
An Experimental and Clinical Study of Flap Monitoring with an Analysis of the Clinical Course of the Flap Using an Infrared Thermal Camera

 , and
, and
Abstract

1. Introduction
2. Materials and Methods
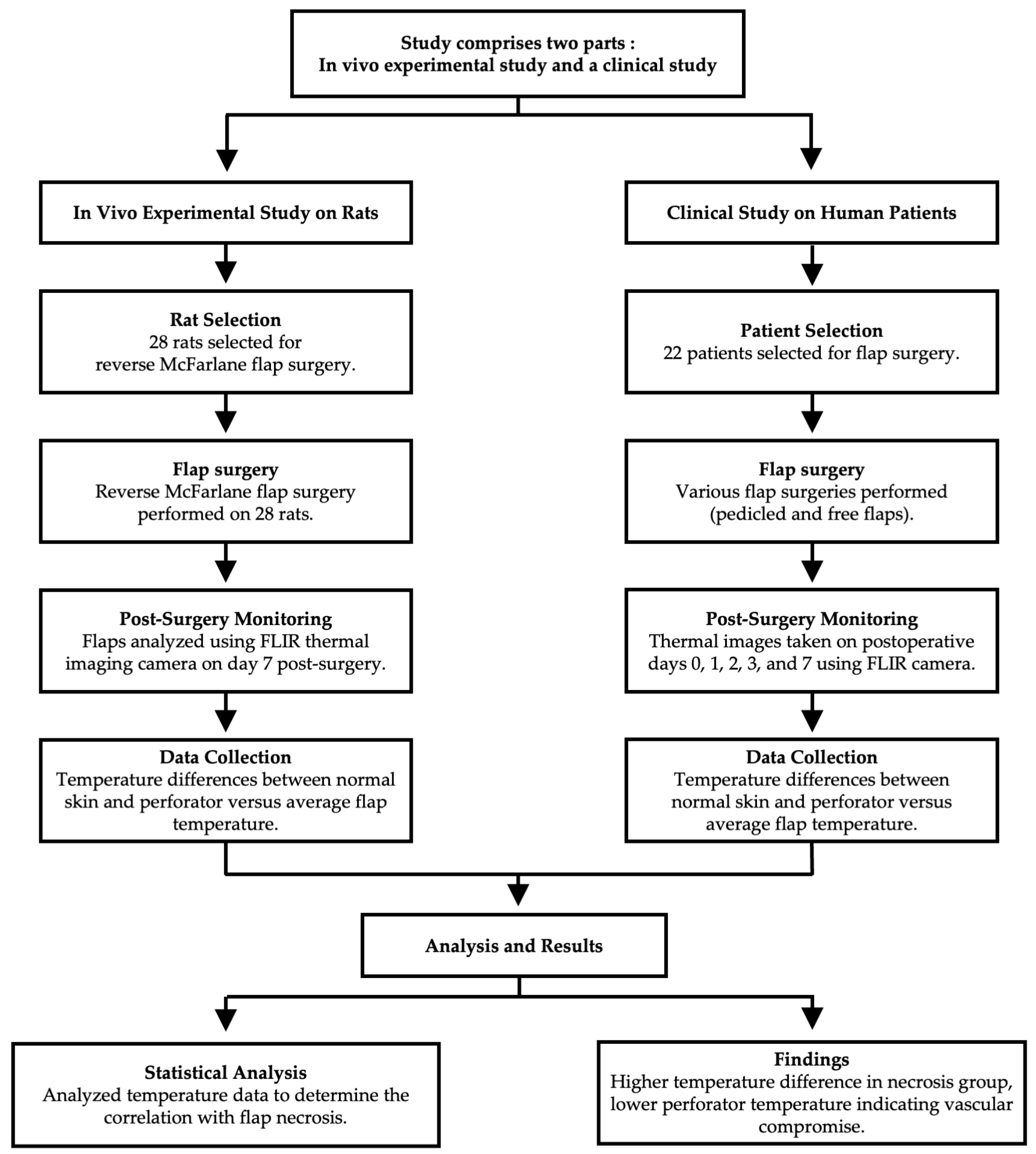
2.1. Study Design
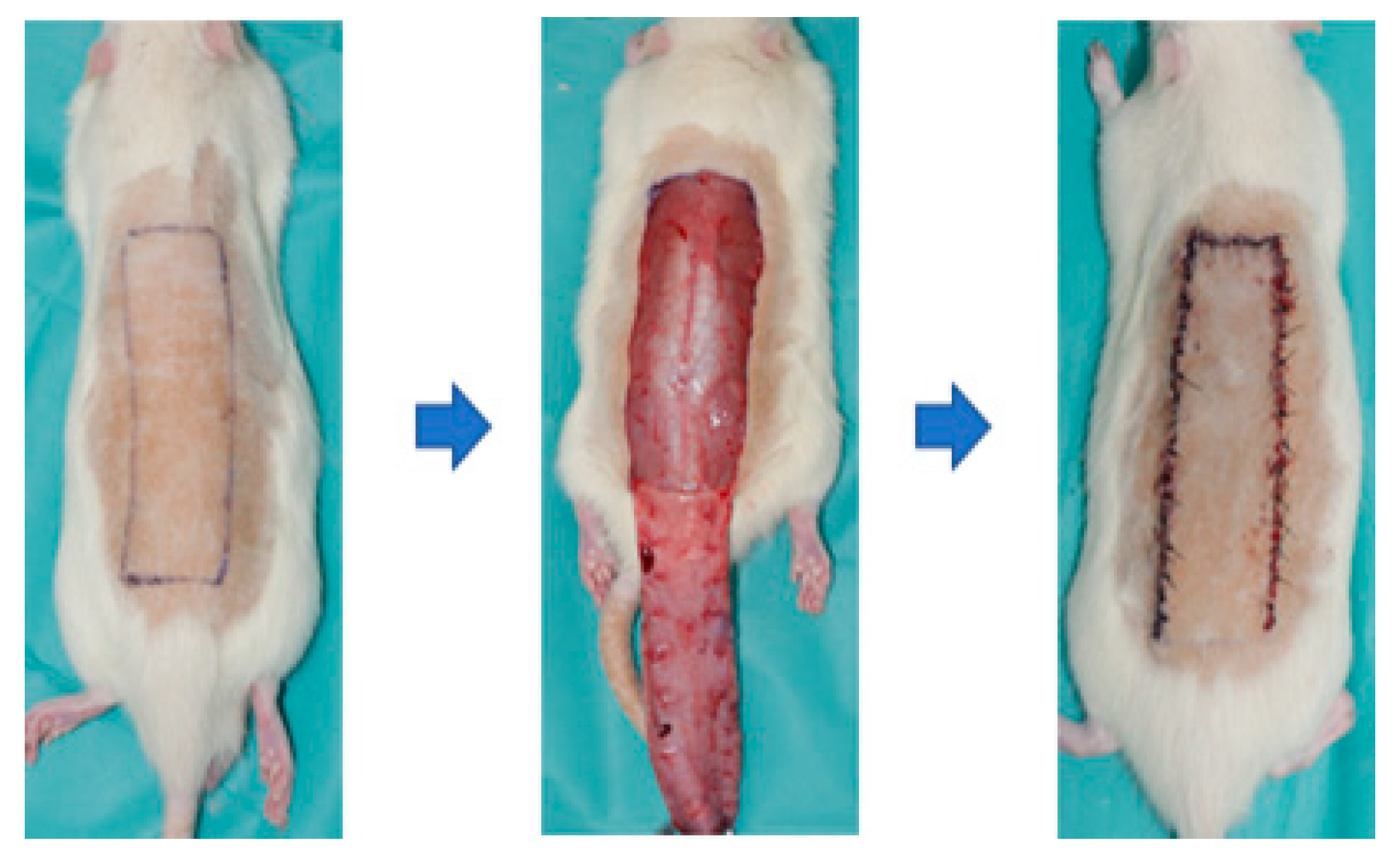
2.2. Rat Models
2.3. Patients
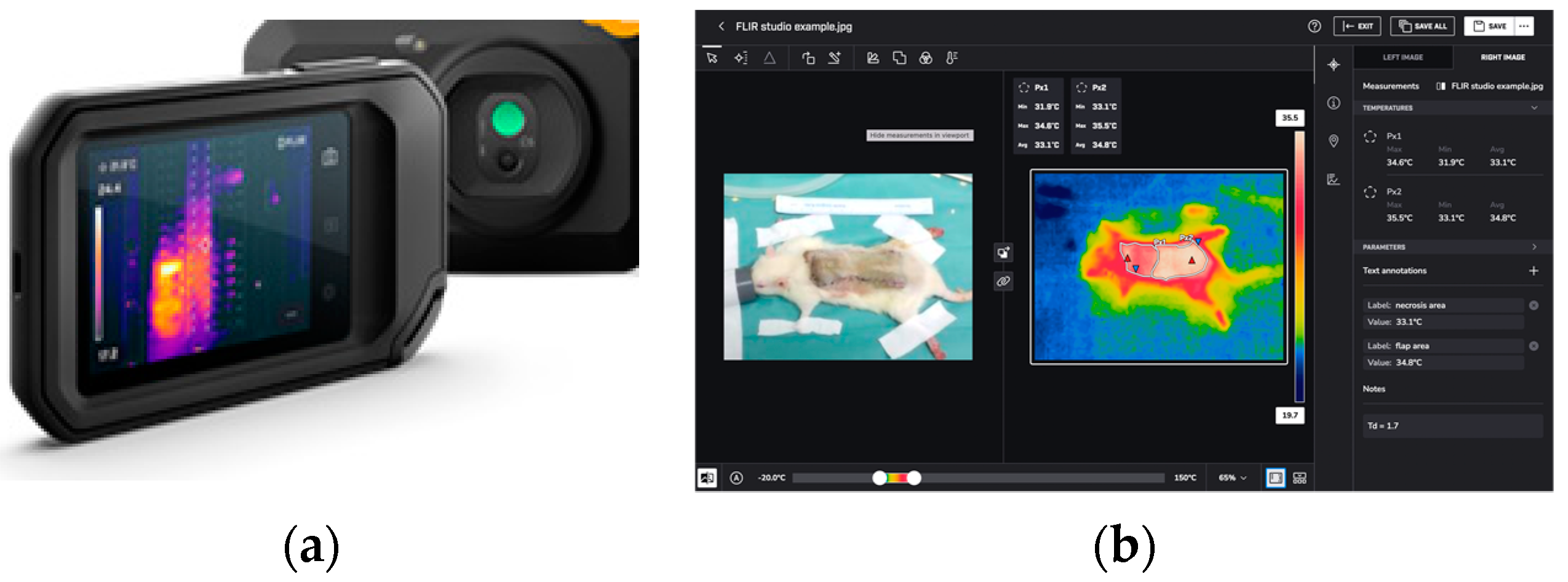
2.4. Infrared Thermal Imaging
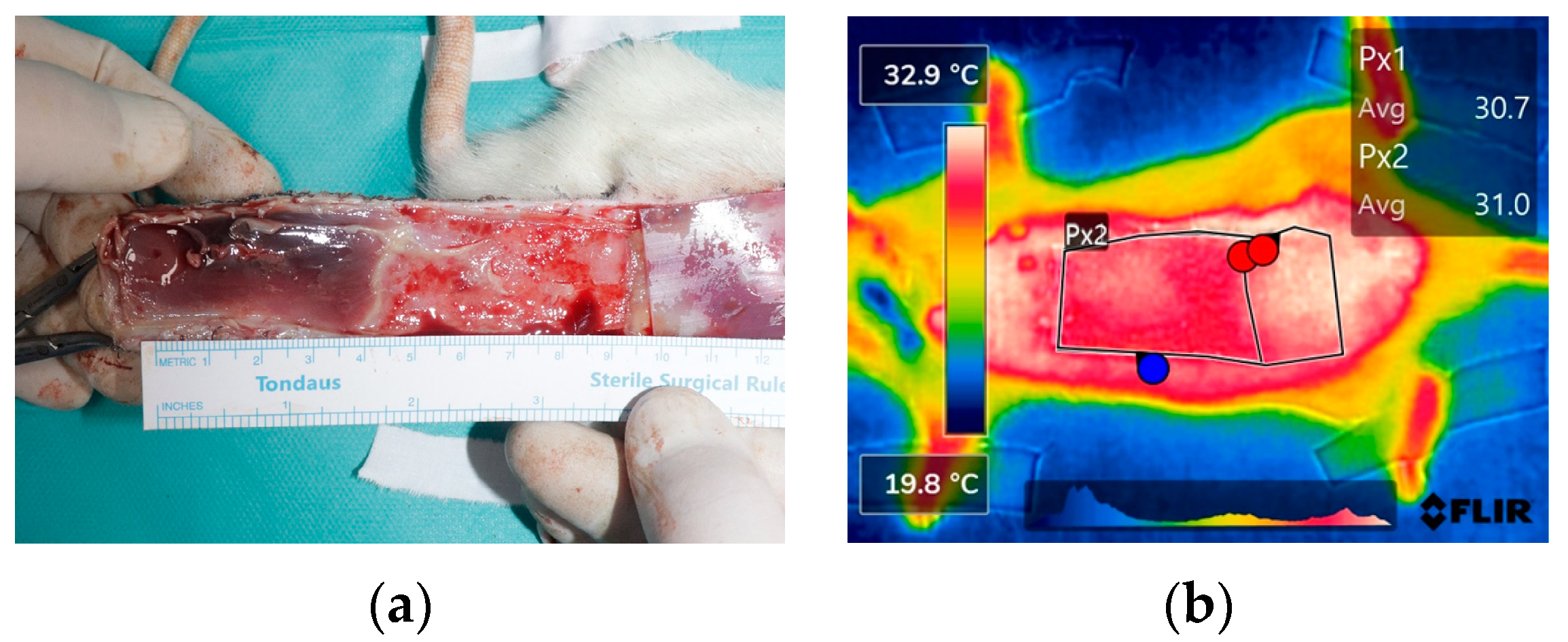
2.5. Infrared Thermal Image Analysis
2.6. Statistical Analysis
3. Results
3.1. Rat Models
3.2. Patients
3.2.1. Patient Demographics and Flap Characteristics
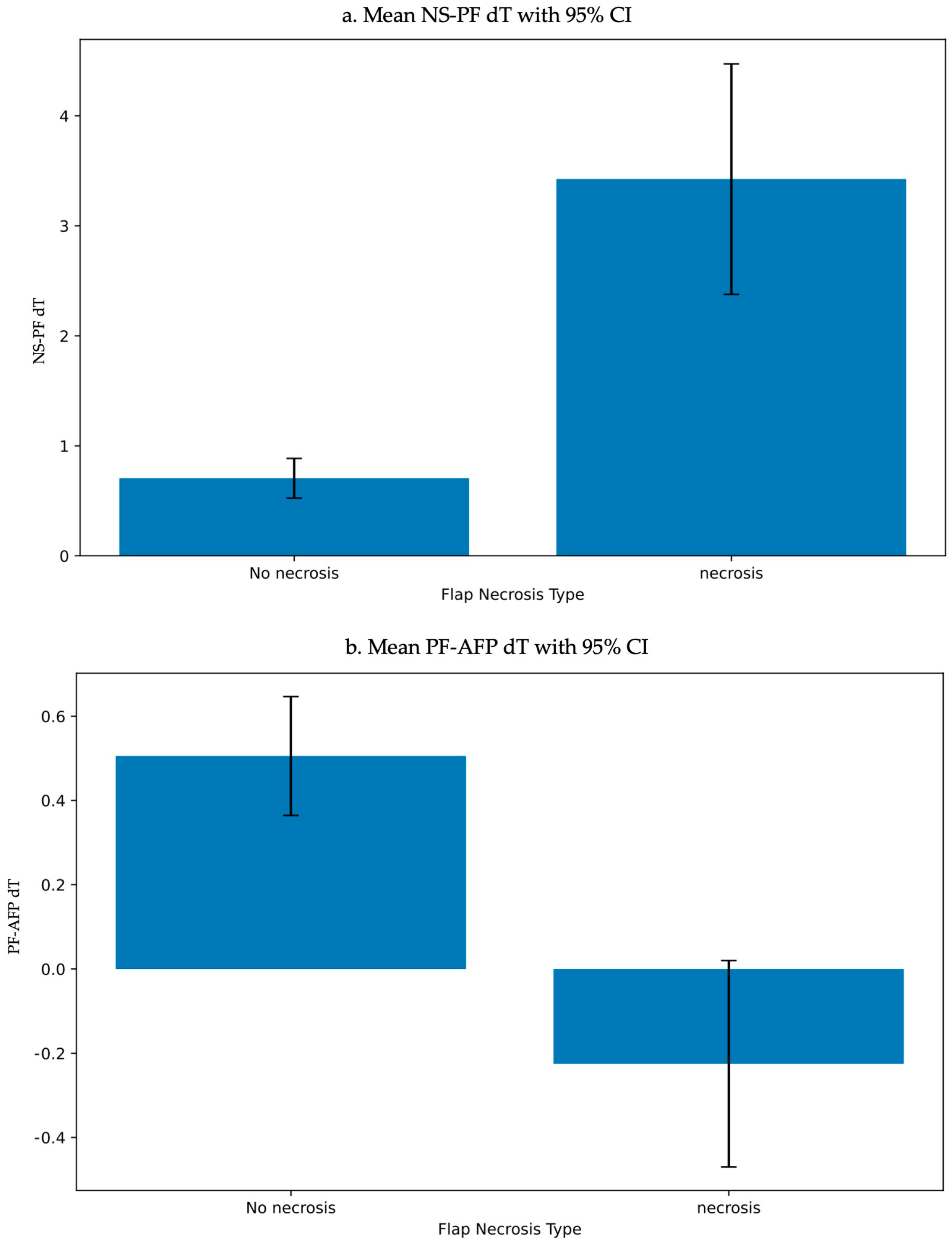
3.2.2. Infrared Thermal Imaging Analysis
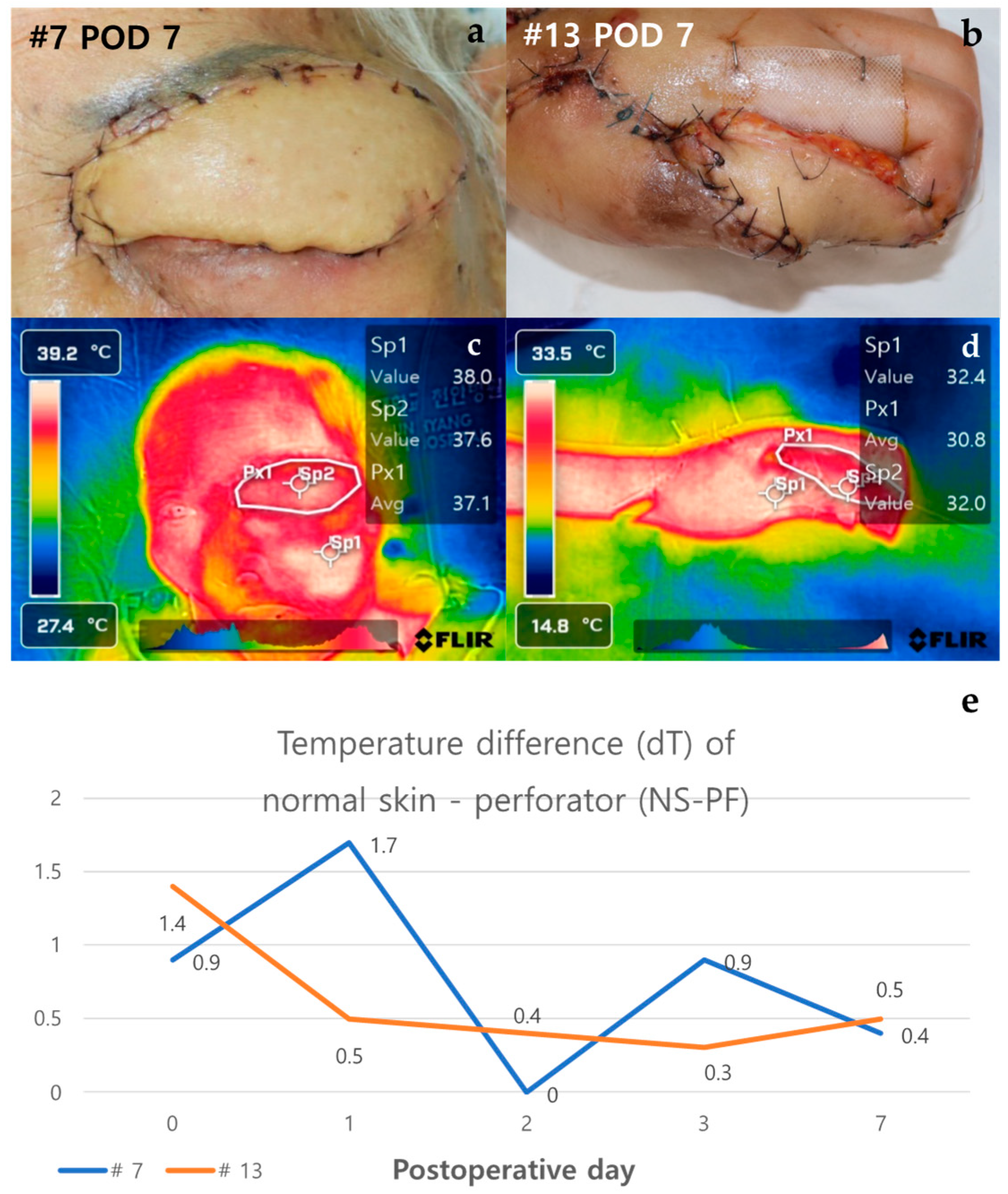
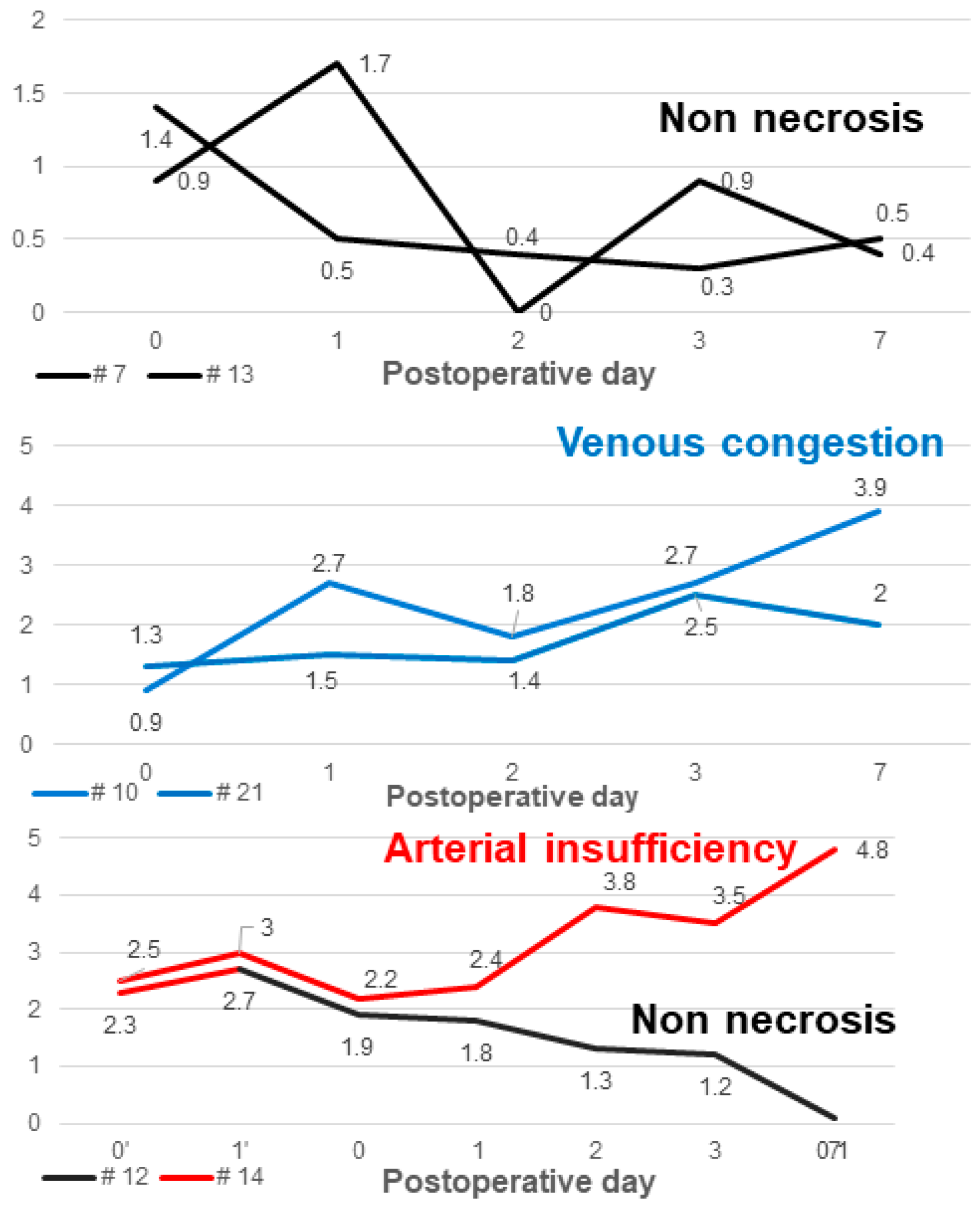
3.2.3. Case of Non-Necrosis Group (Case #7 and Case #13)
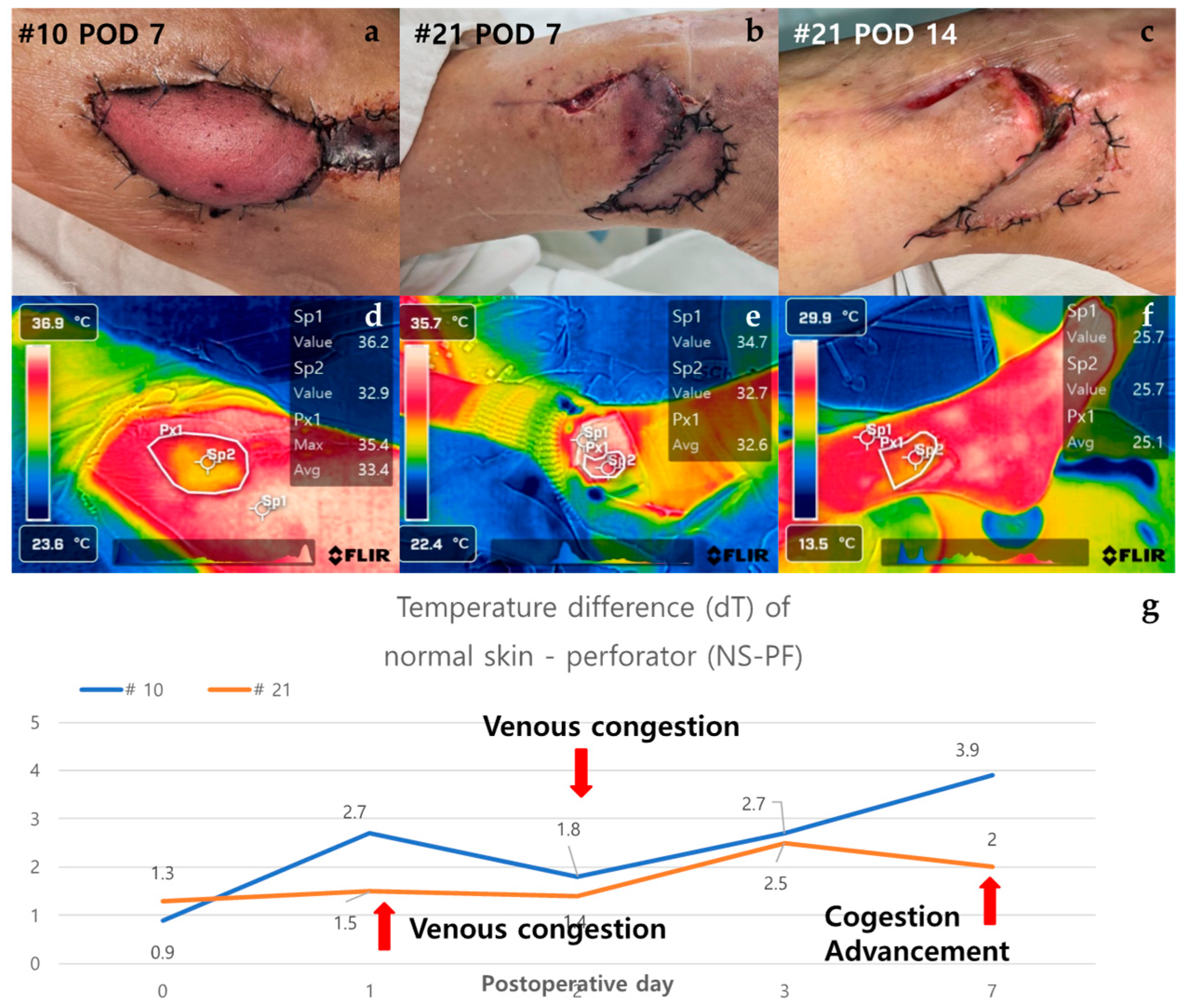
3.2.4. Case of Venous Congestion in Necrosis Group (Case #10 and Case #21)
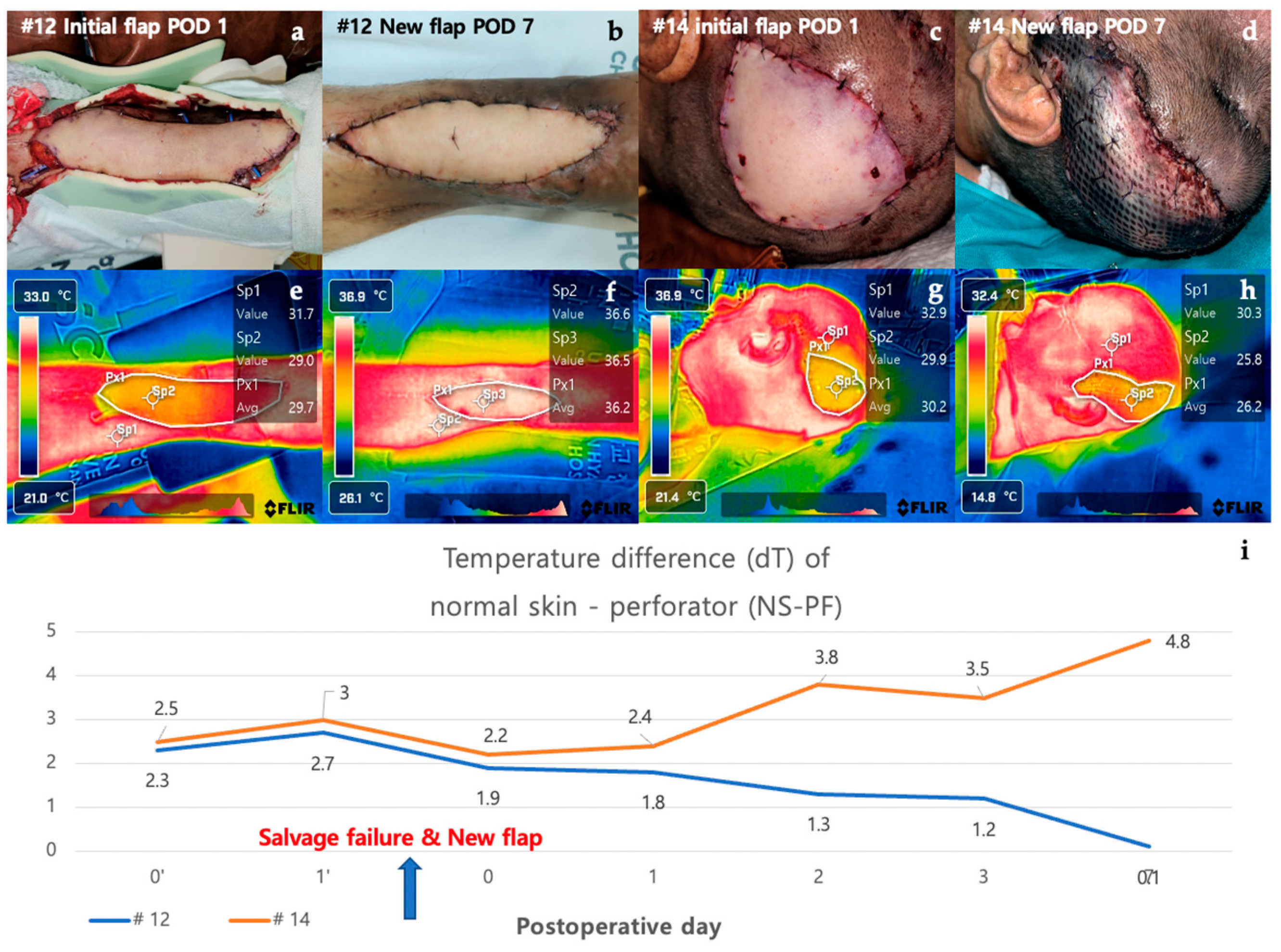
3.2.5. Case in which a New Flap was Applied after Salvage Procedure for Arterial Insufficiency (Case #12 and Case #14)
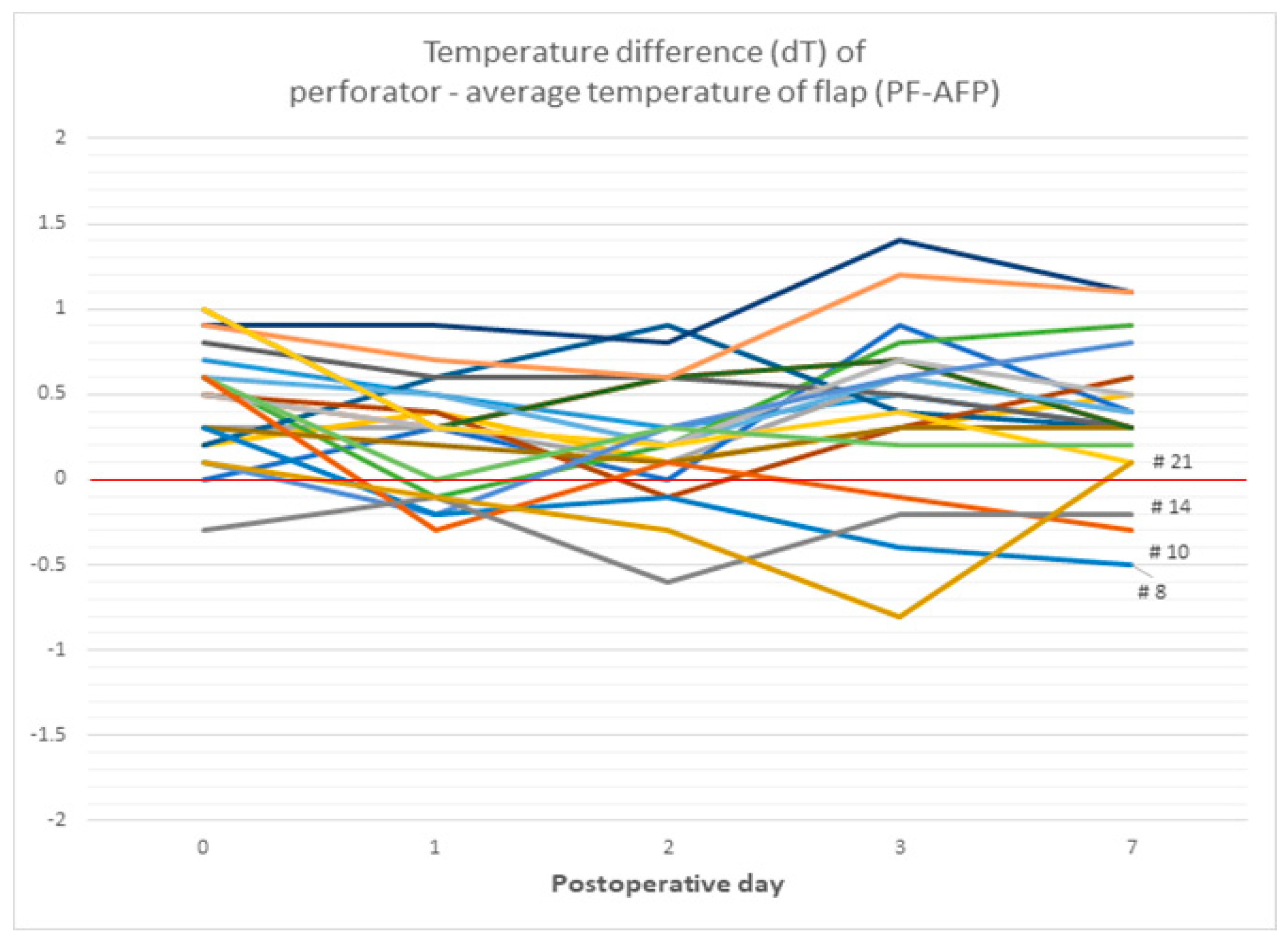
3.2.6. The Difference between the Temperature of Perforator Area and the Average Temperature of Total Flap (dT of PF-AFP)
3.2.7. Comparison of Pedicle Flaps and Free Flaps
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gottlieb, L.J.; Krieger, L.M.M. From the reconstructive ladder to the reconstructive elevator. Plast. Reconstr. Surg. 1994, 93, 1503–1504. [Google Scholar] [CrossRef] [PubMed]
- Shen, A.Y.; Lonie, S.; Lim, K.; Farthing, H.; Hunter-Smith, D.J.; Rozen, W.M. Free flap monitoring, salvage, and failure timing: A systematic review. J. Reconstr. Microsurg. 2021, 37, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Knoedler, S.; Hoch, C.C.; Huelsboemer, L.; Knoedler, L.; Stögner, V.A.; Pomahac, B.; Kauke-Navarro, M.; Colen, D. Postoperative free flap monitoring in reconstructive surgery-man or machine? Front. Surg. 2023, 10, 1130566. [Google Scholar] [CrossRef] [PubMed]
- Hosein, R.C.; Cornejo, A.; Wang, H.T. Postoperative monitoring of free flap reconstruction: A comparison of external Doppler ultrasonography and the implantable Doppler probe. Plast. Surg. 2016, 24, 11–19. [Google Scholar] [CrossRef]
