
Cone-Beam Computed Tomographic Assessment of the Mandibular Condylar Volume in Different Skeletal Patterns: A Retrospective Study in Adult Patients


 ,
,  ,
, 

 and
and 
Abstract
1. Introduction
2. Materials and Methods
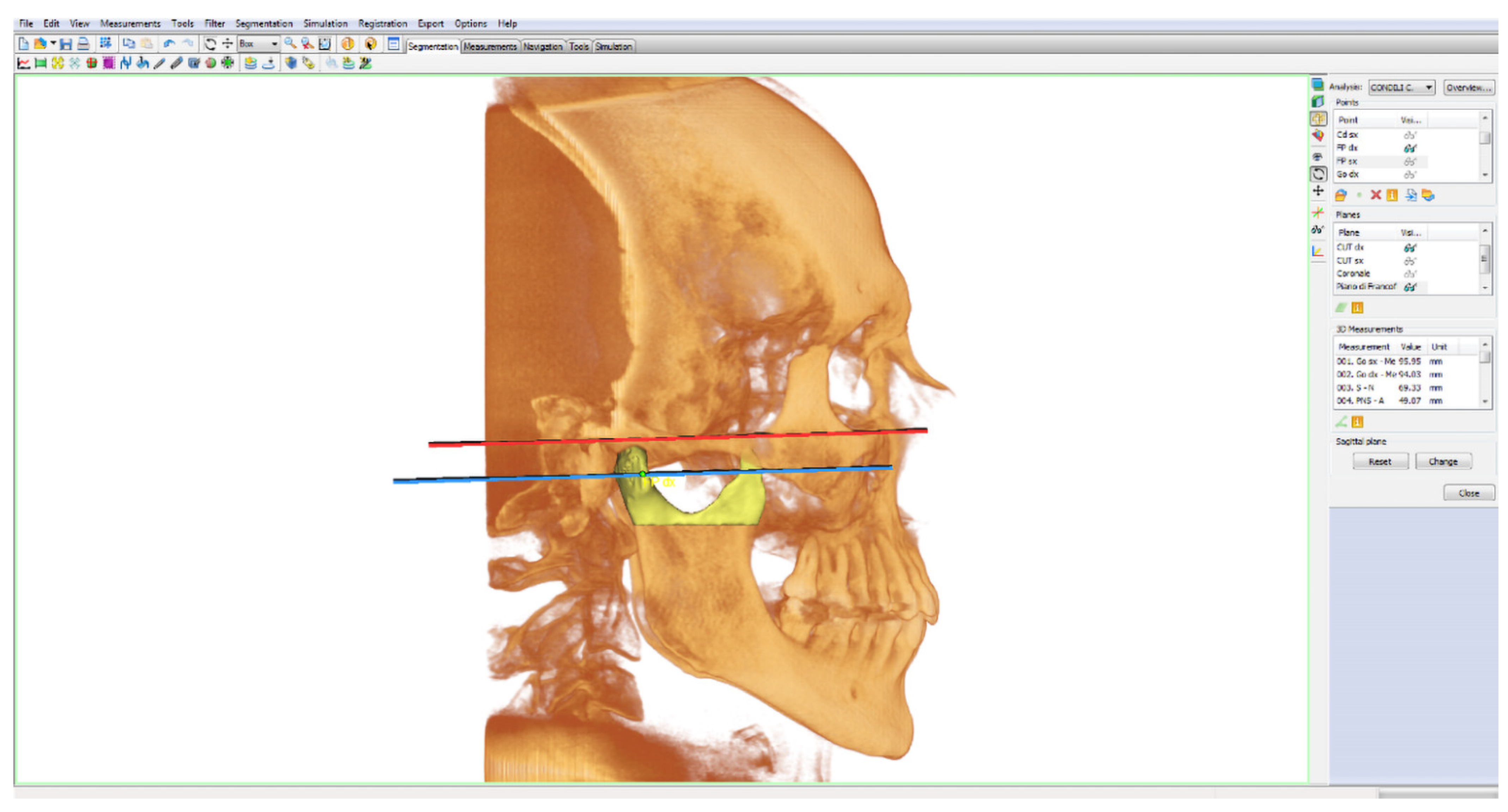
2.1. Mandibular Condylar Segmentation and Volume
- Porion point (right/left Po): highest point of the external acoustic meatus;
- Lower orbital point (right/left OR): lowest point of the orbital edge, the base of the orbital cavity;
- Pterygoid fovea point (right/left FP): most recessed point on the front face of the mandibular neck, identifiable in the three projections: axial, coronal and sagittal. It was chosen as the point that delimits the separation passage between the head and neck of the mandibular condyle.
