
The Development and Implementation of Innovative Blind Source Separation Techniques for Real-Time Extraction and Analysis of Fetal and Maternal Electrocardiogram Signals



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. System Architecture
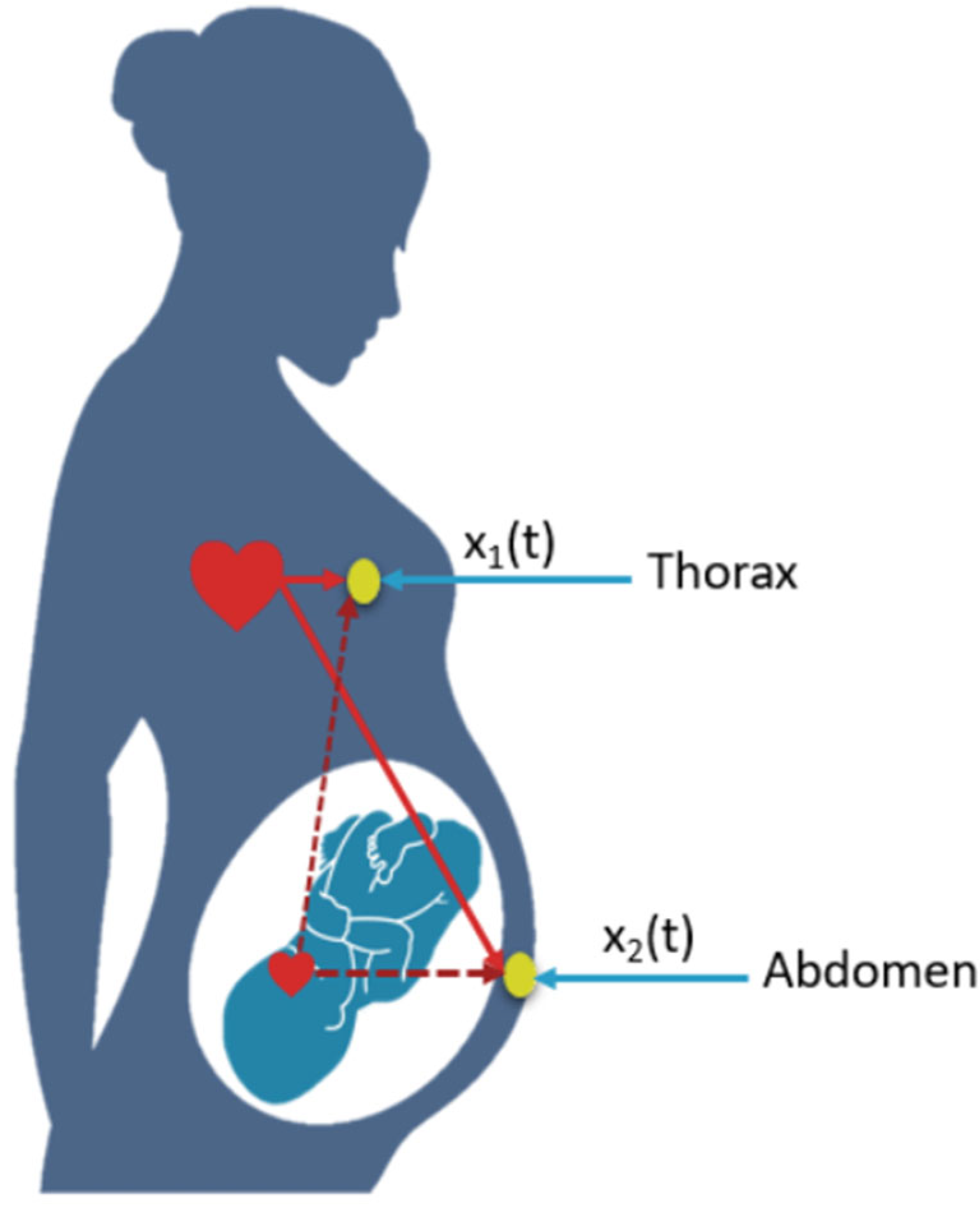
- Acquisition Block: The acquisition system consists of two electrodes, one placed on the abdomen and the other on the thorax of a pregnant woman. The signals captured by these electrodes will be sent in real time to a separation and processing system;