- Rabbani, M.J.; Bhatti, A.Z.; Shahzad, A. Flap monitoring using thermal imaging camera: A contactless method. J. Coll. Physicians Surg. Pak. 2021, 31, 703–706. [Google Scholar] [CrossRef] [PubMed]
- John, H.E.; Niumsawatt, V.; Rozen, W.M.; Whitaker, I.S. Clinical applications of dynamic infrared thermography in plastic surgery: A systematic review. Gland. Surg. 2016, 5, 122–132. [Google Scholar] [CrossRef] [PubMed]
- Hennessy, O.; Potter, S.M. Use of infrared thermography for the assessment of free flap perforators in autologous breast reconstruction: A systematic review. JPRAS Open 2019, 23, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Sittitrai, P.; Ruenmarkkaew, D.; Klibngern, H. Pedicled flaps versus free flaps for oral cavity cancer reconstruction: A comparison of complications, hospital costs, and functional outcomes. Int. Arch. Otorhinolaryngol. 2022, 27, e32–e42. [Google Scholar] [CrossRef] [PubMed]
- Neusner, A.D.; Pribaz, J.J.; Guo, L. Free your mind, not your flap. Plast. Reconstr. Surg.—Glob. Open 2022, 10, e4384. [Google Scholar] [CrossRef]
- Lewis, R.S.; Kontos, M. Autologous tissue immediate breast reconstruction: Desired but oncologically safe? Int. J. Clin. Pract. 2009, 63, 1642–1646. [Google Scholar] [CrossRef]
- Suh, J.M.; Chung, C.H.; Chang, Y.J. Head and neck reconstruction using free flaps: A 30-year medical record review. Arch. Craniofacial Surg. 2021, 22, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Khouri, R.K.; Shaw, W.W. Monitoring of free flaps with surface-temperature recordings: Is it reliable? Plast. Reconstr. Surg. 1992, 89, 495–499. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, G.K.; Hwang, B.H.; Zhang, Y.; Monahan, J.F.W.; Davis, G.B.; Lee, Y.S.; Ragina, N.P.; Wang, C.; Zhou, Z.Y.; Hong, Y.K.; et al. Novel biomarkers of arterial and venous ischemia in microvascular flaps. PLoS ONE 2013, 8, e71628. [Google Scholar] [CrossRef] [PubMed]