- Frankfurt plane: calculated as the plane passing through the lower right and left orbital points (right/left OR) and from the right and left porion points (right/left Po);
- Cut plane of the right condyle (right CUT): plane passing through right FP and parallel to the Frankfurt plane;
- Cut plane of the left condyle (left CUT): plane passing through left FP and parallel to the Frankfurt plane.
2.2. Statistics
- Divergence angle, also called the intermaxillary angle, is the angle formed between the maxillary plane (Ans-Pns) with the mandibular plane (right/left Go-Me). This angle identifies and distinguishes the subjects as: normo/hyper/hypo divergent = 41 ± 1 (°);
- Total goniac angle is the angle that is formed between the body (right/left Go-Me) and the branch of the jaw (right/left Cd-right/left Go) of each side = 120° ± 5°. Increased values of the angle indicate a post-rotation growth pattern while decreased values indicate a horizontal growth.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hegde, S.; Bn, P.; Shetty, S.R. Morphological and Radiological Variations of Mandibular Condyles in Health and Diseases: A Systematic Review. Dentistry 2013, 3, 1–5. [Google Scholar] [CrossRef]
- Ahmed, J.; Sujir, N.; Shenoy, N.; Binnal, A.; Ongole, R. Morphological Assessment of TMJ Spaces, Mandibular Condyle, and Glenoid Fossa Using Cone Beam Computed Tomography (CBCT): A Retrospective Analysis. Indian J. Radiol Imaging 2021, 31, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Park, I.Y.; Kim, J.H.; Park, Y.H. Three-dimensional cone-beam computed tomography based comparison of condylar position and morphology according to the vertical skeletal pattern. Korean J. Orthod. 2014, 45, 66–73. [Google Scholar] [CrossRef]
- Saccucci, M.; D’Attilio, M.; Rodolfino, D.; Festa, F.; Polimeni, A.; Tecco, S. Condylar volume and condylar area in class I, class II and class III young adult subjects. Head Face Med. 2012, 8, 34. [Google Scholar] [CrossRef] [PubMed]
- Farronato, M.; Cavagnetto, D.; Abate, A.; Cressoni, P.; Fama, A.; Maspero, C. Assessment of condylar volume and ramus height in JIA patients with unilateral and bilateral TMJ involvement: Retrospective case-control study. Clin. Oral Investig. 2019, 24, 2635–2643. [Google Scholar] [CrossRef] [PubMed]
- Farronato, G.; Carletti, V.; Maspero, C.; Farronato, D.; Giannini, L.; Bellintani, C. Craniofacial growth in children affected by juvenile idiopathic arthritis involving the temporomandibular joint: Functional therapy management. J. Clin. Pediatr. Dent. 2009, 33, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Ludlow, J.B.; Timothy, R.; Walker, C.; Hunter, R.; Benavides, E.; Samuelson, D.B.; Scheske, M.J. Effective dose of dental CBCT-a meta analysis of published data and additional data for nine CBCT units. Dentomaxillofac. Radiol. 2015, 44, 20140197. [Google Scholar] [CrossRef]
- Farronato, G.; Salvadori, S.; Nolet, F.; Zoia, A.; Farronato, D. Assessment of inter- and intra-operator cephalometric tracings on cone beam CT radiographs: Comparison of the precision of the cone beam CT versus the latero-lateral radiograph tracing. Prog. Orthod. 2014, 15, 1. [Google Scholar] [CrossRef] [PubMed]
