


Leukocyte-Rich Platelet-Rich Plasma’s Clinical Effectiveness in Arthroscopic Rotator Cuff Repair: A Meta-Analysis of Randomized Controlled Trials

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction and Quality Assessment
2.4. Grading the Evidence
2.5. Statistical Analyses
3. Results
3.1. Search Results
3.2. Study Characteristics
3.3. Quality Evaluation
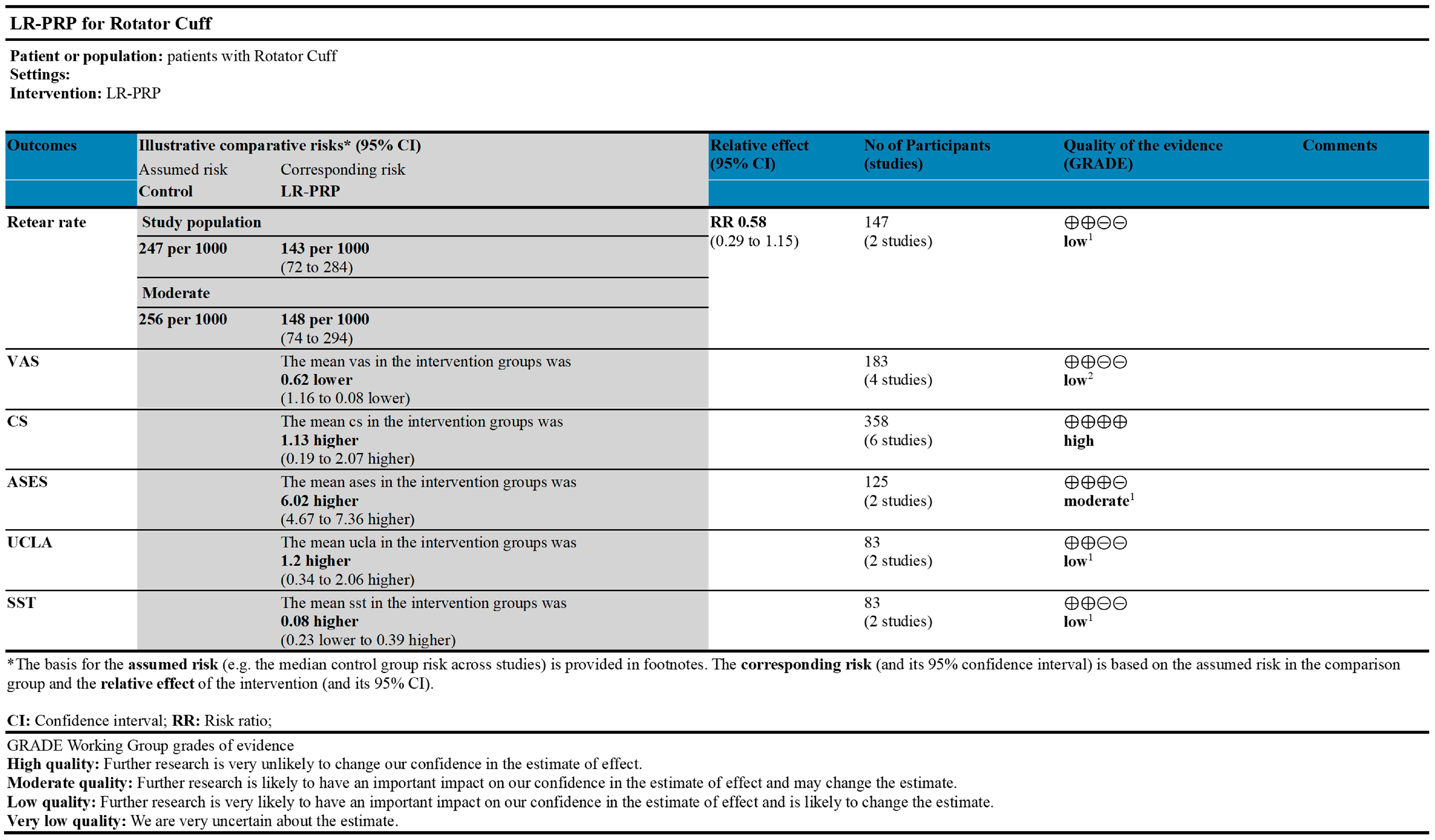
3.4. GRADE Results
3.5. Results of Meta-Analysis
3.5.1. Constant Score
3.5.2. Visual Analog Scale
3.5.3. Other Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PRP | Platelet-rich plasma |
| LR | Leukocyte-rich |
| CS | Constant Score |
| VAS | Visual Analog Scale |
| ASES | American Shoulder and Elbow Surgeons score |
| UCLA | University of California, Los Angeles score |
| SST | Simple Shoulder Test |
References
- Teunis, T.; Lubberts, B.; Reilly, B.T.; Ring, D. A systematic review and pooled analysis of the prevalence of rotator cuff disease with increasing age. J. Shoulder Elb. Surg. 2014, 23, 1913–1921. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R.S. Abnormal findings on magnetic resonance images of asymptomatic shoulders. J. Bone Jt. Surg. Am. 1996, 78, 633. [Google Scholar] [CrossRef]
- Arce, G.; Bak, K.; Bain, G.; Calvo, E.; Ejnisman, B.; Di Giacomo, G.; Gutierrez, V.; Guttmann, D.; Itoi, E.; Ben Kibler, W.; et al. Management of disorders of the rotator cuff: Proceedings of the ISAKOS upper extremity committee consensus meeting. Arthroscopy 2013, 29, 1840–1850. [Google Scholar] [CrossRef]
- Giuseppe, M.; Niccolò, V.; Giuseppe, F.; Maristella, F.S. Rationale of Tendon-to-Bone Healing. In Fundamentals of the Shoulder; Springer International Publishing: Cham, Switzerland, 2022; pp. 61–74. [Google Scholar]
- Kirschner, J.S.; Cheng, J.; Hurwitz, N.; Santiago, K.; Lin, E.; Beatty, N.; Kingsbury, D.; Wendel, I.; Milani, C. Ultrasound-guided percutaneous needle tenotomy (PNT) alone versus PNT plus platelet-rich plasma injection for the treatment of chronic tendinosis: A randomized controlled trial. PmR 2021, 13, 1340–1349. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E.; Sánchez, M.; Nurden, A.T.; Nurden, P.; Orive, G.; Andía, I. New insights into and novel applications for platelet-rich fibrin therapies. Trends Biotechnol. 2006, 24, 227–234. [Google Scholar] [CrossRef]
- Zhang, C.; Wu, J.; Li, X.; Wang, Z.; Lu, W.W.; Wong, T.-M. Current Biological Strategies to Enhance Surgical Treatment for Rotator Cuff Repair. Front. Bioeng. Biotechnol. 2021, 9, 657584. [Google Scholar] [CrossRef]
