

A Fully Automated Analysis Pipeline for 4D Flow MRI in the Aorta
 , , ,
, , ,  , , and
, , and
Abstract
1. Introduction
2. Methods
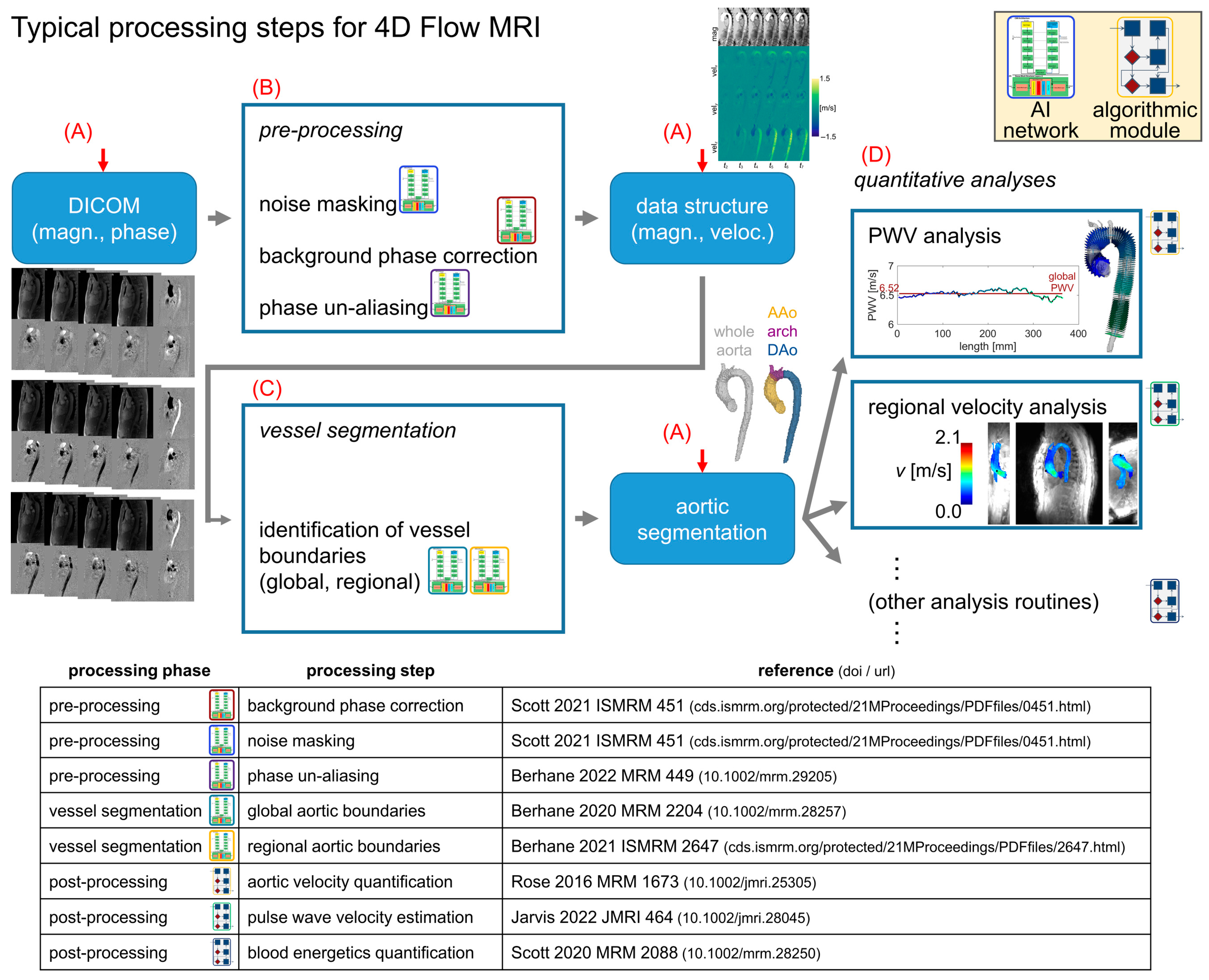
2.1. Analysis Pipeline Architecture for 4D Flow MRI
2.2. Analysis Pipeline for 4D Flow MRI—Processing Tasks
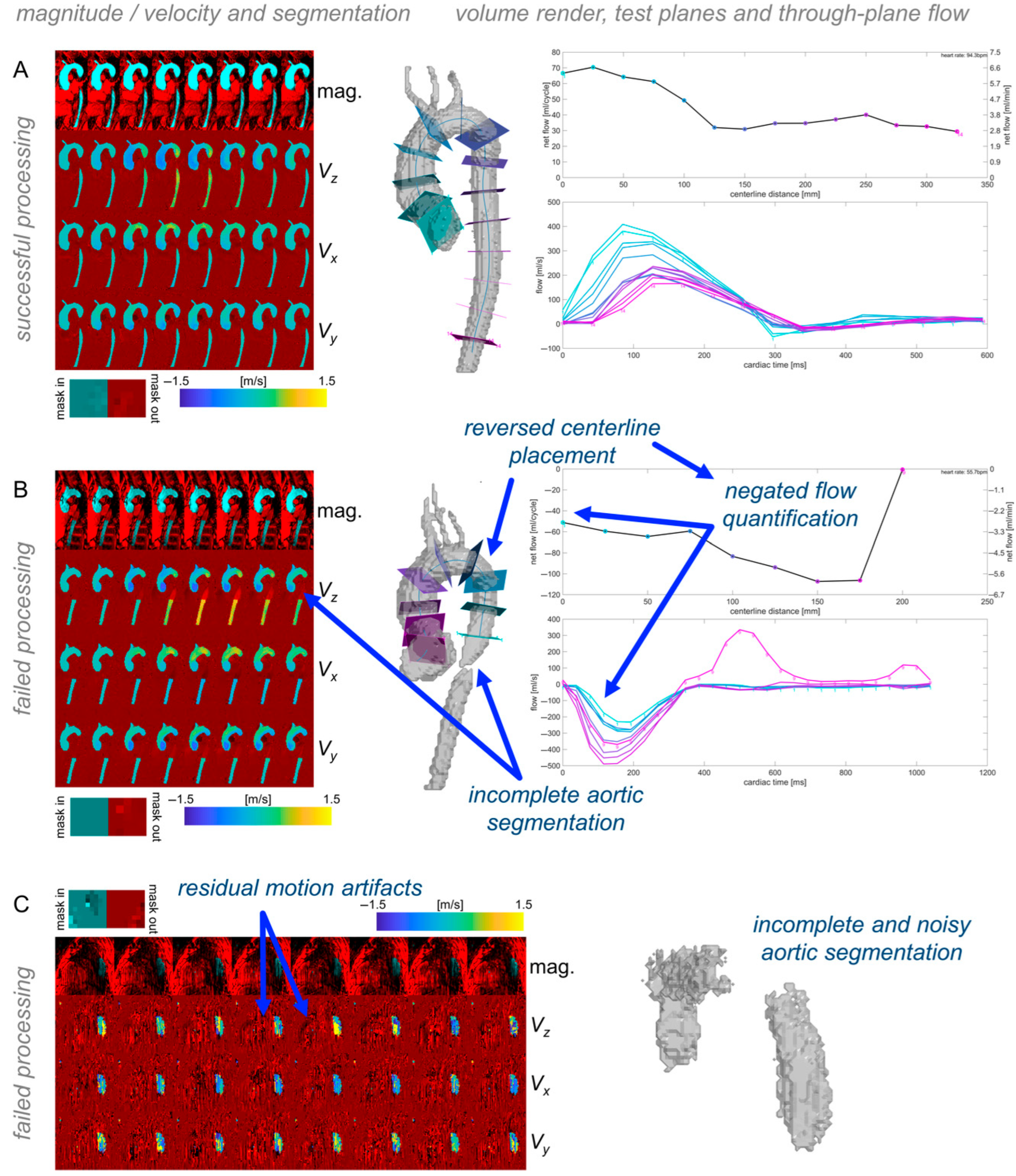
2.3. Analysis Pipeline for 4D Flow MRI—Quality Control
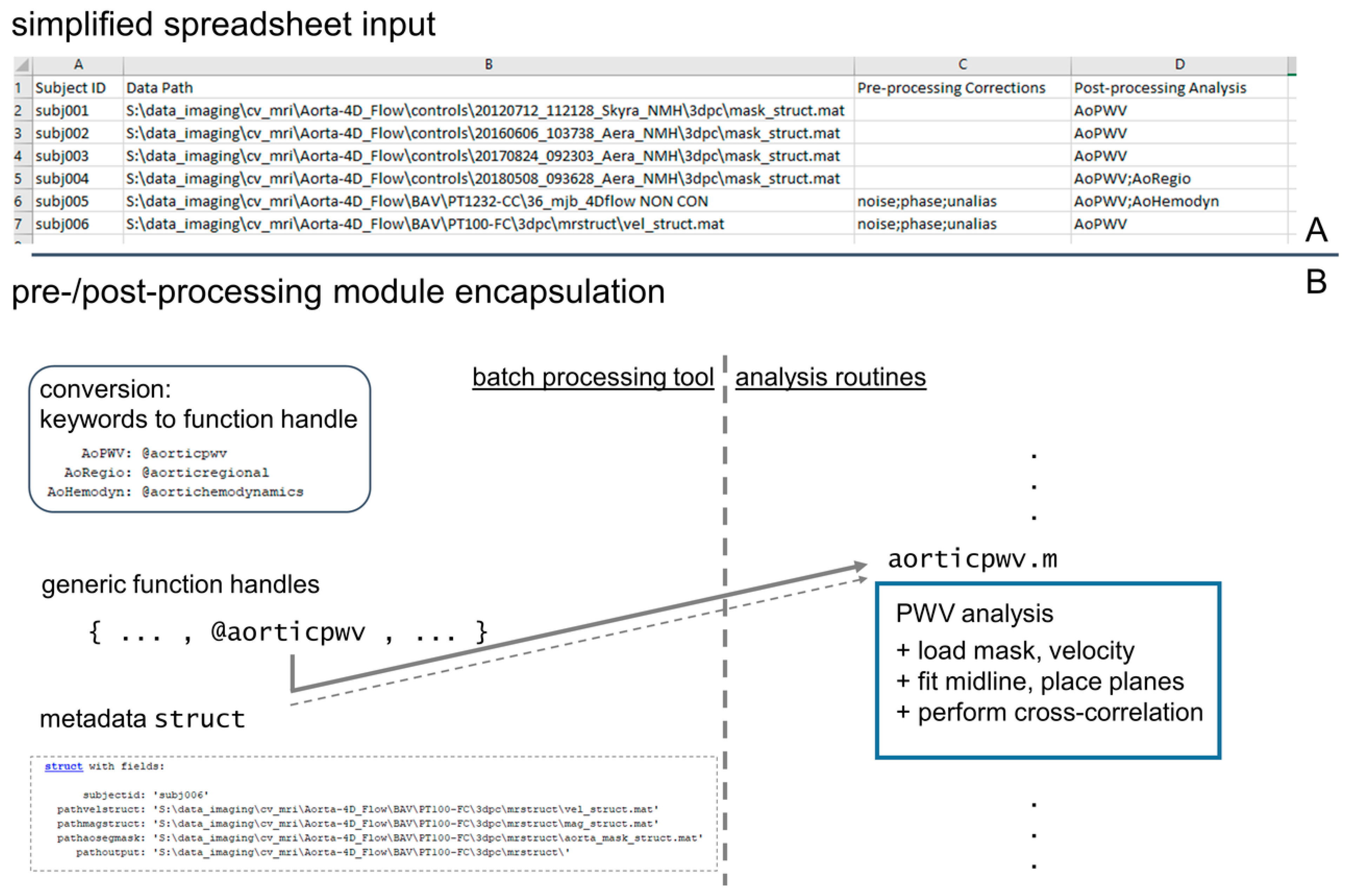
2.4. Technical Implementation of Processing Pipeline
2.5. Study Cohort and Image Acquisition
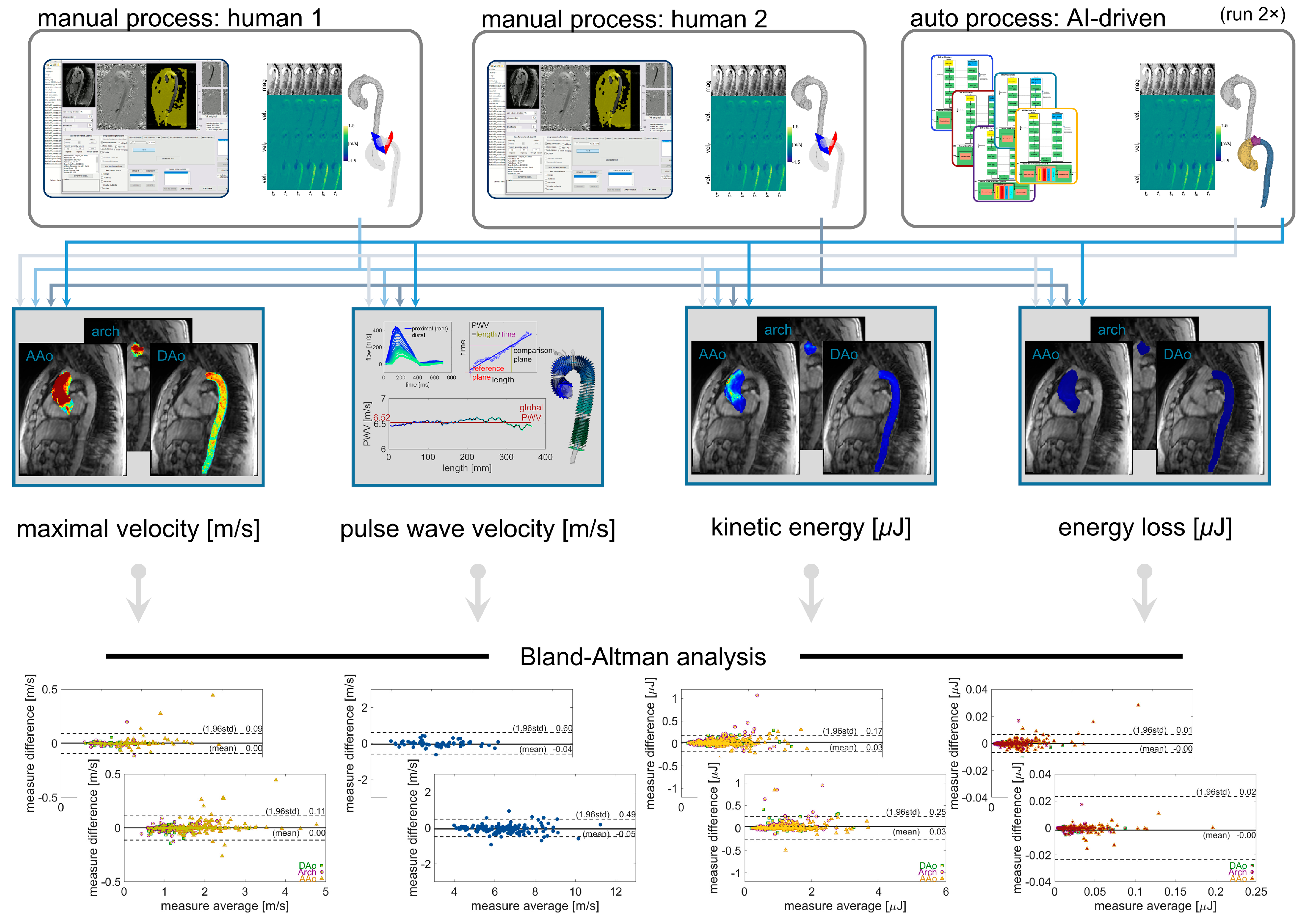
2.6. Study Design and Reference Standards
2.7. Statistics
3. Results
3.1. Study Cohort
3.2. Automated AI-Based Analysis Pipeline Performance—Success Rate and Processing Time
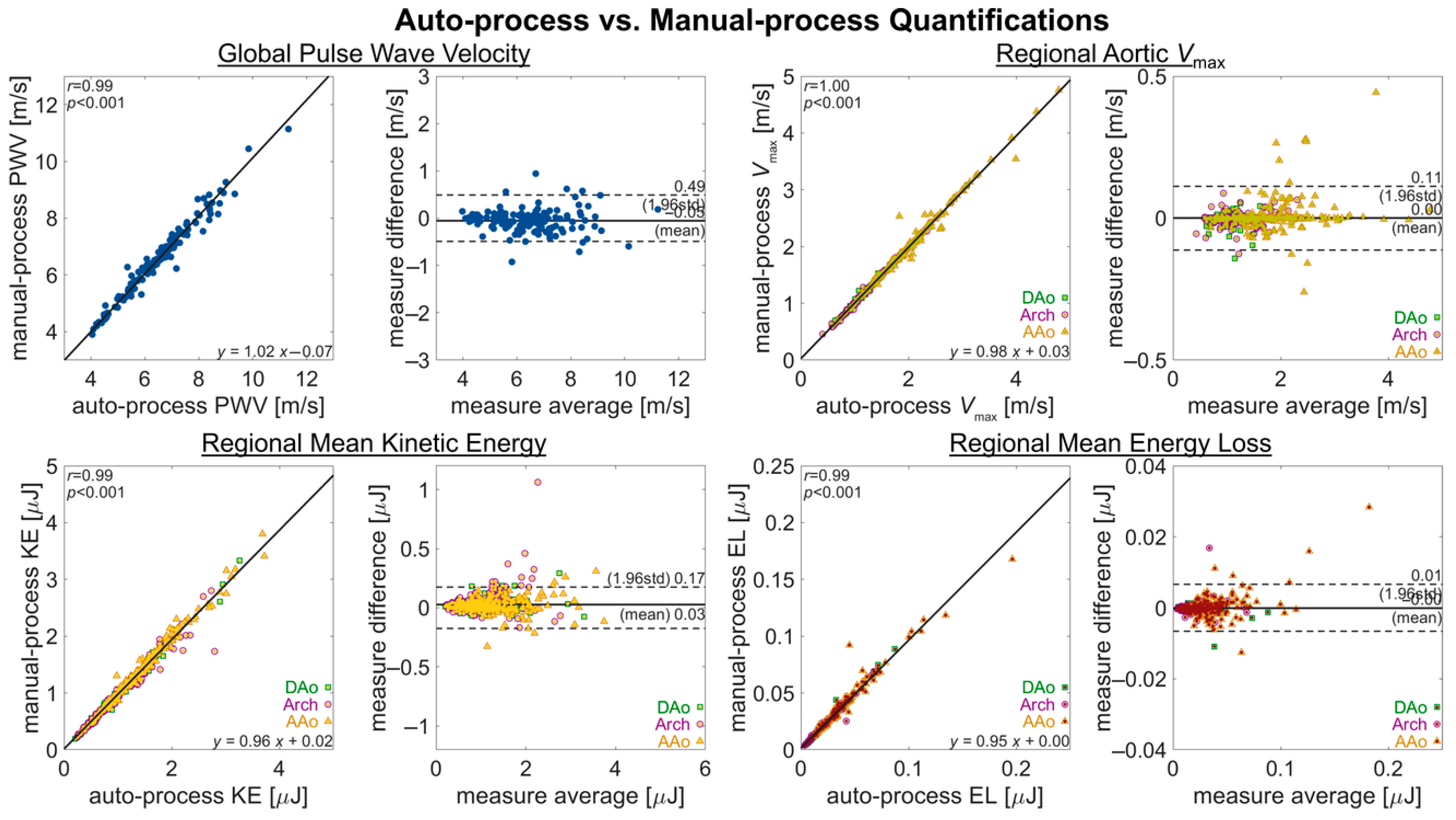
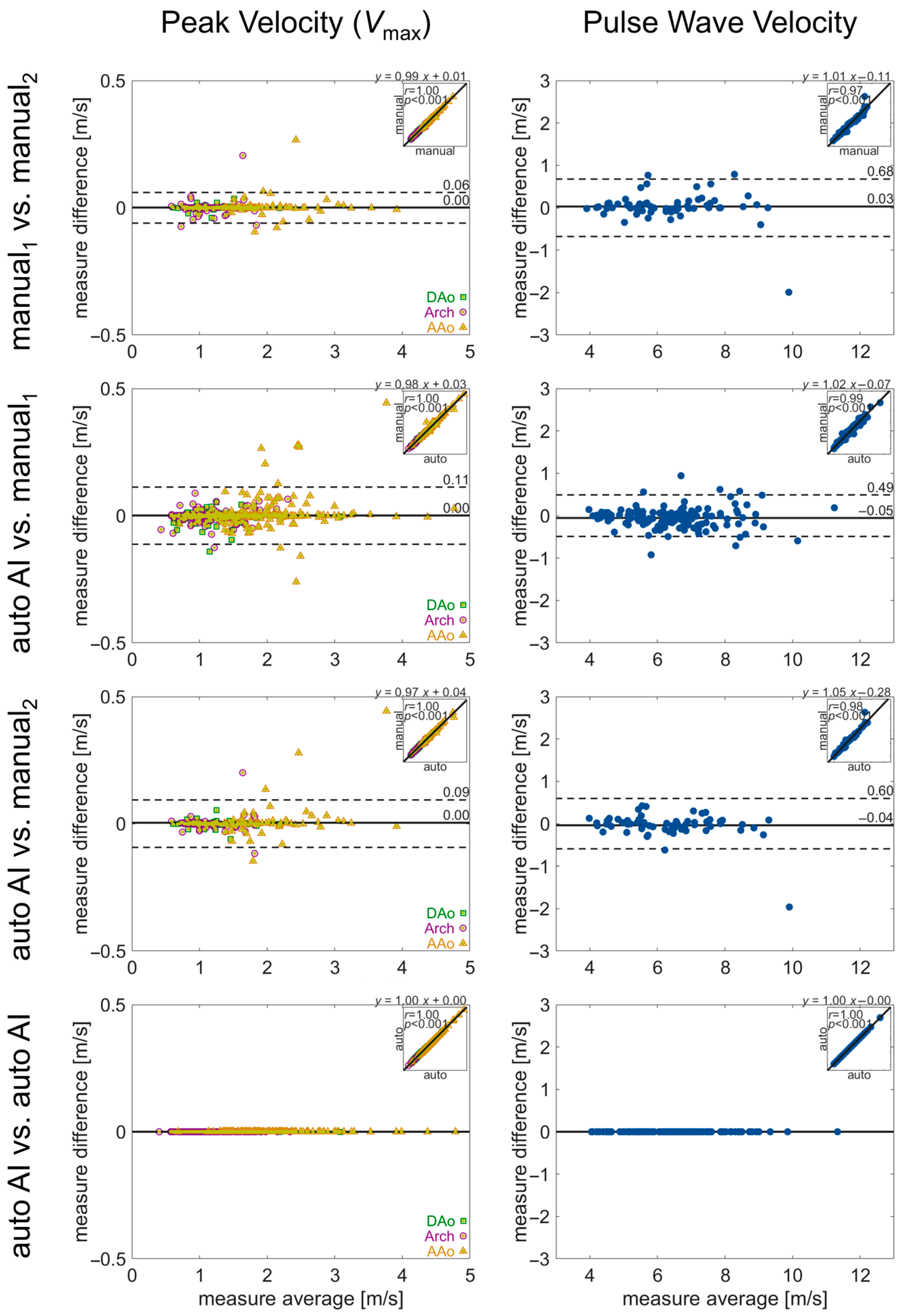
3.3. Automated AI-Based Analysis Pipeline Performance—Hemodynanamic Quantification
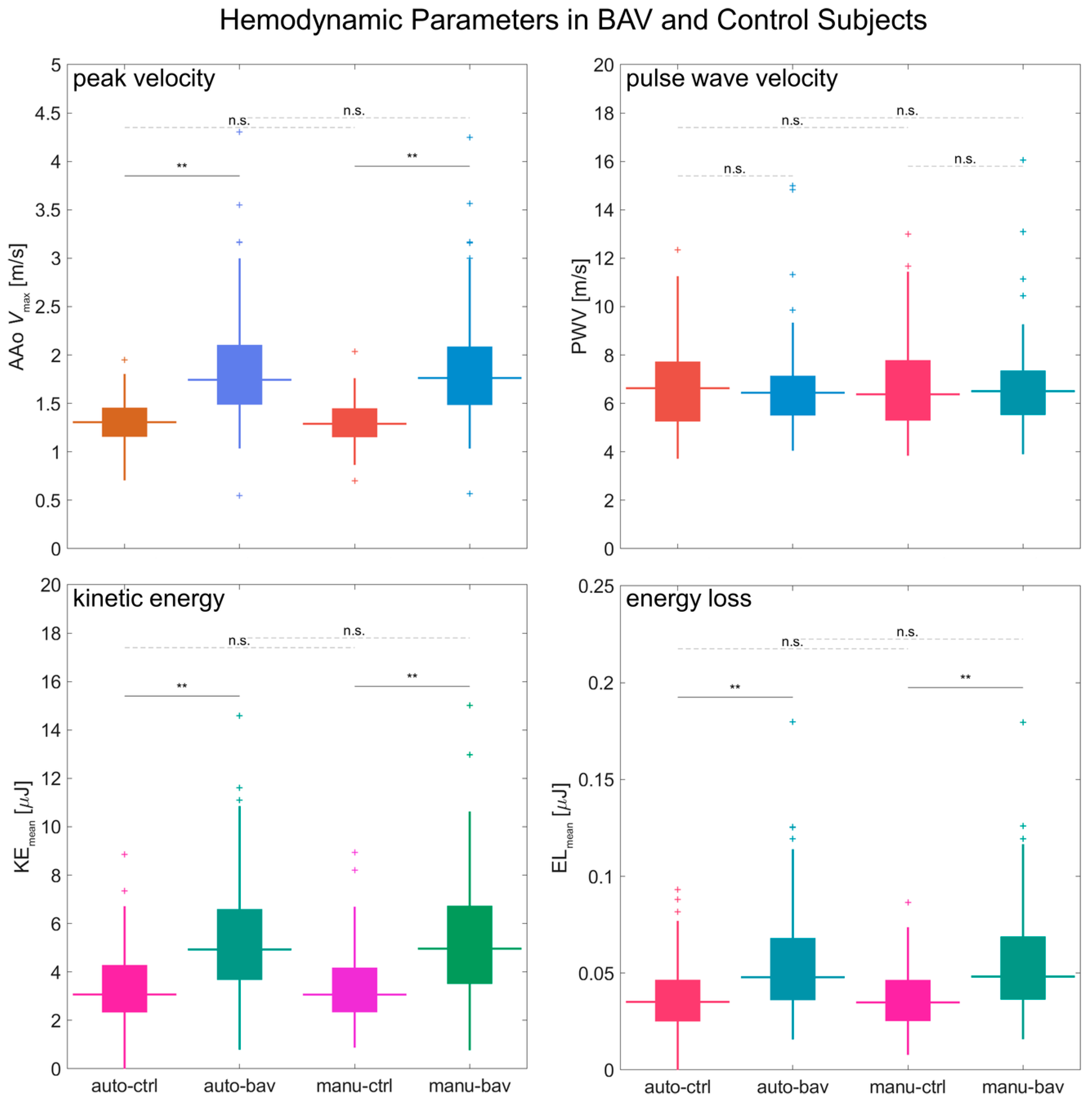
3.4. Automated AI-Based Analysis Pipeline Performance—BAV Patients vs. Controls
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 4D | four-dimensional |
| AAo | ascending aorta |
| AI | artificial intelligence |
| DAo | descending aorta |
| EL | energy loss |
| KE | kinetic energy |
| LDS | Loeys–Dietz syndrome |
| MFS | Marfan syndrome |
| PWV | pulse wave velocity |
| Vmax | maximal or peak velocity |
References
- Rose, M.J.; Jarvis, K.; Chowdhary, V.; Barker, A.J.; Allen, B.D.; Robinson, J.D.; Markl, M.; Rigsby, C.K.; Schnell, S. Efficient method for volumetric assessment of peak blood flow velocity using 4D flow MRI: Peak Velocity Assessment With 4D Flow. J. Magn. Reson. Imaging 2016, 44, 1673–1682. [Google Scholar] [CrossRef]
