

Surgical Medical Education via 3D Bioprinting: Modular System for Endovascular Training

 ,
,  , ,
, ,  , and
, and 
Abstract
1. Introduction
1.1. Simulation and Training in Vascular Surgery
1.2. 3D Printing and Bioprinting in the Healthcare Context
2. Materials and Methods
2.1. Anatomical Accuracy
2.2. Design and Conceptualization
- Torquability: the response of the tip of the guidewire to the physician’s rotational movement, maintaining control and precision;
- Trackability: the capability to follow the desired path to reach the target site;
- Tactile feedback from the guidewire: increased resistance or friction during guidewire advancement attempts (the guidewire is encountering difficulty in navigating through the vessel or is not following the intended path).
2.3. Material Selection and 3D Printing Process
2.4. Evaluation and Testing
2.4.1. Participants
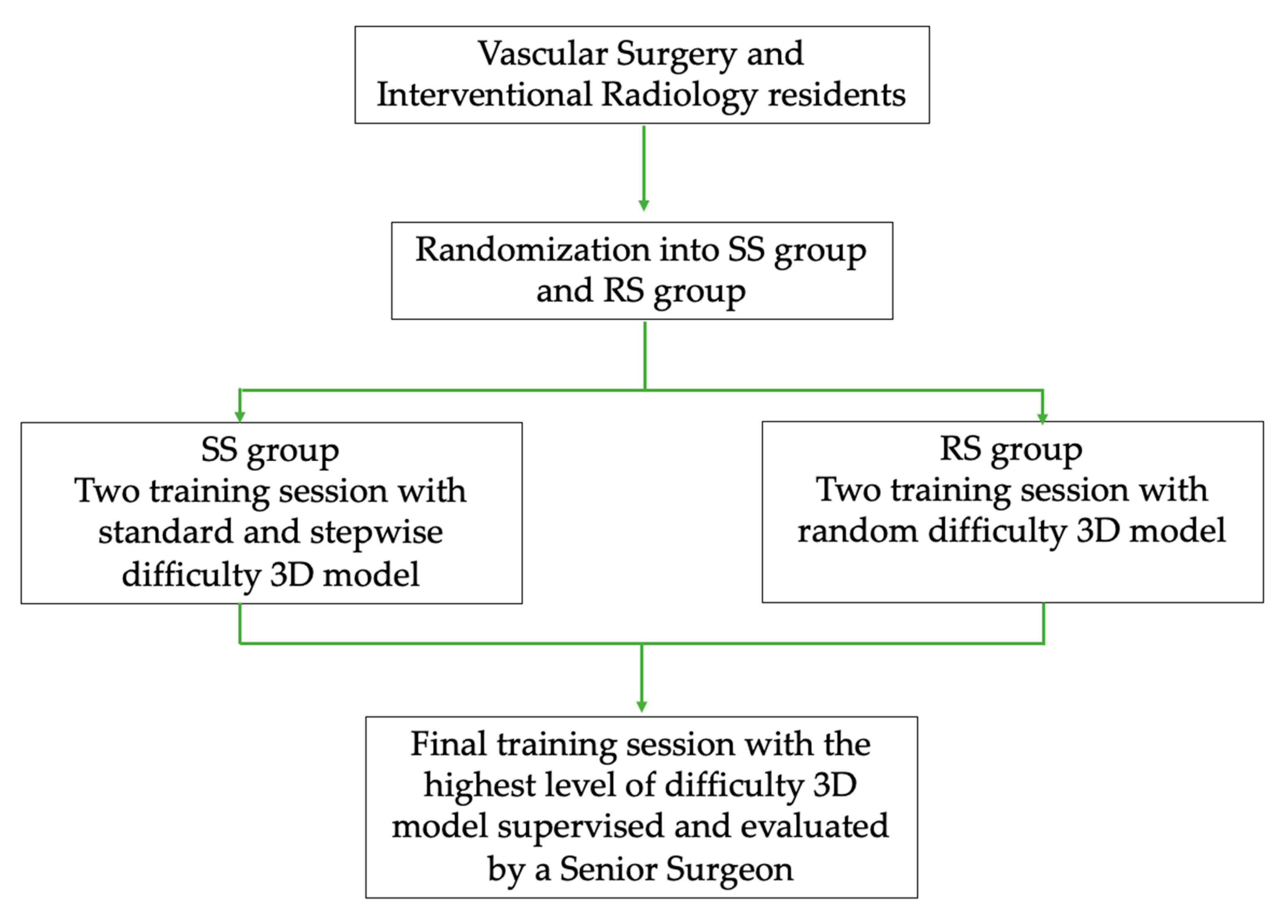
2.4.2. Study Design
2.4.3. Evaluation Instruments
2.5. Statistical Analysis
3. Results
3.1. Anatomical Accuracy
3.2. 3D Model
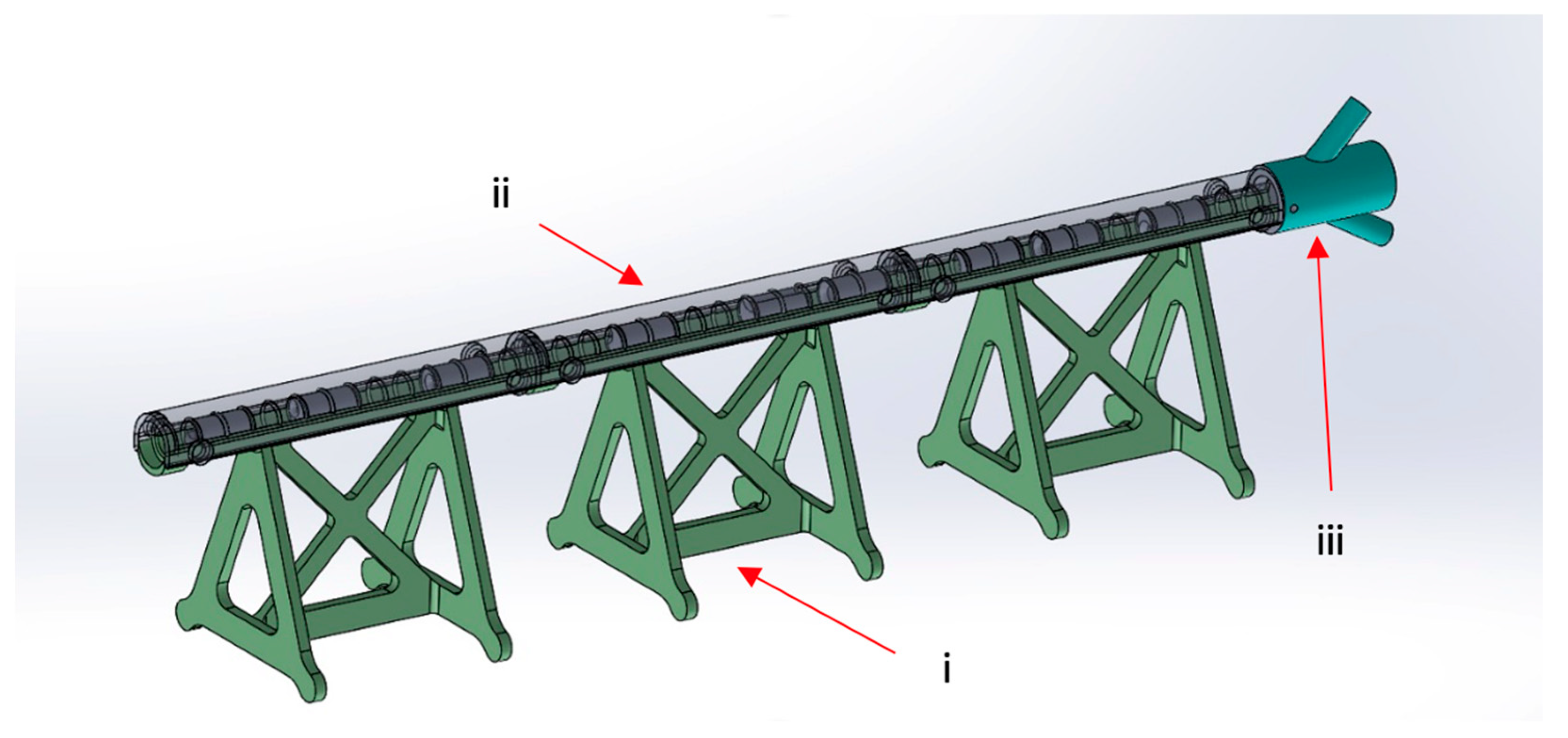
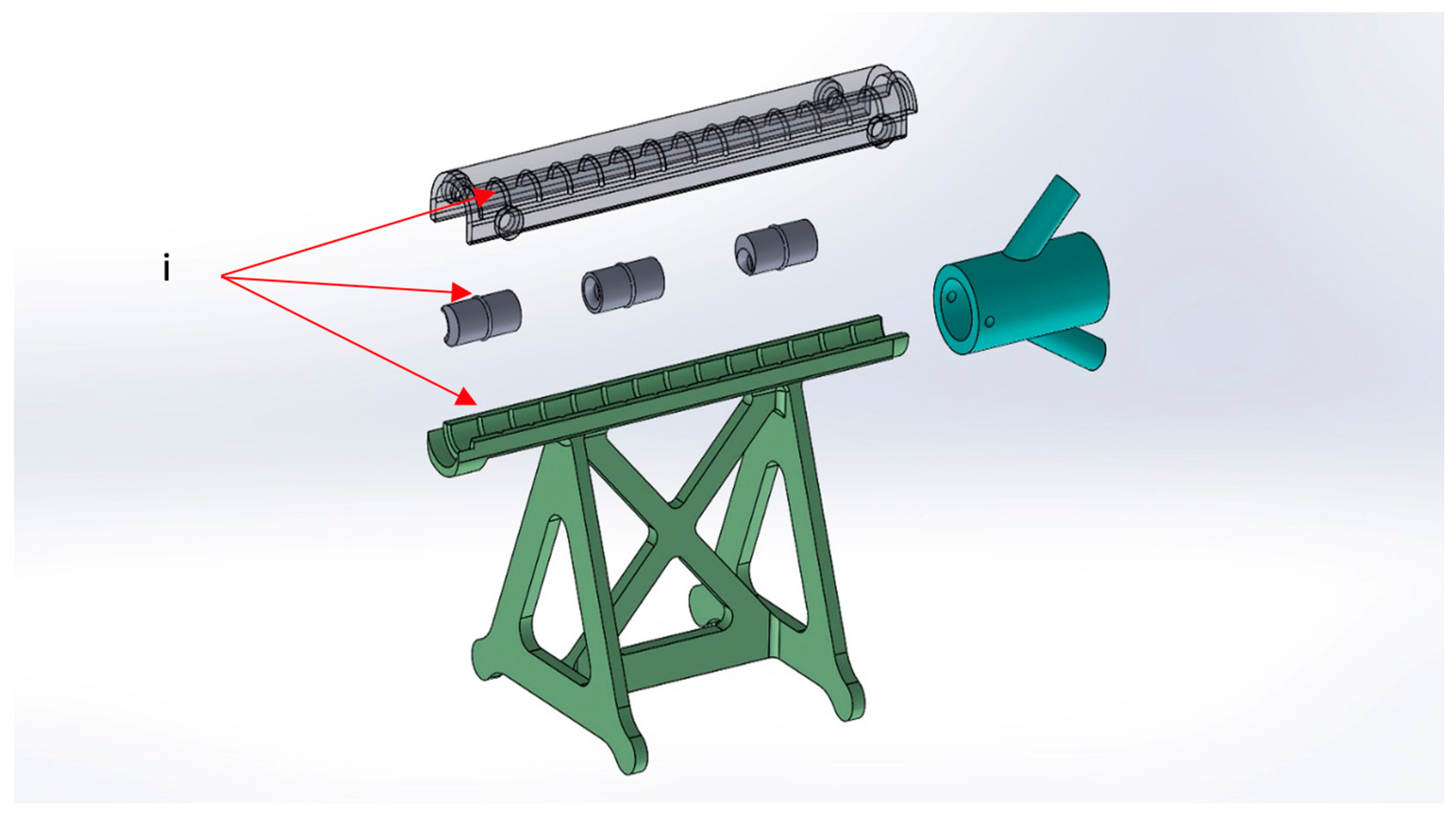
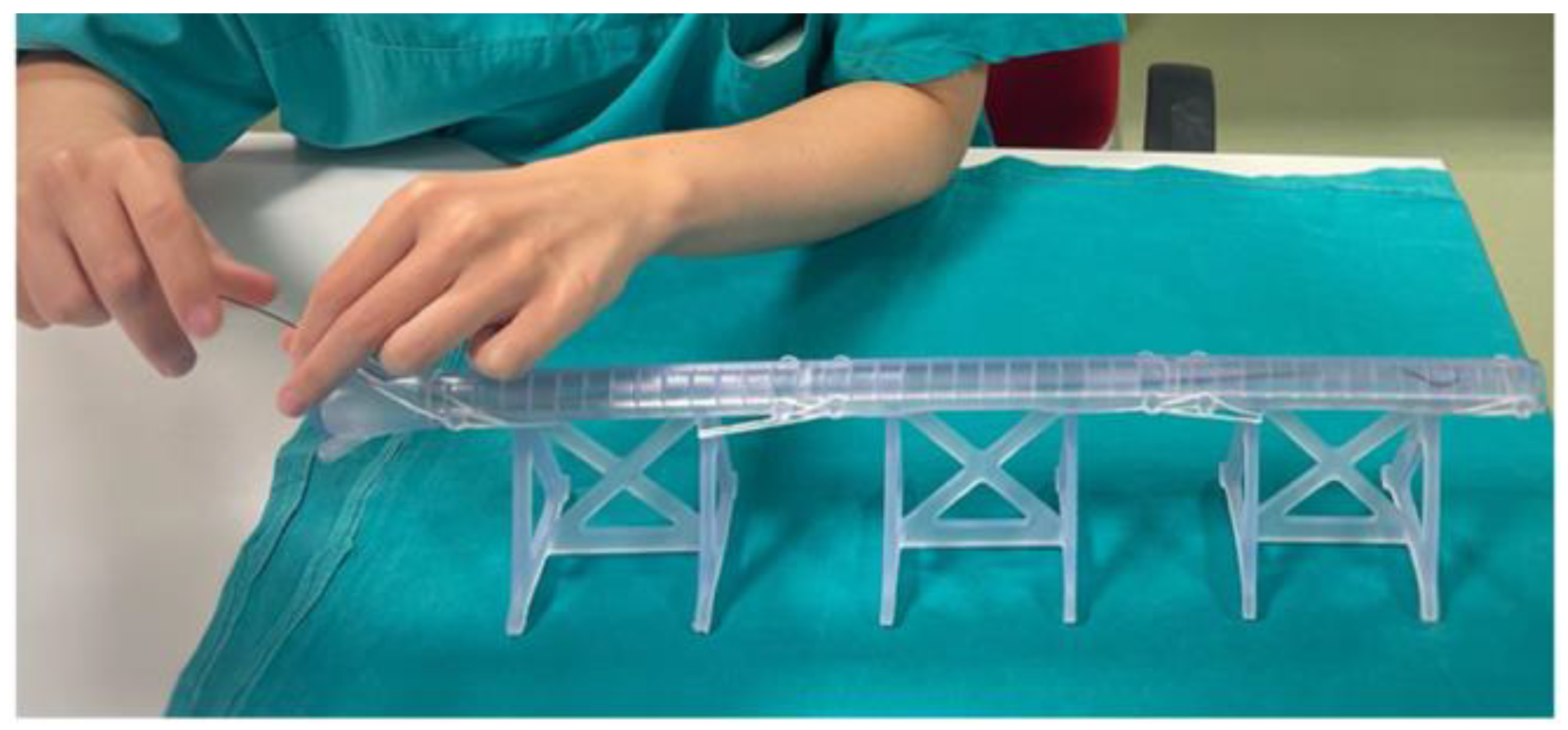
- The vessel: 1 cm diameter tube of 14 cm in length (for each module), consisting of a fixed part that is attached to pedestals and a transparent lid that can be detached to allow spacer insertion; any module can be connected to the others, increasing the total length. At the proximal end of the model, there is a cup for guidewire insertion to simulate the introducer sheath with two tunnels of different angulations (30 and 45 degrees);
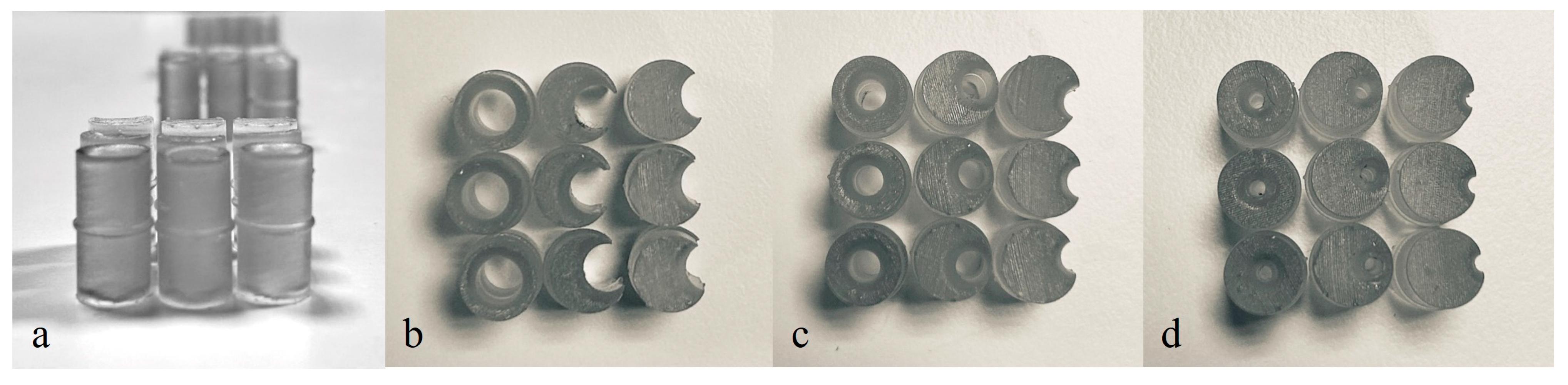
- The atheromatous plaques are cylinders with a length of 2 cm and an external diameter of 1 cm, called spacers. Each spacer is crossed by one of three different diameter channels (6, 4, and 2 mm) positioned with the circle barycenter uniformly distributed: aligned with the spacer barycenter, half radius as a distance from the center, and tangent to the perimeter. The combination of different diameters and positions of the channels allow mimicking different degrees and sites of stenosis. Due to their circular shape and coupling system, spacers can be easily turned and placed at different distances. The spacers were developed with 3 configurations (3 different positions of the channel) for the 3 different diameters of the channel (Figure 4). Spacers and channels can be customized (gate shape, tortuosity, and number of channels in the same spacer).