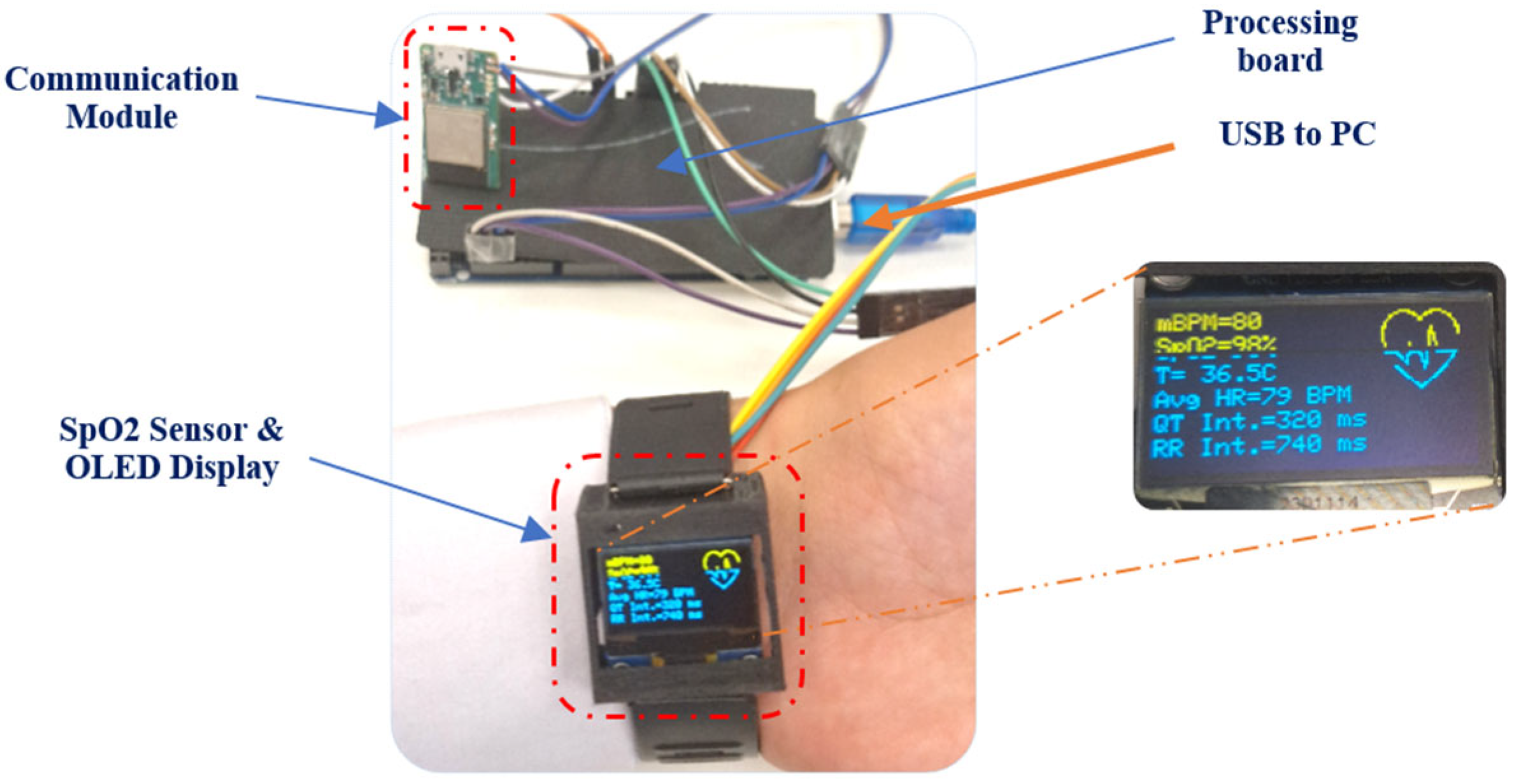
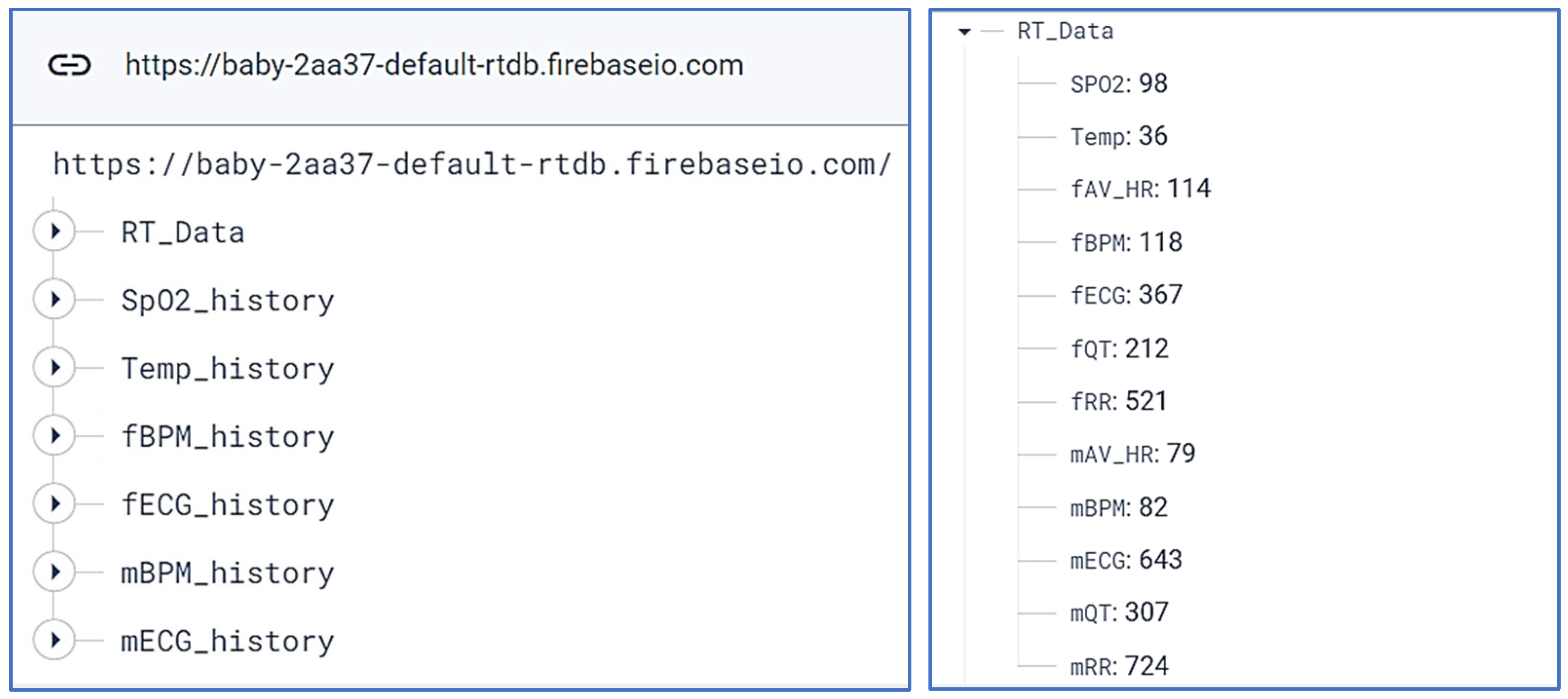
- Separation and Communication System: This block consists of a high-performance on-board board for extracting the ECG signal from the fetus and its mother based on blind source separation algorithms, then calculating the heartbeat and extracting information related to each signal, such as the duration of each ECG wave. The card also measures blood oxygen saturation using a SpO2 sensor, after which these data are displayed on an OLED display and sent to an online database to facilitate fetal monitoring online or via a smartphone application;
- Supervision System: This is a smartphone application that serves as a secure platform, enabling not only parents but also the family doctor to remotely monitor and supervise the state of health of the fetus and its mother. Equipped with an alert system and full tracking of historical data, it provides a real-time overview of vital health parameters, promoting better care and peace of mind for families expecting a fetus.
