering9050181
Chicago/Turabian StyleDe Lazzari, Beatrice, Attilio Iacovoni, Massimo Capoccia, Silvia Papa, Roberto Badagliacca, Domenico Filomena, and Claudio De Lazzari. 2022. "Ventricular and Atrial Pressure—Volume Loops: Analysis of the Effects Induced by Right Centrifugal Pump Assistance" Bioengineering 9, no. 5: 181. https://doi.org/10.3390/bioengineering9050181
APA StyleDe Lazzari, B., Iacovoni, A., Capoccia, M., Papa, S., Badagliacca, R., Filomena, D., & De Lazzari, C. (2022). Ventricular and Atrial Pressure—Volume Loops: Analysis of the Effects Induced by Right Centrifugal Pump Assistance. Bioengineering, 9(5), 181. https://doi.org/10.3390/bioengineering9050181