- Simple configuration: 9 spacers with 6 mm channels, 3 for each different channel configuration, with 1 cm distance between each spacer;
- Medium configuration: 9 spacers with 4 mm channels, 3 for each different channel configuration, with 1 cm distance between each spacer;
- Difficult configuration: 9 spacers with 2 mm channels, 3 for each different channel configuration, with 1 cm distance between each spacer;
- Random configuration: 3 spacers with 6 mm channels, 3 spacers with 4 mm channels, and 3 spacers with 2 mm channels, 1 for each different channel configuration, randomly placed inside the model, with 1 cm distance between each spacer.
3.3. Evaluation and Testing
4. Discussion
Limitations and Future Prospective
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nayahangan, L.J.; Konge, L.; Schroeder, T.V.; Paltved, C.; Lindorff-Larsen, K.G.; Nielsen, B.U.; Eiberg, J.P. A National Needs Assessment to Identify Technical Procedures in Vascular Surgery for Simulation Based Training. Eur. J. Vasc. Endovasc. Surg. 2017, 53, 591–599. [Google Scholar] [CrossRef]
- Maertens, H.; Vermassen, F.; Aggarwal, R.; Doyen, B.; Desender, L.; Van Herzeele, I.; Annemans, L. Endovascular Training Using a Simulation Based Curriculum Is Less Expensive than Training in the Hybrid Angiosuite. Eur. J. Vasc. Endovasc. Surg. 2018, 56, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Desender, L.; Rancic, Z.; Aggarwal, R.; Duchateau, J.; Glenck, M.; Lachat, M.; Vermassen, F.; Van Herzeele, I. Patient-Specific Rehearsal Prior to EVAR: A Pilot Study. Eur. J. Vasc. Endovasc. Surg. 2013, 45, 639–647. [Google Scholar] [CrossRef]
- Jabbour, N.; Snyderman, C.H. The Economics of Surgical Simulation. Otolaryngol. Clin. N. Am. 2017, 50, 1029–1036. [Google Scholar] [CrossRef]
- Gardner, A.K.; Nepomnayshy, D.; Reickert, C.; Gee, D.W.; Brydges, R.; Korndorffer, J.R.; Scott, D.J.; Sachdeva, A.K. The Value Proposition of Simulation. Surgery 2016, 160, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Itagaki, M.W. Using 3D Printed Models for Planning and Guidance during Endovascular Intervention: A Technical Advance. Diagn. Interv. Radiol. 2015, 21, 338–341. [Google Scholar] [CrossRef]
- Marro, A.; Bandukwala, T.; Mak, W. Three-Dimensional Printing and Medical Imaging: A Review of the Methods and Applications. Curr. Probl. Diagn. Radiol. 2016, 45, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, E.L.; Arora, S.; Moneta, G.L. Ensuring Vascular Surgical Training Is on the Right Track. J. Vasc. Surg. 2011, 53, 517–525. [Google Scholar] [CrossRef]
- Bismuth, J.; Donovan, M.A.; O’Malley, M.K.; El Sayed, H.F.; Naoum, J.J.; Peden, E.K.; Davies, M.G.; Lumsden, A.B. Incorporating Simulation in Vascular Surgery Education. J. Vasc. Surg. 2010, 52, 1072–1080. [Google Scholar] [CrossRef] [PubMed]
- Sternbergh, W.C.; York, J.W.; Conners, M.S.; Money, S.R. Trends in Aortic Aneurysm Surgical Training for General and Vascular Surgery Residents in the Era of Endovascular Abdominal Aortic Aneurysm Repair. J. Vasc. Surg. 2002, 36, 685–689. [Google Scholar] [CrossRef]
- Roberts, K.E.; Bell, R.L.; Duffy, A.J. Evolution of Surgical Skills Training. World J. Gastroenterol. 2006, 12, 3219–3224. [Google Scholar] [CrossRef]
- Sweet, R.M.; Beach, R.; Sainfort, F.; Gupta, P.; Reihsen, T.; Poniatowski, L.H.; McDougall, E.M. Introduction and Validation of the American Urological Association Basic Laparoscopic Urologic Surgery Skills Curriculum. J. Endourol. 2012, 26, 190–196. [Google Scholar] [CrossRef]
- Neequaye, S.K.; Aggarwal, R.; Van Herzeele, I.; Darzi, A.; Cheshire, N.J. Endovascular Skills Training and Assessment. J. Vasc. Surg. 2007, 46, 1055–1064. [Google Scholar] [CrossRef] [PubMed]
- Mittal, M.K.; Dumon, K.R.; Edelson, P.K.; Acero, N.M.; Hashimoto, D.; Danzer, E.; Selvan, B.; Resnick, A.S.; Morris, J.B.; Williams, N.N. Successful Implementation of the American College of Surgeons/Association of Program Directors in Surgery Surgical Skills Curriculum via a 4-Week Consecutive Simulation Rotation. Simul. Healthc. 2012, 7, 147–154. [Google Scholar] [CrossRef]