- Amon, M.; Menger, M.D.; Vollmar, B. Heme oxygenase and nitric oxide synthase mediate cooling-associated protection against TNF-α-induced microcirculatory dysfunction and apoptotic cell death. FASEB J. 2003, 17, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Menger, M.D.; Rücker, M.; Vollmar, B. Capillary dysfunction in striated muscle ischemia/reperfusion: On the mechanisms of capillary “no-reflow”. Shock 1997, 8, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Akita, S. Advances and challenges in perforator flap surgery. Glob. Health Med. 2020, 2, 114–121. [Google Scholar]
- Chao, A.H.; Meyerson, J.; Povoski, S.P.; Kocak, E. A review of devices used in the monitoring of microvascular free tissue transfers. Expert Rev. Med. Devices 2013, 10, 649–660. [Google Scholar] [CrossRef] [PubMed]
- Lohman, R.F.; Langevin, C.-J.; Bozkurt, M.; Kundu, N.; Djohan, R. A prospective analysis of free flap monitoring techniques: Physical examination, external doppler, implantable doppler, and tissue oximetry. J. Reconstr. Microsurg. 2013, 29, 051–056. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Shen, Z.; Shao, Z.; Yu, P. Free flap monitoring using near-infrared spectroscopy: A systemic review. Ann. Plast. Surg. 2016, 76, 590–597. [Google Scholar] [CrossRef]
- Ricci, J.A.; Vargas, C.R.; Lin, S.J.; Tobias, A.M.; Taghinia, A.H.; Lee, B.T. A novel free flap monitoring system using tissue oximetry with text message alerts. J. Reconstr. Microsurg. 2016, 32, 415–420. [Google Scholar] [CrossRef]
- Wang, Z.; Jiao, L.; Chen, S.; Li, Z.; Xiao, Y.; Du, F.; Huang, J.; Long, X. Flap perfusion assessment with indocyanine green angiography in deep inferior epigastric perforator flap breast reconstruction: A systematic review and meta-analysis. Microsurgery 2023, 43, 627–638. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.W.; Hwang, Y.S.; Byeon, J.Y.; Kim, J.H.; Choi, H.J. Does the advantage of transcutaneous oximetry measurements in diabetic foot ulcer apply equally to free flap reconstruction? World J. Clin. Cases 2023, 11, 7570–7582. [Google Scholar] [CrossRef] [PubMed]
- Nam, H.J.; Wee, S.Y.; Kim, S.Y.; Jeong, H.G.; Lee, D.W.; Byeon, J.; Park, S.; Choi, H.J. The correlation between transcutaneous oxygen pressure (TcPO2) and forward-looking infrared (FLIR) thermography in the evaluation of lower extremity perfusion according to angiosome. Int. Wound J. 2023, 21, e14431. [Google Scholar] [CrossRef] [PubMed]
