

Precision Identification of Locally Advanced Rectal Cancer in Denoised CT Scans Using EfficientNet and Voting System Algorithms

 , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
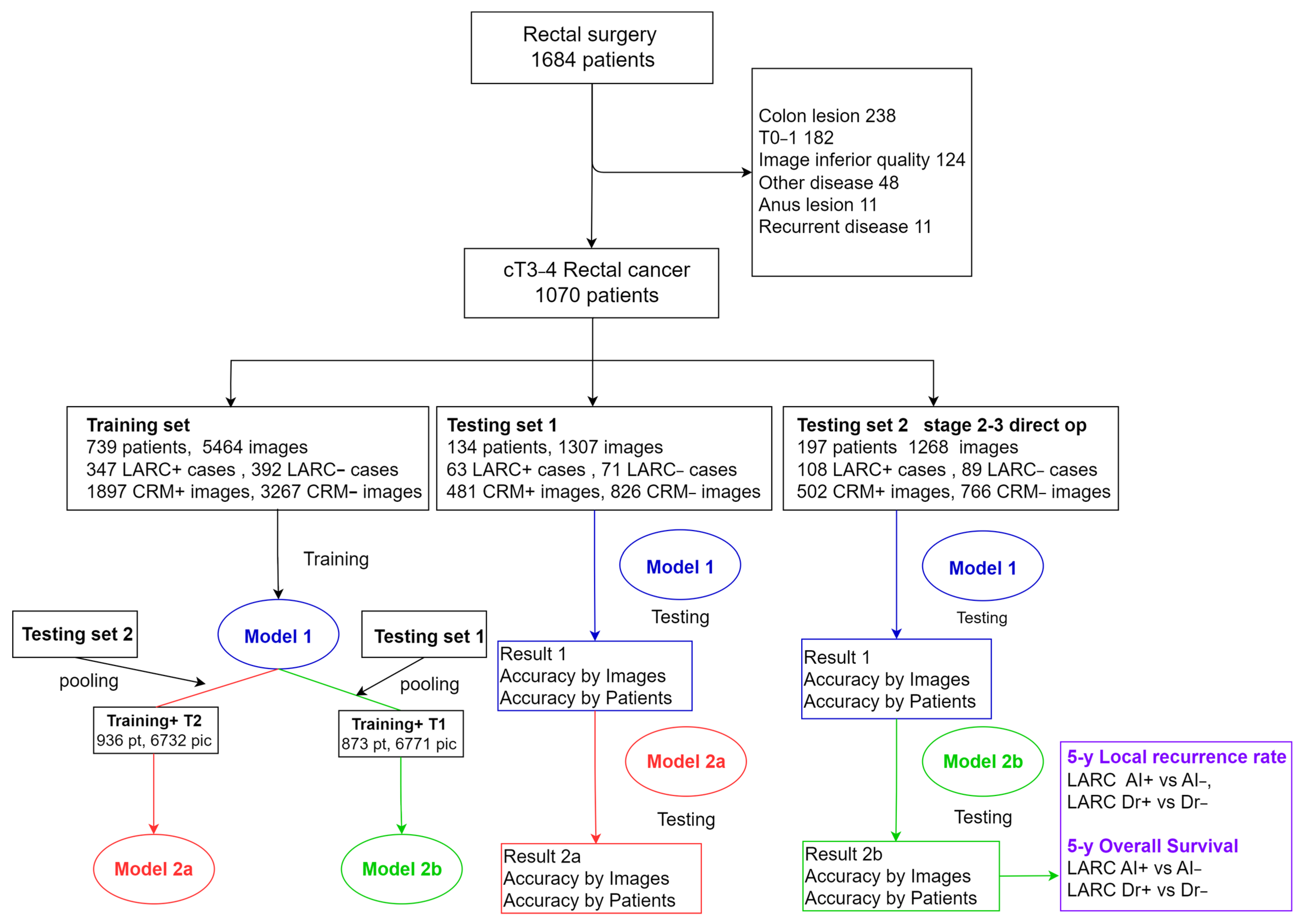
2.1. Dataset
2.2. CT Imaging Methods
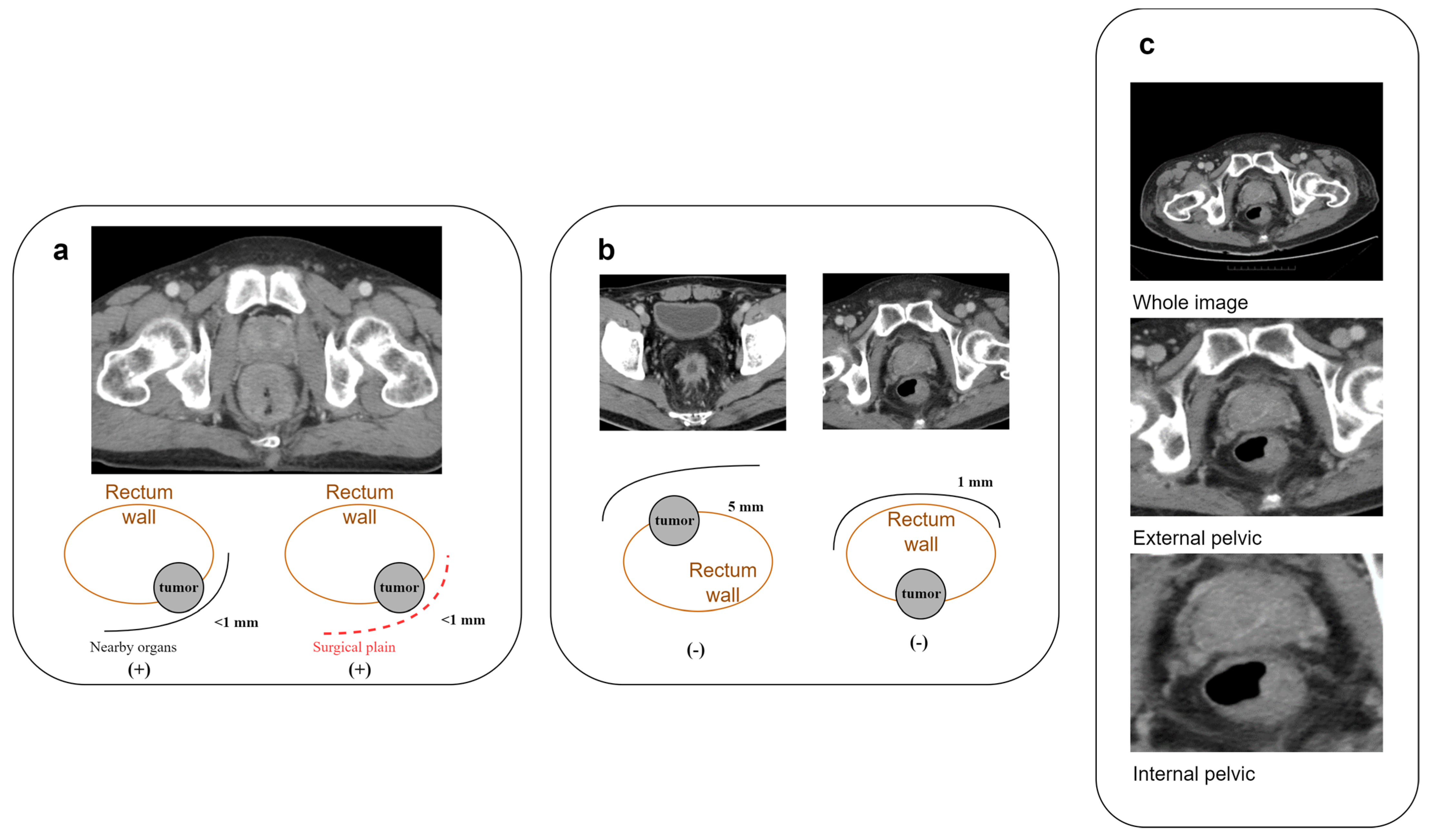
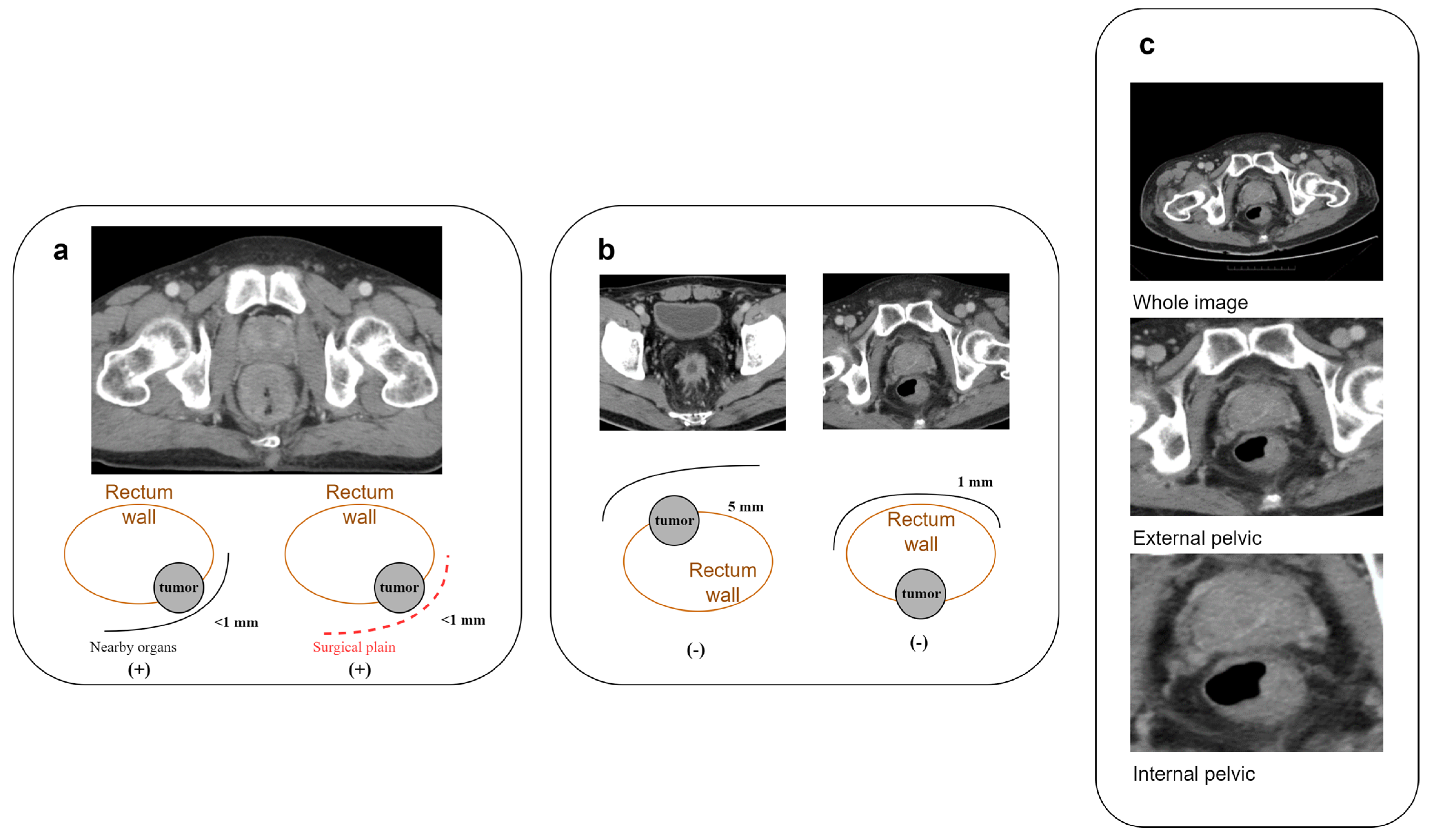
2.3. Annotation of CRM-Threatening LARC Cases
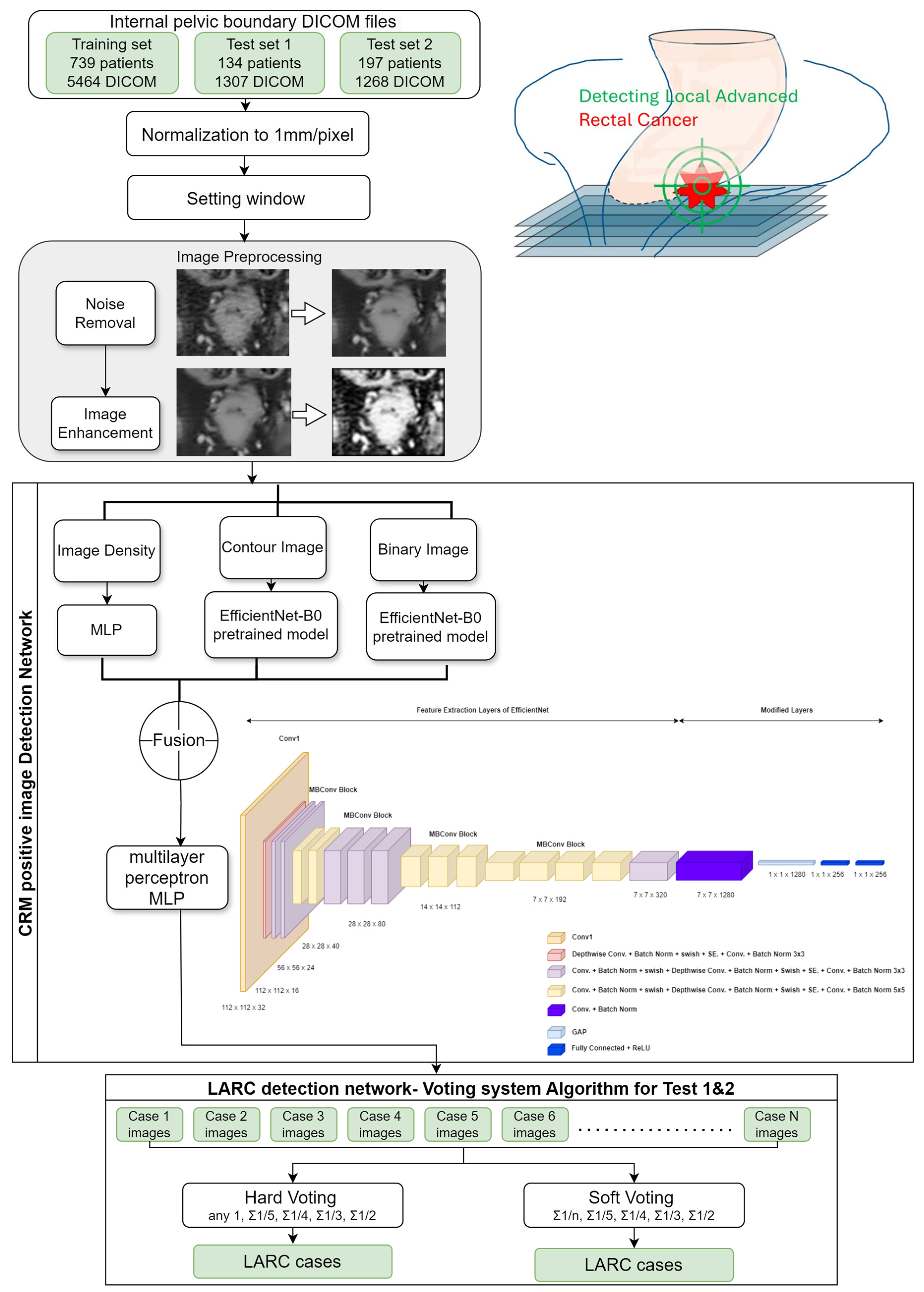
2.4. Image Processing
2.5. Deep Learning Algorithm for CRM-Positive Image Identification
2.6. Determining LARC Cases through Series of Images
2.7. Local Recurrence Rate Analysis
2.8. Statistical Analysis
3. Results
3.1. Training Set and Test Set Materials
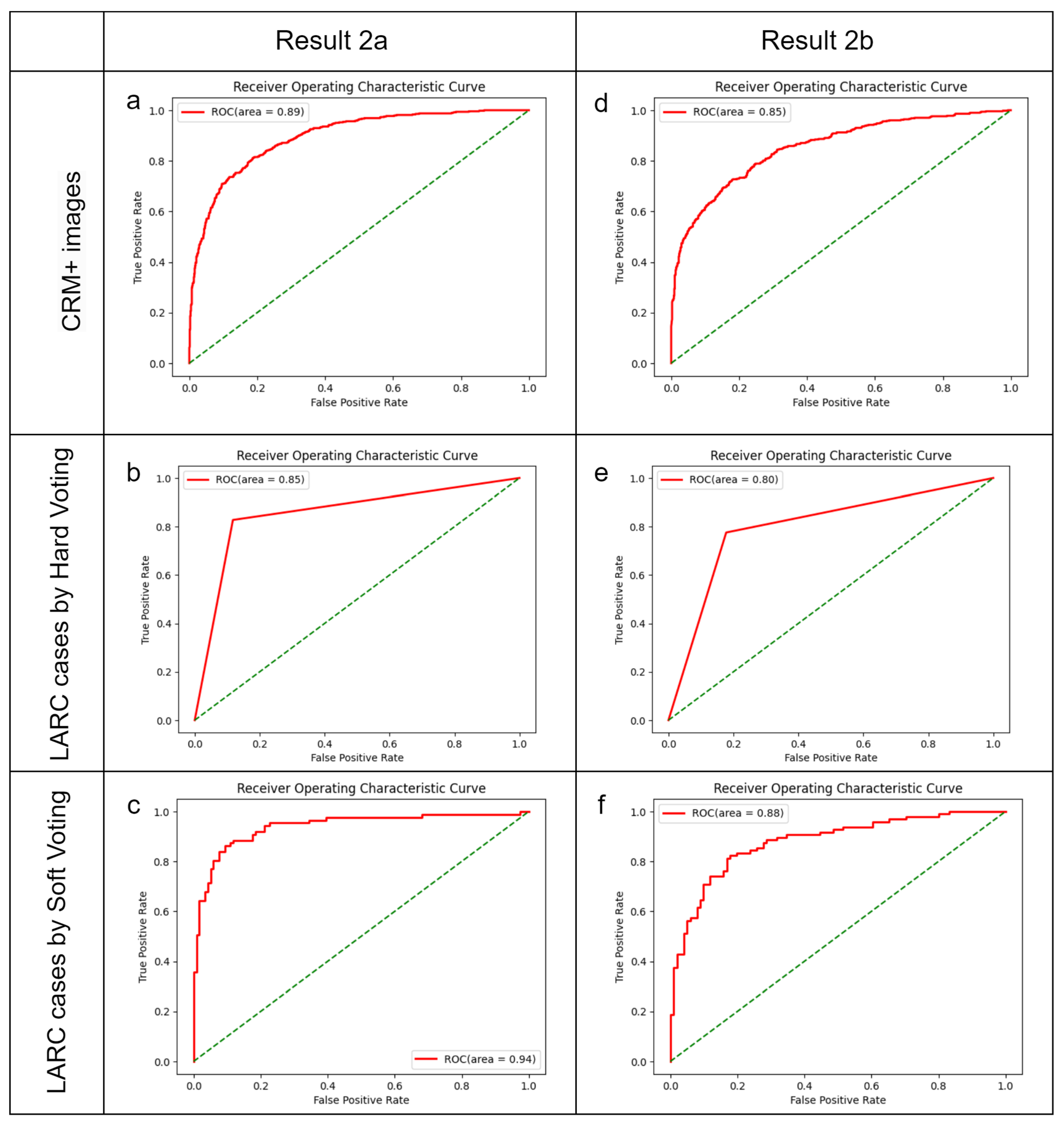
3.2. Model Performance by Image
3.3. Model Performance by Patient
3.4. Expanding the Training Set
3.5. Prediction Results and Survival Analysis in Test Set 2
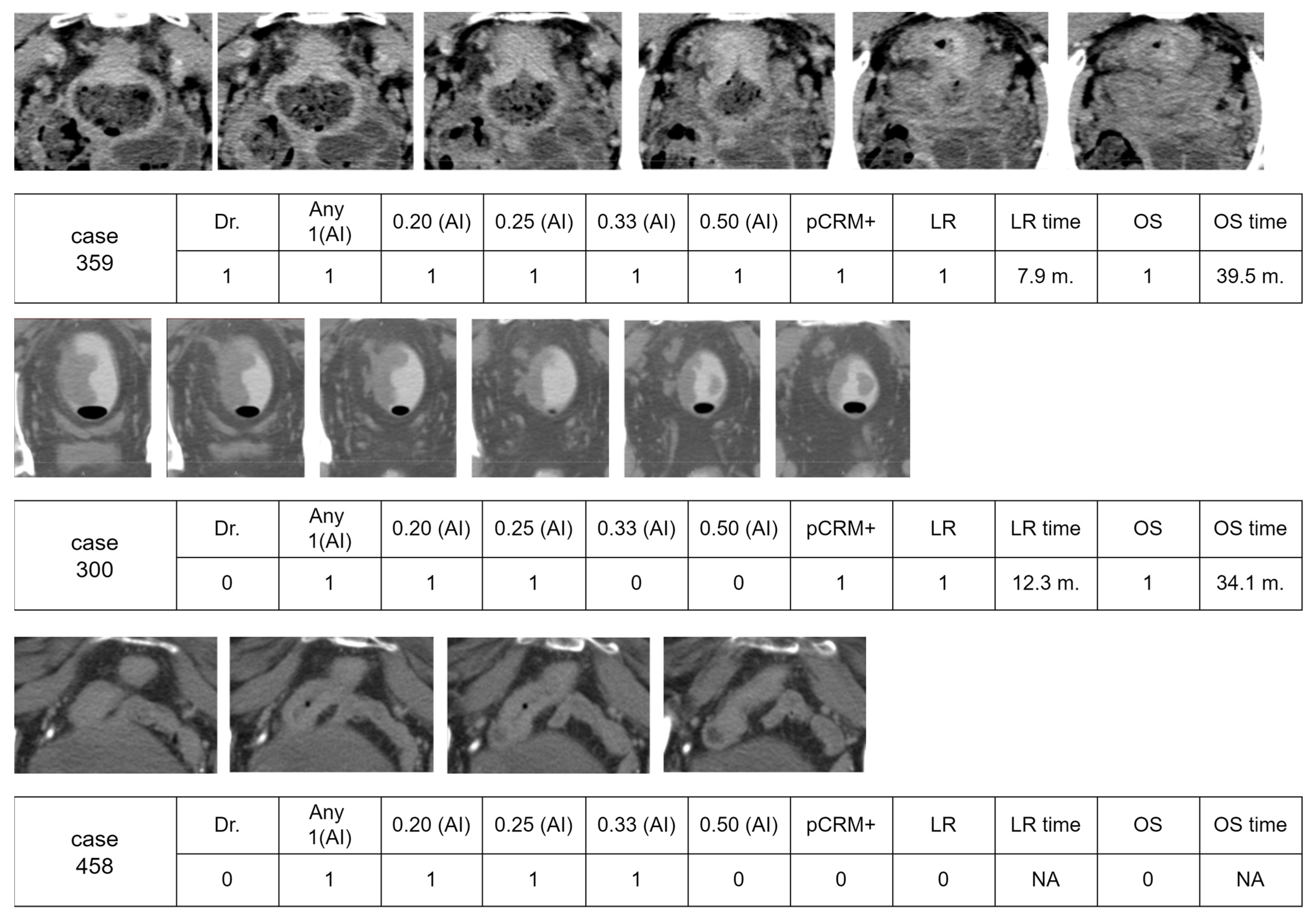
3.6. Visual Examples of Interpretation by AI and Doctor
4. Discussion
4.1. Integration of Key Results with Existing Research
4.2. Significant Achievements and Contributions
4.3. Combining Current Findings with Original Study Aspects
4.4. State-of-the-Art Method for CRM+ Images and LARC Cases
4.5. How to Utilize the AI Prediction Results
4.6. Limitations and Future Directions
4.7. Possible Applications of this Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Heald, R.J.; Ryall, R.D. Recurrence and survival after total mesorectal excision for rectal cancer. Lancet 1986, 1, 1479–1482. [Google Scholar] [CrossRef] [PubMed]
- Nagtegaal, I.D.; Quirke, P. What Is the Role for the Circumferential Margin in the Modern Treatment of Rectal Cancer? J. Clin. Oncol. 2008, 26, 303–312. [Google Scholar] [CrossRef] [PubMed]
- van Gijn, W.; Marijnen, C.A.; Nagtegaal, I.D.; Kranenbarg, E.M.; Putter, H.; Wiggers, T.; Rutten, H.J.; Påhlman, L.; Glimelius, B.; van de Velde, C.J. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer: 12-year follow-up of the multicentre, randomised controlled TME trial. Lancet Oncol. 2011, 12, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Taylor, F.G.; Quirke, P.; Heald, R.J.; Moran, B.J.; Blomqvist, L.; Swift, I.R.; Sebag-Montefiore, D.; Tekkis, P.; Brown, G. Preoperative magnetic resonance imaging assessment of circumferential resection margin predicts disease-free survival and local recurrence: 5-year follow-up results of the MERCURY study. J. Clin. Oncol. 