- Alaraj, A.; Lemole, M.; Finkle, J.; Yudkowsky, R.; Wallace, A.; Luciano, C.; Banerjee, P.P.; Rizzi, S.; Charbel, F. Virtual Reality Training in Neurosurgery: Review of Current Status and Future Applications. Surg. Neurol. Int. 2011, 2, 52. [Google Scholar] [CrossRef]
- Gallagher, A.G.; Ritter, E.M.; Champion, H.; Higgins, G.; Fried, M.P.; Moses, G.; Smith, C.D.; Satava, R.M. Virtual Reality Simulation for the Operating Room: Proficiency-Based Training as a Paradigm Shift in Surgical Skills Training. Ann. Surg. 2005, 241, 364–372. [Google Scholar] [CrossRef]
- Haiser, A.; Aydin, A.; Kunduzi, B.; Ahmed, K.; Dasgupta, P. A Systematic Review of Simulation-Based Training in Vascular Surgery. J. Surg. Res. 2022, 279, 409–419. [Google Scholar] [CrossRef] [PubMed]
- Rudarakanchana, N.; Van Herzeele, I.; Desender, L.; Cheshire, N.J. Virtual Reality Simulation for the Optimization of Endovascular Procedures: Current Perspectives. Vasc. Health Risk Manag. 2015, 11, 195–202. [Google Scholar] [CrossRef]
- See, K.W.M.; Chui, K.H.; Chan, W.H.; Wong, K.C.; Chan, Y.C. Evidence for Endovascular Simulation Training: A Systematic Review. Eur. J. Vasc. Endovasc. Surg. 2016, 51, 441–451. [Google Scholar] [CrossRef] [PubMed]
- Schijven, M.; Jakimowicz, J. Virtual Reality Surgical Laparoscopic Simulators: How to Choose. Surg. Endosc. Other Interv. Tech. 2003, 17, 1943–1950. [Google Scholar] [CrossRef]
- Dankelman, J.; Chmarra, M.K.; Verdaasdonk, E.G.G.; Stassen, L.P.S.; Grimbergen, C.A. Fundamental Aspects of Learning Minimally Invasive Surgical Skills. Minim. Invasive Ther. Allied. Technol. 2005, 14, 247–256. [Google Scholar] [CrossRef]
- Chevallier, C.; Willaert, W.; Kawa, E.; Centola, M.; Steger, B.; Dirnhofer, R.; Mangin, P.; Grabherr, S. Postmortem Circulation: A New Model for Testing Endovascular Devices and Training Clinicians in Their Use. Clinl. Anat. 2014, 27, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Nelson, K.; Bagnall, A.; Nesbitt, C.; Davey, P.; Mafeld, S. Developing Cross-Specialty Endovascular Simulation Training. Clin. Teach. 2014, 11, 411–415. [Google Scholar] [CrossRef] [PubMed]
- Mafeld, S.; Nesbitt, C.; McCaslin, J.; Bagnall, A.; Davey, P.; Bose, P.; Williams, R. Three-Dimensional (3D) Printed Endovascular Simulation Models: A Feasibility Study. Ann. Transl. Med. 2017, 5, 42. [Google Scholar] [CrossRef]
- Gerbolés, A.G.; Galetti, M.; Rossi, S.; lo Muzio, F.P.; Pinelli, S.; Delmonte, N.; Caffarra Malvezzi, C.; Macaluso, C.; Miragoli, M.; Foresti, R. Three-Dimensional Bioprinting of Organoid-Based Scaffolds (OBST) for Long-Term Nanoparticle Toxicology Investigation. Int. J. Mol. Sci. 2023, 24, 6595. [Google Scholar] [CrossRef]
- Foresti, R.; MacAluso, C.; Rossi, S.; Selleri, S.; Perini, P.; Freyrie, A.; Raposio, E.; Fenaroli, P.; Concari, G.; De Filippo, M.; et al. 3D Reconstruction Cutting and Smart Devices for Personalized Medicine. In Proceedings of the 2020 Italian Conference on Optics and Photonics, Parma, Italy, 9–11 September 2020. [Google Scholar] [CrossRef]
- Ganguli, A.; Pagan-Diaz, G.J.; Grant, L.; Cvetkovic, C.; Bramlet, M.; Vozenilek, J.; Kesavadas, T.; Bashir, R. 3D Printing for Preoperative Planning and Surgical Training: A Review. Biomed. Microdevices 2018, 20, 65. [Google Scholar] [CrossRef]
- Foresti, R.; Rossi, S.; Pinelli, S.; Alinovi, R.; Barozzi, M.; Sciancalepore, C.; Galetti, M.; Caffarra, C.; Lagonegro, P.; Scavia, G.; et al. Highly-Defined Bioprinting of Long-Term Vascularized Scaffolds with Bio-Trap: Complex Geometry Functionalization and Process Parameters with Computer Aided Tissue Engineering. Materialia 2020, 9, 100560. [Google Scholar] [CrossRef]
- Wang, C.; Zhang, L.; Qin, T.; Xi, Z.; Sun, L.; Wu, H.; Li, D. 3D Printing in Adult Cardiovascular Surgery and Interventions: A Systematic Review. J. Thorac. Dis. 2020, 12, 3227–3237. [Google Scholar] [CrossRef] [PubMed]
- Gillaspie, E.A.; Matsumoto, J.S.; Morris, N.E.; Downey, R.J.; Shen, K.R.; Allen, M.S.; Blackmon, S.H. From 3-Dimensional Printing to 5-Dimensional Printing: Enhancing Thoracic Surgical Planning and Resection of Complex Tumors. Ann. Thorac. Surg. 2016, 101, 1958–1962. [Google Scholar] [CrossRef]