- Asif, A.; Poyiatzis, C.; Raheman, F.J.; Rojoa, D.M. The use of infrared thermography (IRT) in burns depth assessment: A diagnostic accuracy meta-analysis. Eur. Burn. J. 2022, 3, 432–446. [Google Scholar] [CrossRef]
- Berner, J.E.; Pereira, N.; Troisi, L.; Will, P.; Nanchahal, J.; Jain, A. Accuracy of infrared thermography for perforator mapping: A systematic review and meta-analysis of diagnostic studies. J. Plast. Reconstr. Aesthetic Surg. 2021, 74, 1173–1179. [Google Scholar] [CrossRef] [PubMed]
- Park, C. Applications of the reverse McFarlane flap in hand surgery. J. Hand Surg. 2021, 46, 432–439. [Google Scholar]
- Lee, Y.S.; Kim, S.H. Reconstructive techniques using reverse McFarlane flaps. Plast. Reconstr. Surg. 2022, 49, 210–215. [Google Scholar]
- Patel, R.; Tan, E. Vascular considerations in reverse McFarlane flap procedures. Int. J. Reconstr. Surg. 2020, 36, 95–102. [Google Scholar]
- Nguyen, A.; Patel, V. Retrograde flap hemodynamics and clinical applications. J. Microsurg. 2022, 39, 315–320. [Google Scholar]
- Sowa, M.G.; Friesen, J.R.; Levasseur, M.; Schattka, B.; Sigurdson, L.; Hayakawa, T. The utility of near infrared imaging in intra-operative prediction of flap outcome: A reverse mcfarlane skin flap model study. J. Near Infrared Spectrosc. 2012, 20, 601–615. [Google Scholar] [CrossRef]
- Mahbub, S.I.; Kim, Y.J.; Choi, H.; Lee, B.-T. Papaverine loaded injectable and thermosensitive hydrogel system for improving survival of rat dorsal skin flaps. J. Mater. Sci. Mater. Med. 2023, 34, 28. [Google Scholar] [CrossRef] [PubMed]
- Czapla, N.; Łokaj, M.; Falkowski, A.; Prowans, P. The use of thermography to design tissue flaps—Experimental studies on animals. Videosurgery Other Miniinvasive Tech. 2014, 3, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Kraemer, R.; Lorenzen, J.; Knobloch, K.; Papst, S.; Kabbani, M.; Koennecker, S.; Vogt, P. Free flap microcirculatory monitoring correlates to free flap temperature assessment. J. Plast. Reconstr. Aesthetic Surg. 2011, 64, 1353–1358. [Google Scholar] [CrossRef] [PubMed]
- Hummelink, S.; Kruit, A.S.; van Vlaenderen, A.R.W.; Schreinemachers, M.J.M.; Steenbergen, W.; Ulrich, D.J.O. Post-operative monitoring of free flaps using a low-cost thermal camera: A pilot study. Eur. J. Plast. Surg. 2020, 43, 589–596. [Google Scholar] [CrossRef]