2.2. ECG Fetal
2.3. Composite ECG of a Pregnant Woman
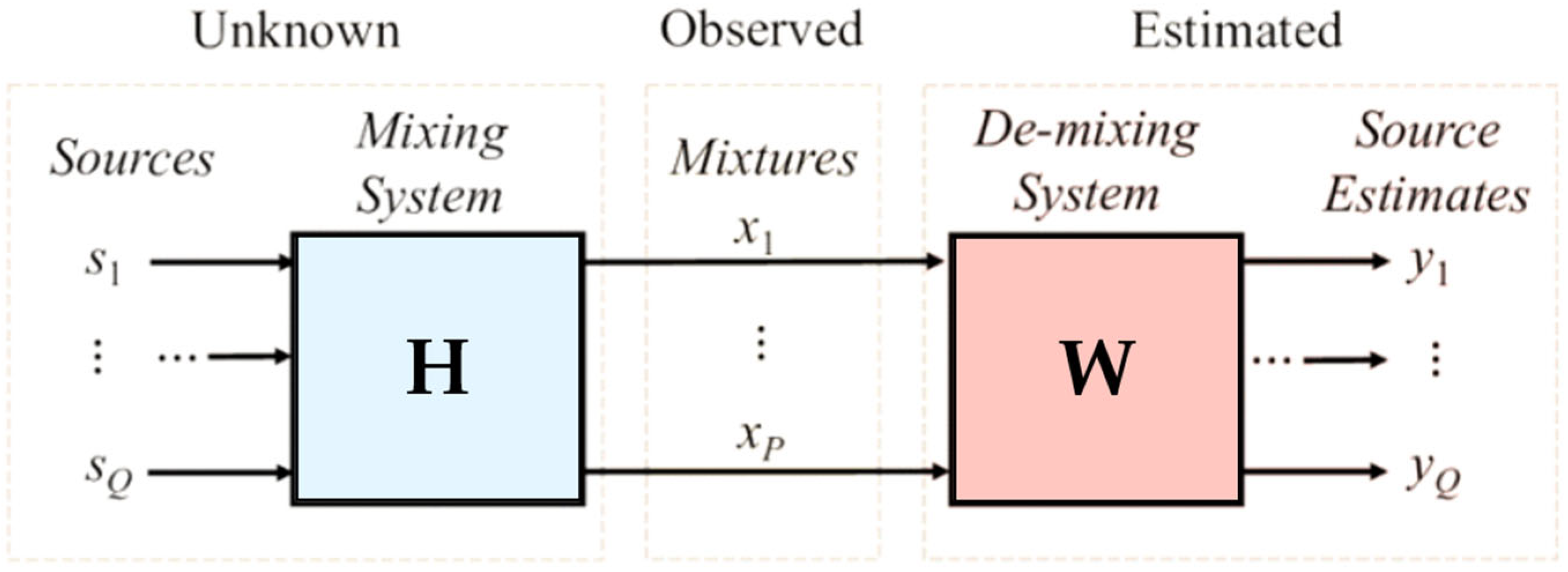
2.4. About Blind Source Separation
- The sources are statistically independent;
- The number of sensors is higher or equal to the number of sources;
- A mixing matrix between the sources and the sensors.
- x(k): the vector containing the observations;
- s(k): the vector containing N signals emitted by N unknown sources;
- y(k): the vector of estimated sources;
- H: mixture matrix of size Q × P;
- W: the estimated Matrix H = W−1.
3. Implementation Results
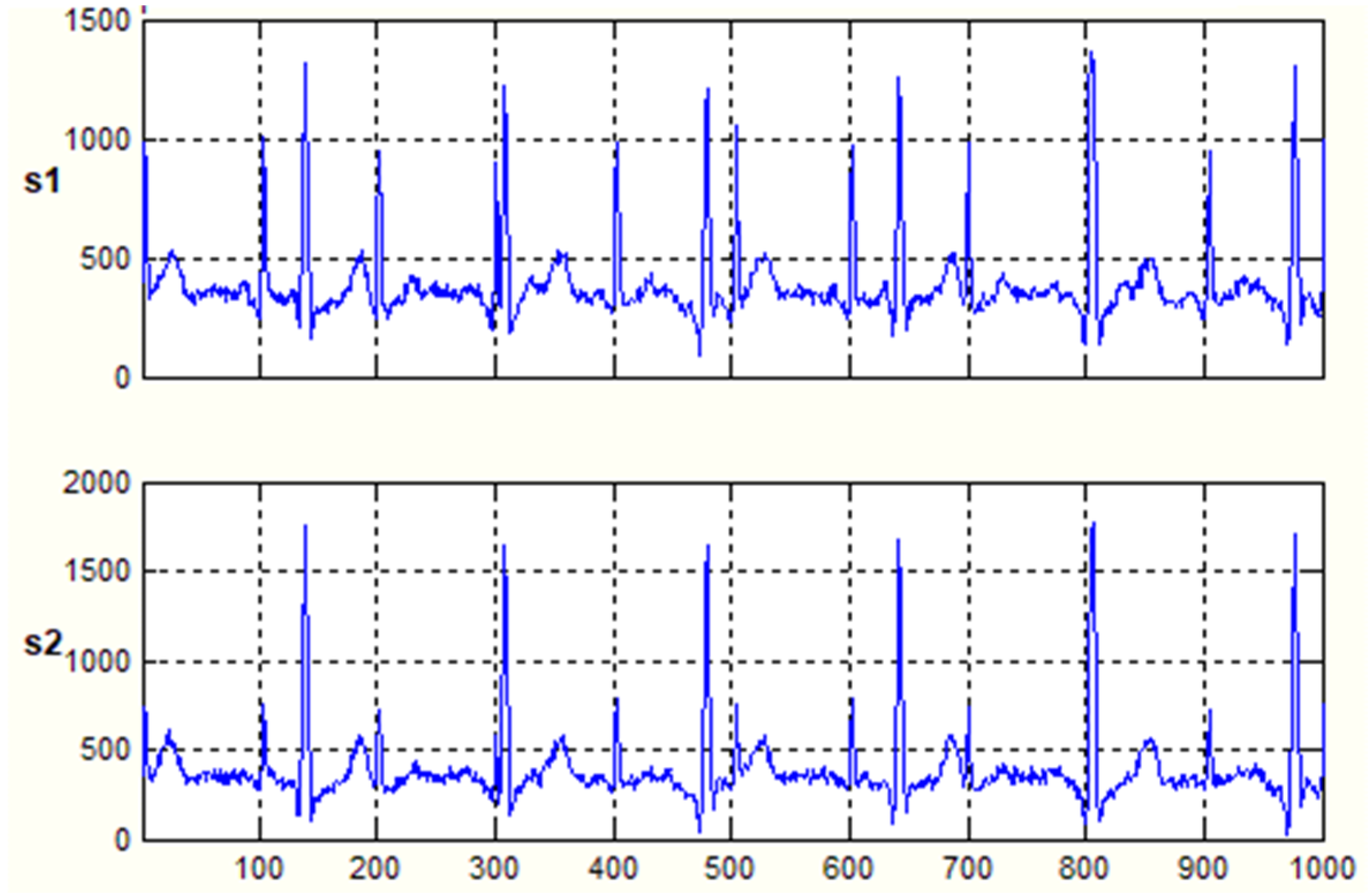
3.1. Database
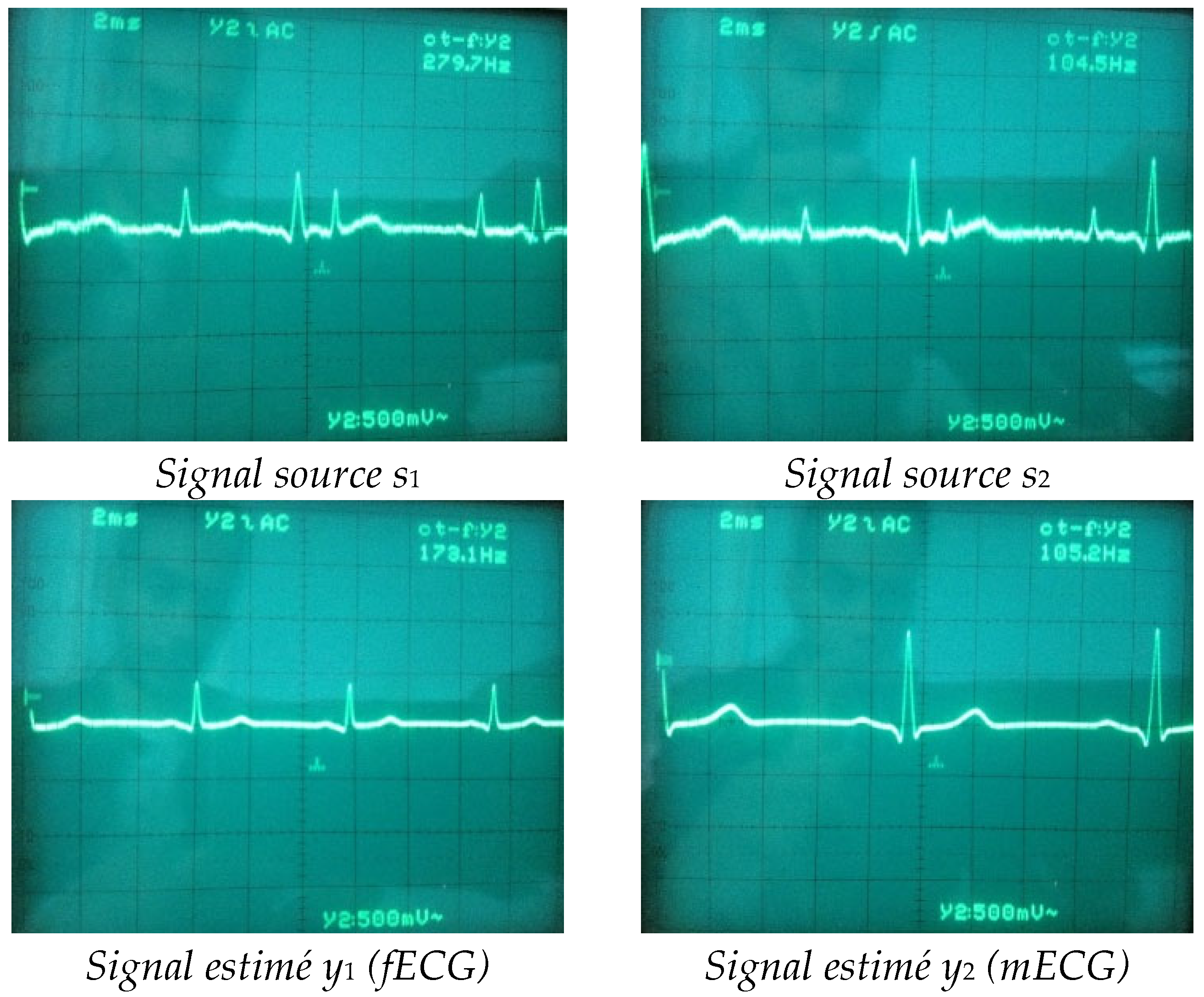
3.2. Hardware Implementation
- Maternal heart rate (mBPM);
- Fetal heart rate (fBPM);
- Oxygen saturation level (SpO2);
- Pregnant woman’s body temperature (T);
- The time interval between the R wave and the T wave (QT Interval);
- Variation in time between each R-R heartbeat (RR).
- The first option enables exporting and sharing all data related to the ECG signals and the history of fBPM and mBPM.
- The second option enables sharing a screenshot of the real-time results, including the graph, via various connectivity tools, such as email or social media.
- The third option provides information about the mother and her fetus and technical support details.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- El Idrissi Slitine, N.; Bennaoui, F.; Sable, C.A.; Martin, G.R.; Hom, L.A.; Fadel, A.; Moussaoui, S.; Inajjarne, N.; Boumzebra, D.; Mouaffak, Y.; et al. Pulse Oximetry and Congenital Heart Disease Screening: Results of the First Pilot Study in Morocco. Int. J. Neonatal Screen. 2020, 6, 53. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Gu, A.; Xiao, Z.; Xing, Y.; Yang, C.; Li, J.; Liu, C. Wearable Fetal ECG Monitoring System from Abdominal Electrocardiography Recording. Biosensors 2022, 12, 475. [Google Scholar] [CrossRef] [PubMed]
- Matonia, A.; Jezewski, J.; Kupka, T.; Jezewski, M.; Horoba, K.; Wrobel, J.; Czabanski, R.; Kahankowa, R. Fetal electrocardiograms, direct and abdominal with reference heartbeat annotations. Sci. Data 2020, 7, 200. [Google Scholar] [CrossRef] [PubMed]
