



Explainable Precision Medicine in Breast MRI: A Combined Radiomics and Deep Learning Approach for the Classification of Contrast Agent Uptake
 , ,
, ,
Abstract

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Materials and Methods
2.1. MRI Datasets
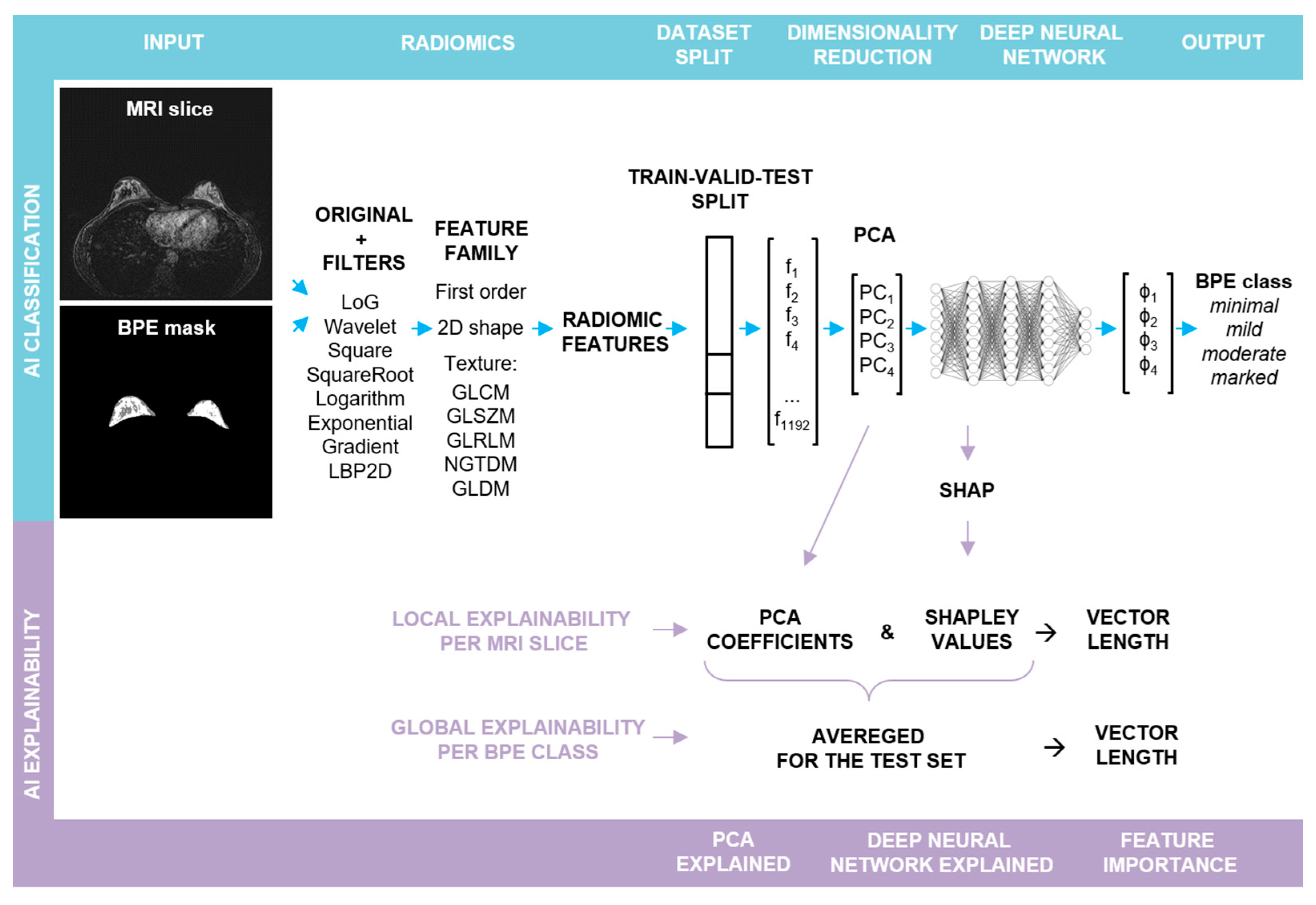
2.2. Explainable BPE Classification Pipeline
- (a)
- BPE Segmentation. The BPE was segmented in a semi-automatic way in a 3D slicer [22] using a grow from seeds algorithm as well as thresholding.
