

Quantification of Analgesic and Anti-Inflammatory Lipid Mediators in Long-Term Cryopreserved and Freeze-Dried Preserved Human Amniotic Membrane
 ,
,
Abstract
1. Introduction
2. Materials and Methods
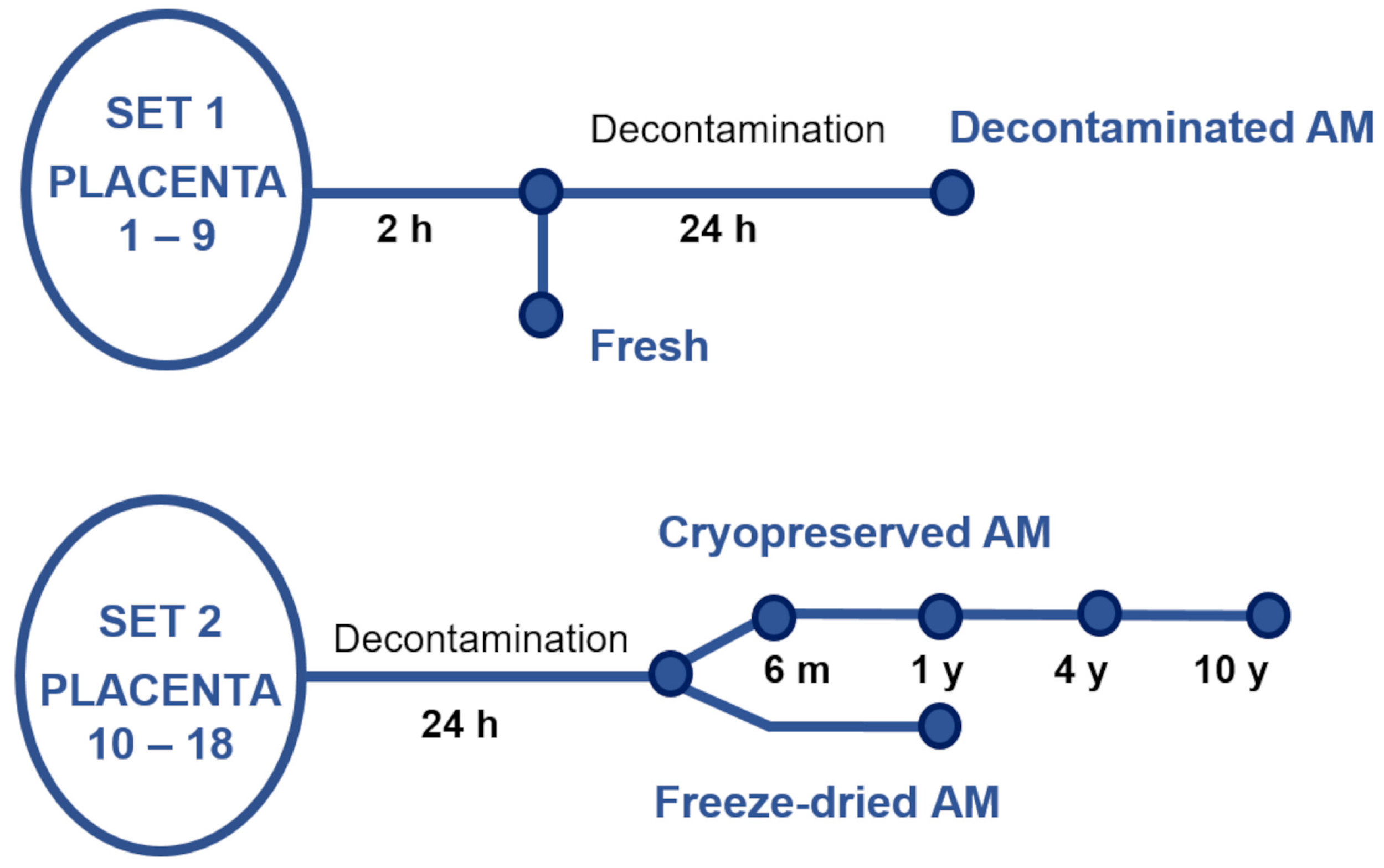
2.1. Placenta Retrieval, Decontamination, and Amniotic Membrane Preparation
2.2. Sample Preparation
2.2.1. Fresh and Decontaminated Samples
2.2.2. Cryopreserved and Lyophilized Samples
2.3. Sample Preparation and UHPLC/MS of NAEs
2.4. Immunohistochemistry for PPAR α Receptor
2.5. Statistical Analysis
3. Results
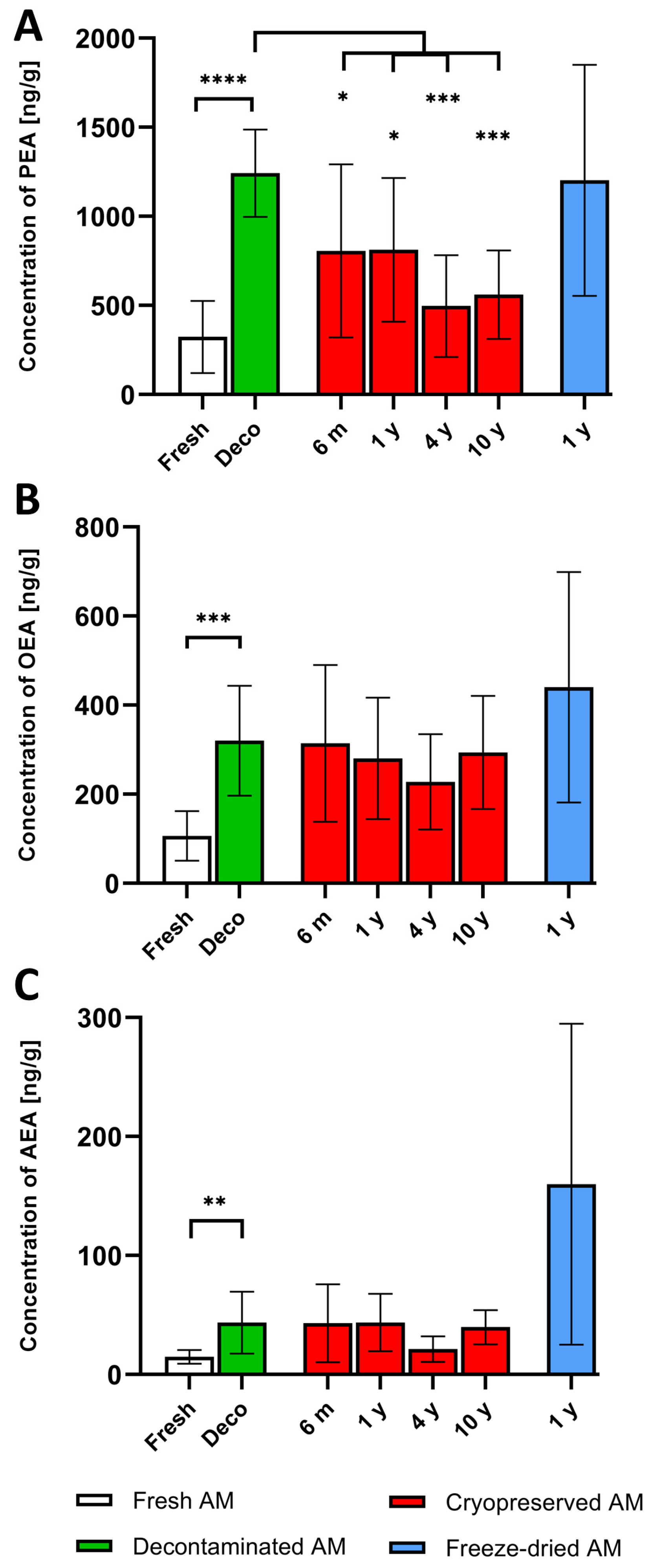
3.1. NAE Concentrations in Fresh, Cryopreserved and Freeze-Dried Amniotic Membrane
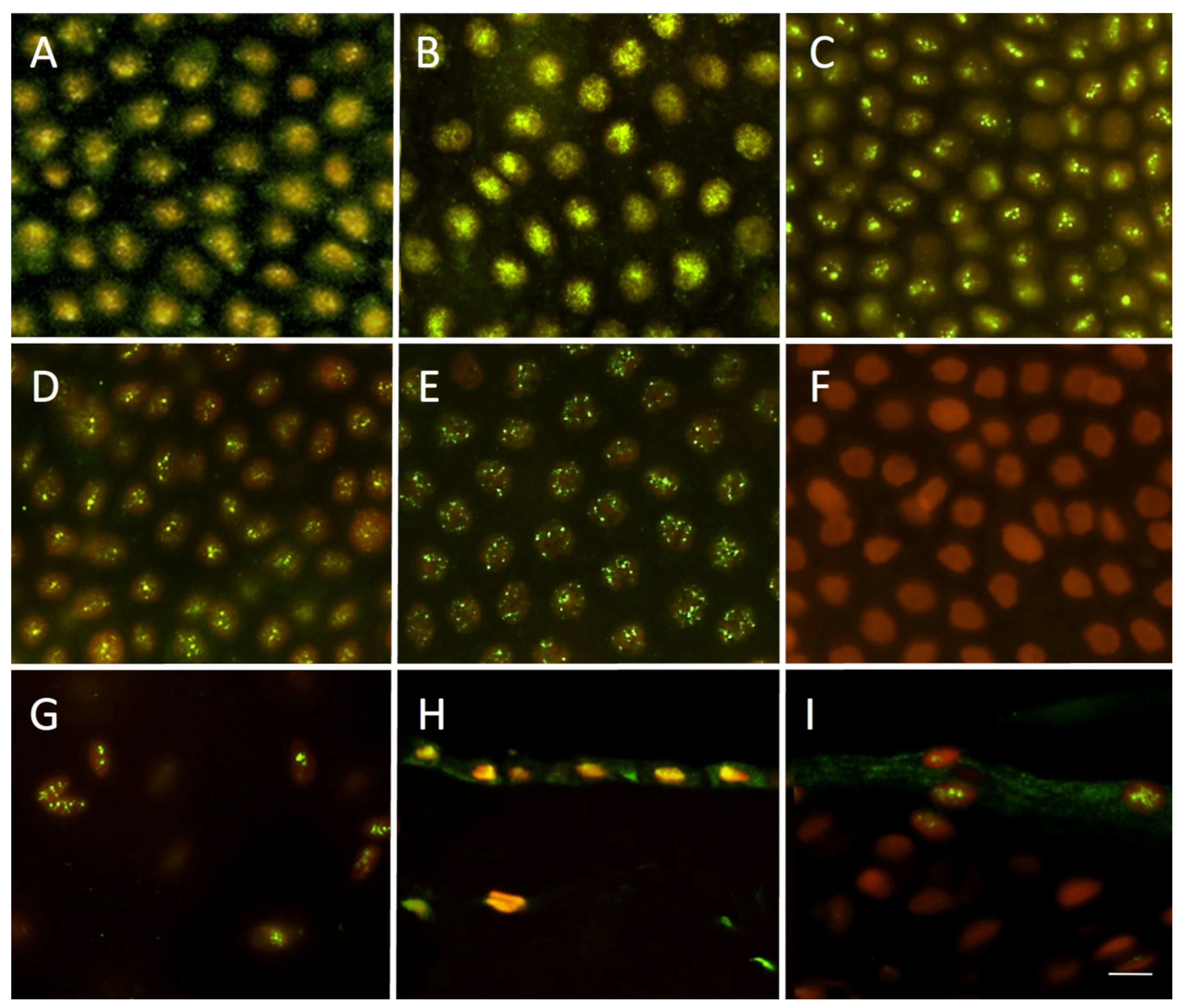
3.2. The Detection of PPAR-α Receptor Using Indirect Immunohistochemistry
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nejad, A.R.; Hamidieh, A.A.; Amirkhani, M.A.; Sisakht, M.M. Update review on five top clinical applications of human amniotic membrane in regenerative medicine. Placenta 2021, 103, 104–119. [Google Scholar] [CrossRef]