2014, 32, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Bahadoer, R.R.; Dijkstra, E.A.; van Etten, B.; Marijnen, C.A.M.; Putter, H.; Kranenbarg, E.M.; Roodvoets, A.G.H.; Nagtegaal, I.D.; Beets-Tan, R.G.H.; Blomqvist, L.K.; et al. Short-course radiotherapy followed by chemotherapy before total mesorectal excision (TME) versus preoperative chemoradiotherapy, TME, and optional adjuvant chemotherapy in locally advanced rectal cancer (RAPIDO): A randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Conroy, T.; Bosset, J.-F.; Etienne, P.-L.; Rio, E.; François, É.; Mesgouez-Nebout, N.; Vendrely, V.; Artignan, X.; Bouché, O.; Gargot, D.; et al. Neoadjuvant chemotherapy with FOLFIRINOX and preoperative chemoradiotherapy for patients with locally advanced rectal cancer (UNICANCER-PRODIGE 23): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 702–715. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.I.; Hong, S.W.; Lim, S.B.; Yang, D.H.; Kim, E.B.; Kim, M.H.; Kim, C.W.; Lee, J.L.; Yoon, Y.S.; Park, I.J.; et al. Risk factors for the failure of endoscopic balloon dilation to manage anastomotic stricture from colorectal surgery: Retrospective cohort study. Surg. Endosc. 2024, 38, 1775–1783. [Google Scholar] [CrossRef]
- Schrag, D.; Shi, Q.; Weiser, M.R.; Gollub, M.J.; Saltz, L.B.; Musher, B.L.; Goldberg, J.; Al Baghdadi, T.; Goodman, K.A.; McWilliams, R.R.; et al. Preoperative Treatment of Locally Advanced Rectal Cancer. N. Engl. J. Med. 2023, 389, 322–334. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.B.; Kim, H.S.; Ham, A.; Chang, J.S.; Shin, S.J.; Beom, S.H.; Koom, W.S.; Kim, T.; Han, Y.D.; Han, D.H.; et al. Role of Preoperative Chemoradiotherapy in Clinical Stage II/III Rectal Cancer Patients Undergoing Total Mesorectal Excision: A Retrospective Propensity Score Analysis. Front. Oncol. 2020, 10, 609313. [Google Scholar] [CrossRef] [PubMed]
- Maizlin, Z.V.; Brown, J.A.; So, G.; Brown, C.; Phang, T.P.; Walker, M.L.; Kirby, J.M.; Vora, P.; Tiwari, P. Can CT replace MRI in preoperative assessment of the circumferential resection margin in rectal cancer? Dis. Colon. Rectum 2010, 53, 308–314. [Google Scholar] [CrossRef]
- Heo, S.H.; Kim, J.W.; Shin, S.S.; Jeong, Y.Y.; Kang, H.K. Multimodal imaging evaluation in staging of rectal cancer. World J. Gastroenterol. 2014, 20, 4244–4255. [Google Scholar] [CrossRef] [PubMed]
