
Upper Midline Correction Using the Mesial-Distalslider

 ,
, 

Abstract

1. Introduction
2. Materials and Methods
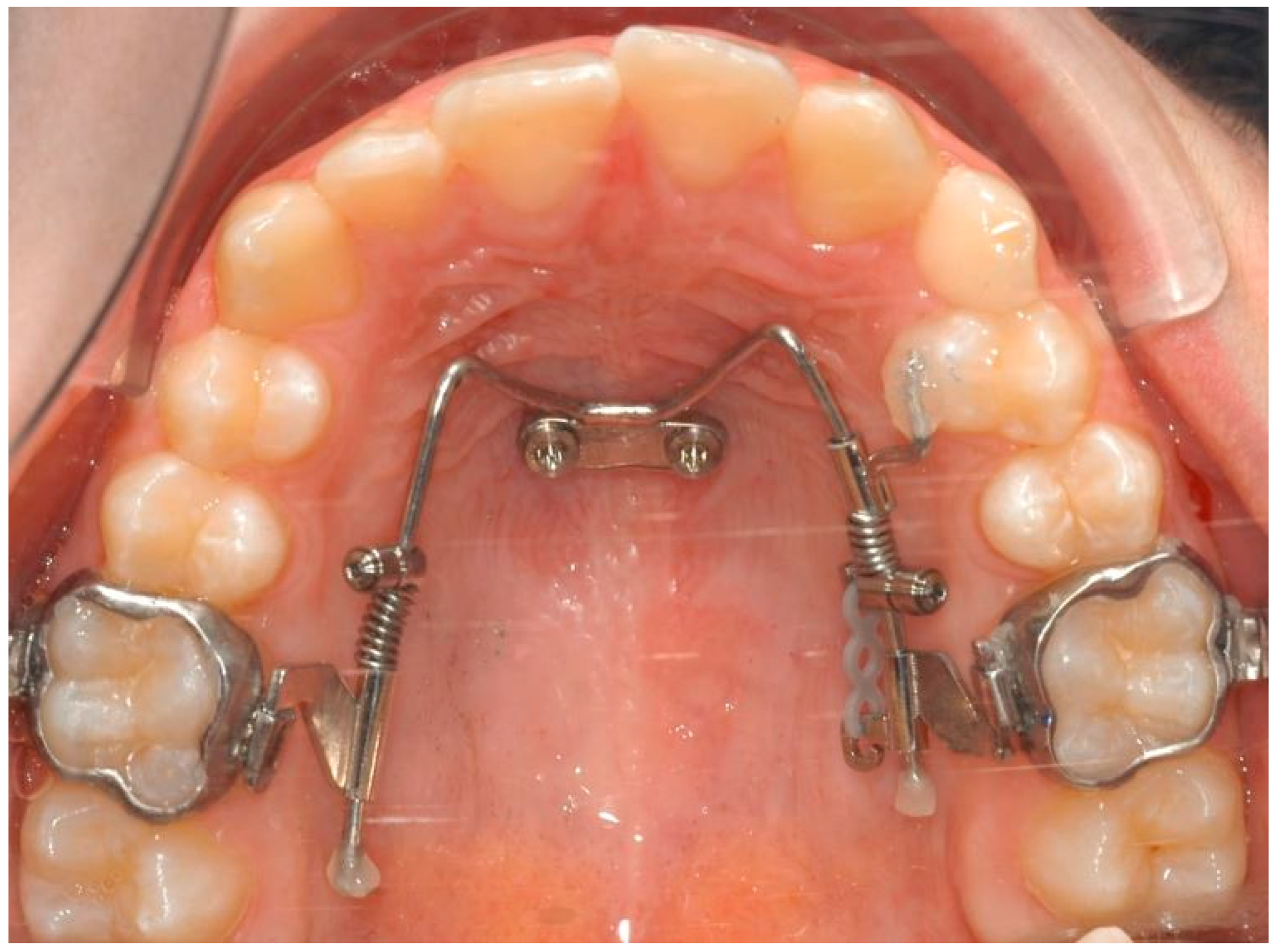
2.1. The Appliance
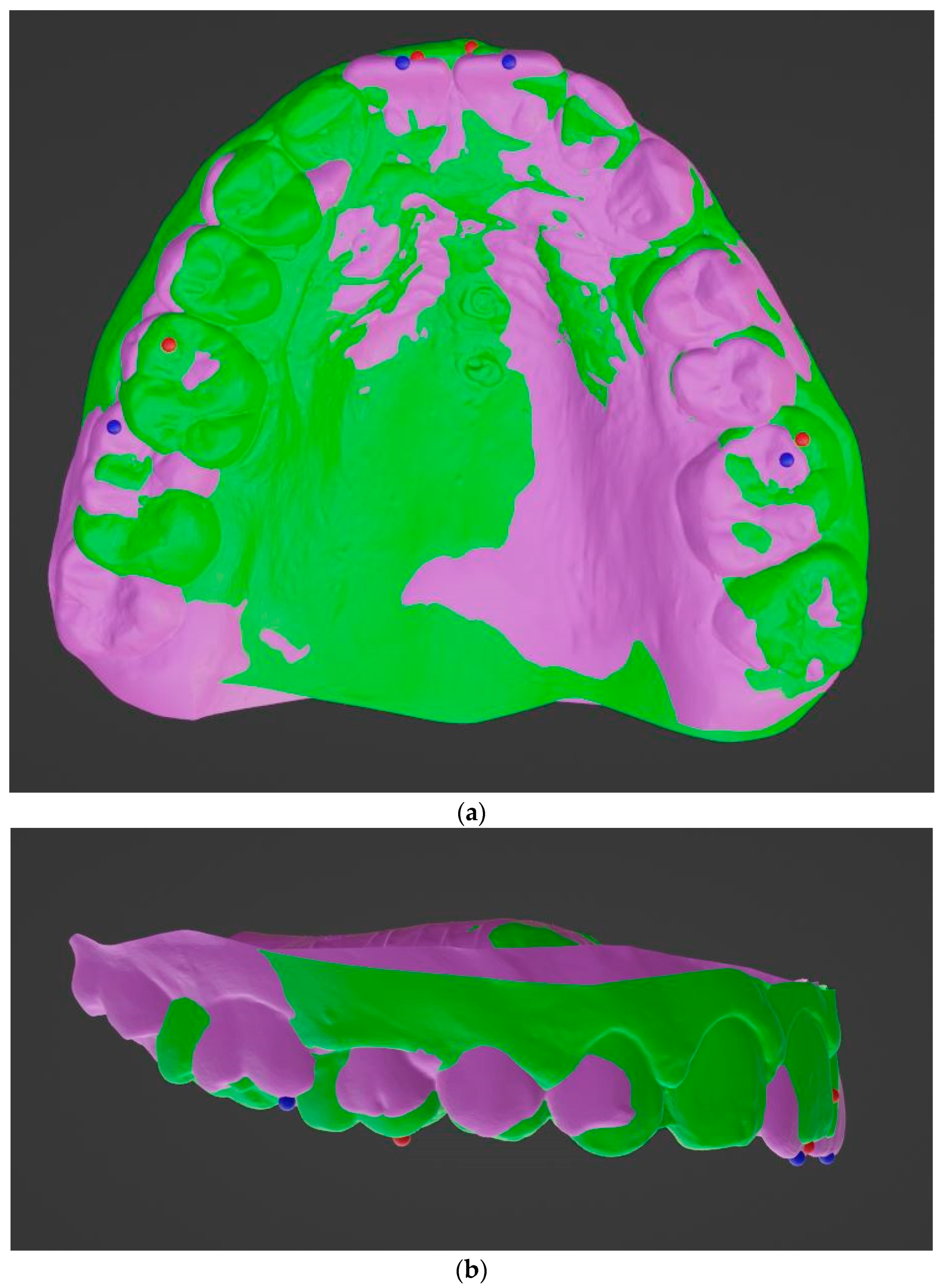