- Dohan Ehrenfest, D.M.; Rasmusson, L.; Albrektsson, T. Classification of platelet concentrates: From pure platelet-rich plasma (P-PRP) to leucocyte- and platelet-rich fibrin (L-PRF). Trends Biotechnol. 2009, 27, 158–167. [Google Scholar] [CrossRef]
- Sánchez, M.; Anitua, E.; Orive, G.; Mujika, I.; Andia, I. Platelet-rich therapies in the treatment of orthopaedic sport injuries. Sports Med. 2009, 39, 345–354. [Google Scholar] [CrossRef]
- Andia, I.; Sanchez, M.; Maffulli, N. Tendon healing and platelet-rich plasma therapies. Expert. Opin. Biol. Ther. 2010, 10, 1415–1426. [Google Scholar] [CrossRef]
- Rodeo, S.A.; Delos, D.; Williams, R.J.; Adler, R.S.; Pearle, A.; Warren, R.F. The effect of platelet-rich fibrin matrix on rotator cuff tendon healing: A prospective, randomized clinical study. Am. J. Sports Med. 2012, 40, 1234–1241. [Google Scholar] [CrossRef]
- Zhou, S.-F.; Estrera, A.L.; Miller, C.C.; Ignacio, C.; Panthayi, S.; Loubser, P.; Sagun, D.L.; Sheinbaum, R.; Safi, H.J. Analysis of autologous platelet-rich plasma during ascending and transverse aortic arch surgery. Ann. Thorac. Surg. 2013, 95, 1525–1530. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, ED000142. [Google Scholar] [CrossRef] [PubMed]
- Tang, P.; Wen, T.; Lu, W.; Jin, H.; Pan, L.; Li, H.; Zeng, B.; Zhou, Y.; Xiao, W.; Li, Y. The efficacy of extracorporeal shock wave therapy for knee osteoarthritis: An umbrella review. Int. J. Surg. 2024, 110, 2389–2395. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [PubMed]
- Castricini, R.; Longo, U.G.; De Benedetto, M.; Panfoli, N.; Pirani, P.; Zini, R.; Maffulli, N.; Denaro, V. Platelet-rich plasma augmentation for arthroscopic rotator cuff repair: A randomized controlled trial. Am. J. Sport. Med. 2011, 39, 258–265. [Google Scholar] [CrossRef]
- Randelli, P.; Arrigoni, P.; Ragone, V.; Aliprandi, A.; Cabitza, P. Platelet rich plasma in arthroscopic rotator cuff repair: A prospective RCT study, 2-year follow-up. J. Shoulder Elb. Surg. 2011, 20, 518–528. [Google Scholar] [CrossRef]
- Zhang, Z.; Wang, Y.; Sun, J. The effect of platelet-rich plasma on arthroscopic double-row rotator cuff repair: A clinical study with 12-month follow-up. Acta Orthop. Traumatol. Turc. 2016, 50, 191–197. [Google Scholar] [CrossRef]
- Snow, M.; Hussain, F.; Pagkalos, J.; Kowalski, T.; Green, M.; Massoud, S.; James, S. The Effect of Delayed Injection of Leukocyte-Rich Platelet-Rich Plasma Following Rotator Cuff Repair on Patient Function: A Randomized Double-Blind Controlled Trial. Arthroscopy 2020, 36, 648–657. [Google Scholar] [CrossRef] [PubMed]
