
Finite Element Analysis of Ocular Impact Forces and Potential Complications in Pickleball-Related Eye Injuries

 , , ,
, , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
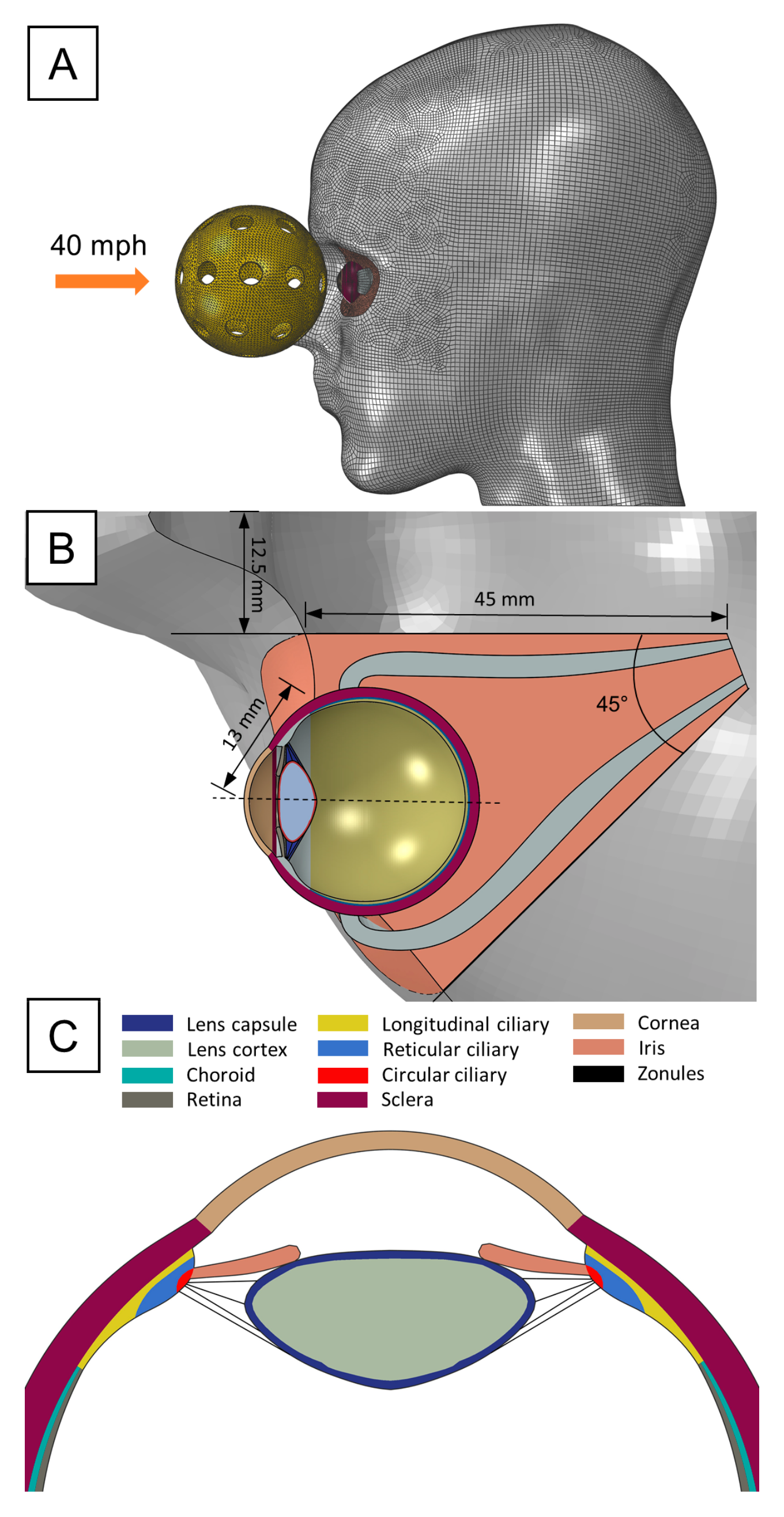
2.1. Model Construction
2.2. Computational Simulation of Pickleball Impact
2.3. Material Properties
3. Results
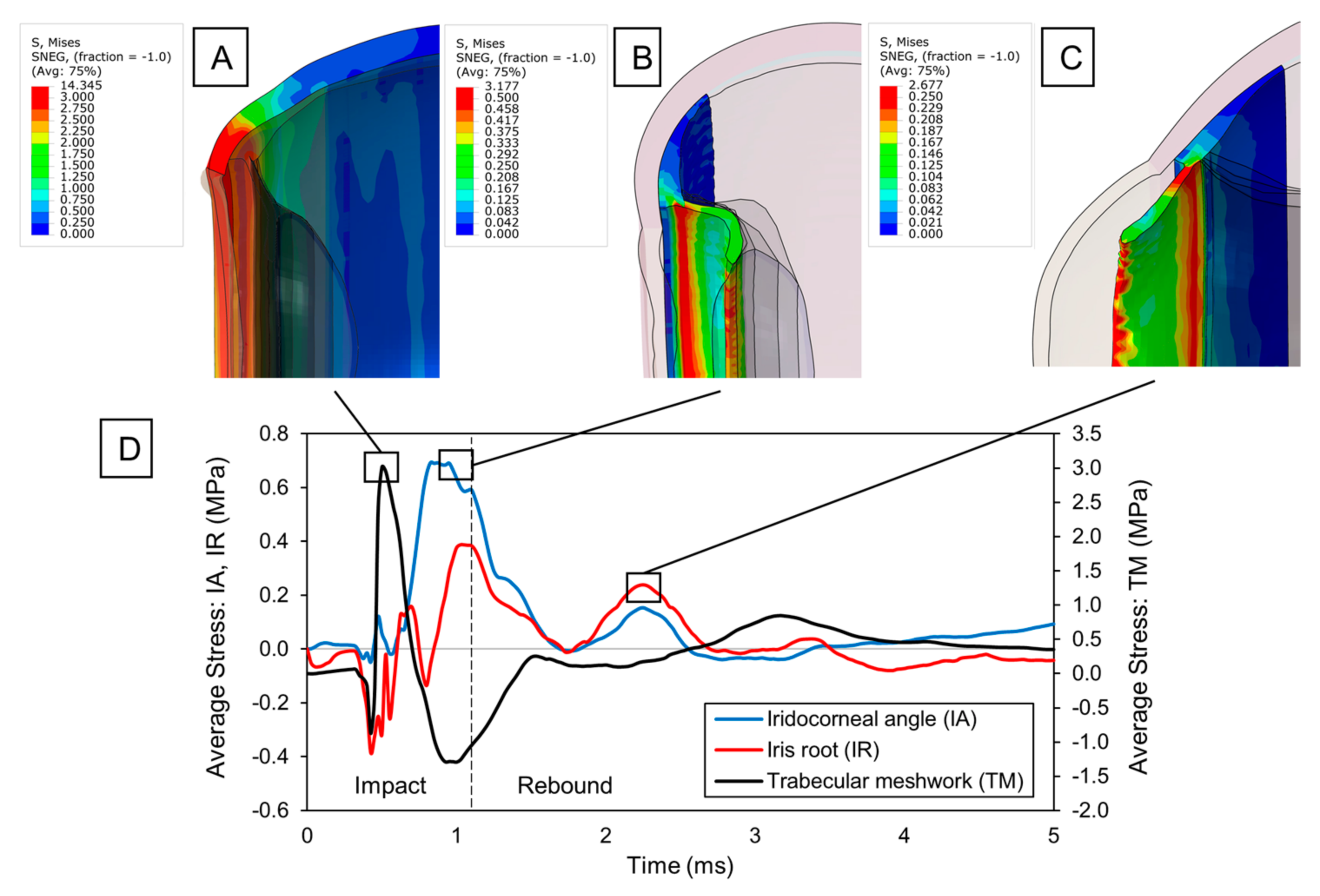
3.1. Impact of Pickleball-Related Trauma on Anterior Segment of the Eye
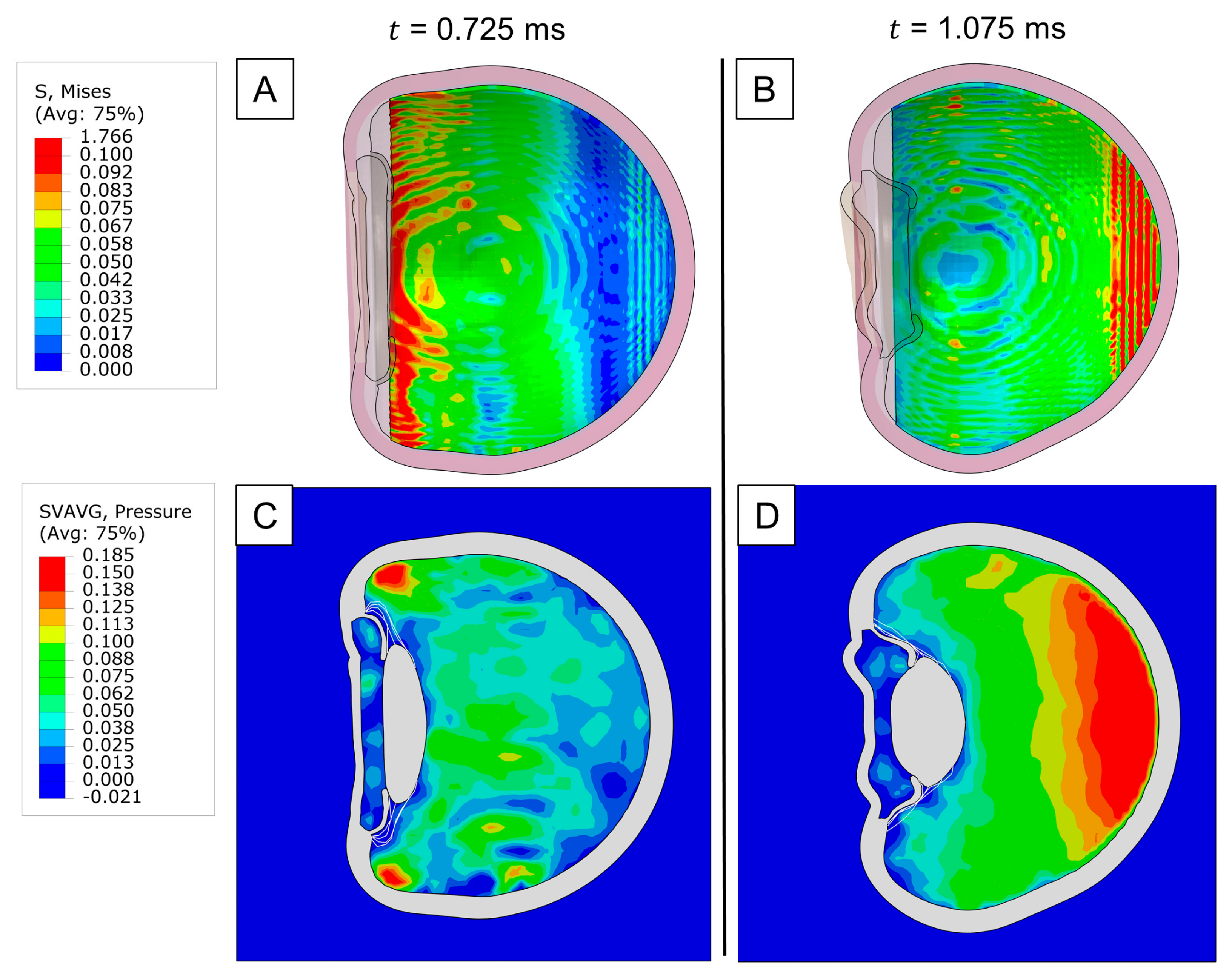