2.2. Statistical Analysis
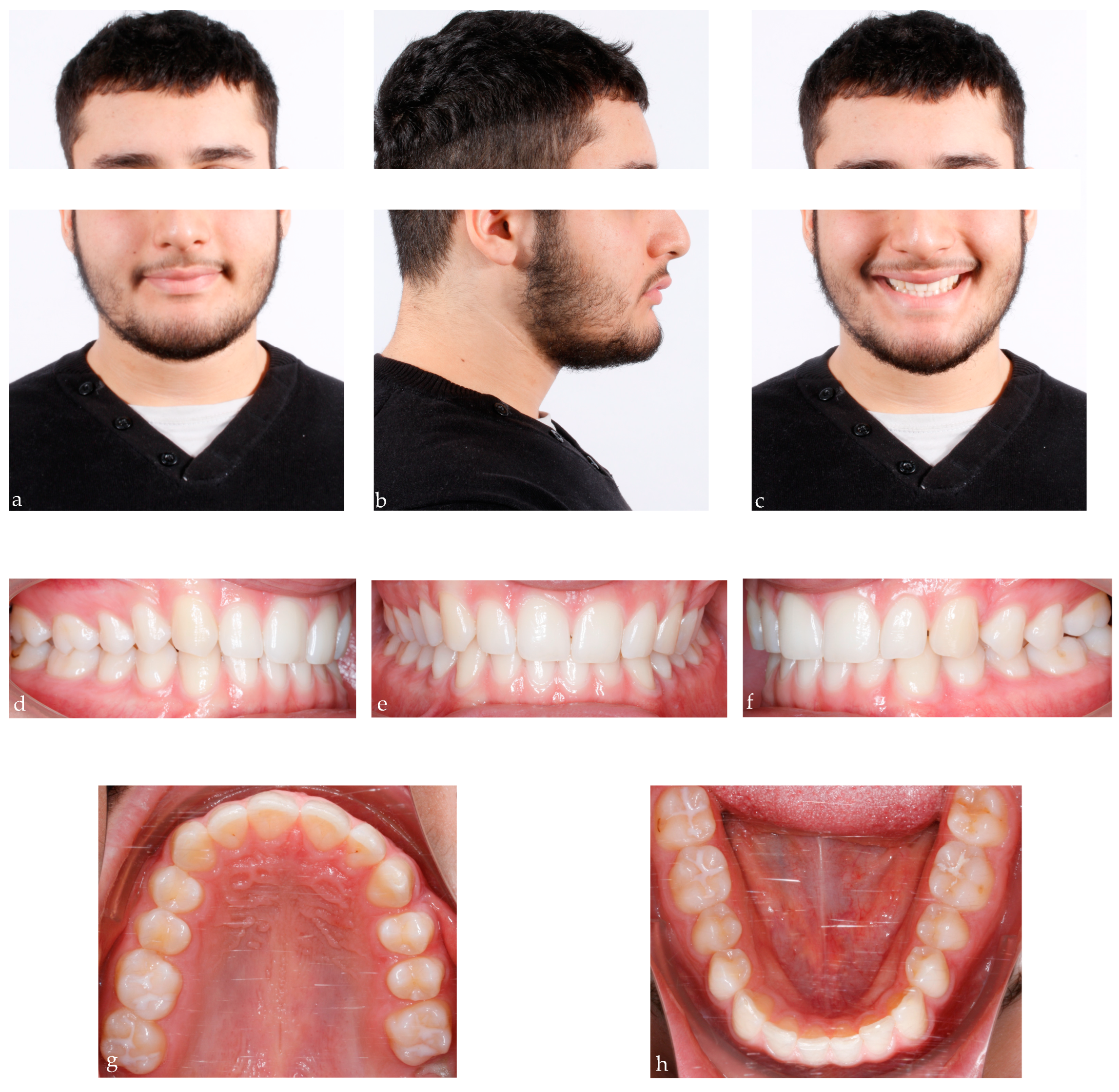
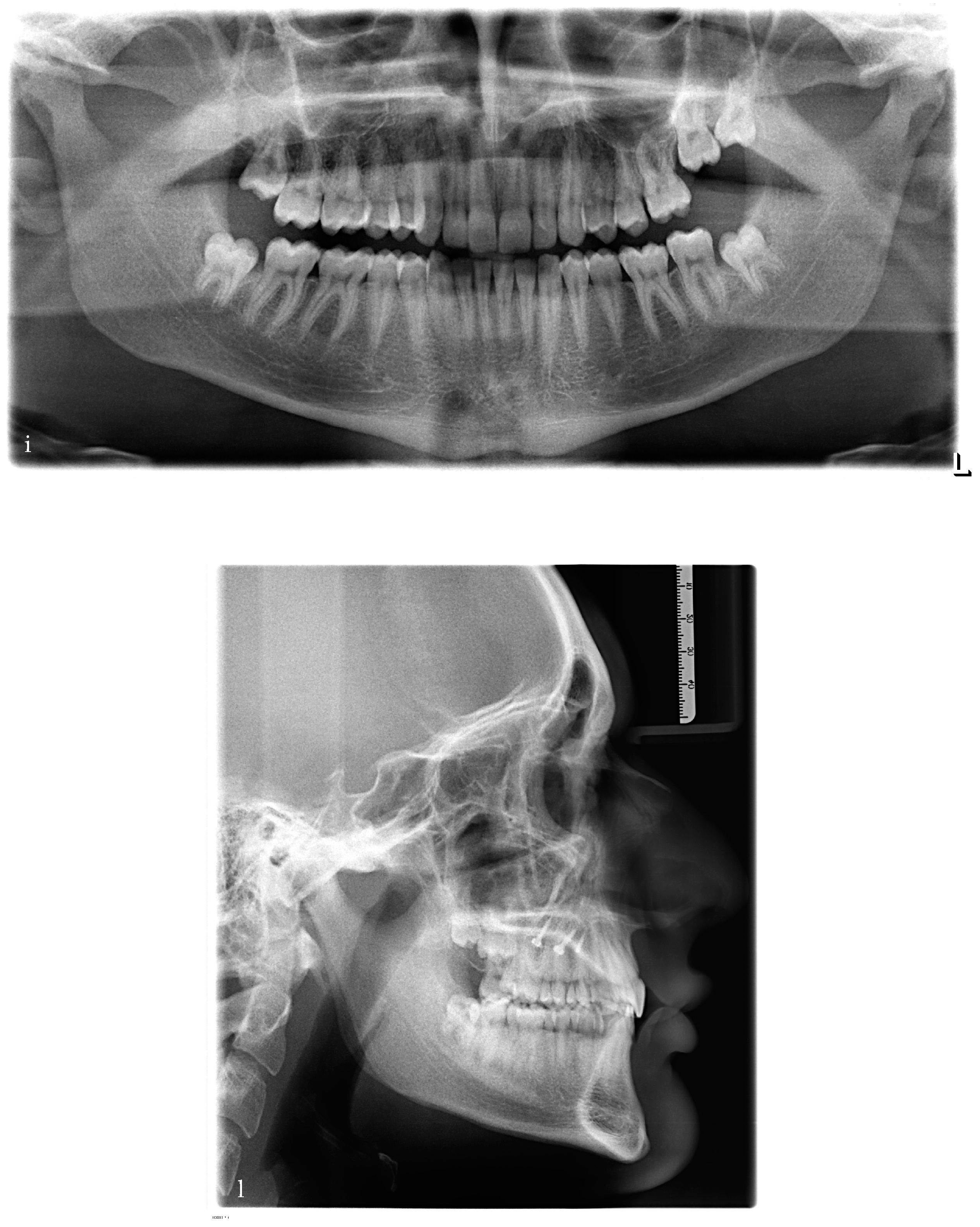
2.3. Case Description
2.4. Treatment Objectives and Alternatives
- The first option, corresponding to our choice, involved the distalization of the upper right quadrant in order to reach the molar and canine Class I occlusion and to correct the upper midline deviation. At the same time, it involved the mesialization of the upper left quadrant in order to close the spaces opened during the treatment.
- The second option involved the extraction of the upper right first premolar in order to correct the Class II canine relationship and the deviation of the upper midline.