- (b)
- Radiomic feature extraction. Prior to slice-wise feature extraction, the volumes were normalized. PyRadiomics v. 3.0.1 was used for the extraction of radiomic features [23]. The resampling was performed with a Bspline interpolator, [1, 1] resampled pixel spacing, a pad distance of 10 and enabled pre-crop. The bin width for discretization was set to 20 and the voxel array shift to 300. First post-contrast subtraction MRI images with corresponding BPE masks served as the input for the radiomic toolbox: first order, shape, and texture features were extracted from each slice in its original form, as well as from the same slice after the application of different filters (cf. Figure 1). For each slice, 1192 features were obtained.
- (c)
- Train–validation–test split. In the first step, the dataset was split into two parts. The first part, containing approximately 80% of the data, was utilized for hyperparameter optimization through 5-fold cross-validation (CV). The optimized hyperparameters were then applied to train the final model, with the first part of the data serving as both the training and the validation sets (comprising 62% and 19% of slices, respectively) and the second part serving as an outer test set (comprising 19% of slices), cf. Figure S1. The initial split as well as the CV splits were performed randomly in a patient-stratified manner. As the distribution of the BPE classes in the dataset is imbalanced, the initial split was performed with the requirement that in each set, each BPE class had to be represented by a minimum of 10% slices with respect to all the slices contained in this set. For the cross validation, the requirement had to be lowered to a minimum of 2% slices.
- (d)
- Feature pre-processing and PCA. Feature standardization followed by PCA was performed for each training set, with the validation and the test sets being transformed accordingly.
- (e)
- Deep Neural Network: training and evaluation. A fully connected deep neural network (DNN) was built using sequential blocks consisting of dense layers, followed by batch normalization and dropout layers from the tensorflow.keras library. Hyperparameter tuning using different numbers of Principal Components (PCs) as input, different number of blocks with varying number of neurons and dropout rates, and different learning rates was performed (cf. Supporting Table S1). To ensure comparability, the random seed was fixed globally, and the weights were initialized with the use of the glorot uniform method and the biases at the value of zero. To compensate for the class imbalance, a weighted categorical cross-entropy loss was used. Each training run was performed for 150 epochs, and a model characterized by the lowest validation loss was chosen for the performance evaluation: confusion matrix and accuracy were calculated for the test set. For each parameter set, the mean and the standard deviation of accuracy of CV splits were calculated. Additionally, the confusion matrices were reviewed for false positive and false negative rates. The best parameter set was chosen, and the training was repeated for 10 runs without a fixed global random seed.Average accuracy and standard deviation were calculated for the resulting 10 models and p-value was computed using Student’s t-test (accuracy > 0.25). To evaluate a single model, bootstrap resampling with replacement was performed on the obtained predictions for a test set (n = 10,000). Accuracy and Cohen’s kappa (κ) scores were obtained for each resample and average values were calculated together with 95% confidence intervals (CI). p-values were determined utilizing Student’s t-test.The best performance was achieved for a deep neural network taking the first four PCs as input, with four blocks, each having 512, 256, 128, and 64 neurons in the dense layer, respectively. The dropout rate was equal to 0.45. The Adam optimizer with a learning rate of 0.0001 was applied. The training was performed in batches, each containing 50 samples.
- (f)
- Explainability. From the trained final models, two were chosen for detailed analysis with a focus on the explainability and its robustness. The results obtained for one of them are presented in the main text (including an evaluation on the external test set), whereas for the second one the results can be found in the Supplementary Material. The next sections describe the analysis in detail.