3.2. Dynamic Changes in Lens Zonules upon Impact
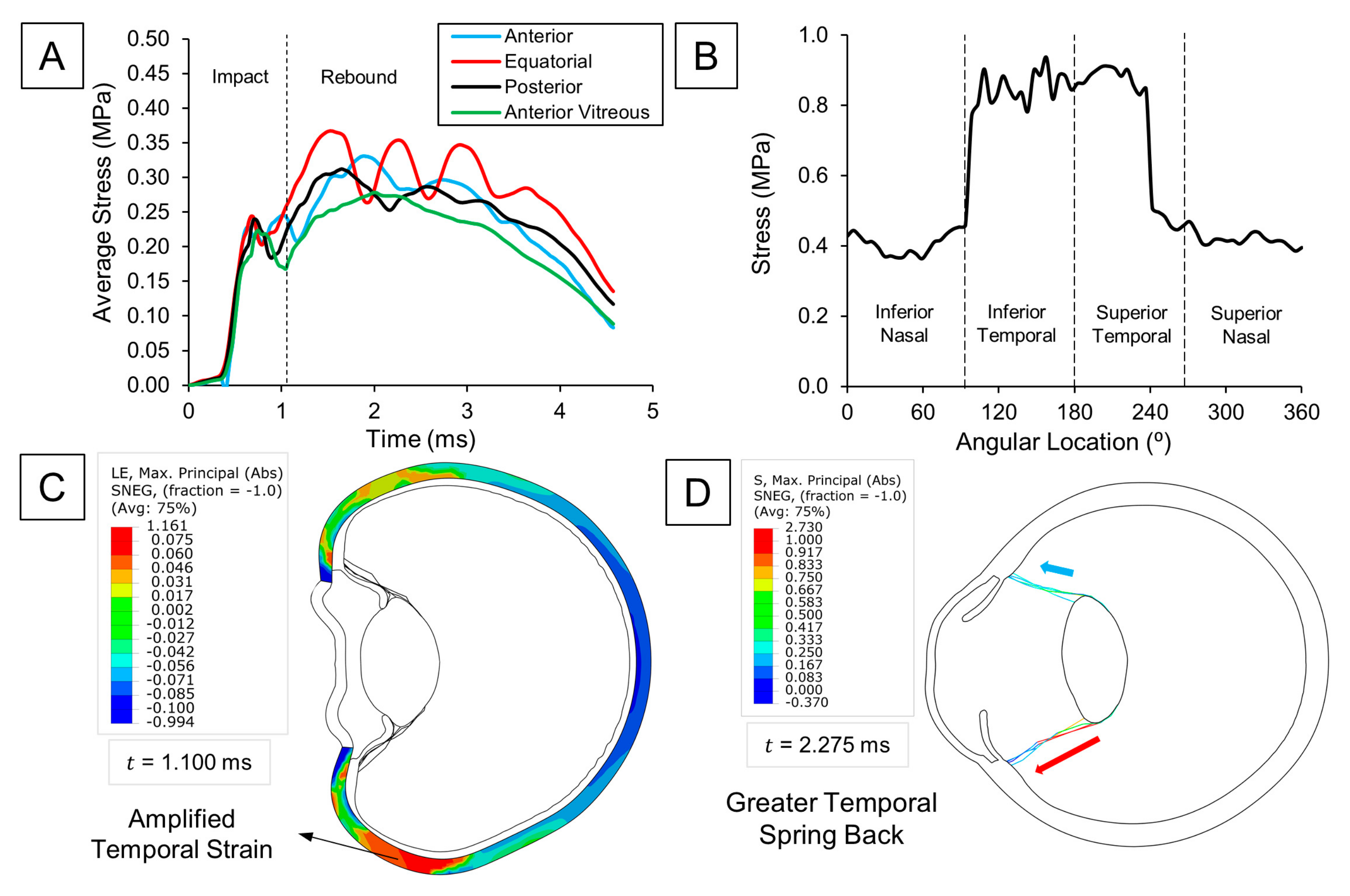
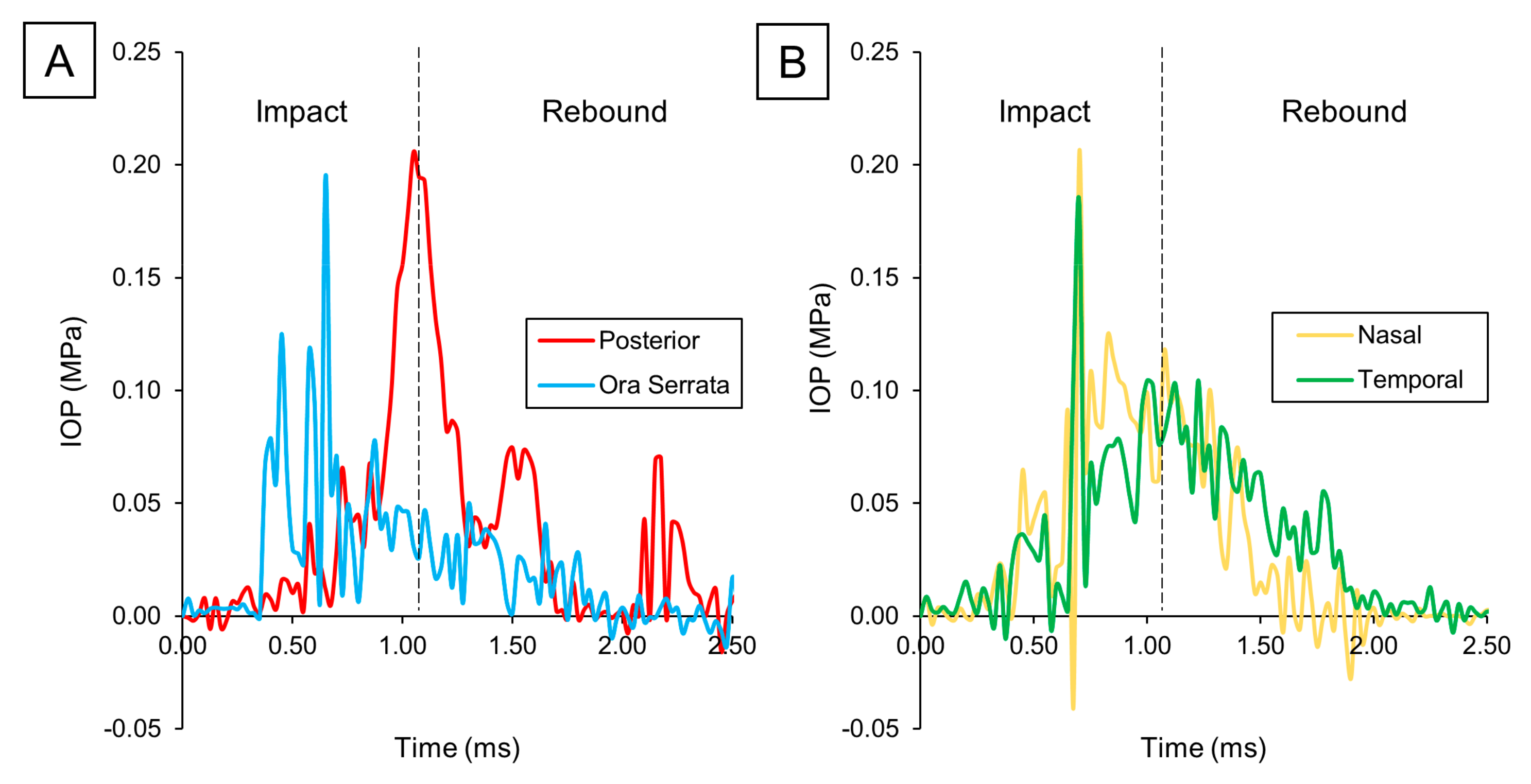
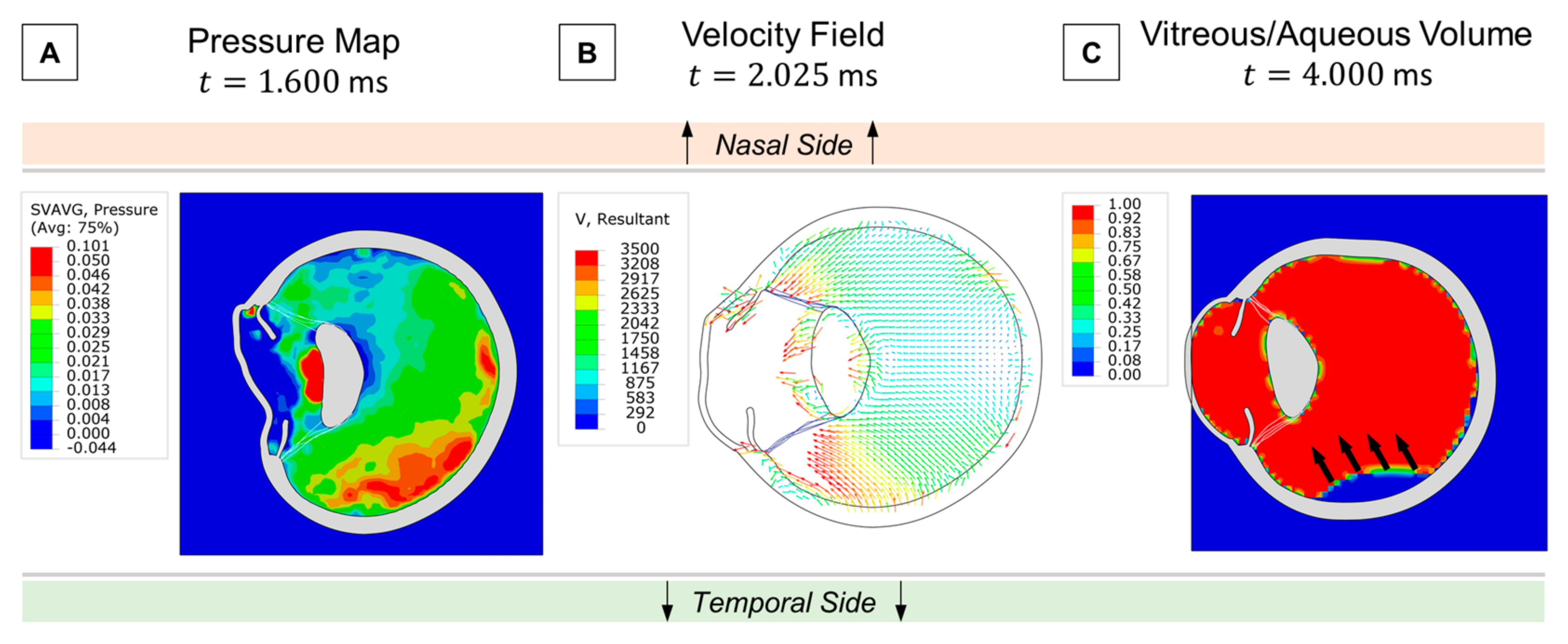
3.3. Pickleball-Related Injury Impact on the Retina
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- More Than a Pickle: Fastest-Growing, U.S. Sport May Pose Ocular Injury Risks-American Academy of Ophthalmology. Available online: https://www.aao.org/eyenet/article/more-than-a-pickle-ocular-injury-risks (accessed on 13 August 2024).