- Kapila, S.D.; Nervina, J.M. CBCT in orthodontics: Assessment of treatment outcomes and indications for its use. Dentomaxillofac. Radiol. 2015, 44, 20140282. [Google Scholar] [CrossRef] [PubMed]
- Venkatesh, E.; Elluru, S.V. Cone beam computed tomography: Basics and applications in dentistry. J. Istanb. Univ. Fac. Dent. 2017, 51, S102–S121. [Google Scholar] [CrossRef] [PubMed]
- Farronato, G.; Garagiola, U.; Dominici, A.; Periti, G.; de Nardi, S.; Carletti, V.; Farronato, D. “Ten-point” 3D cephalometric analysis using low-dosage cone beam computed tomography. Prog. Orthod. 2010, 11, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.J.; Lagravere, M.O.; Kaipatur, N.R.; Major, P.W.; Romanyk, D.L. Reliability and accuracy of a method for measuring temporomandibular joint condylar volume. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 131, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Tecco, S.; Saccucci, M.; Nucera, R.; Polimeni, A.; Pagnoni, M.; Cordasco, G.; Festa, F.; Iannetti, G. Condylar volume and surface in Caucasian young adult subjects. BMC Med. Imaging 2010, 10, 28. [Google Scholar] [CrossRef] [PubMed]
- Bayram, M.; Kayipmaz, S.; Sezgin, Ö.S.; Küçük, M. Volumetric analysis of the mandibular condyle using cone beam computed tomography. Eur. J. Radiol. 2012, 81, 1812–1816. [Google Scholar] [CrossRef] [PubMed]
- Mendoza-García, L.V.; Bellot-Arcís, C.; Montiel-Company, J.M.; García-Sanz, V.; Almerich-Silla, J.M.; Paredes-Gallardo, V. Linear and Volumetric Mandibular Asymmetries in Adult Patients with Different Skeletal Classes and Vertical Patterns: A Cone-Beam Computed Tomography Study. Sci. Rep. 2018, 8, 12319. [Google Scholar] [CrossRef] [PubMed]
- Lo Giudice, A.; Rustico, L.; Caprioglio, A.; Migliorati, M.; Nucera, R. Evaluation of condylar cortical bone thickness in patient groups with different vertical facial dimensions using cone-beam computed tomography. Odontology 2020, 108, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Ferrario, V.F.; Sforza, C.; Miani, A.; D’Addona, A.; Tartaglia, G. Statistical evaluation of some mandibular reference positions in normal young people. Int. J. Prosthodont. 1992, 5, 158–165. [Google Scholar]
- Bernal-Mañas, C.M.; González-Sequeros, O.; Moreno-Cascales, M.; Sarria-Cabrera, R.; Latorre-Reviriego, R.M. New anatomo-radiological findings of the lateral pterygoid muscle. Surg. Radiol. Anat. 2016, 38, 1033–1043. [Google Scholar] [CrossRef] [PubMed]
- Sakaguchi-Kuma, T.; Hayashi, N.; Fujishiro, H.; Yamaguchi, K.; Shimazaki, K.; Ono, T.; Akita, K. An anatomic study of the attachments on the condylar process of the mandible: Muscle bundles from the temporalis. Surg. Radiol. Anat. 2016, 38, 461–467. [Google Scholar] [CrossRef]
- Hofmann, E.; Fimmers, R.; Schmid, M.; Hirschfelder, U.; Detterbeck, A.; Hertrich, K. Landmarks of the Frankfort horizontal plane: Reliability in a three-dimensional Cartesian coordinate system. J. Orofac. Orthop. 2016, 77, 373–383. [Google Scholar] [CrossRef]
- Roberts, W.E.; Goodacre, C.J. The Temporomandibular Joint: A Critical Review of Life-Support Functions, Development, Articular Surfaces, Biomechanics and Degeneration. J. Prosthodont. 2020, 29, 772–779. [Google Scholar] [CrossRef]