2.3. Shapley Values
2.4. Shapley-Scaled Vectors
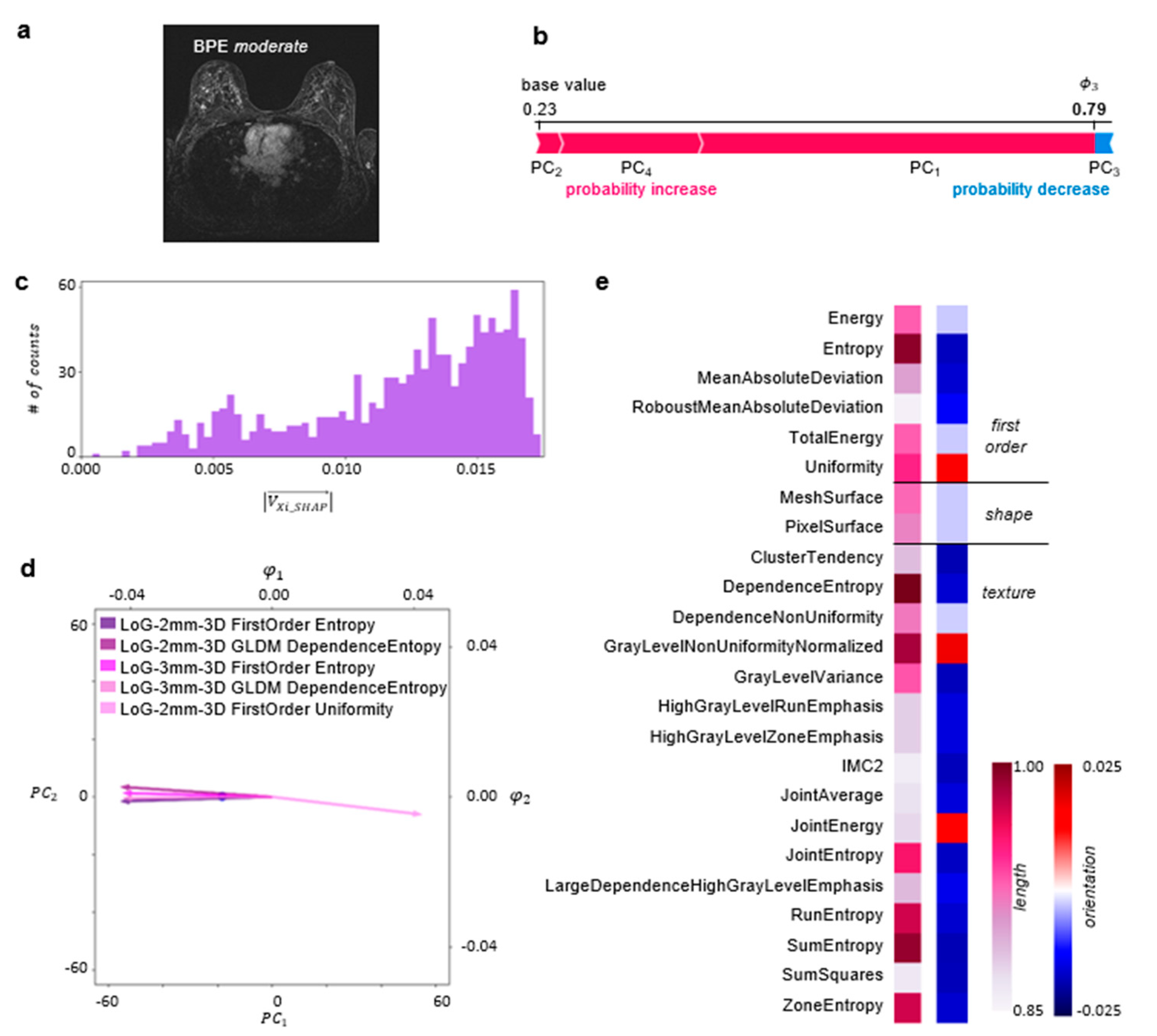
2.5. Local Explainability
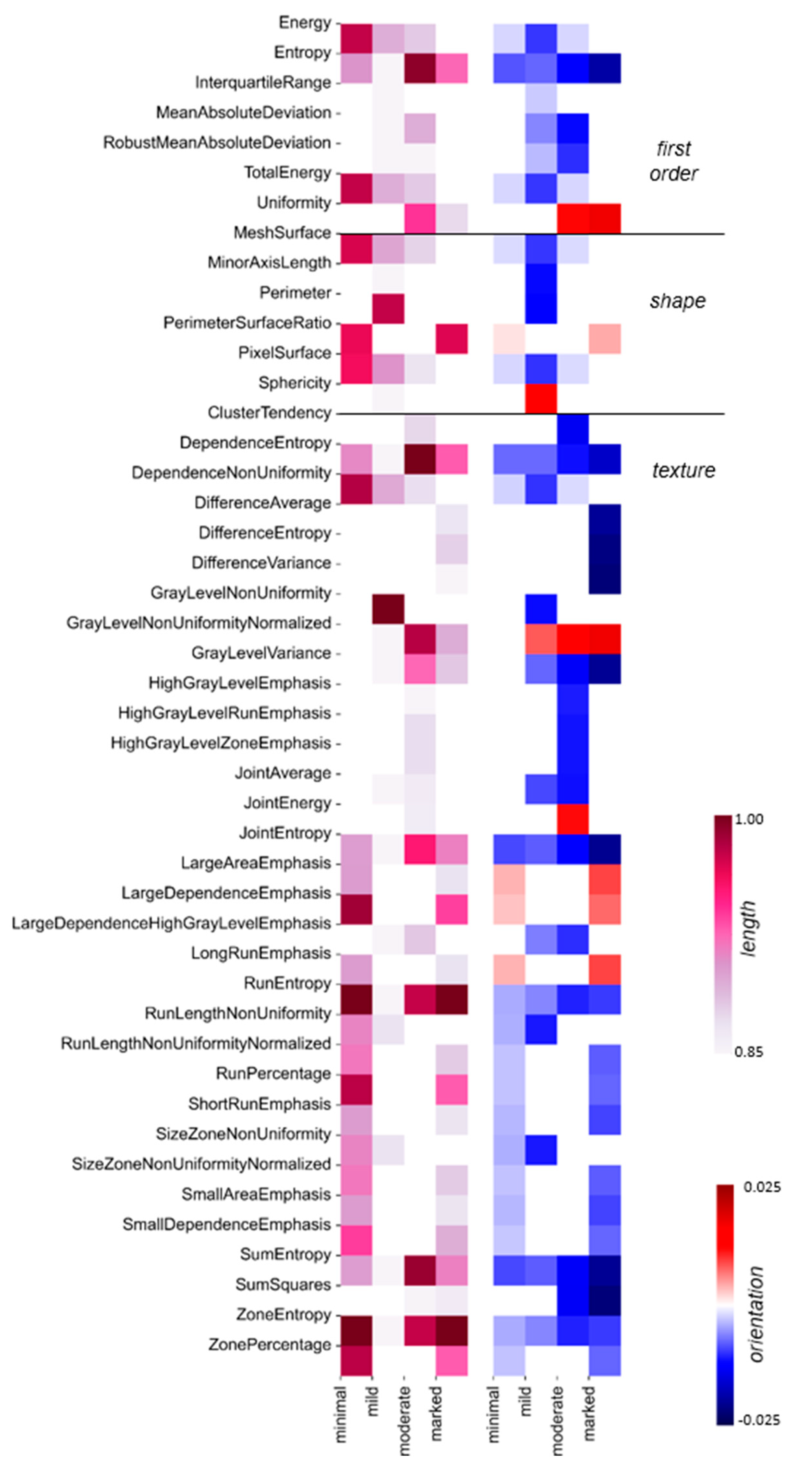
2.6. Global Explainability
3. Results
3.1. BPE Classification
3.2. Explainability of the BPE Classification
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, S.-Y.; Cho, N.; Park, I.-A.; Kwon, B.R.; Shin, S.U.; Kim, S.Y.; Lee, S.H.; Chang, J.M.; Moon, W.K. Dynamic Contrast-Enhanced Breast MRI for Evaluating Residual Tumor Size after Neoadjuvant Chemotherapy. Radiology 2018, 289, 327–334. [Google Scholar] [CrossRef]
- Mann, R.M.; Cho, N.; Moy, L. Breast MRI: State of the Art. Radiology 2019, 292, 520–536. [Google Scholar] [CrossRef]
- Hashem, L.M.B.; Gareer, S.W.Y.; Hashem, A.M.B.; Fakhry, S.; Tohamey, Y.M. Can DWI-MRI Be an Alternative to DCE-MRI in the Diagnosis of Troublesome Breast Lesions? Egypt. J. Radiol. Nucl. Med. 2021, 52, 138. [Google Scholar] [CrossRef]
- Scaranelo, A.M. What’s Hot in Breast MRI. Can. Assoc. Radiol. J. 2022, 73, 125–140. [Google Scholar] [CrossRef]
- Wekking, D.; Porcu, M.; De Silva, P.; Saba, L.; Scartozzi, M.; Solinas, C. Breast MRI: Clinical Indications, Recommendations, and Future Applications in Breast Cancer Diagnosis. Curr. Oncol. Rep. 2023, 25, 257–267. [Google Scholar] [CrossRef]
- Mann, R.M.; Athanasiou, A.; Baltzer, P.A.T.; Camps-Herrero, J.; Clauser, P.; Fallenberg, E.M.; Forrai, G.; Fuchsjäger, M.H.; Helbich, T.H.; Killburn-Toppin, F.; et al. Breast Cancer Screening in Women with Extremely Dense Breasts Recommendations of the European Society of Breast Imaging (EUSOBI). Eur. Radiol. 2022, 32, 4036–4045. [Google Scholar] [CrossRef]
- Liao, G.J.; Bancroft, L.H.; Strigel, R.M.; Chitalia, R.D.; Kontos, D.; Moy, L.; Partridge, S.C.; Rahbar, H. Background Parenchymal Enhancement on Breast MRI: A Comprehensive Review. J. Magn. Reson. Imaging 2020, 51, 43–61. [Google Scholar] [CrossRef]
- Bauer, E.; Levy, M.S.; Domachevsky, L.; Anaby, D.; Nissan, N. Background Parenchymal Enhancement and Uptake as Breast Cancer Imaging Biomarkers: A State-of-the-Art Review. Clin. Imaging 2022, 83, 41–50. [Google Scholar] [CrossRef]