- Liew, W.S.; Tang, T.B.; Lin, C.H.; Lu, C.K. Automatic colonic polyp detection using integration of modified deep residual convolutional neural network and ensemble learning approaches. Comput. Methods Programs Biomed. 2021, 206, 106114. [Google Scholar] [CrossRef] [PubMed]
- Muniz, F.B.; Baffa, M.F.O.; Garcia, S.B.; Bachmann, L.; Felipe, J.C. Histopathological diagnosis of colon cancer using micro-FTIR hyperspectral imaging and deep learning. Comput. Methods Programs Biomed. 2023, 231, 107388. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Lan, L.; You, L.; Chen, K.; Peng, L.; Zhao, W.; Song, B.; Wang, Y.; Ji, Z.; Zhou, X. Automated CT Pancreas Segmentation for Acute Pancreatitis Patients by combining a Novel Object Detection Approach and U-Net. Biomed. Signal Process. Control 2023, 81, 104430. [Google Scholar] [CrossRef] [PubMed]
- Wong, P.K.; Yan, T.; Wang, H.; Chan, I.N.; Wang, J.; Li, Y.; Ren, H.; Wong, C.H. Automatic detection of multiple types of pneumonia: Open dataset and a multi-scale attention network. Biomed. Signal Process. Control 2022, 73, 103415. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Guo, S.; Han, L.; Cekderi, A.B. Two-dimensional reciprocal cross entropy multi-threshold combined with improved firefly algorithm for lung parenchyma segmentation of COVID-19 CT image. Biomed. Signal Process. Control 2022, 78, 103933. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.D.; Zhang, Z.; Zhang, X.; Wang, S.H. MIDCAN: A multiple input deep convolutional attention network for COVID-19 diagnosis based on chest CT and chest X-ray. Pattern Recognit. Lett. 2021, 150, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, C.; Kumar, I.; Vijayakumar, V.; Singh, K.U.; Kumar, A. The state of the art of deep learning models in medical science and their challenges. Multimed. Syst. 2021, 27, 599–613. [Google Scholar] [CrossRef]
- Skiadopoulos, S.; Karatrantou, A.; Korfiatis, P.; Costaridou, L.; Vassilakos, P.; Apostolopoulos, D.; Panayiotakis, G. Evaluating image denoising methods in myocardial perfusion single photon emission computed tomography (SPECT) imaging. Meas. Sci. Technol. 2009, 20, 104023. [Google Scholar] [CrossRef]
- Hanzouli, H.; Lapuyade-Lahorgue, J.; Monfrini, E.; Delso, G.; Pieczynski, W.; Visvikis, D.; Hatt, M. PECT/CT image denoising and segmentation based on a multi observation and multi scale Markov tree model. In Proceedings of the IEEE Nuclear Science Symposium Conference Record 2013, Seoul, Republic of Korea, 27 October–2 November 2013. [Google Scholar] [CrossRef]