- Garcia, J.; Barker, A.J.; Markl, M. The Role of Imaging of Flow Patterns by 4D Flow MRI in Aortic Stenosis. JACC Cardiovasc. Imaging 2019, 12, 252–266. [Google Scholar] [CrossRef]
- Bollache, E.; Barker, A.J.; Dolan, R.S.; Carr, J.C.; van Ooij, P.; Ahmadian, R.; Powell, A.; Collins, J.D.; Geiger, J.; Markl, M. k-t accelerated aortic 4D flow MRI in under two minutes: Feasibility and impact of resolution, k-space sampling patterns, and respiratory navigator gating on hemodynamic measurements. Magn. Reson. Med. 2018, 79, 195–207. [Google Scholar] [CrossRef]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P.; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease. J. Am. Coll. Cardiol. 2021, 77, e25–e197. [Google Scholar] [CrossRef]
- Cavalcante, J.L.; Lima, J.A.C.; Redheuil, A.; Al-Mallah, M.H. Aortic Stiffness. J. Am. Coll. Cardiol. 2011, 57, 1511–1522. [Google Scholar] [CrossRef]
- Humphrey, J.D.; Tellides, G. Central artery stiffness and thoracic aortopathy. Am. J. Physiol.-Heart Circ. Physiol. 2019, 316, H169–H182. [Google Scholar] [CrossRef]
- Bock, J.; Kreher, B.; Hennig, J.; Markl, M. Optimized pre-processing of time-resolved 2D and 3D phase contrast MRI data. In Proceedings of the 15th Annual Meeting of ISMRM, Berlin, Germany, 18–25 May 2007. [Google Scholar]
- Berhane, H.; Scott, M.; Elbaz, M.; Jarvis, K.; McCarthy, P.; Carr, J.; Malaisrie, C.; Avery, R.; Barker, A.J.; Robinson, J.D.; et al. Fully automated 3D aortic segmentation of 4D flow MRI for hemodynamic analysis using deep learning. Magn. Reson. Med. 2020, 84, 2204–2218. [Google Scholar] [CrossRef]