- Uematsu, T.; Kasami, M.; Watanabe, J. Does the Degree of Background Enhancement in Breast MRI Affect the Detection and Staging of Breast Cancer? Eur. Radiol. 2011, 21, 2261–2267. [Google Scholar] [CrossRef]
- ACR BI-RADS MRI-Reporting. Available online: https://www.acr.org/-/media/ACR/Files/RADS/BI-RADS/MRI-Reporting.pdf (accessed on 15 December 2021).
- Grimm, L.J.; Anderson, A.L.; Baker, J.A.; Johnson, K.S.; Walsh, R.; Yoon, S.C.; Ghate, S.V. Interobserver Variability Between Breast Imagers Using the Fifth Edition of the BI-RADS MRI Lexicon. Am. J. Roentgenol. 2015, 204, 1120–1124. [Google Scholar] [CrossRef]
- Melsaether, A.; McDermott, M.; Gupta, D.; Pysarenko, K.; Shaylor, S.D.; Moy, L. Inter- and Intrareader Agreement for Categorization of Background Parenchymal Enhancement at Baseline and After Training. Am. J. Roentgenol. 2014, 203, 209–215. [Google Scholar] [CrossRef]
- Nam, Y.; Park, G.E.; Kang, J.; Kim, S.H. Fully Automatic Assessment of Background Parenchymal Enhancement on Breast MRI Using Machine-Learning Models. J. Magn. Reson. Imaging 2021, 53, 818–826. [Google Scholar] [CrossRef]
- Borkowski, K.; Rossi, C.; Ciritsis, A.; Marcon, M.; Hejduk, P.; Stieb, S.; Boss, A.; Berger, N. Fully Automatic Classification of Breast MRI Background Parenchymal Enhancement Using a Transfer Learning Approach. Medicine 2020, 99, e21243. [Google Scholar] [CrossRef]
- Dilorenzo, G.; Telegrafo, M.; La Forgia, D.; Stabile Ianora, A.A.; Moschetta, M. Breast MRI Background Parenchymal Enhancement as an Imaging Bridge to Molecular Cancer Sub-Type. Eur. J. Radiol. 2019, 113, 148–152. [Google Scholar] [CrossRef]
- Brooks, J.D.; Sung, J.S.; Pike, M.C.; Orlow, I.; Stanczyk, F.Z.; Bernstein, J.L.; Morris, E.A. MRI Background Parenchymal Enhancement, Breast Density and Serum Hormones in Postmenopausal Women. Int. J. Cancer 2018, 143, 823–830. [Google Scholar] [CrossRef]
- Nowakowska, S.; Borkowski, K.; Ruppert, C.M.; Landsmann, A.; Marcon, M.; Berger, N.; Boss, A.; Ciritsis, A.; Rossi, C. Generalizable Attention U-Net for Segmentation of Fibroglandular Tissue and Background Parenchymal Enhancement in Breast DCE-MRI. Insights Imaging 2023, 14, 185. [Google Scholar] [CrossRef]