- Shao, W.j.; Ni, J.; Zhu, C. A Hybrid Method of Image Restoration and Denoise of CT Images. In Proceedings of the 2012 Sixth International Conference on Internet Computing for Science and Engineering, Washington, DC, USA, 21–23 April 2012; pp. 117–121. [Google Scholar]
- Guo, S.; Wang, G.; Han, L.; Song, X.; Yang, W. COVID-19 CT image denoising algorithm based on adaptive threshold and optimized weighted median filter. Biomed. Signal Process. Control 2022, 75, 103552. [Google Scholar] [CrossRef] [PubMed]
- Abdullah-Al-Wadud, M.; Kabir, M.H.; Dewan, M.A.A.; Chae, O. A Dynamic Histogram Equalization for Image Contrast Enhancement. IEEE Trans. Consum. Electron. 2007, 53, 593–600. [Google Scholar] [CrossRef]
- Lee, Y.; Hwang, H.; Shin, J.; Oh, B.T. Pedestrian detection using multi-scale squeeze-and-excitation module. Mach. Vis. Appl. 2020, 31, 55. [Google Scholar] [CrossRef]
- Tan, M.; Le, Q.V. EfficientNet: Rethinking Model Scaling for Convolutional Neural Networks. arXiv 2019, arXiv:1905.11946. [Google Scholar]
- James, A.P.; Dasarathy, B.V. Medical image fusion: A survey of the state of the art. Inf. Fusion 2014, 19, 4–19. [Google Scholar] [CrossRef]
- Rana, M.; Bhushan, M. Machine learning and deep learning approach for medical image analysis: Diagnosis to detection. Multimed. Tools Appl. 2022, 82, 26731–26769. [Google Scholar] [CrossRef] [PubMed]
- Susič, D.; Syed-Abdul, S.; Dovgan, E.; Jonnagaddala, J.; Gradišek, A. Artificial intelligence based personalized predictive survival among colorectal cancer patients. Comput. Methods Programs Biomed. 2023, 231, 107435. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.H.; Chen, W.C.; Chen, J.B.; Huang, H.C.; Chuang, L.Y. Overall mortality risk analysis for rectal cancer using deep learning-based fuzzy systems. Comput. Biol. Med. 2023, 157, 106706. [Google Scholar] [CrossRef] [PubMed]
- Morís, D.I.; de Moura, J.; Marcos, P.J.; Rey, E.M.; Novo, J.; Ortega, M. Comprehensive analysis of clinical data for COVID-19 outcome estimation with machine learning models. Biomed. Signal Process. Control 2023, 84, 104818. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Raldow, A.C.; Weidhaas, J.B.; Zhou, Q.; Qi, X.S. Prediction of Radiation Treatment Response for Locally Advanced Rectal Cancer via a Longitudinal Trend Analysis Framework on Cone-Beam CT. Cancers 2023, 15, 5142. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Zhang, Y.; Hu, J.; Zhou, W.; Hu, X.; Cui, T.; Yue, N.J.; Sun, X.; Nie, K. Radiomics for the Prediction of Pathological Complete Response to Neoadjuvant Chemoradiation in Locally Advanced Rectal Cancer: A Prospective Observational Trial. Bioengineering 2023, 10, 634. [Google Scholar] [CrossRef] [PubMed]
- Hamabe, A.; Ishii, M.; Kamoda, R.; Sasuga, S.; Okuya, K.; Okita, K.; Akizuki, E.; Sato, Y.; Miura, R.; Onodera, K.; et al. Artificial intelligence-based technology for semi-automated segmentation of rectal cancer using high-resolution MRI. PLoS ONE 2022, 17, e0269931. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, P.K.; Gupta, P.; Lai, Y.-C.; Chiang, S.-F.; You, J.-F.; Onthoni, D.D.; Chern, Y.-J. Localization of Colorectal Cancer Lesions in Contrast-Computed Tomography Images via a Deep Learning Approach. Bioengineering 2023, 10, 972. [Google Scholar] [CrossRef] [PubMed]
- Manjunath, K.N.; Siddalingaswamy, P.C.; Prabhu, G.K. Domain-Based Analysis of Colon Polyp in CT Colonography Using Image-Processing Techniques. Asian Pac. J. Cancer Prev. 2019, 20, 629–637. [Google Scholar] [CrossRef]
- Ferreira, A.; Li, J.; Pomykala, K.L.; Kleesiek, J.; Alves, V.; Egger, J. GAN-based generation of realistic 3D volumetric data: A systematic review and taxonomy. Med. Image Anal. 2024, 93, 103100. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Training (n = 739) | Testing 1 (n = 134) | Testing 2 (n = 197) | p Value | |||||
|---|---|---|---|---|---|---|---|---|
| Gender | Female | 283 | (38.3%) | 53 | (39.6%) | 73 | (37.1%) | 0.898 |
| Male | 456 | (61.7%) | 81 | (60.4%) | 124 | (62.9%) | ||
| Age | 66.40 | ±14.02 | 68.88 | ±12.18 | 69.86 | ±13.92 | 0.003 ** | |
| Site of lesions | Upper | 169 | (22.9%) | 45 | (33.6%) | 70 | (35.5%) | <0.001 ** |
| Middle | 257 | (34.8%) | 49 | (36.6%) | 81 | (41.1%) | ||
| Lower | 313 | (42.4%) | 40 | (29.9%) | 46 | (23.4%) | ||
| Clinical T stage | T3 | 554 | (79.0%) | 98 | (74.8%) | 170 | (86.3%) | 0.024 * |
| T4 | 147 | (21.0%) | 33 | (25.2%) | 27 | (13.7%) | ||
| Clinical N stage | N0 | 197 | (26.7%) | 33 | (24.6%) | 108 | (54.8%) | <0.001 ** |
| N1–2 | 542 | (73.3%) | 101 | (75.4%) | 89 | (45.2%) | ||
| Clinical Stage | 2 | 179 | (24.2%) | 31 | (23.1%) | 108 | (54.8%) | <0.001 ** |
| 3 | 454 | (61.4%) | 65 | (48.5%) | 89 | (45.2%) | ||