- Benahmed, A.; Mekhfioui, M.; Guennoun, Z. FPGA based Hardware Co-Simulation Implementation for Real-Time Image Blind Separation using ICA Algorithms. Int. J. Emerg. Technol. Adv. Eng. 2022, 12, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Hao, J.; Yang, Y.; Zhou, Z.; Wu, S. Fetal Electrocardiogram Signal Extraction Based on Fast Independent Component Analysis and Singular Value Decomposition. Sensors 2022, 22, 3705. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-González, A.; Castañeda-Villa, N. Blind extraction of fetal and maternal components from the abdominal electrocardiogram: An ICA implementation for low-dimensional recordings. Biomed. Signal Process. Control 2020, 58, 101836. [Google Scholar] [CrossRef]
- Hasan, M.A.; Ibrahimy, M.I.; Reaz, M.B.I.; Uddin, M.J.; Hussain, M.S. VHDL modeling of FECG extraction from the composite abdominal ECG using Atificial Intelligence. In Proceedings of the 2009 IEEE International Conference on Industrial Technology, Churchill, VIC, Australia, 10–13 February 2009; pp. 1–5. [Google Scholar] [CrossRef]
- Chareonsak, C.; Sana, F.; Wei, Y.; Bing, X. Design of FPGA hardware for a real-time blind source separation of fetal ECG signals. In Proceedings of the 2004 IEEE International Workshop on Biomedical Circuits and Systems, Singapore, 1–3 December 2004; pp. S2/4–13. [Google Scholar] [CrossRef]
- Torti, E.; Koliopoulos, D.; Matraxia, M.; Danese, G.; Leporati, F. Custom FPGA processing for real-time fetal ECG extraction and identification. Comput. Biol. Med. 2017, 80, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Pani, D.; Dessì, A.; Cabras, B.; Raffo, L. A real-time algorithm for tracking of foetal ECG sources obtained by block-on-line BSS techniques. In Proceedings of the 2012 Computing in Cardiology, Krakow, Poland, 9–12 September 2012; pp. 65–68. [Google Scholar]
- Vasudeva, B.; Deora, P.; Pradhan, P.M.; Dasgupta, S. Efficient implementation of LMS adaptive filter-based FECG extraction on an FPGA. Healthc. Technol. Lett. 2020, 7, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Raj, A.; Brablik, J.; Kahankova, R.; Jaros, R.; Barnova, K.; Snasel, V.; Mirjalili, S.; Martinek, R. Nature inspired method for noninvasive fetal ECG extraction. Sci. Rep. 2022, 12, 20159. [Google Scholar] [CrossRef]