3. Results
3.1. Mesialization Side
3.2. Distalization Side
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lewis, P.D. The deviated midline. Am. J. Orthod. 1976, 70, 601–616. [Google Scholar] [CrossRef]
- Shroff, B.; Lindauer, S.J.; Burstone, C.J. Class II subdivision treatment with tip-back moments. Eur. J. Orthod. 1997, 19, 93–101. [Google Scholar] [CrossRef]
- Daskalogiannakis, J.; World Federation of Orthodontists. Glossary of Orthodontic Terms; Quintessence Books: Chicago, IL, USA; London, UK, 2000. [Google Scholar]
- Arnett, G.W.; Bergman, R.T. Facial keys to orthodontic diagnosis and treatment planning. Part I Am. J. Orthod. Dentofac. Orthop. 1993, 103, 299–312. [Google Scholar] [CrossRef] [PubMed]
- Beyer, J.W.; Lindauer, J. Evaluation of dental midline position. Semin. Orthod. 1998, 4, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Johnston, C.D.; Burden, D.J.; Stevenson, M.R. The influence of dental to facial midline discrepancies on dental attractiveness ratings. Eur. J. Orthod. 1999, 21, 517–522. [Google Scholar] [CrossRef]
- Ker, A.J.; Chan, R.; Fields, H.W.; Beck, M.; Rosenstiel, S. Esthetics and Smile Characteristics from the Layperson’s Perspective: A Computer-Based Survey Study. J. Am. Dent. Assoc. 2008, 139, 1318–1327. [Google Scholar] [CrossRef] [PubMed]
- Burstone, C.J. Diagnosis and treatment planning of patients with asymmetries. Semin. Orthod. 1998, 4, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Chrapla, P.; Paradowska-Stolarz, A.; Skoskiewicz-Malinowska, K. Subjective and Objective Evaluation of the Symmetry of Maxillary Incisors among Residents of Southwest Poland. Symmetry 2022, 14, 1257. [Google Scholar] [CrossRef]
- Gallão, S.; Ortolani, C.L.F.; Santos-Pinto, A.; Santos-Pinto, L.A.M.; Faltin, K., Jr. Análise Fotográfica Da Simetria e Da Proporção Estética Dos Dentes Anteriores—Photographic Analysis of Symmetry and Aesthetic Proportion of Anterior Teeth. Rev. Inst. Ciênc. 2010, 27, 400–404. [Google Scholar]
- Costa, A.; Raffaini, M.; Melsen, B. Miniscrews as orthodontic anchorage: A preliminary report. Int. J. Adult Orthodon Orthognath. Surg. 1998, 13, 201–209. [Google Scholar]
- Fritz, U.; Diedrich, P.; Kinzinger, G.; Al-Said, M. The anchorage quality of mini-implants towards translatory and extrusive forces. J. Orofac. Orthop. 2003, 64, 293–304, (In English, German). [Google Scholar] [CrossRef] [PubMed]
- Lim, H.J.; Choi, Y.J.; Evans, C.A.; Hwang, H.S. Predictors of initial stability of orthodontic miniscrew implants. Eur. J. Orthod. 2011, 33, 528–532. [Google Scholar] [CrossRef] [PubMed]
- Baumgaertel, S. Temporary skeletal anchorage devices: The case for miniscrews. Am. J. Orthod. Dentofac. Orthop. 2014, 145, 558–564. [Google Scholar] [CrossRef] [PubMed]
- Kuroda, S.; Sugawara, Y.; Deguchi, T.; Kyung, H.-M.; Takano-Yamamoto, T. Clinical use of miniscrew implants as orthodontic anchorage: Success rates and postoperative discomfort. Am. J. Orthod. Dentofac. Orthop. 2007, 131, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Wilmes, B.; Nanda, R.; Nienkemper, M.; Ludwig, B.; Drescher, D. Correction of upper-arch asymmetries using the Mesial-Distalslider. J. Clin. Orthod. 2013, 47, 648–655. [Google Scholar] [PubMed]
- Wilmes, B.; Nienkemper, M.; Ludwig, B.; Kau, C.H.; Pauls, A.; Drescher, D. Esthetic Class II treatment with the Beneslider and aligners. J. Clin. Orthod. 2012, 46, 390–398. [Google Scholar] [PubMed]