- Caruso, S.; Storti, E.; Nota, A.; Ehsani, S.; Gatto, R. Temporomandibular Joint Anatomy Assessed by CBCT Images. BioMed Res. Int. 2017, 2017, 2916953. [Google Scholar] [CrossRef] [PubMed]
- Willems, N.M.B.K.; Langenbach, G.E.J.; Everts, V.; Zentner, A. The microstructural and biomechanical development of the condylar bone: A review. Eur. J. Orthod. 2014, 36, 479–485. [Google Scholar] [CrossRef]
- Almashraqi, A.A. Dimensional and Positional Associations between the Mandibular Condyle and Glenoid Fossa: A Three-dimensional Cone-beam Computed Tomography-based Study. J. Contemp. Dent. Pract. 2020, 21, 1075–1083. [Google Scholar] [CrossRef] [PubMed]
- Kaur, A.; Natt, A.S.; Mehra, S.K.; Maheshwari, K.; Singh, G.; Kaur, A.; Patil, S. Improved Visualization and Assessment of Condylar Position in the Glenoid Fossa for Different Occlusions: A CBCT Study. J. Contemp. Dent. Pract. 2016, 17, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Bielecki-Kowalski, B.; Kozakiewicz, M. Assessment of Differences in the Dimensions of Mandible Condyle Models in Fan-versus Cone-Beam Computer Tomography Acquisition. Materials 2021, 14, 1388. [Google Scholar] [CrossRef] [PubMed]
- Nakawaki, T.; Yamaguchi, T.; Tomita, D.; Hikita, Y.; Adel, M.; Katayama, K.; Maki, K. Evaluation of mandibular volume classified by vertical skeletal dimensions with cone-beam computed tomography. Angle Orthod. 2016, 86, 949–954. [Google Scholar] [CrossRef] [PubMed]
- Katayama, K.; Yamaguchi, T.; Sugiura, M.; Haga, S.; Maki, K. Evaluation of mandibular volume using cone-beam computed tomography and correlation with cephalometric values. Angle Orthod. 2014, 84, 337–342. [Google Scholar] [CrossRef]
- Loiola, M.E.D.A.; Fuziy, A.; Higa, R.H.; Fuziy, C.H.F.; Júnior, L.G.G.; Costa, A.L.F. In vivo three-dimensional cephalometric landmarks using CBCT for assessment of condylar volume and surface in individuals with Class I, II, and III malocclusions. Cranio 2020, Dec 9, 1–6. [Google Scholar] [CrossRef]
- Di Palma, E.; Gasparini, G.; Pelo, S.; Tartaglia, G.M.; Chimenti, C. Activities of masticatory muscles in patients after orthognathic surgery. J. Cranio Maxillofac. Surg. 2009, 37, 417–420. [Google Scholar] [CrossRef]
- Hasebe, A.; Yamaguchi, T.; Nakawaki, T.; Hikita, Y.; Katayama, K.; Maki, K. Comparison of condylar size among different anteroposterior and vertical skeletal patterns using cone-beam computed tomography. Angle Orthod. 2019, 89, 306–311. [Google Scholar] [CrossRef]
- Sella-Tunis, T.; Pokhojaev, A.; Sarig, R.; O’Higgins, P.; May, H. Human mandibular shape is associated with masticatory muscle force. Sci. Rep. 2018, 8, 6042. [Google Scholar] [CrossRef] [PubMed]
- Santander, P.; Quast, A.; Olbrisch, C.; Rose, M.; Moser, N.; Schliephake, H.; Meyer-Marcotty, P. Comprehensive 3D analysis of condylar morphology in adults with different skeletal patterns—A cross-sectional study. Head Face Med. 2020, 16, 33. [Google Scholar] [CrossRef] [PubMed]
- Morita, T.; Hiraba, K.; Matsunaga, T.; Ito, Y.; Maruo, H.; Kurita, K. Unusual postero-inferior condylar movements that depend on the position of occlusal contact during fictive mastication in rabbits. Arch. Oral Biol. 2015, 60, 370–384. [Google Scholar] [CrossRef]