- Sodhi, A.; Brown, N.K.; Robinson, J.D.; Popescu, A.R.; Markl, M.; Rigsby, C.K. Going with the flow: Implementing a 4D flow MRI program at a children’s hospital. Pediatr. Radiol. 2024, 14. [Google Scholar] [CrossRef]
- Oechtering, T.H.; Nowak, A.; Sieren, M.M.; Stroth, A.M.; Kirschke, N.; Wegner, F.; Balks, M.; König, I.R.; Jin, N.; Graessner, J.; et al. Repeatability and reproducibility of various 4D Flow MRI postprocessing software programs in a multi-software and multi-vendor cross-over comparison study. J. Cardiovasc. Magn. Reson. 2023, 25, 22. [Google Scholar] [CrossRef]
- Scott, M.B.; Berhane, H.; Baraboo, J.; Rigsby, C.K.; Robinson, J.D.; McCarthy, P.M.; Malaisrie, S.C.; Avery, R.J.; Allen, B.D.; Barker, A.; et al. Fully automated aortic 4D flow MRI large-cohort analysis using deep learning. In Proceedings of the ISMRM, Online, 15–20 May 2021; p. 451. [Google Scholar]
- You, S.; Masutani, E.M.; Alley, M.T.; Vasanawala, S.S.; Taub, P.R.; Liau, J.; Roberts, A.C.; Hsiao, A. Deep Learning Automated Background Phase Error Correction for Abdominopelvic 4D Flow MRI. Radiology 2022, 302, 584–592. [Google Scholar] [CrossRef]
- Peper, E.S.; van Ooij, P.; Jung, B.; Huber, A.; Gräni, C.; Bastiaansen, J.A.M. Advances in machine learning applications for cardiovascular 4D flow MRI. Front. Cardiovasc. Med. 2022, 9, 1052068. [Google Scholar] [CrossRef]
- Bustamante, M.; Viola, F.; Engvall, J.; Carlhäll, C.; Ebbers, T. Automatic Time-Resolved Cardiovascular Segmentation of 4D Flow MRI Using Deep Learning. Magn. Reson. Imaging 2023, 57, 191–203. [Google Scholar] [CrossRef]