- Ye, D.-M.; Wang, H.-T.; Yu, T. The Application of Radiomics in Breast MRI: A Review. Technol. Cancer Res. Treat. 2020, 19, 1533033820916191. [Google Scholar] [CrossRef]
- Pesapane, F.; Marco, P.D.; Rapino, A.; Lombardo, E.; Nicosia, L.; Tantrige, P.; Rotili, A.; Bozzini, A.C.; Penco, S.; Dominelli, V.; et al. How Radiomics Can Improve Breast Cancer Diagnosis and Treatment. J. Clin. Med. 2023, 12, 1372. [Google Scholar] [CrossRef]
- Eskreis-Winkler, S.; Sutton, E.J.; D’Alessio, D.; Gallagher, K.; Saphier, N.; Stember, J.; Martinez, D.F.; Morris, E.A.; Pinker, K. Breast MRI Background Parenchymal Enhancement Categorization Using Deep Learning: Outperforming the Radiologist. J. Magn. Reson. Imaging 2022, 56, 1068–1076. [Google Scholar] [CrossRef]
- Comstock, C.E.; Gatsonis, C.; Newstead, G.M.; Snyder, B.S.; Gareen, I.F.; Bergin, J.T.; Rahbar, H.; Sung, J.S.; Jacobs, C.; Harvey, J.A.; et al. Abbreviated Breast MRI and Digital Tomosynthesis Mammography in Screening Women with Dense Breasts (EA1141); The Cancer Imaging Archive: Little Rock, AR, USA, 2023. [Google Scholar]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.-C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an Image Computing Platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef]
- van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.-C.; Pieper, S.; Aerts, H.J.W.L. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [PubMed]
- Molnar, C. Interpretable Machine Learning: A Guide For Making Black Box Models Explainable; Independently Published: Munich, Germany, 2022; ISBN 9798411463330. [Google Scholar]
- Molnar, C. 9.6 SHAP (SHapley Additive exPlanations)|Interpretable Machine Learning. Available online: https://christophm.github.io/interpretable-ml-book/shapley.html (accessed on 5 January 2024).
- Scapicchio, C.; Gabelloni, M.; Barucci, A.; Cioni, D.; Saba, L.; Neri, E. A Deep Look into Radiomics. Radiol. Med. 2021, 126, 1296–1311. [Google Scholar] [CrossRef]