- Hsieh, T.Y.; Dedhia, R.; Cervenka, B.; Tollefson, T.T. 3D Printing: Current Use in Facial Plastic and Reconstructive Surgery. Curr. Opin. Otolaryngol. Head Neck Surg. 2017, 25, 291–299. [Google Scholar] [CrossRef]
- Larochelle, R.D.; Mann, S.E.; Ifantides, C. 3D Printing in Eye Care. Ophthalmol. Ther. 2021, 10, 733–752. [Google Scholar] [CrossRef]
- Zoccali, F.; Colizza, A.; Cialente, F.; Di Stadio, A.; La Mantia, I.; Hanna, C.; Minni, A.; Ralli, M.; Greco, A.; de Vincentiis, M. 3D Printing in Otolaryngology Surgery: Descriptive Review of Literature to Define the State of the Art. Healthcare 2023, 11, 108. [Google Scholar] [CrossRef]
- Meglioli, M.; Naveau, A.; Macaluso, G.M.; Catros, S. 3D Printed Bone Models in Oral and Cranio-Maxillofacial Surgery: A Systematic Review. 3D Print Med. 2020, 6, 30. [Google Scholar] [CrossRef]
- Vakharia, V.N.; Vakharia, N.N.; Hill, C.S. Review of 3-Dimensional Printing on Cranial Neurosurgery Simulation Training. World Neurosurg. 2016, 88, 188–198. [Google Scholar] [CrossRef]
- Chen, P.-C.; Chang, C.-C.; Chen, H.-T.; Lin, C.-Y.; Ho, T.-Y.; Chen, Y.-J.; Tsai, C.-H.; Tsou, H.-K.; Lin, C.-S.; Chen, Y.-W.; et al. The Accuracy of 3D Printing Assistance in the Spinal Deformity Surgery. Biomed. Res. Int. 2019, 11, 7196528. [Google Scholar] [CrossRef]
- Demeco, A.; Foresti, R.; Frizziero, A.; Daracchi, N.; Renzi, F.; Rovellini, M.; Salerno, A.; Martini, C.; Pelizzari, L.; Costantino, C. The Upper Limb Orthosis in the Rehabilitation of Stroke Patients: The Role of 3D Printing. Bioengineering 2023, 10, 1256. [Google Scholar] [CrossRef] [PubMed]
- Goda, I.; Nachtane, M.; Qureshi, Y.; Benyahia, H.; Tarfaoui, M. COVID-19: Current Challenges Regarding Medical Healthcare Supplies and Their Implications on the Global Additive Manufacturing Industry. Proc. Inst. Mech. Eng. Part H 2022, 236, 613–627. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Wang, J.; Fang, S.; Wang, H.; Bai, Y.; Zhao, Z.; Zhu, Q.; Wang, C.; Chen, G.; Jiang, H.; et al. Effect of Polycaprolactone Impregnation on the Properties of Calcium Silicate Scaffolds Fabricated by 3D Printing. Mater. Des. 2022, 220, 110856. [Google Scholar] [CrossRef]
- Ghidini, T. Regenerative Medicine and 3D Bioprinting for Human Space Exploration and Planet Colonisation. J. Thorac. Dis. 2018, 10, S2363–S2375. [Google Scholar] [CrossRef] [PubMed]
- Culmone, C.; Smit, G.; Breedveld, P. Additive Manufacturing of Medical Instruments: A State-of-the-Art Review. Addit. Manuf. 2019, 27, 461–473. [Google Scholar] [CrossRef]
- Dehghan-Manshadi, A.; Yu, P.; Dargusch, M.; StJohn, D.; Qian, M. Metal Injection Moulding of Surgical Tools, Biomaterials and Medical Devices: A Review. Powder Technol. 2020, 364, 189–204. [Google Scholar] [CrossRef]
- ISO/ASTM 52900:2021(en); Additive Manufacturing – General Principles – Fundamentals and Vocabulary. ISO: Geneva Switzerland, 2021. Available online: https://www.iso.org/obp/ui/#iso:std:iso-astm:52900:ed-2:v1:en (accessed on 21 December 2023).
- Jahnke, P.; Schwarz, S.; Ziegert, M.; Schwarz, F.B.; Hamm, B.; Scheel, M. Paper-Based 3D Printing of Anthropomorphic CT Phantoms: Feasibility of Two Construction Techniques. Eur. Radiol. 2019, 29, 1384–1390. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, M.A.; Popescu, A.C. 3D Printing at Micro-Level: Laser-Induced Forward Transfer and Two-Photon Polymerization. Polymers 2021, 13, 2034. [Google Scholar] [CrossRef]
- Trenfield, S.J.; Januskaite, P.; Goyanes, A.; Wilsdon, D.; Rowland, M.; Gaisford, S.; Basit, A.W. Prediction of Solid-State Form of SLS 3D Printed Medicines Using NIR and Raman Spectroscopy. Pharmaceutics 2022, 14, 589. [Google Scholar] [CrossRef]
- Chen, X.; Wang, S.; Wu, J.; Duan, S.; Wang, X.; Hong, X.; Han, X.; Li, C.; Kang, D.; Wang, Z.; et al. The Application and Challenge of Binder Jet 3D Printing Technology in Pharmaceutical Manufacturing. Pharmaceutics 2022, 14, 2589. [Google Scholar] [CrossRef] [PubMed]
- Salmi, M. Additive Manufacturing Processes in Medical Applications. Materials 2021, 14, 191. [Google Scholar] [CrossRef] [PubMed]