- Marin-Castrillon, D.M.; Lalande, A.; Leclerc, S.; Ambarki, K.; Morgant, M.C.; Cochet, A.; Lin, S.; Bouchot, O.; Boucher, A.; Presles, B. 4D segmentation of the thoracic aorta from 4D flow MRI using deep learning. Magn. Reson. Imaging 2023, 99, 20–25. [Google Scholar] [CrossRef]
- Berhane, H.; Scott, M.; Baraboo, J.; Rigsby, C.; Robinson, J.; Allen, B.; Malaisrie, C.; McCarthy, P.; Avery, R.; Markl, M. Deep Learning based Automatic Multi-Regional Segmentation of the Aorta form 4D Flow MRI. In Proceedings of the ISMRM, 15–20 May 2021; p. 2647. [Google Scholar]
- Berhane, H.; Scott, M.B.; Barker, A.J.; McCarthy, P.; Avery, R.; Allen, B.; Malaisrie, C.; Robinson, J.D.; Rigsby, C.K.; Markl, M. Deep learning–based velocity antialiasing of 4D-flow MRI. Magn. Reson. Med. 2022, 88, 449–463. [Google Scholar] [CrossRef]
- Barker, A.J.; van Ooij, P.; Bandi, K.; Garcia, J.; Albaghdadi, M.; McCarthy, P.; Bonow, R.O.; Carr, J.; Collins, J.; Malaisrie, S.C.; et al. Viscous energy loss in the presence of abnormal aortic flow. Magn. Reson. Med. 2014, 72, 620–628. [Google Scholar] [CrossRef]
- Scott, M.B.; Huh, H.; van Ooij, P.; Chen, V.; Herrera, B.; Elbaz, M.; McCarthy, P.; Malaisrie, S.C.; Carr, J.; Fedak, P.W.M.; et al. Impact of age, sex, and global function on normal aortic hemodynamics. Magn. Reson. Med. 2020, 84, 2088–2102. [Google Scholar] [CrossRef]
- Jarvis, K.; Soulat, G.; Scott, M.; Vali, A.; Pathrose, A.; Syed, A.A.; Kinno, M.; Prabhakaran, S.; Collins, J.D.; Markl, M. Investigation of Aortic Wall Thickness, Stiffness and Flow Reversal in Patients with Cryptogenic Stroke: A 4D Flow MRI Study. J. Magn. Reson. Imaging 2020, 53, 942–952. [Google Scholar] [CrossRef]