- Randelli, P.S.; Stoppani, C.A.; Santarsiero, G.; Nocerino, E.; Menon, A. Platelet-Rich Plasma in Arthroscopic Rotator Cuff Repair: Clinical and Radiological Results of a Prospective Randomized Controlled Trial Study at 10-Year Follow-Up. Arthroscopy 2022, 38, 51–61. [Google Scholar] [CrossRef] [PubMed]
- D’Ambrosi, R.; Palumbo, F.; Paronzini, A.; Ragone, V.; Facchini, R.M. Platelet-rich plasma supplementation in arthroscopic repair of full-thickness rotator cuff tears: A randomized clinical trial. Musculoskelet. Surg. 2016, 100 (Suppl. S1), 25–32. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Li, T.; Li, J.; Tang, X.; Li, R.; Xiong, Y. Platelet-Rich Plasma Has Better Results for Retear Rate, Pain, and Outcome Than Platelet-Rich Fibrin After Rotator Cuff Repair: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Arthroscopy 2022, 38, 539–550. [Google Scholar] [CrossRef]
- Xu, W.; Xue, Q. Application of Platelet-Rich Plasma in Arthroscopic Rotator Cuff Repair: A Systematic Review and Meta-analysis. Orthop. J. Sports Med. 2021, 9, 23259671211016847. [Google Scholar] [CrossRef]
- Yang, F.A.; Liao, C.D.; Wu, C.W.; Shih, Y.C.; Wu, L.C.; Chen, H.C. Effects of applying platelet-rich plasma during arthroscopic rotator cuff repair: A systematic review and meta-analysis of randomised controlled trials. Sci. Rep. 2020, 10, 17171. [Google Scholar] [CrossRef]
- Feltri, P.; Gonalba, G.C.; Boffa, A.; Candrian, C.; Menon, A.; Randelli, P.S.; Filardo, G. Platelet-rich plasma does not improve clinical results in patients with rotator cuff disorders but reduces the retear rate. A systematic review and meta-analysis. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 1940–1952. [Google Scholar] [CrossRef]
- Cai, Y.Z.; Zhang, C.; Lin, X.J. Efficacy of platelet-rich plasma in arthroscopic repair of full-thickness rotator cuff tears: A meta-analysis. J. Shoulder Elb. Surg. 2015, 24, 1852–1859. [Google Scholar] [CrossRef]
- Zhao, J.G.; Zhao, L.; Jiang, Y.X.; Wang, Z.L.; Wang, J.; Zhang, P. Platelet-rich plasma in arthroscopic rotator cuff repair: A meta-analysis of randomized controlled trials. Arthroscopy 2015, 31, 125–135. [Google Scholar] [CrossRef]
- Andia, I.; Martin, J.I.; Maffulli, N. Platelet-rich Plasma and Mesenchymal Stem Cells: Exciting, But … are we there Yet? Sports Med. Arthrosc. Rev. 2018, 26, 59–63. [Google Scholar] [CrossRef]
- Hersant, B.; SidAhmed-Mezi, M.; Bosc, R.; Meningaud, J.-P. Autologous Platelet-Rich Plasma/Thrombin Gel Combined with Split-Thickness Skin Graft to Manage Postinfectious Skin Defects: A Randomized Controlled Study. Adv. Skin. Wound Care 2017, 30, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Kuffler, D.P. Platelet-Rich Plasma Promotes Axon Regeneration, Wound Healing, and Pain Reduction: Fact or Fiction. Mol. Neurobiol. 