- Papillion, P.; Wong, L.; Waldrop, J.; Sargent, L.; Brzezienski, M.; Kennedy, W.; Rehm, J. Infrared surface temperature monitoring in the postoperative management of free tissue transfers. Can. J. Plast. Surg. 2009, 17, 97–101. [Google Scholar] [CrossRef]
- Whitaker, I.S.; Lie, K.H.; Rozen, W.M.; Chubb, D.; Ashton, M.W. Dynamic infrared thermography for the preoperative planning of microsurgical breast reconstruction: A comparison with CTA. J. Plast. Reconstr. Aesthetic Surg. 2012, 65, 130–132. [Google Scholar] [CrossRef]
- Perng, C.-K.; Ma, H.; Chiu, Y.-J.; Lin, P.-H.; Tsai, C.-H. Detection of free flap pedicle thrombosis by infrared surface temperature imaging. J. Surg. Res. 2018, 229, 169–176. [Google Scholar] [CrossRef]
- Moran-Romero, M.A.; Mendoza, F.J.L. Postoperative monitoring of free flaps using smartphone thermal imaging may lead to ambiguous results: Three case reports. Int. Microsurg. J. 2022, 6, 4. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Flap Models (n = 28) | POD 3 | POD 7 |
|---|---|---|
| Necrotic area/total flap ratio (%) | 24.4 | 27.5 |
| Temperature difference between total flap and necrotic area | 0.800 | 0.792 |
| Statistic | Value |
|---|---|
| t-value | 0.084 |
| p-value | 0.934 |
| Dependent Variable | Coefficient | Std. Error | t-Value | p-Value |
|---|---|---|---|---|
| POD3 Necrotic Area Temp | ||||
| Intercept | 28.069 | 4.663 | 6.020 | 0.000 |
| Before Flap Temp | 0.149 | 0.141 | 1.057 | 0.300 |
| POD7 Necrotic Area Temp | ||||
| Intercept | 27.592 | 5.045 | 5.469 | 0.000 |
| Before Flap Temp | 0.156 | 0.153 | 1.024 | 0.315 |
| Variable | Coefficient | Std. Error | z-Value | p-Value | 95% CI Lower | 95% CI Upper |
|---|---|---|---|---|---|---|
| Intercept (POD3) | 0.274 | 1.126 | 0.243 | 0.808 | −1.934 | 2.481 |
| Before Flap Temp | −0.040 | 0.023 | −1.734 | 0.083 | −0.085 | 0.005 |
| POD3 Total Flap Temp | 1.007 | 0.031 | 32.568 | 0.000 | 0.946 | 1.068 |
| Intercept (POD7) | 0.003 | 0.881 | 0.003 | 0.997 | −1.724 | 1.730 |
| Before Flap Temp | −0.004 | 0.001 | −2.988 | 0.003 | −0.006 | −0.001 |