- Jarvis, K.; Pruijssen, J.T.; Son, A.Y.; Allen, B.D.; Soulat, G.; Vali, A.; Barker, A.J.; Hoel, A.W.; Eskandari, M.K.; Malaisrie, S.C.; et al. Parametric Hemodynamic 4D Flow MRI Maps for the Characterization of Chronic Thoracic Descending Aortic Dissection. Magn. Reson. Imaging 2020, 51, 1357–1368. [Google Scholar] [CrossRef]
- Griswold, M.A.; Jakob, P.M.; Heidemann, R.M.; Nittka, M.; Jellus, V.; Wang, J.; Kiefer, B.; Haase, A. Generalized autocalibrating partially parallel acquisitions (GRAPPA). Magn. Reson. Med. 2002, 47, 1202–1210. [Google Scholar] [CrossRef]
- Lustig, M.; Donoho, D.; Pauly, J.M. Sparse MRI: The application of compressed sensing for rapid MR imaging. Magn. Reson. Reson. Med. 2007, 58, 1182–1195. [Google Scholar] [CrossRef]
- Schrauben, E.; Wåhlin, A.; Ambarki, K.; Spaak, E.; Malm, J.; Wieben, O.; Eklund, A. Fast 4D flow MRI intracranial segmentation and quantification in tortuous arteries. Magn. Reson. Imaging 2015, 42, 1458–1464. [Google Scholar] [CrossRef]
- Rothenberger, S.M.; Patel, N.M.; Zhang, J.; Schnell, S.; Craig, B.A.; Ansari, S.A.; Markl, M.; Vlachos, P.P.; Rayz, V.L. Automatic 4D Flow MRI Segmentation Using the Standardized Difference of Means Velocity. IEEE Trans. Med. Imaging 2023, 42, 2360–2373. [Google Scholar] [CrossRef]
- Johnson, E.M.I.; Berhane, H.; Andrae, J.; Strecker, C.; Mast, H.; Horst, U.; Markl, M.; Harloff, A. Fully Automated Segmentation and Hemodynamic Quantification of Carotid Artery 4D Flow MRI. In Proceedings of the ISMRM, Hololulu, HI, USA, 10–15 May 2025; p. 1215. [Google Scholar]