| 4 | 106 | (14.3%) | 38 | (28.4%) | 0 | (0.0%) | ||
| c CRM | negative | 392 | (53.0%) | 71 | (53.0%) | 89 | (45.2%) | 0.936 |
| positive | 347 | (47.0%) | 63 | (47.0%) | 108 | (54.8%) | ||
| c CRM+ image | negative | 3267 | (63.3%) | 826 | (63.2%) | 766 | (60.4%) | |
| positive | 1897 | (36.7%) | 481 | (36.8%) | 502 | (39.6%) | ||
| Radiation therapy | 279 | (37.8%) | 36 | (26.9%) | 0 | (0.0%) | <0.001 ** | |
| Operation | 683 | (92.4%) | 134 | (100.0%) | 197 | (100.0%) | <0.001 ** | |
| Pathology T | T0–1 | 11 | (1.6%) | 0 | (0.0%) | 5 | (2.5%) | <0.001 ** |
| T2 | 30 | (4.4%) | 5 | (3.7%) | 46 | (23.4%) | ||
| T3 | 512 | (75.0%) | 96 | (71.6%) | 122 | (61.9%) | ||
| T4 | 130 | (19.0%) | 33 | (24.6%) | 24 | (12.2%) | ||
| Pathology N | N0 | 175 | (25.6%) | 33 | (24.6%) | 85 | (43.4%) | <0.001 ** |
| N1–2 | 508 | (74.4%) | 101 | (75.4%) | 111 | (56.6%) | ||
| Pathology Stage | 1 | 0 | (0.0%) | 0 | (0.0%) | 32 | (16.2%) | <0.001 ** |
| 2 | 161 | (23.6%) | 30 | (22.4%) | 53 | (26.9%) | ||
| 3 | 423 | (61.9%) | 66 | (49.3%) | 112 | (56.9%) | ||
| 4 | 99 | (14.5%) | 38 | (28.4%) | 0 | (0.0%) | ||
| p CRM | negative | 574 | (84.0%) | 98 | (73.1%) | 172 | (87.8%) | 0.001 ** |
| positive | 109 | (16.0%) | 36 | (26.9%) | 24 | (12.2%) | ||
| Sensitivity | Specificity | Accuracy | AUC | |
|---|---|---|---|---|
| whole picture | 0.44 | 0.702 | 0.621 | 0.59 |
| external pelvis | 0.48 | 0.784 | 0.67 | 0.7 |
| internal pelvis | 0.527 | 0.816 | 0.713 | 0.77 |
| image processed | 0.811 | 0.809 | 0.81 | 0.89 |
| Image-Based | Sensitivity | Specificity | Accuracy | Balanced Accuracy | AUC |
|---|---|---|---|---|---|
| Training and validation (739 series, 5164 images) | 0.80 | 0.82 | 0.82 | 0.81 | 0.9 |
| Testing 1 (134 series, 1307 images) | 0.81 | 0.81 | 0.81 | 0.81 | 0.89 |
| Testing 2 (197 series, 1268 images) | 0.75 | 0.81 | 0.79 | 0.78 | 0.86 |
| Testing 1 Set | Threshold | Sensitivity | Specificity | Accuracy | Balanced Accuracy | AUC |
|---|---|---|---|---|---|---|
| any 1 | 0.96 | 0.65 | 0.80 | 0.81 | 0.81 | |
| >Σ1/5 | 0.90 | 0.78 | 0.84 | 0.84 | 0.84 | |
| hard voting | >Σ1/4 | 0.85 | 0.83 | 0.84 | 0.84 | 0.84 |
| >Σ1/3 | 0.76 | 0.89 | 0.83 | 0.82 | 0.82 | |
| >Σ1/2 | 0.65 | 0.91 | 0.79 | 0.78 | 0.78 | |
| any 1 (>Σ1/n) | 0.88 | 0.74 | 0.81 | 0.81 | 0.89 | |
| >Σ1/5 | 0.91 | 0.78 | 0.84 | 0.85 | 0.91 | |
| soft voting | >Σ1/4 | 0.85 | 0.82 | 0.84 | 0.84 | 0.91 |