| POD7 Total Flap Temp | 0.980 | 0.025 | 39.099 | 0.000 | 0.931 | 1.029 |
| No. of Patient | Sex | Age | Location | Flap | Flap Type | Flap Necrosis |
|---|---|---|---|---|---|---|
| 1 | M | 61 | Lt. ankle | ALT free flap | Free flap | No necrosis |
| 2 | F | 27 | Scalp | ALT free flap | Free flap | No necrosis |
| 3 | M | 16 | Lt. ankle | ALT free flap | Free flap | No necrosis |
| 4 | M | 55 | Lt. lower leg | ALT free flap | Free flap | No necrosis |
| 5 | M | 72 | Philtrum | ALT free flap | Free flap | No necrosis |
| 6 | F | 66 | Lt. ankle | ALT free flap | Free flap | No necrosis |
| 7 | F | 100 | Lt. upper eyelid | ALT free flap | Free flap | No necrosis |
| 8 | M | 60 | Lt. foot | ALT free flap | Free flap | Total necrosis |
| 9 | M | 63 | Lt. ankle | ALT free flap | Free flap | No necrosis |
| 10 | M | 51 | Lt. foot | ALT free flap | Free flap | Total necrosis |
| 11 | F | 70 | Rt. foot | ALT free flap | Free flap | No necrosis |
| 12 | M | 48 | Lt. ankle | TDAP free flap → ALT free flap | Free flap | No necrosis |
| 13 | F | 23 | Lt. hand | SCIP free flap | Free flap | No necrosis |
| 14 | M | 75 | Scalp | ALT free flap → vastus lateralis muscle free flap | Free flap | Total necrosis |
| 15 | M | 81 | Nose | Nasolabial fold flap | Pedicled flap | No necrosis |
| 16 | M | 56 | Nose | Nasolabial fold flap | Pedicled flap | No necrosis |
| 17 | M | 52 | Nose | Nasolabial fold flap | Pedicled flap | No necrosis |
| 18 | M | 91 | Nose | Paramedian forehead flap | Pedicled flap | No necrosis |
| 19 | M | 57 | Nose | Paramedian forehead flap | Pedicled flap | No necrosis |
| 20 | M | 57 | Rt. lower leg | ALT pedicled flap | Pedicled flap | No necrosis |
| 21 | F | 49 | Rt. ankle | Peroneal artery perforator-based FC rotation flap | Pedicled flap | Partial necrosis |
| Necrosis Group (n = 4) | |
|---|---|
| Necrosis type | |
| Total necrosis | 3 |
| Partial necrosis | 1 |
| Vascular compromise | |
| Arterial insufficiency | 2 |
| Venous congestion | 2 |
| Non-Necrosis (n = 18) | Necrosis (n = 4) | Total Necrosis (n = 3) | Partial Necrosis (n = 1) | |
|---|---|---|---|---|
| Age (years) | 57.167 | 58.75 | ||
| Sex | ||||
| Male | 13 | 3 | ||
| Female | 5 | 1 | ||