- Rodríguez-Palomares, J.F.; Dux-Santoy, L.; Guala, A.; Kale, R.; Maldonado, G.; Teixidó-Turà, G.; Galian, L.; Huguet, M.; Valente, F.; Gutiωrrez, L.; et al. Aortic flow patterns and wall shear stress maps by 4D-flow cardiovascular magnetic resonance in the assessment of aortic dilatation in bicuspid aortic valve disease. J. Cardiovasc. Magn. Reson. 2018, 20, 28. [Google Scholar] [CrossRef]
- Pascaner, A.F.; Houriez--Gombaud-Saintonge, S.; Craiem, D.; Gencer, U.; Casciaro, M.E.; Charpentier, E.; Bouaou, K.; De Cesare, A.; Dietenbeck, T.; Chenoune, Y.; et al. Comprehensive assessment of local and regional aortic stiffness in patients with tricuspid or bicuspid aortic valve aortopathy using magnetic resonance imaging. Int. J. Cardiol. 2021, 326, 206–212. [Google Scholar] [CrossRef]
- Johnson, E.M.I.; Scott, M.B.; Jarvis, K.; Allen, B.; Carr, J.; Malaisrie, S.C.; McCarthy, P.; Mehta, C.; Fedak, P.W.; Barker, A.J.; et al. Global Aortic Pulse Wave Velocity is Unchanged in Bicuspid Aortopathy With Normal Valve Function but Elevated in Patients With Aortic Valve Stenosis: Insights From a 4D Flow MRI Study of 597 Subjects. Magn. Reson. Imaging 2022, 57, 126–136. [Google Scholar] [CrossRef]
- Loudon, M.; Bissell, M.M.; Dyverfeldt, P.; Carlhall, C.J.; Ebbers, T.; Hess, A.T.; Prendergast, B.D.; Neubauer, S.; Myerson, S.G. Turbulent kinetic energy in the ascending aorta is greater in bicuspid than tricuspid aortic valve stenosis. J. Cardiovasc. Magn. Reson. 2015, 17, O88. [Google Scholar] [CrossRef]
- Seaman, C.; George Akingba, A.; Sucosky, P. Steady Flow Hemodynamic and Energy Loss Measurements in Normal and Simulated Calcified Tricuspid and Bicuspid Aortic Valves. J. Biomech. Eng. 2014, 136, 041001. [Google Scholar] [CrossRef]