- Dang, V.T.; Alkawally, M. Pickleball Associated Abrasion and Iritis: A Case Study. CRO (Clin. Refract. Optom.) J. 2021, 32, 367–372. Available online: https://clinicaloptometry.scholasticahq.com/article/36828.pdf (accessed on 13 August 2024). [CrossRef]
- Huang, H.; Greven, M.A. Traumatic lens subluxation from pickleball injury: A case series. Retin. Cases Brief Rep. 2024, 18, 15–17. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, C.F.; Patron, M.E.; Joondeph, B.C. Retinal tears due to pickleball injury. Retin. Cases Brief Rep. 2022, 16, 312–313. [Google Scholar] [CrossRef] [PubMed]
- As Pickleball Popularity Skyrockets, Eye Injuries from Sport Also on Rise. Available online: https://www.ophthalmologytimes.com/view/as-pickleball-popularity-skyrockets-eye-injuries-from-sport-also-on-rise (accessed on 12 August 2024).
- Protect Your Eyes When Playing Pickleball-Harvard Health. Available online: https://www.health.harvard.edu/staying-healthy/protect-your-eyes-when-playing-pickleball (accessed on 13 August 2024).
- Waisberg, E.; Ong, J.; Lee, A.G. Pickleball eye injuries: Ocular protection recommendations and guidelines. Eye 2023, 38, 1039–1040. [Google Scholar] [CrossRef]
- The Importance of Protective Eyewear in Pickleball. Available online: https://pickleball.com/gear/the-importance-of-protective-eyewear-in-pickleball (accessed on 12 August 2024).