- Liu, Q.-W.; Huang, Q.-M.; Wu, H.-Y.; Zuo, G.-S.-L.; Gu, H.-C.; Deng, K.-Y.; Xin, H.-B. Characteristics and Therapeutic Potential of Human Amnion-Derived Stem Cells. Int. J. Mol. Sci. 2021, 22, 970. [Google Scholar] [CrossRef]
- Weidinger, A.; Poženel, L.; Wolbank, S.; Banerjee, A. Sub-Regional Differences of the Human Amniotic Membrane and Their Potential Impact on Tissue Regeneration Application. Front. Bioeng. Biotechnol. 2021, 8, 613804. [Google Scholar] [CrossRef]
- Malhotra, C.; Jain, A.K. Human amniotic membrane transplantation: Different modalities of its use in ophthalmology. World J. Transplant. 2014, 4, 111–121. [Google Scholar] [CrossRef]
- Jirsova, K.; Jones, G.L.A. Amniotic membrane in ophthalmology: Properties, preparation, storage and indications for grafting—A review. Cell Tissue Bank 2017, 18, 193–204. [Google Scholar] [CrossRef]
- Anselmo, D.S.; McGuire, J.B.; Love, E.; Vlahovic, T. Application of Viable Cryopreserved Human Placental Membrane Grafts in the Treatment of Wounds of Diverse Etiologies: A Case Series. Wounds 2018, 30, 57–61. [Google Scholar]
- Farivar, B.S.; Toursavadkohi, S.; Monahan, T.S.; Sharma, J.; Ucuzian, A.A.; Kundi, R.; Sarkar, R.; Lal, B.K. Prospective study of cryopreserved placental tissue wound matrix in the management of chronic venous leg ulcers. J. Vasc. Surg. Venous Lymphat. Disord. 2019, 7, 228–233. [Google Scholar] [CrossRef]
- Lopez Martinez, J.A.; Rodriguez Valiente, M.; Fuente-Mora, C.; Garcia-Hernandez, A.M.; Canovas Sanchis, S.; Fernandez Pascual, C.J. Use of cryopreserved human amniotic membrane in the treatment of skin ulcers secondary to calciphylaxis. Dermatol. Ther. 2021, 34, e14769. [Google Scholar] [CrossRef]
- Game, F.; Gray, K.; Davis, D.; Sherman, R.; Chokkalingam, K.; Connan, Z.; Fakis, A.; Jones, M. The effectiveness of a new dried human amnion derived membrane in addition to standard care in treating diabetic foot ulcers: A patient and assessor blind, randomised controlled pilot study. Int. Wound J. 2021, 18, 692–700. [Google Scholar] [CrossRef]