- Isselbacher, E.M.; Preventza, O.; Hamilton Black, I.I.I.J.; Augoustides, J.G.; Beck, A.W.; Bolen, M.A.; Braverman, A.C.; Bray, B.E.; Brown-Zimmerman, M.M.; Chen, E.P.; et al. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease. J. Am. Coll. Cardiol. 2022, 80, e223–e393. [Google Scholar] [CrossRef]
- Guzzardi, D.G.; Barker, A.J.; van Ooij, P.; Malaisrie, S.C.; Puthumana, J.J.; Belke, D.D.; Mewhort, H.E.M.; Svystonyuk, D.A.; Kang, S.; Verma, S.; et al. Valve-Related Hemodynamics Mediate Human Bicuspid Aortopathy. J. Am. Coll. Cardiol. 2015, 66, 892–900. [Google Scholar] [CrossRef]
- Bollache, E.; Guzzardi, D.G.; Sattari, S.; Olsen, K.E.; Di Martino, E.S.; Malaisrie, S.C.; van Ooij, P.; Collins, J.; Carr, J.; McCarthy, P.M.; et al. Aortic valve-mediated wall shear stress is heterogeneous and predicts regional aortic elastic fiber thinning in bicuspid aortic valve-associated aortopathy. J. Thorac. Cardiovasc. Surg. 2018, 156, 2112–2120.e2. [Google Scholar] [CrossRef]
- Soulat, G.; Scott, M.B.; Allen, B.D.; Avery, R.; Bonow, R.O.; Malaisrie, S.C.; McCarthy, P.; Fedak, P.W.; Barker, A.J.; Markl, M. Association of Regional Wall Shear Stress and Progressive Ascending Aorta Dilation in Bicuspid Aortic Valve. JACC Cardiovasc. Imaging 2022, 15, 33–42. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Subjects | Age (Mean ± Std.) [Years] | Sex (%) [Female] | ||
|---|---|---|---|---|
| entire cohort | healthy control | 147 | 51.6 ± 16.9 | 60 (40.8%) |
| bicuspid aortic valve | 147 | 47.4 ± 12.5 | 32 (21.8%) | |
| aortic valve prosthesis | 10 | 50.9 ± 11.3 | 2 (20.0%) | |
| connective tissue disorder | 75 | 16.0 ± 4.3 | 28 (37.3%) | |
| sub-cohort | ||||
| healthy control | 101 | 46.4 ± 15.5 | 51 (50.5%) | |
| bicuspid aortic valve | 147 | 47.4 ± 12.5 | 32 (21.8%) |