- Foresti, R.; Ghezzi, B.; Vettori, M.; Bergonzi, L.; Attolino, S.; Rossi, S.; Tarabella, G.; Vurro, D.; von Zeppelin, D.; Iannotta, S.; et al. 3D Printed Masks for Powders and Viruses Safety Protection Using Food Grade Polymers: Empirical Tests. Polymers 2021, 13, 617. [Google Scholar] [CrossRef]
- Gülcan, O.; Günaydın, K.; Tamer, A. The State of the Art of Material Jetting—A Critical Review. Polymers 2021, 13, 2829. [Google Scholar] [CrossRef]
- Segaran, N.; Saini, G.; Mayer, J.L.; Naidu, S.; Patel, I.; Alzubaidi, S.; Oklu, R. Application of 3d Printing in Preoperative Planning. J. Clin. Med. 2021, 10, 917. [Google Scholar] [CrossRef]
- Patel, P.; Dhal, K.; Gupta, R.; Tappa, K.; Rybicki, F.J.; Ravi, P. Medical 3D Printing Using Desktop Inverted Vat Photopolymerization: Background, Clinical Applications, and Challenges. Bioengineering 2023, 10, 782. [Google Scholar] [CrossRef]
- Foresti, R.; Rossi, S.; Pinelli, S.; Alinovi, R.; Sciancalepore, C.; Delmonte, N.; Selleri, S.; Caffarra, C.; Raposio, E.; Macaluso, G.; et al. In-Vivo Vascular Application via Ultra-Fast Bioprinting for Future 5D Personalised Nanomedicine. Sci. Rep. 2020, 10, 3205. [Google Scholar] [CrossRef]
- Kokkinis, D.; Schaffner, M.; Studart, A.R. Multimaterial Magnetically Assisted 3D Printing of Composite Materials. Nat. Commun. 2015, 6, 8643. [Google Scholar] [CrossRef]
- Hseino, H.; Nugent, E.; Lee, M.J.; Hill, A.D.K.; Neary, P.; Tierney, S.; Moneley, D.; Given, M. Skills Transfer after Proficiency-Based Simulation Training in Superficial Femoral Artery Angioplasty. Simul. Healthc. 2012, 7, 274–281. [Google Scholar] [CrossRef]
- Unver, V.; Basak, T.; Watts, P.; Gaioso, V.; Moss, J.; Tastan, S.; Iyigun, E.; Tosun, N. The Reliability and Validity of Three Questionnaires: The Student Satisfaction and Self-Confidence in Learning Scale, Simulation Design Scale, and Educational Practices Questionnaire. Contemp. Nurse 2017, 53, 60–74. [Google Scholar] [CrossRef]
- Lawaetz, J.; Skovbo Kristensen, J.S.; Nayahangan, L.J.; Van Herzeele, I.; Konge, L.; Eiberg, J.P. Simulation Based Training and Assessment in Open Vascular Surgery: A Systematic Review. Eur. J. Vasc. Endovasc. Surg. 2021, 61, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Sroka, G.; Feldman, L.S.; Vassiliou, M.C.; Kaneva, P.A.; Fayez, R.; Fried, G.M. Fundamentals of Laparoscopic Surgery Simulator Training to Proficiency Improves Laparoscopic Performance in the Operating Room-a Randomized Controlled Trial. Am. J. Surg. 2010, 199, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Kaschwich, M.; Dell, A.; Matysiak, F.; Bouchagiar, J.; Bayer, A.; Scharfschwerdt, M.; Ernst, F.; Kleemann, M.; Horn, M. Development of an Ultrasound-Capable Phantom with Patient-Specific 3D-Printed Vascular Anatomy to Simulate Peripheral Endovascular Interventions. Ann. Anat. 2020, 232, 151563. [Google Scholar] [CrossRef] [PubMed]
- Wooster, M.; Doyle, A.; Hislop, S.; Glocker, R.; Armstrong, P.; Singh, M.; Illig, K.A. REHEARSAL Using Patient-Specific Simulation to Improve Endovascular Efficiency. Vasc. Endovascular. Surg. 2018, 52, 169–172. [Google Scholar] [CrossRef]
- Chaer, R.A.; DeRubertis, B.G.; Lin, S.C.; Bush, H.L.; Karwowski, J.K.; Birk, D.; Morrissey, N.J.; Faries, P.L.; McKinsey, J.F.; Kent, K.C. Simulation Improves Resident Performance in Catheter-Based Intervention: Results of a Randomized, Controlled Study. Ann. Surg. 2006, 244, 343–349. [Google Scholar] [CrossRef]
- Uhl, J.F.; Sufianov, A.; Ruiz, C.; Iakimov, Y.; Mogorron, H.J.; Encarnacion Ramirez, M.; Prat, G.; Lorea, B.; Baldoncini, M.; Goncharov, E.; et al. The Use of 3D Printed Models for Surgical Simulation of Cranioplasty in Craniosynostosis as Training and Education. Brain Sci. 2023, 13, 894. [Google Scholar] [CrossRef]
- Pietrabissa, A.; Marconi, S.; Negrello, E.; Mauri, V.; Peri, A.; Pugliese, L.; Marone, E.M.; Auricchio, F. An Overview on 3D Printing for Abdominal Surgery. Surg. Endosc. 2020, 34, 1–13. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year of Residency | Age (y ± SD) | n = 12 | n. of Previous Arterial Peripheral Revascularization Experience | ||
|---|---|---|---|---|---|
| 1st Operator | 2nd Operator | 3rd Operator | |||
| 1st year | 26.5 ± 0.7 | 2 | 0 | 0 | 3 |