| Temperature difference (dT) between normal skin and perforator (NS-PF) (°C) | ||||
| POD 0 | 1.817 | 1.55 (0.484) | 1.633 (0.740) | 1.3 (0.526) |
| POD 1 | 1.533 | 1.875 (0.434) | 2 (0.262) | 1.5 (0.842) |
| POD 2 | 1.528 | 2.2 (0.434) | 2.467 (0.262) | 1.4 (0.842) |
| POD 3 | 0.989 | 2.525 (0.001 *) | 2.533 (0.006 *) | 2.5 (0.105) |
| POD 7 | 0.706 | 3.5 (<0.001 *) | 4 (0.002 *) | 2 (0.105) |
| Temperature difference (dT) between perforator and average of flap (PF-AFP) (°C) | ||||
| POD 0 | 0.539 | 0.175 (0.118) | 0.2 | 0.1 |
| POD 1 | 0.35 | −0.175 (0.002 *) | −0.2 | −0.1 |
| POD 2 | 0.333 | −0.225 (0.003 *) | −0.2 | −0.3 |
| POD 3 | 0.617 | −0.375 (<0.001 *) | −0.233 | −0.8 |
| POD 7 | 0.489 | −0.225 (<0.001 *) | −0.333 | −0.1 |
| Variable | Coefficient | p-Value |
|---|---|---|
| Sex (male) | 0.475 | <0.001 |
| Flap type (free flap) | 0.185 | 0.611 |
| Flap type (pedicled flap) | −0.647 | 0.003 |
| Flap necrosis (necrosis) | 2.631 | <0.001 |
| Variable | Coefficient | p-Value |
|---|---|---|
| Sex (male) | −0.258 | 0.088 |
| Flap type (free flap) | −0.070 | 0.768 |
| Flap type (pedicled flap) | 0.093 | 0.515 |
| Flap necrosis (necrosis) | −0.716 | <0.001 |
| POD | t-Statistic | p-Value |
|---|---|---|
| NS-PF POD 0 | 0.927 | 0.366 |
| NS-PF POD 1 | 0.271 | 0.789 |
| NS-PF POD 2 | −0.217 | 0.831 |
| NS-PF POD 3 | −0.656 | 0.520 |
| NS-PF POD 7 | −1.547 | 0.139 |
| PF-AFP POD 0 | 1.554 | 0.138 |
| PF-AFP POD 1 | −0.054 | 0.957 |
| PF-AFP POD 2 | 0.326 | 0.748 |
| PF-AFP POD 3 | 0.068 | 0.946 |
| PF-AFP POD 7 | 0.610 | 0.550 |
| Monitoring Method | Advantages | Limitations | References |
|---|---|---|---|
| Clinical Examination | Non-invasive Widely available Low cost | Limited applicability in buried flaps Risk of poor interrater agreement due to inconsistent flap (failure) appearances | [18] |
| Acoustic Doppler Sonography | Non-invasive High sensitivity and specificity Real-time monitoring | Limited applicability in buried flaps Operator-dependent Limited ability to detect venous thrombosis | [17,18] |
| Implantable Doppler | Continuous monitoring High sensitivity and specificity Real-time monitoring | Invasive Requires surgical implantation Risk of infection Limited applicability in buried flaps | [17,18] |