- Dadgar-Yeganeh, A.; Hatcher, D.C.; Oberoi, S. Association between degenerative temporomandibular joint disorders, vertical facial growth, and airway dimension. J. World Fed. Orthod. 2021, 10, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Zhou, P.; Zhang, J.; Zhang, M.; Yang, H.; Liu, Q.; Zhang, H.; Liu, J.; Duan, J.; Lu, Y.; Wang, M. Effects of occlusion modification on the remodelling of degenerative mandibular condylar processes. Oral Dis. 2020, 26, 597–608. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | N Condyles | Median | Mean | Min–Max | SD | p-Value * | p-Value ** |
|---|---|---|---|---|---|---|---|
| Anb 2 ± 2 (°) | |||||||
| Class I | 42 | 802 | 824 | 301–1362 | 266 | Reference | Reference |
| Class II | 60 | 665 | 726 | 329–1653 | 249 | 0.10 | 0.03 |
| Class III | 44 | 633 | 703 | 378–1365 | 239 | 0.15 | 0.08 |
| Divergence 41 ± 1 (°) | |||||||
| Hypodivergent | 59 | 798 | 812 | 378–1365 | 259 | 0.50 | 0.51 |
| Normodivergent | 29 | 727 | 753 | 347–1222 | 229 | Reference | Reference |
| Hyperdivergent | 58 | 624 | 688 | 301–1653 | 246 | 0.16 | 0.17 |
| Total goniac angle 120 ± 5 (°) | |||||||
| Horizontal growth | 31 | 926 | 900 | 347–1362 | 252 | 0.14 | 0.31 |
| Normal growth | 87 | 679 | 733 | 329–1653 | 238 | Reference | Reference |
| Post rotation growth | 28 | 596 | 625 | 301–1184 | 229 | 0.03 | 0.13 |
| Females | Males | |||||
|---|---|---|---|---|---|---|
| Variable | Slope | 95% Confidence Interval | p-Value | Slope | 95% Confidence Interval | p-Value |
| Anb (°) | −1 | −17 to +16 | 0.94 | −38 | −63 to −14 | 0.002 |
| Divergence (°) | −7 | −15 to +2 | 0.14 | −8 | −23 to +7 | 0.29 |
| Total goniac angle (°) | −10 | −17 to −4 | 0.003 | −1 | −15 to +12 | 0.83 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ceratti, C.; Maspero, C.; Consonni, D.; Caprioglio, A.; Connelly, S.T.; Inchingolo, F.; Tartaglia, G.M. Cone-Beam Computed Tomographic Assessment of the Mandibular Condylar Volume in Different Skeletal Patterns: A Retrospective Study in Adult Patients. Bioengineering 2022, 9, 102. https://doi.org/10.3390/bioengineering9030102
Ceratti C, Maspero C, Consonni D, Caprioglio A, Connelly ST, Inchingolo F, Tartaglia GM. Cone-Beam Computed Tomographic Assessment of the Mandibular Condylar Volume in Different Skeletal Patterns: A Retrospective Study in Adult Patients. Bioengineering. 2022; 9(3):102. https://doi.org/10.3390/bioengineering9030102
Chicago/Turabian StyleCeratti, Chiara, Cinzia Maspero, Dario Consonni, Alberto Caprioglio, Stephen Thaddeus Connelly, Francesco Inchingolo, and Gianluca Martino Tartaglia. 2022. "Cone-Beam Computed Tomographic Assessment of the Mandibular Condylar Volume in Different Skeletal Patterns: A Retrospective Study in Adult Patients" Bioengineering 9, no. 3: 102. https://doi.org/10.3390/bioengineering9030102
APA StyleCeratti, C., Maspero, C., Consonni, D., Caprioglio, A., Connelly, S. T., Inchingolo, F., & Tartaglia, G. M. (2022). Cone-Beam Computed Tomographic Assessment of the Mandibular Condylar Volume in Different Skeletal Patterns: A Retrospective Study in Adult Patients. Bioengineering, 9(3), 102. https://doi.org/10.3390/bioengineering9030102