| 2nd year | 27 | 1 | 0 | 2 | 5 |
| 3rd year | 29.8 ± 1.7 | 6 | 3 | 10 | 15 |
| 4th year | 29 | 1 | 4 | 15 | 20 |
| 5th year | 31.5 ± 0.7 | 2 | 5 | 20 | 25 |
| Male/Female | 4/8 | ||||
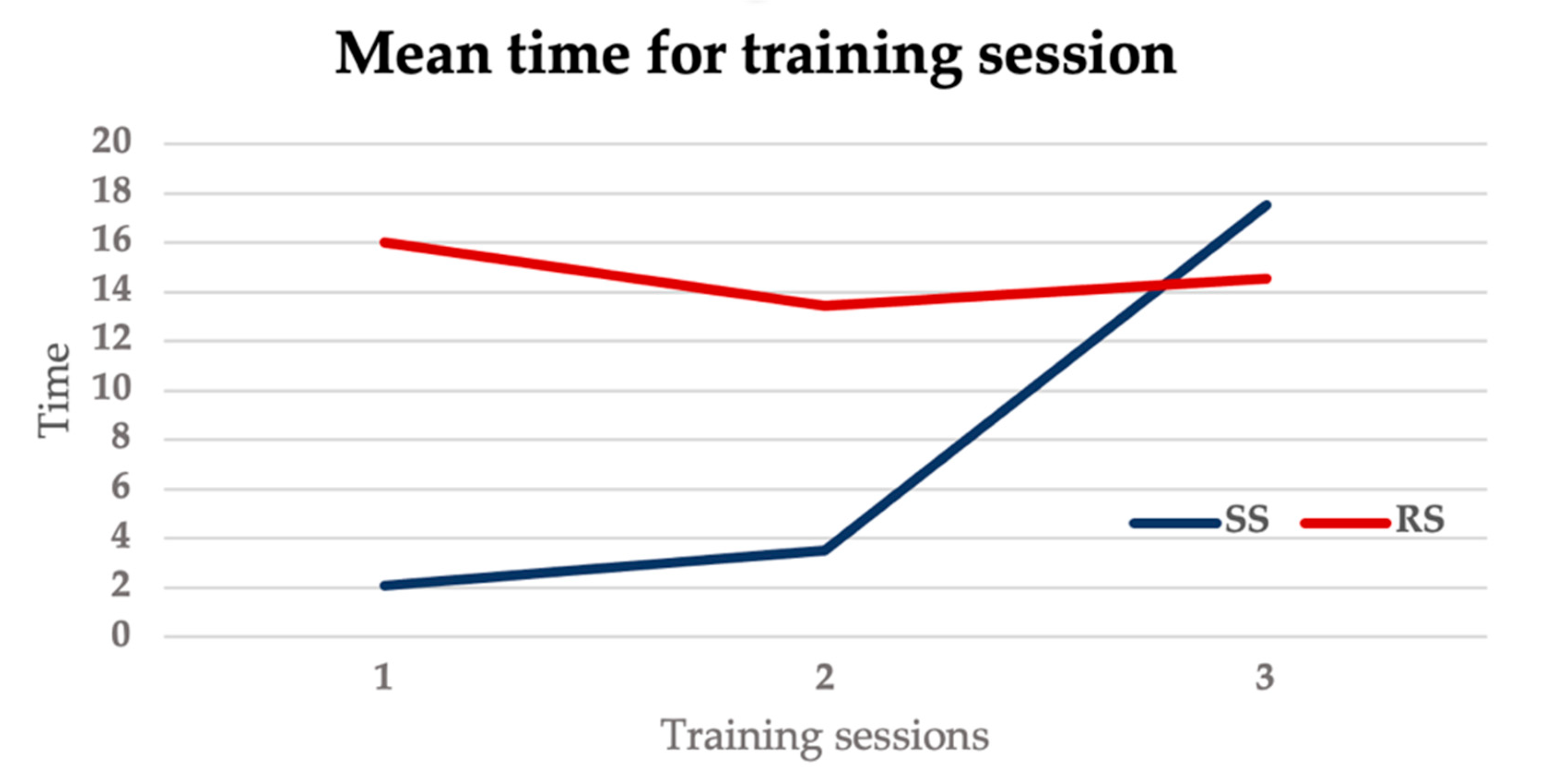
| Randomization Group | Training Sessions (Time, min.s ± SD) | |||
|---|---|---|---|---|
| 1 | 2 | 3 (Evaluated) | Total | |
| SS group | 2.10 ± 1.74 | 3.49 ± 2.59 | 17.54 ± 8.43 | 23.13 ± 9.2 |
| RS group | 15.59 ± 18.54 | 13.42 ± 9.54 | 14.55 ± 8.4 | 44.6 ± 12.8 |
| Global Rating Scale of Endovascular Performance | SS Group | RS Group |
|---|---|---|
| Time and motion | 2.33 | 2.66 |
| Wire and catheter handling | 2.5 | 2.66 |
| Awareness of wire position | 2 | 2.66 |
| Maintenance of wire stability | 2.66 | 2.33 |
| Precision of wire/catheter technique | 2.17 | 2 |
| Flow of operation | 2.33 | 2.33 |
| Ability to complete the simulation | 3.33 | 3.66 |
| Need for verbal prompts | 2.33 | 1.83 |
| Attending takeover | 1.83 | 1.33 |
| Total score | 21.5 | 21.5 |
| Satisfaction with Current Learning | SD | D | UN | A | SA |
|---|---|---|---|---|---|
| n = 12 (%) | |||||
| The teaching methods used in this simulation were helpful and effective | 6 (50) | 6 (50) | |||
| The simulation provided me with a variety of learning materials and activities to promote my learning the medical surgical curriculum | 2 (16.6) | 5 (41.7) | 5 (41.7) | ||
| I enjoyed how my instructor taught the simulation | 4 (33.3) | 8 (66.7) | |||
| The teaching materials used in this simulation were motivating and helped me to learn | 1 (8.4) | 4 (33.3) | 7 (58.3) | ||
| The way my instructor taught the simulation was suitable to the way I learn | 1 (8.4) | 1 (33.3) | 7 (58.3) | ||
| Self Confidence in Learning | SD | D | UN | A | SA |
| n = 12 (%) | |||||
| I am confident that I am mastering the content of the simulation activity that my instructors presented to me | 8 (66.7) | 4 (33.3) | |||
| I am confident that this simulation covered critical content necessary for the mastery of medical surgical curriculum | 4 (33.3) | 4 (33.3) | 4 (33.3) | ||
| I am confident that I am developing the skills and obtaining the required knowledge from this simulation to perform necessary tasks in a clinical setting | 2 (16.6) | 5 (41.7) | 5 (41.7) | ||
| My instructors used helpful resources to teach the simulation | 5 (41.7) | 7 (58.3) | |||
| It is my responsibility as the student to learn what I need to know from this simulation activity | 1 (8.4) | 3 (24.9) | 8 (66.7) | ||
| I know how to get help when I do not understand the concepts covered in the simulation | 1 (8.4) | 5 (41.7) | 6 (50) | ||
| I know how to use simulation activities to learn critical aspects of these skills | 8 (66.7) | 4 (33.3) | |||
| It is the instructor’s responsibility to tell me what I need to learn of the simulation activity content during class time | 1 (8.4) | 5 (41.7) | 6 (50) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Foresti, R.; Fornasari, A.; Bianchini Massoni, C.; Mersanne, A.; Martini, C.; Cabrini, E.; Freyrie, A.; Perini, P. Surgical Medical Education via 3D Bioprinting: Modular System for Endovascular Training. Bioengineering 2024, 11, 197. https://doi.org/10.3390/bioengineering11020197
Foresti R, Fornasari A, Bianchini Massoni C, Mersanne A, Martini C, Cabrini E, Freyrie A, Perini P. Surgical Medical Education via 3D Bioprinting: Modular System for Endovascular Training. Bioengineering. 2024; 11(2):197. https://doi.org/10.3390/bioengineering11020197
Chicago/Turabian StyleForesti, Ruben, Anna Fornasari, Claudio Bianchini Massoni, Arianna Mersanne, Chiara Martini, Elisa Cabrini, Antonio Freyrie, and Paolo Perini. 2024. "Surgical Medical Education via 3D Bioprinting: Modular System for Endovascular Training" Bioengineering 11, no. 2: 197. https://doi.org/10.3390/bioengineering11020197
APA StyleForesti, R., Fornasari, A., Bianchini Massoni, C., Mersanne, A., Martini, C., Cabrini, E., Freyrie, A., & Perini, P. (2024). Surgical Medical Education via 3D Bioprinting: Modular System for Endovascular Training. Bioengineering, 11(2), 197. https://doi.org/10.3390/bioengineering11020197