- Dash, S.S.; Nath, M.K.; Anbalagan, T. Identification of FECG from AECG Recordings using ICA over EMD. Proceedings of 2023 International Conference on Medical Imaging and Computer-Aided Diagnosis (MICAD 2023), Cambridge, UK, 9–10 December 2023; Su, R., Zhang, Y.D., Frangi, A.F., Eds.; Lecture Notes in Electrical Engineering. Springer: Singapore, 2024; Volume 1166. [Google Scholar] [CrossRef]
- Sarafan, S.; Le, T.; Lau, M.P.H.; Hameed, A.; Ghirmai, T.; Cao, H. Fetal Electrocardiogram Extraction from the Mother’s Abdominal Signal Using the Ensemble Kalman Filter. Sensors 2022, 22, 2788. [Google Scholar] [CrossRef]
- Shi, X.; Yamamoto, K.; Ohtsuki, T.; Matsui, Y.; Owada, K. Unsupervised Learning-Based Non-Invasive Fetal ECG Muti-Level Signal Quality Assessment. Bioengineering 2023, 10, 66. [Google Scholar] [CrossRef] [PubMed]
- Subha, T.D.; Reshma, V.D. A study of non-invasiveheart rate monitoring system by using FPGA. Mater. Today Proc. 2017, 4, 4228–4238. [Google Scholar] [CrossRef]
- Boudet, S.; Houzé de l’Aulnoit, A.; Peyrodie, L.; Demailly, R.; Houzé de l’Aulnoit, D. Use of Deep Learning to Detect the Maternal Heart Rate and False Signals on Fetal Heart Rate Recordings. Biosensors 2022, 12, 691. [Google Scholar] [CrossRef]
- Karpiński, R.; Krakowski, P.; Jonak, J.; Machrowska, A.; Maciejewski, M.; Nogalski, A. Diagnostics of Articular Cartilage Damage Based on Generated Acoustic Signals Using ANN—Part I: Femoral-Tibial Joint. Sensors 2022, 22, 2176. [Google Scholar] [CrossRef] [PubMed]
- Karpiński, R.; Krakowski, P.; Jonak, J.; Machrowska, A.; Maciejewski, M.; Nogalski, A. Diagnostics of Articular Cartilage Damage Based on Generated Acoustic Signals Using ANN—Part II: Patellofemoral Joint. Sensors 2022, 22, 3765. [Google Scholar] [CrossRef] [PubMed]
- Mekhfioui, M.; Elgouri, R.; Satif, A.; Hlou, L. Real-time implementation of a new efficient algorithm for source separation using matlab & arduino due. Int. J. Sci. Technol. Res. 2020, 9, 531–535. [Google Scholar]