2015, 52, 990–1014. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Middleton, K.K.; Fu, F.H.; Im, H.-J.; Wang, J.H.C. HGF mediates the anti-inflammatory effects of PRP on injured tendons. PLoS ONE 2013, 8, e67303. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Sample Size | Age | Gender | Tear Size | Follow-Up (M) | Level of Evidence | Outcomes | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| LR-PRP | Control | LR-PRP | Control | Man | Woman | ||||||
| Castricini, R [19] | 2011 | 43 | 45 | 55.5 ± 7.8 | 55.2 ± 8.0 | 40 | 48 | Small to Moderate | 20 | II | CS |
| Randelli, P [20] | 2011 | 22 | 23 | 61.6 ± 8.3 | 59.5 ± 10.7 | 21 | 24 | Small to Moderate | 24 | II | VAS, CS, UCLA, SST |
| Zhang Z [21] | 2016 | 30 | 30 | 57.2 ± 7.4 | 56.9 ± 6.0 | 31 | 29 | Small (<1 cm) | 12 | II | VAS, CS |
| D’Ambrosi, R [24] | 2016 | 20 | 20 | 57.9 ± 8.7 | 62.0 ± 10.0 | 19 | 21 | Small to Moderate | 6 | II | VAS, CS |
| Snow M [22] | 2020 | 40 | 47 | 59.8 ± 7.37 | 62.6 ± 7.37 | 46 | 41 | Moderate (1–3 cm) | 12 | II | CS, ASES |
| Randelli PS [23] | 2022 | 17 | 21 | 61.5 ± 3.3 | 61.56 ± 8.24 | 23 | 15 | Small to Moderate | 120 | II | VAS, CS, UCLA, ASES, SST |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tang, P.; Huang, M.; Xiao, W.; Wen, T.; Volotovsky, P.; Gerasimenko, M.; Chu, S.; Liu, S.; Zhang, K.; Li, Y. Leukocyte-Rich Platelet-Rich Plasma’s Clinical Effectiveness in Arthroscopic Rotator Cuff Repair: A Meta-Analysis of Randomized Controlled Trials. Bioengineering 2025, 12, 617. https://doi.org/10.3390/bioengineering12060617
Tang P, Huang M, Xiao W, Wen T, Volotovsky P, Gerasimenko M, Chu S, Liu S, Zhang K, Li Y. Leukocyte-Rich Platelet-Rich Plasma’s Clinical Effectiveness in Arthroscopic Rotator Cuff Repair: A Meta-Analysis of Randomized Controlled Trials. Bioengineering. 2025; 12(6):617. https://doi.org/10.3390/bioengineering12060617
Chicago/Turabian StyleTang, Peiyuan, Meihui Huang, Wenfeng Xiao, Ting Wen, Pavel Volotovsky, Mikhail Gerasimenko, Shiyao Chu, Shuguang Liu, Kai Zhang, and Yusheng Li. 2025. "Leukocyte-Rich Platelet-Rich Plasma’s Clinical Effectiveness in Arthroscopic Rotator Cuff Repair: A Meta-Analysis of Randomized Controlled Trials" Bioengineering 12, no. 6: 617. https://doi.org/10.3390/bioengineering12060617
APA StyleTang, P., Huang, M., Xiao, W., Wen, T., Volotovsky, P., Gerasimenko, M., Chu, S., Liu, S., Zhang, K., & Li, Y. (2025). Leukocyte-Rich Platelet-Rich Plasma’s Clinical Effectiveness in Arthroscopic Rotator Cuff Repair: A Meta-Analysis of Randomized Controlled Trials. Bioengineering, 12(6), 617. https://doi.org/10.3390/bioengineering12060617