| >Σ1/3 | 0.87 | 0.89 | 0.88 | 0.88 | 0.93 | |
| >Σ1/2 | 0.76 | 0.91 | 0.86 | 0.83 | 0.93 | |
| Testing 2 Set | ||||||
| Any 1 | 0.90 | 0.61 | 0.77 | 0.75 | 0.75 | |
| >Σ1/5 | 0.85 | 0.72 | 0.79 | 0.79 | 0.79 | |
| hard voting | >Σ1/4 | 0.82 | 0.76 | 0.80 | 0.79 | 0.79 |
| >Σ1/3 | 0.73 | 0.85 | 0.79 | 0.79 | 0.79 | |
| >Σ1/2 | 0.57 | 0.91 | 0.73 | 0.74 | 0.74 | |
| any 1 (>Σ1/n) | 0.84 | 0.70 | 0.78 | 0.77 | 0.86 | |
| >Σ1/5 | 0.85 | 0.74 | 0.80 | 0.80 | 0.88 | |
| soft voting | >Σ1/4 | 0.81 | 0.77 | 0.79 | 0.79 | 0.87 |
| >Σ1/3 | 0.78 | 0.87 | 0.83 | 0.83 | 0.88 | |
| >Σ1/2 | 0.67 | 0.90 | 0.81 | 0.78 | 0.87 |
| Result 2a of Testing Set 1 | Sensitivity | Specificity | Accuracy | Balanced Accuracy | AUC | |
|---|---|---|---|---|---|---|
| Image-based | 0.76 | 0.87 | 0.82 | 0.83 | 0.89 | |
| any 1 | 0.94 | 0.66 | 0.81 | 0.80 | 0.80 | |
| >Σ1/5 | 0.90 | 0.79 | 0.84 | 0.84 | 0.84 | |
| hard voting | >Σ1/4 | 0.87 | 0.83 | 0.85 | 0.85 | 0.85 |
| >Σ1/3 | 0.83 | 0.88 | 0.86 | 0.85 | 0.86 | |
| >Σ1/2 | 0.70 | 0.92 | 0.84 | 0.81 | 0.81 | |
| any 1 (>Σ1/n) | 0.84 | 0.85 | 0.84 | 0.84 | 0.91 | |
| >Σ1/5 | 0.90 | 0.82 | 0.86 | 0.86 | 0.93 | |
| soft voting | >Σ1/4 | 0.81 | 0.92 | 0.87 | 0.86 | 0.93 |
| >Σ1/3 | 0.86 | 0.91 | 0.89 | 0.88 | 0.94 | |
| >Σ1/2 | 0.92 | 0.86 | 0.88 | 0.89 | 0.94 | |
| Result 2b of Testing Set 2 | Sensitivity | Specificity | Accuracy | Balanced Accuracy | AUC | |
| Image-based | 0.68 | 0.86 | 0.78 | 0.77 | 0.85 | |
| any 1 | 0.88 | 0.69 | 0.80 | 0.78 | 0.78 | |
| >Σ1/5 | 0.82 | 0.76 | 0.80 | 0.79 | 0.79 | |
| hard voting | >Σ1/4 | 0.78 | 0.82 | 0.80 | 0.80 | 0.80 |
| >Σ1/3 | 0.55 | 0.93 | 0.75 | 0.74 | 0.74 | |
| >Σ1/2 | 0.64 | 0.90 | 0.80 | 0.77 | 0.77 | |
| any 1 (>Σ1/n) | 0.78 | 0.86 | 0.81 | 0.82 | 0.87 | |
| >Σ1/5 | 0.81 | 0.85 | 0.83 | 0.83 | 0.88 | |
| soft voting | >Σ1/4 | 0.80 | 0.84 | 0.82 | 0.82 | 0.87 |
| >Σ1/3 | 0.82 | 0.82 | 0.82 | 0.82 | 0.88 | |
| >Σ1/2 | 0.85 | 0.73 | 0.78 | 0.79 | 0.86 | |
| Model | Total | Local Recurrence (n) | Censored | LR Rate (%) | p | Overall Survival (Mortality) | Censored | Overall Survival (Mortality) Rate | p | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (n) | % | 1y | 3y | 5y | (n) | % | 1y | 3y | 5y | |||||||
| Dr | − | 89 | 8 | 81 | 91.0 | 97.5 | 89.2 | 89.2 | 0.106 | 24 | 65 | 73.0 | 96.2 | 82.2 | 71.7 | 0.172 |
| + | 108 | 18 | 90 | 83.3 | 94.0 | 84.8 | 79.8 | 41 | 67 | 62.0 | 94.1 | 76.2 | 60.7 | |||