- Satake, H.; Ishigaki, S.; Ito, R.; Naganawa, S. Radiomics in Breast MRI: Current Progress toward Clinical Application in the Era of Artificial Intelligence. Radiol. Med. 2022, 127, 39–56. [Google Scholar] [CrossRef] [PubMed]
- Demircioğlu, A. Evaluation of the Dependence of Radiomic Features on the Machine Learning Model. Insights Imaging 2022, 13, 28. [Google Scholar] [CrossRef]
- Avanzo, M.; Wei, L.; Stancanello, J.; Vallières, M.; Rao, A.; Morin, O.; Mattonen, S.A.; El Naqa, I. Machine and Deep Learning Methods for Radiomics. Med. Phys. 2020, 47, e185–e202. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nowakowska, S.; Borkowski, K.; Ruppert, C.; Hejduk, P.; Ciritsis, A.; Landsmann, A.; Marcon, M.; Berger, N.; Boss, A.; Rossi, C. Explainable Precision Medicine in Breast MRI: A Combined Radiomics and Deep Learning Approach for the Classification of Contrast Agent Uptake. Bioengineering 2024, 11, 556. https://doi.org/10.3390/bioengineering11060556
Nowakowska S, Borkowski K, Ruppert C, Hejduk P, Ciritsis A, Landsmann A, Marcon M, Berger N, Boss A, Rossi C. Explainable Precision Medicine in Breast MRI: A Combined Radiomics and Deep Learning Approach for the Classification of Contrast Agent Uptake. Bioengineering. 2024; 11(6):556. https://doi.org/10.3390/bioengineering11060556
Chicago/Turabian StyleNowakowska, Sylwia, Karol Borkowski, Carlotta Ruppert, Patryk Hejduk, Alexander Ciritsis, Anna Landsmann, Magda Marcon, Nicole Berger, Andreas Boss, and Cristina Rossi. 2024. "Explainable Precision Medicine in Breast MRI: A Combined Radiomics and Deep Learning Approach for the Classification of Contrast Agent Uptake" Bioengineering 11, no. 6: 556. https://doi.org/10.3390/bioengineering11060556
APA StyleNowakowska, S., Borkowski, K., Ruppert, C., Hejduk, P., Ciritsis, A., Landsmann, A., Marcon, M., Berger, N., Boss, A., & Rossi, C. (2024). Explainable Precision Medicine in Breast MRI: A Combined Radiomics and Deep Learning Approach for the Classification of Contrast Agent Uptake. Bioengineering, 11(6), 556. https://doi.org/10.3390/bioengineering11060556