- Zhang, Y.; Yu, S. Single-lead noninvasive fetal ECG extraction by means of combining clustering and principal components analysis. Med. Biol. Eng. Comput. 2020, 58, 419–432. [Google Scholar] [CrossRef] [PubMed]
- Abel, J.D.K.; Dhanalakshmi, S.; Kumar, R. A comprehensive survey on signal processing and machine learning techniques for non-invasive fetal ECG extraction. Multimed. Tools Appl. 2023, 82, 1373–1400. [Google Scholar] [CrossRef]
- Zhong, W.; Liao, L.; Guo, X.; Wang, G. Fetal electrocardiography extraction with residual convolutional encoder–decoder networks. Australas. Phys. Eng. Sci. Med. 2019, 42, 1081–1089. [Google Scholar] [CrossRef]
- Rashkovska, A.; Avbelj, V. Abdominal fetal ECG measured with differential ECG sensor. In Proceedings of the 2017 40th International Convention on Information and Communication Technology, Electronics and Microelectronics (MIPRO), Opatija, Croatia, 22–26 May 2017; pp. 289–291. [Google Scholar]
- Varanini, M.; Tartarisco, G.; Balocchi, R.; Macerata, A.; Pioggia, G.; Billeci, L. A new method for QRS complex detection in multichannel ECG: Application to self-monitoring of fetal health. Comput. Biol. Med. 2017, 85, 125–134. [Google Scholar] [CrossRef]
- Ramli, D.A.; Shiong, Y.H.; Hassan, N. Blind Source Separation (BSS) of Mixed Maternal and Fetal Electrocardiogram (ECG) Signal: A comparative Study. Procedia Comput. Sci. 2020, 176, 582–591. [Google Scholar] [CrossRef]
- Mekhfioui, M.; Elgouri, R.; Satif, A.; Benahmed, A.; Hamzaoui, E.; Abdelkader, H.; Hlou, L. A Comparative Study and Implementation of Blind Source Separation Algorithm using MATLAB and TMS320c6713 DSK. J. Eng. Appl. Sci. 2020, 15, 1074–1081. [Google Scholar] [CrossRef]
- Behar, J.; Andreotti, F.; Zaunseder, S.; Li, Q.; Oster, J.; Clifford, G.D. An ECG model for simulating maternal-foetal activity mixtures on abdominal ECG recordings. Physiol. Meas. 2014, 35, 1537–1550. [Google Scholar] [CrossRef] [PubMed]
- Andreotti, F.; Behar, J.; Zaunseder, S.; Oster, J.; Clifford, G.D. An Open-Source Framework for Stress-Testing Non-Invasive Foetal ECG Extraction Algorithms. Physiol Meas 2016, 5, 627–648. [Google Scholar] [CrossRef] [PubMed]