- Wear Eye Protection When Playing Pickleball-American Academy of Ophthalmology. Available online: https://www.aao.org/eye-health/tips-prevention/pickleball-eye-protection-black-eye (accessed on 12 August 2024).
- Pickleball Injuries May Cost Nearly $400 Million This Year|Fortune Well. Available online: https://fortune.com/well/2023/06/27/pickleball-injuries-may-cost-americans-nearly-400-million-this-year/ (accessed on 12 August 2024).
- Raul, J.S.; Baumgartner, D.; Willinger, R.; Ludes, B. Finite element modelling of human head injuries caused by a fall. Int. J. Legal. Med. 2006, 120, 212–218. [Google Scholar] [CrossRef]
- Roth, S.; Raul, J.S.; Ludes, B.; Willinger, R. Finite element analysis of impact and shaking inflicted to a child. Int. J. Leg. Med. 2007, 121, 223–228. [Google Scholar] [CrossRef]
- Klinich, K.; Hulbert, G.; Schneider, L. Estimating Infant Head Injury Criteria and Impact Response Using Crash Reconstruction and Finite Element Modeling. Published online 2002. Available online: https://www.sae.org/publications/technical-papers/content/2002-22-0009/ (accessed on 21 April 2024).
- Lapeer, R.J.; Prager, R.W. Fetal head moulding: Finite element analysis of a fetal skull subjected to uterine pressures during the first stage of labour. J. Biomech. 2001, 34, 1125–1133. [Google Scholar] [CrossRef]
- Stitzel, J.D.; Duma, S.M.; Cormier, J.M.; Herring, I.P. A nonlinear finite element model of the eye with experimental validation for the prediction of globe rupture. Stapp Car Crash J. 2002, 46, 81–102. [Google Scholar] [CrossRef]
- Burd, H.J.; Judge, S.J.; Cross, J.A. Numerical modelling of the accommodating lens. Vis. Res. 2002, 42, 2235–2251. [Google Scholar] [CrossRef]
- Development of an Anatomically Accurate Finite Element Human Ocular Globe Model for Blast-Related Fluid-Structure Interaction Studies. Available online: https://apps.dtic.mil/sti/citations/AD1027738 (accessed on 12 November 2024).
- Knaus, K.R.; Hipsley, A.M.; Blemker, S.S. The action of ciliary muscle contraction on accommodation of the lens explored with a 3D model. Biomech. Model. Mechanobiol. 2021, 20, 879–894. [Google Scholar] [CrossRef]
- Tamm, S.; Tamm, E.; Rohen, J.W. Age-related changes of the human ciliary muscle. A quantitative morphometric study. Mech. Ageing Dev. 1992, 62, 209–221. [Google Scholar] [CrossRef] [PubMed]
- Weeber, H.A.; van der Heijde, R.G.L. Internal deformation of the human crystalline lens during accommodation. Acta Ophthalmol. 2008, 86, 642–647. [Google Scholar] [CrossRef] [PubMed]
- Ganpule, S.; Gu, L.; Alai, A.; Chandra, N. Role of helmet in the mechanics of shock wave propagation under blast loading conditions. Comput. Methods Biomech. Biomed. Eng. 2012, 15, 1233–1244. [Google Scholar] [CrossRef]
- Fitzhugh, A.; Naveed, H.; Davagnanam, I.; Messiha, A. Proposed three-dimensional model of the orbit and relevance to orbital fracture repair. Surg. Radiol. Anat. 2016, 38, 557–561. [Google Scholar] [CrossRef]
- Michael, R.; Mikielewicz, M.; Gordillo, C.; Montenegro, G.A.; Pinilla Cortés, L.; Barraquer, R.I. Elastic Properties of Human Lens Zonules as a Function of Age in Presbyopes. Investig. Ophthalmol. Vis. Sci. 2012, 53, 6109–6114. [Google Scholar] [CrossRef]
- Herlihy, J.T.; Murphy, R.A. Length-Tension Relationship of Smooth Muscle of the Hog Carotid Artery. Circ. Res. 1973, 33, 275–283. [Google Scholar] [CrossRef]
- Li, J.; Jia, Y.; Li, T.; Zhu, Z.; Zhou, H.; Peng, X.; Jiang, S. Tensile Behavior of Acrylonitrile Butadiene Styrene at Different Temperatures. Adv. Polym. Technol. 2020, 2020, 8946591. [Google Scholar] [CrossRef]
- Hong, J.D.; Colmenarez, J.A.; Choi, E.H.; Suh, A.; Suh, A.; Lam, M.; Hoskin, A.; Minckler, D.S.; Lin, K.Y.; Shahraki, K.; et al. Finite Element Analysis of Mechanical Ocular Sequelae from Badminton Shuttlecock Projectile Impact. Ophthalmol. Sci. 2025, 5, 100625. [Google Scholar] [CrossRef]
- Nambiar, M.; Liechti, L.; Studer, H.; Roy, A.S.; Seiler, T.G.; Büchler, P. Biomechanical Characterization of Human Corneal Lenticules. Curr. Dir. Biomed. Eng. 2022, 8, 463–465. [Google Scholar] [CrossRef]