- Wilmes, B.; Drescher, D. Application and effectiveness of the Beneslider: A device to move molars distally. World J. Orthod. 2010, 11, 331–340. [Google Scholar] [PubMed]
- Wilmes, B.; Nienkemper, M.; Nanda, R.; Lübberink, G.; Drescher, D. Palatally anchored maxillary molar mesialization using the Mesialslider. J. Clin. Orthod. 2013, 47, 172–179. [Google Scholar] [PubMed]
- Wilhelmy, L.; Willmann, J.H.; Tarraf, N.E.; Wilmes, B.; Drescher, D. Maxillary space closure using a digital manufactured Mesialslider in a single appointment workflow. Korean J. Orthod. 2022, 52, 236–245. [Google Scholar] [CrossRef]
- Wilmes, B.; Drescher, D. CAD-CAM Workflows for Palatal TAD Anchored Appliances, Seminars in Orthodontics. Semin. Orthod. 2023, 29, 51–59. [Google Scholar] [CrossRef]
- Wilmes, B.; Schwarze, J.; Vasudavan, S.; Drescher, D. Maxillary Space Closure Using Aligners and Palatal Mini-Implants in Patients with Congenitally Missing Lateral Incisors. J. Clin. Orthod. 2021, 55, 20–33. [Google Scholar]
- Becker, K.; Wilmes, B.; Grandjean, C.; Drescher, D. Impact of manual control point selection accuracy on automated surface matching of digital dental models. Clin. Oral. Investig. 2018, 22, 801–810. [Google Scholar] [CrossRef]
- Almeida, M.A.; Phillips, C.; Kula, K.; Tulloch, C. Stability of the palatal rugae as landmarks for analysis of dental casts. Angle Orthod. 1995, 65, 43–48. [Google Scholar]
- Hoggan, B.R.; Sadowsky, C. The use of palatal rugae for the assessment of anteroposterior tooth movements. Am. J. Orthod. Dentofac. Orthop. 2001, 119, 482–488. [Google Scholar] [CrossRef]
- Kim, H.K.; Moon, S.C.; Lee, S.J.; Park, Y.S. Three-dimensional biometric study of palatine rugae in children with a mixed-model analysis: A 9-year longitudinal study. Am. J. Orthod. Dentofac. Orthop. 2012, 141, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Choi, D.S.; Jeong, Y.M.; Jang, I.; Jost-Brinkmann, P.G.; Cha, B.K. Accuracy and reliability of palatal superimposition of three-dimensional digital models. Angle Orthod. 2010, 80, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.I.; Cha, B.K.; Jost-Brinkmann, P.G.; Choi, D.S.; Jang, I.S. Validity of palatal superimposition of 3-dimensional digital models in cases treated with rapid maxillary expansion and maxillary protraction headgear. Korean J. Orthod. 2012, 42, 235–241. [Google Scholar] [CrossRef]
- Ashmore, J.L.; Kurland, B.F.; King, G.J.; Wheeler, T.T.; Ghafari, J.; Ramsay, D.S. A 3-dimensional analysis of molar movement during headgear treatment. Am. J. Orthod. Dentofac. Orthop. 2002, 121, 18–29; discussion 29–30. [Google Scholar] [CrossRef] [PubMed]
- Proffit, W.R.; Fields, H.W.; Larson, B.; Sarver, D.M. Contemporary, 6th ed.; Mosby Elsevier: St. Louis, MO, USA, 2018; pp. 262–263. [Google Scholar]
- Cornelis, M.A.; Scheffler, N.R.; De Clerck, H.J.; Tulloch, J.F.; Behets, C.N. Systematic review of the experimental use of temporary skeletal anchorage devices in orthodontics. Am. J. Orthod. Dentofac. Orthop. 2007, 131 (Suppl. S4), S52–S58. [Google Scholar] [CrossRef]
- Cha, J.-Y.; Kil, J.-K.; Yoon, T.-M.; Hwang, C.-J. Miniscrew stability evaluated with computerized tomography scanning. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 73–79. [Google Scholar] [CrossRef]
- Ludwig, B.; Glasl, B.; Bowman, S.J.; Wilmes, B.; Kinzinger, G.S.; Lisson, J.A. Anatomical guidelines for miniscrew insertion: Palatal sites. J. Clin. Orthod. 2011, 45, 433–441, quiz 467. [Google Scholar] [PubMed]