| Indocyanine Green Fluorescence Angiography | Non-invasive High sensitivity and specificity Real-time monitoring Ability to detect venous thrombosis | Limited applicability in buried flaps Requires specialized equipment Limited ability to detect arterial thrombosis | [18,20] |
| Near-Infrared Spectroscopy | Non-invasive Real-time monitoring Ability to detect arterial thrombosis | Limited applicability in buried flaps Requires specialized equipment Limited ability to detect venous thrombosis | [19] |
| Tissue Oximetry | Non-invasive Real-time monitoring Ability to detect arterial thrombosis | Limited applicability in buried flaps Requires specialized equipment Limited ability to detect venous thrombosis | [12] |
| Transcutaneous Oximetry Measurement | Non-invasive Quantifying measurement Potential for thermal injury | Limited applicability in buried flaps Time required for measurement Low sensitivity | [23] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.; Kwak, S.H.; Byeon, J.Y.; Lee, D.W.; Kim, J.H.; Lim, S.; Choi, H.J. An Experimental and Clinical Study of Flap Monitoring with an Analysis of the Clinical Course of the Flap Using an Infrared Thermal Camera. Bioengineering 2024, 11, 688. https://doi.org/10.3390/bioengineering11070688
Kim H, Kwak SH, Byeon JY, Lee DW, Kim JH, Lim S, Choi HJ. An Experimental and Clinical Study of Flap Monitoring with an Analysis of the Clinical Course of the Flap Using an Infrared Thermal Camera. Bioengineering. 2024; 11(7):688. https://doi.org/10.3390/bioengineering11070688
Chicago/Turabian StyleKim, Hyun, Si Hyun Kwak, Je Yeon Byeon, Da Woon Lee, Jun Hyuk Kim, Soomin Lim, and Hwan Jun Choi. 2024. "An Experimental and Clinical Study of Flap Monitoring with an Analysis of the Clinical Course of the Flap Using an Infrared Thermal Camera" Bioengineering 11, no. 7: 688. https://doi.org/10.3390/bioengineering11070688
APA StyleKim, H., Kwak, S. H., Byeon, J. Y., Lee, D. W., Kim, J. H., Lim, S., & Choi, H. J. (2024). An Experimental and Clinical Study of Flap Monitoring with an Analysis of the Clinical Course of the Flap Using an Infrared Thermal Camera. Bioengineering, 11(7), 688. https://doi.org/10.3390/bioengineering11070688