- Weeber, H.A.; Eckert, G.; Pechhold, W.; van der Heijde, R.G.L. Stiffness gradient in the crystalline lens. Graefe’s Arch. Clin. Exp. Ophthalmol. 2007, 245, 1357–1366. [Google Scholar] [CrossRef]
- Berggren, C.C.; Ameku, K.A.; Pedrigi, R.M. Altered stress field of the human lens capsule after cataract surgery. J. Biomech. 2021, 115, 110127. [Google Scholar] [CrossRef] [PubMed]
- Ciasca, G.; Pagliei, V.; Minelli, E.; Palermo, F.; Nardini, M.; Pastore, V.; Papi, M.; Caporossi, A.; De Spirito, M.; Minnella, A.M. Nanomechanical mapping helps explain differences in outcomes of eye microsurgery: A comparative study of macular pathologies. PLoS ONE 2019, 14, e0220571. [Google Scholar] [CrossRef] [PubMed]
- Heys, J.; Barocas, V.H. Mechanical characterization of the bovine iris. J. Biomech. 1999, 32, 999–1003. [Google Scholar] [CrossRef]
- Colmenarez, J.A.; Zhai, Y.; Mendoza, V.O.; Dong, P.; Nunes, K.; Suh, D.W.; Gu, L. Damage-Induced Softening of the Sclera: A Pseudo-Elastic Modeling Approach. J. Eng. Sci. Med. Diagn. Ther. 2024, 7, 031001. [Google Scholar] [CrossRef]
- Chen, K.; Weiland, J.D. Mechanical properties of orbital fat and its encapsulating connective tissue. J. Biomech. Eng. 2011, 133, 064505. [Google Scholar] [CrossRef]
- Boopathiraj, N.; Wagner, I.V.; Krambeer, C.J.; Lentz, P.C.; Miller, D.D.; Mashayekhi, A.; Dorairaj, S.K. In a pickle: Cases of pickleball related ocular injuries. Am. J. Ophthalmol. Case Rep. 2024, 35, 102082. [Google Scholar] [CrossRef]
- Stitzel, J.D.; Hansen, G.A.; Herring, I.P.; Duma, S.M. Blunt trauma of the aging eye: Injury mechanisms and increasing lens stiffness. Arch. Ophthalmol. 2005, 123, 789–794. [Google Scholar] [CrossRef]
- Guo, Y.; Guo, L.L.; Yang, W.; Tian, L.; Jie, Y. Age-related analysis of corneal biomechanical parameters in healthy Chinese individuals. Sci. Rep. 2024, 14, 1–13. [Google Scholar] [CrossRef]
- Grossniklaus, H.E.; Nickerson, J.M.; Edelhauser, H.F.; Bergman, L.A.M.K.; Berglin, L. Anatomic Alterations in Aging and Age-Related Diseases of the Eye. Investig. Ophthalmol. Vis. Sci. 2013, 54, ORSF23–ORSF27. [Google Scholar] [CrossRef]
- Lam, M.R.; Dong, P.; Shokrollahi, Y.; Gu, L.; Suh, D.W. Finite Element Analysis of Soccer Ball-Related Ocular and Retinal Trauma and Comparison with Abusive Head Trauma. Ophthalmol. Sci. 2022, 2, 100129. [Google Scholar] [CrossRef]
- Suh, A.; Suh, A.; Colmenarez, J.A.; Lam, M.; Dong, P.; Hoskin, A.K.; Shahraki, K.; Agrawal, R.V.; Gu, L.; Suh, D.W. Quantifying Ocular Stresses in Badminton-Related Eye Injuries. Investig. Ophthalmol. Vis. Sci. 2024, 65, 123. [Google Scholar]
- Seven Rings of Trauma-EyeWiki. Available online: https://eyewiki.org/Seven_Rings_of_Trauma (accessed on 14 May 2025).
- Ross, W.H. Traumatic Retinal Dialyses. Arch. Ophthalmol. 1981, 99, 1371–1374. [Google Scholar] [CrossRef] [PubMed]
- Mahmoudzadeh, R.; Huang, D.; Salabati, M.; Awh, K.; Garg, S.; Hsu, J.; Ho, A.; Regillo, C. Clinical Characteristics and Management Outcomes of Rhegmatogenous Retinal Detachments Due to Retinal Dialysis. J. Vitreoretin. Dis. 2021, 5, 405. [Google Scholar] [CrossRef] [PubMed]
- Rohowetz, L.J.; Jabbehdari, S.; Smiddy, W.E.; Berrocal, A.M.; Townsend, J.H.; Chang, J.S.; Yannuzzi, N.; Sridhar, J.; Haddock, L.J.; Fortun, J.A.; et al. Retinal Detachment Associated with Retinal Dialysis: Clinical Features and Outcomes of Surgery in a 10-Year Study. Ophthalmol. Retin. 2023, 7, 857–861. [Google Scholar] [CrossRef]
- Ayalon, A.; Okrent, L.; Rubowitz, A. Posterior pole retinal tears following blunt ocular trauma. Am. J. Ophthalmol. Case Rep. 2020, 18, 100642. [Google Scholar] [CrossRef]
- Capão Filipe, J.A.; Fernandes, V.L.; Barros, H.; Falcão-Reis, F.; Castro-Correia, J. Soccer-Related Ocular Injuries. Arch. Ophthalmol. 2003, 121, 687–694. [Google Scholar] [CrossRef]
- Trauma: Posterior Segment Injuries-American Academy of Ophthalmology. Available online: https://www.aao.org/education/disease-review/posterior-segment-injuries (accessed on 12 November 2024).