- Rebellato, J. Asymmetric extractions used in the treatment of patients with asymmetries. Semin. Orthod. 1998, 4, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Ciavarella, D.; Maci, M.; Guida, L.; Cazzolla, A.P.; Muzio, E.L.; Tepedino, M. Correction of Midline Deviation and Unilateral Crossbite Treated with Fixed Appliance. Case Rep. Dent. 2023, 2023, 5620345. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.J.; Chang, H.H.; Huang, C.Y.; Hung, H.C.; Lai, E.H.H.; Yao, C.C.J. A retrospective analysis of the failure rate of three different orthodontic skeletal anchorage systems. Clin. Oral. Implant. Res. 2007, 18, 768–775. [Google Scholar] [CrossRef] [PubMed]
- Lai, E.H.; Yao, C.C.; Chang, J.Z.; Chen, I.; Chen, Y.J. Three-dimensional dental model analysis of treatment outcomes for protrusive maxillary dentition: Comparison of headgear, miniscrew, and miniplate skeletal anchorage. Am. J. Orthod. Dentofac. Orthop. 2008, 134, 636–645. [Google Scholar] [CrossRef]
- Kilkis, D.; Celikoglu, M.; Nur, M.; Bayram, M.; Candirli, C. Effects of zygoma-gear appliance for unilateral maxillary molar distalization: A prospective clinical study. Am. J. Orthod. Dentofac. Orthop. 2016, 150, 989–996. [Google Scholar] [CrossRef] [PubMed]
- Oberti, G.; Villegas, C.; Ealo, M.; Palacio, J.C.; Baccetti, T. Maxillary molar distalization with the dual-force distalizer supported by mini-implants: A clinical study. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 282.e1–282.e5. [Google Scholar] [CrossRef] [PubMed]
- Vilanova, L.; Castillo, A.A.-D.; Bellini-Pereira, S.A.; Henriques, J.F.C.; Janson, G.; Garib, D.; Patel, M.P.; Grec, R.H.d.C.; Yatabe, M.; Cevidanes, L.; et al. Three-dimensional changes after maxillary molar distalization with a miniscrew-anchored cantilever. Angle Orthod. 2023, 93, 513–523. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, L.; Colonna, A.; Carlucci, A.; Oliverio, T.; Siciliani, G. Class II subdivision correction with clear aligners using intermaxilary elastics. Prog. Orthod. 2018, 19, 32. [Google Scholar] [CrossRef]
- Alcan, T.; Ceylanoğlu, C. Upper midline correction in conjunction with rapid maxillary expansion. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 671–675. [Google Scholar] [CrossRef]
- Maspero, C.; Giannini, L.; Galbiati, G.; Farronato, G. Modified transversal sagittal maxillary expander for correction of upper midline deviation associated with maxillary arch deficiency. Minerva Stomatol. 2015, 64, 53–58, (In English, Italian). [Google Scholar] [PubMed]
- Migliorati, M.; Signori, A.; Silvestrini-Biavati, A. Temporary anchorage device stability: An evaluation of thread shape factor. Eur. J. Orthod. 2012, 34, 582–586. [Google Scholar] [CrossRef] [PubMed]
- Pradal, A.; Nucci, L.; Derton, N.; De Felice, M.E.; Turco, G.; Grassia, V.; Contardo, L. Mechanical Evaluation of the Stability of One or Two Miniscrews under Loading on Synthetic Bone. J. Funct. Biomater. 2020, 11, 80. [Google Scholar] [CrossRef] [PubMed]
- Ferrillo, M.; Nucci, L.; Gallo, V.; Bruni, A.; Montrella, R.; Fortunato, L.; Giudice, A.; Perillo, L. Temporary anchorage devices in orthodontics: A bibliometric analysis of the 50 most-cited articles from 2012 to 2022. Angle Orthod. 2023, 93, 591–602. [Google Scholar] [CrossRef] [PubMed]