| Total | Included | Excluded | |||
|---|---|---|---|---|---|
| healthy control | 147 | 146 | (99%) | 1 | (1%) |
| bicuspid aortic valve | 147 | 143 | (97%) | 4 | (3%) |
| aortic valve prosthesis | 10 | 10 | (100%) | 0 | (0%) |
| pediatric Marfan | 62 | 55 | (89%) | 7 | (11%) |
| pediatric Loeys-Dietz | 11 | 9 | (82%) | 2 | (18%) |
| pediatric Ehler-Danlos | 2 | 2 | (100%) | 0 | (0%) |
| all groups | 379 | 365 | (96%) | 14 | (4%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Johnson, E.M.I.; Berhane, H.; Weiss, E.; Jarvis, K.; Sodhi, A.; Yang, K.; Robinson, J.D.; Rigsby, C.K.; Allen, B.D.; Markl, M. A Fully Automated Analysis Pipeline for 4D Flow MRI in the Aorta. Bioengineering 2025, 12, 807. https://doi.org/10.3390/bioengineering12080807
Johnson EMI, Berhane H, Weiss E, Jarvis K, Sodhi A, Yang K, Robinson JD, Rigsby CK, Allen BD, Markl M. A Fully Automated Analysis Pipeline for 4D Flow MRI in the Aorta. Bioengineering. 2025; 12(8):807. https://doi.org/10.3390/bioengineering12080807
Chicago/Turabian StyleJohnson, Ethan M. I., Haben Berhane, Elizabeth Weiss, Kelly Jarvis, Aparna Sodhi, Kai Yang, Joshua D. Robinson, Cynthia K. Rigsby, Bradley D. Allen, and Michael Markl. 2025. "A Fully Automated Analysis Pipeline for 4D Flow MRI in the Aorta" Bioengineering 12, no. 8: 807. https://doi.org/10.3390/bioengineering12080807
APA StyleJohnson, E. M. I., Berhane, H., Weiss, E., Jarvis, K., Sodhi, A., Yang, K., Robinson, J. D., Rigsby, C. K., Allen, B. D., & Markl, M. (2025). A Fully Automated Analysis Pipeline for 4D Flow MRI in the Aorta. Bioengineering, 12(8), 807. https://doi.org/10.3390/bioengineering12080807