- Geng, X.; Liu, X.; Wei, W.; Wang, Y.; Wang, L.; Chen, K.; Huo, H.; Zhu, Y.; Fan, Y. Mechanical Evaluation of Retinal Damage Associated with Blunt Craniomaxillofacial Trauma: A Simulation Analysis. Transl. Vis. Sci. Technol. 2018, 7, 16. [Google Scholar] [CrossRef]
- Colmenarez, J.A.; Lam, M.; Dong, P.; Hoskin, A.K.; Agrawal, R.V.; Shahraki, K.; Suh, D.W.; Gu, L. Comparative biomechanical study of blunt ocular traumas and shaken baby syndrome. Investig. Ophthalmol. Vis. Sci. 2024, 65, 2877. [Google Scholar]
- Pang, G.; Wang, C.; Wang, X.; Li, X.; Meng, Q. A review of human cornea finite element modeling: Geometry modeling, constitutive modeling, and outlooks. Front. Bioeng. Biotechnol. 2024, 12, 1455027. [Google Scholar] [CrossRef]
- Yoo, L.; Reed, J.; Shin, A.; Kung, J.; Gimzewski, J.K.; Poukens, V.; Goldberg, R.A.; Mancini, R.; Taban, M.; Moy, R.; et al. Characterization of Ocular Tissues Using Microindentation and Hertzian Viscoelastic Models. Investig. Ophthalmol. Vis. Sci. 2011, 52, 3475. [Google Scholar] [CrossRef]
- Perez, B.C.; Morris, H.J.; Hart, R.T.; Liu, J. Finite element modeling of the viscoelastic responses of the eye during microvolumetric changes. J. Biomed. Sci. Eng. 2013, 6, 29–37. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Component | Constitutive Model | Material Constants | Reference |
|---|---|---|---|
| Pickleball | Linear elastic | Li et al. [25] | |
| Choroid | Neo-Hookean hyperelastic | Colmenarez et al. [26] | |
| Ciliary body | GHO hyperelastic | Herlihy et al. [24] | |
| Cornea | GHO hyperelastic | Nambiar et al. [27] | |
| Zonules | Linear elastic | Michael et al. [23] | |
| Lens cortex | Neo-Hookean hyperelastic | Weeber et al. [28] | |
| Lens capsule | GHO hyperelastic | Berggren et al. [29] | |
| Retina | Neo-Hookean hyperelastic | Ciasca et al. [30] | |
| Iris | Neo-Hookean hyperelastic | Heys et al. [31] | |
| Sclera | Yeoh’s hyperelastic | Colmenarez et al. [32] | |
| Orbital adipose | Neo-Hookean hyperelastic, and viscoelastic | Chen et al. [33] | |
| Humor bodies | Mie-Grüneisen equation of state with linear Us-Up Hugoniot condition | N·s/mm2 | Dassault Systemes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rydz, C.; Colmenarez, J.A.; Shahraki, K.; Dong, P.; Gu, L.; Suh, D.W. Finite Element Analysis of Ocular Impact Forces and Potential Complications in Pickleball-Related Eye Injuries. Bioengineering 2025, 12, 570. https://doi.org/10.3390/bioengineering12060570
Rydz C, Colmenarez JA, Shahraki K, Dong P, Gu L, Suh DW. Finite Element Analysis of Ocular Impact Forces and Potential Complications in Pickleball-Related Eye Injuries. Bioengineering. 2025; 12(6):570. https://doi.org/10.3390/bioengineering12060570
Chicago/Turabian StyleRydz, Cezary, Jose A. Colmenarez, Kourosh Shahraki, Pengfei Dong, Linxia Gu, and Donny W. Suh. 2025. "Finite Element Analysis of Ocular Impact Forces and Potential Complications in Pickleball-Related Eye Injuries" Bioengineering 12, no. 6: 570. https://doi.org/10.3390/bioengineering12060570
APA StyleRydz, C., Colmenarez, J. A., Shahraki, K., Dong, P., Gu, L., & Suh, D. W. (2025). Finite Element Analysis of Ocular Impact Forces and Potential Complications in Pickleball-Related Eye Injuries. Bioengineering, 12(6), 570. https://doi.org/10.3390/bioengineering12060570