- Keenan, E.; Karmakar, C.K.; Palaniswami, M. The effects of asymmetric volume conductor modeling on non-invasive fetal ECG extraction. Physiol. Meas. 2018, 39, 105–113. [Google Scholar] [CrossRef]
- Mekhfioui, M.; Elgouri, R.; Satif, A.; Moumouh, M.; Hlou, L. Implementation of least mean square algorithm using arduino & Simulink. Int. J. Sci. Technol. Res. 2020, 9, 664–667. [Google Scholar]
- Benahmed, A.; Mekhfioui, M.; Hamzaoui, E.M.; Guennoun, Z. FPGA Implementation of Adaptive Zero-Tracking Algorithm For Real-Time Doa Estimation Using A Linear Antenna Array. ASEAN Eng. J. 2024, 14, 207–212. [Google Scholar] [CrossRef]
- Cichocki, A.; Osowski, S.; Siwek, K. Prewhitening Algorithms of Signals in the Presence of White Noise. In Proceedings of the 6th International Workshop Computational Problems of Electrical Engineering, Zakopane, Poland, 1–4 September 2004. [Google Scholar]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mekhfioui, M.; Benahmed, A.; Chebak, A.; Elgouri, R.; Hlou, L. The Development and Implementation of Innovative Blind Source Separation Techniques for Real-Time Extraction and Analysis of Fetal and Maternal Electrocardiogram Signals. Bioengineering 2024, 11, 512. https://doi.org/10.3390/bioengineering11050512
Mekhfioui M, Benahmed A, Chebak A, Elgouri R, Hlou L. The Development and Implementation of Innovative Blind Source Separation Techniques for Real-Time Extraction and Analysis of Fetal and Maternal Electrocardiogram Signals. Bioengineering. 2024; 11(5):512. https://doi.org/10.3390/bioengineering11050512
Chicago/Turabian StyleMekhfioui, Mohcin, Aziz Benahmed, Ahmed Chebak, Rachid Elgouri, and Laamari Hlou. 2024. "The Development and Implementation of Innovative Blind Source Separation Techniques for Real-Time Extraction and Analysis of Fetal and Maternal Electrocardiogram Signals" Bioengineering 11, no. 5: 512. https://doi.org/10.3390/bioengineering11050512
APA StyleMekhfioui, M., Benahmed, A., Chebak, A., Elgouri, R., & Hlou, L. (2024). The Development and Implementation of Innovative Blind Source Separation Techniques for Real-Time Extraction and Analysis of Fetal and Maternal Electrocardiogram Signals. Bioengineering, 11(5), 512. https://doi.org/10.3390/bioengineering11050512