- Wilmes, B.; Ludwig, B.; Vasudavan, S.; Nienkemper, M.; Drescher, D. The T-Zone: Median vs. Paramedian Insertion of Palatal Mini-Implants. J. Clin. Orthod. 2016, 50, 543–551. [Google Scholar] [PubMed]
- Han, C.-M.; Watanabe, K.; Tsatalis, A.E.; Lee, D.; Zheng, F.; Kyung, H.-M.; Deguchi, T.; Kim, D.-G. Evaluations of miniscrew type-dependent mechanical stability. Clin. Biomech. 2019, 69, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Chang, Z.-C.J.; Chen, Y.-J.; Tung, Y.-Y.; Chiang, Y.-Y.; Lai, E.H.-H.; Chen, W.-P.; Lin, C.-P. Effects of thread depth, taper shape, and taper length on the mechanical properties of mini-implants. Am. J. Orthod. Dentofac. Orthop. 2012, 141, 279–288. [Google Scholar] [CrossRef]
- Lee, J.; Jeong, Y.; Pittman, J.; Deguchi, T.; Johnston, W.M.; Fields, H.W.; Kim, D.-G. Primary stability and viscoelastic displacement of mini-implant system under loading. Clin. Biomech. 2017, 41, 28–33. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mesialization Side | ||||||||
|---|---|---|---|---|---|---|---|---|
| Molar Movement (mm) | Axys | Mean | SD | Min | Max | 25th | Median | 75th |
| y | 4.5 | 2.2 | 0.0 | 8.4 | 3.1 | 4.9 | 5.8 | |
| x | −0.4 | 2.4 | −5.0 | 4.3 | −1.4 | −0.1 | 1.1 | |
| z | 0.3 | 0.9 | −1.9 | 1.6 | −0.2 | 0.4 | 1.2 | |
| Incisor Movement (mm) | y | 0.9 | 1.7 | −2.8 | 5.3 | 0.0 | 0.3 | 1.9 |
| Distalization side | ||||||||
| Molar Movement (mm) | Axys | Mean | SD | Min | Max | 25th | Median | 75th |
| y | −2.4 | 1.7 | −4.6 | −0.0 | −4.2 | −2.4 | −0.5 | |
| x | −0.5 | 1.5 | −2.9 | 1.4 | −1.9 | −0.6 | 1.0 | |
| z | 0.2 | 1.4 | −2.0 | 2.4 | −0.5 | −0.1 | 1.6 | |
| Incisor Movement (mm) | y | 0.6 | 0.7 | −0.4 | 1.8 | 0.1 | 0.3 | 1.3 |
| Mesialization Side | Distalization Side | |||||||
|---|---|---|---|---|---|---|---|---|
| Molar Movements | T0 | T1 | Mean Differences | p Value | T0 | T1 | Mean Differences | p Value |
| y (antero-posterior) | −2.7 (SD 4) | 1.7 (SD 4.5) | 4.4 (SD 2.2) | 0.000 | −0.3 (SD 6.3) | −2.4 (SD 6.2) | −2.1 (SD 1.5) | 0.006 |
| x (transversal) | 4 (SD 26) | 3.6 (SD 24.1) | −0.4 (SD 2.4) | 0.515 | −6.7 (SD 25.7) | −7.3 (SD 27.1) | −0.5 (SD 1.5) | 0.322 |
| z (vertical) | 5.8 (SD 3.1) | 7.7 (SD 1,6) | 0.4 (SD 0.9) | 0.122 | 7.1 (SD 1.5) | 7.3 (SD 0.5) | 0.2 (SD 1.4) | 0.698 |
| Incisors Displacement | T0 | T1 | Mean differences | p value | T0 | T1 | Mean differences | p value |
| y (antero-posterior) | 21.1 (SD 10.4) | 22.1 (SD 10.7) | 0.9 (SD 1.7) | 0.042 | 25.4 (SD 3.6) | 26 (SD 3.3) | 0.6 (SD 0.7) | 0.048 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Felice, M.E.; Caruso, S.; Kueffer, M.; Gatto, R.; Wilmes, B. Upper Midline Correction Using the Mesial-Distalslider. Bioengineering 2024, 11, 450. https://doi.org/10.3390/bioengineering11050450
De Felice ME, Caruso S, Kueffer M, Gatto R, Wilmes B. Upper Midline Correction Using the Mesial-Distalslider. Bioengineering. 2024; 11(5):450. https://doi.org/10.3390/bioengineering11050450
Chicago/Turabian StyleDe Felice, Maria Elena, Silvia Caruso, Maximilian Kueffer, Roberto Gatto, and Benedict Wilmes. 2024. "Upper Midline Correction Using the Mesial-Distalslider" Bioengineering 11, no. 5: 450. https://doi.org/10.3390/bioengineering11050450
APA StyleDe Felice, M. E., Caruso, S., Kueffer, M., Gatto, R., & Wilmes, B. (2024). Upper Midline Correction Using the Mesial-Distalslider. Bioengineering, 11(5), 450. https://doi.org/10.3390/bioengineering11050450