| AI any 1 (>Σ1/n) | − | 82 | 7 | 75 | 91.5 | 97.4 | 91.2 | 89.2 | 0.113 | 23 | 59 | 72.0 | 95.8 | 82.6 | 71.1 | 0.336 |
| + | 115 | 19 | 96 | 83.5 | 94.3 | 83.6 | 80.5 | 42 | 73 | 63.5 | 94.5 | 76.2 | 61.8 | |||
| AI (>Σ1/5) | − | 89 | 7 | 82 | 92.1 | 97.6 | 91.8 | 90.0 | 0.052 | 26 | 63 | 70.8 | 96.1 | 82.4 | 70.3 | 0.431 |
| + | 108 | 19 | 89 | 82.4 | 94.0 | 82.7 | 79.5 | 39 | 69 | 63.9 | 94.2 | 75.9 | 61.9 | |||
| AI (>Σ1/4) | − | 99 | 8 | 91 | 91.9 | 97.8 | 91.4 | 89.6 | 0.044 | 29 | 70 | 70.7 | 96.5 | 82.8 | 69.1 | 0.483 |
| + | 98 | 18 | 80 | 81.6 | 93.4 | 82.2 | 78.8 | 36 | 62 | 63.3 | 93.7 | 74.9 | 62.2 | |||
| AI (>Σ1/3) | − | 118 | 10 | 108 | 91.5 | 98.1 | 90.6 | 89.1 | 0.030 | 32 | 86 | 72.9 | 96.2 | 82.5 | 70.6 | 0.198 |
| + | 79 | 16 | 63 | 79.7 | 91.9 | 81.3 | 77.1 | 33 | 46 | 58.2 | 93.5 | 73.8 | 58.9 | |||
| AI (>Σ1/2) | − | 146 | 13 | 133 | 91.1 | 97.7 | 90.8 | 88.6 | 0.003 | 39 | 107 | 73.3 | 96.2 | 83.6 | 72.0 | 0.005 |
| + | 51 | 13 | 38 | 74.5 | 89.8 | 75.6 | 71.9 | 26 | 25 | 49.0 | 92.0 | 66.5 | 49.3 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-Y.; Wu, J.C.-H.; Kuan, Y.-M.; Liu, Y.-C.; Chang, P.-Y.; Chen, J.-P.; Lu, H.H.-S.; Lee, O.K.-S. Precision Identification of Locally Advanced Rectal Cancer in Denoised CT Scans Using EfficientNet and Voting System Algorithms. Bioengineering 2024, 11, 399. https://doi.org/10.3390/bioengineering11040399
Lin C-Y, Wu JC-H, Kuan Y-M, Liu Y-C, Chang P-Y, Chen J-P, Lu HH-S, Lee OK-S. Precision Identification of Locally Advanced Rectal Cancer in Denoised CT Scans Using EfficientNet and Voting System Algorithms. Bioengineering. 2024; 11(4):399. https://doi.org/10.3390/bioengineering11040399
Chicago/Turabian StyleLin, Chun-Yu, Jacky Chung-Hao Wu, Yen-Ming Kuan, Yi-Chun Liu, Pi-Yi Chang, Jun-Peng Chen, Henry Horng-Shing Lu, and Oscar Kuang-Sheng Lee. 2024. "Precision Identification of Locally Advanced Rectal Cancer in Denoised CT Scans Using EfficientNet and Voting System Algorithms" Bioengineering 11, no. 4: 399. https://doi.org/10.3390/bioengineering11040399
APA StyleLin, C.-Y., Wu, J. C.-H., Kuan, Y.-M., Liu, Y.-C., Chang, P.-Y., Chen, J.-P., Lu, H. H.-S., & Lee, O. K.-S. (2024). Precision Identification of Locally Advanced Rectal Cancer in Denoised CT Scans Using EfficientNet and Voting System Algorithms. Bioengineering, 11(4), 399. https://doi.org/10.3390/bioengineering11040399