- Mimouni, M.; Trinh, T.; Sorkin, N.; Cohen, E.; Santaella, G.; Rootman, D.S.; Slomovic, A.R.; Chan, C.C. Sutureless dehydrated amniotic membrane for persistent epithelial defects. Eur. J. Ophthalmol. 2022, 32, 875–879. [Google Scholar] [CrossRef]
- Serena, T.E.; Orgill, D.P.; Armstrong, D.G.; Galiano, R.D.; Glat, P.M.; Carter, M.J.; Kaufman, J.P.; Li, W.W.; Zelen, C.M. A Multicenter, Randomized, Controlled, Clinical Trial Evaluating Dehydrated Human Amniotic Membrane in the Treatment of Venous Leg Ulcers. Plast Reconstr. Surg. 2022, 150, 1128–1136. [Google Scholar] [CrossRef]
- Allen, C.L.; Clare, G.; Stewart, E.A.; Branch, M.J.; McIntosh, O.D.; Dadhwal, M.; Dua, H.S.; Hopkinson, A. Augmented dried versus cryopreserved amniotic membrane as an ocular surface dressing. PLoS ONE 2013, 8, e78441. [Google Scholar] [CrossRef]
- Morkin, M.I.; Hamrah, P. Efficacy of self-retained cryopreserved amniotic membrane for treatment of neuropathic corneal pain. Ocul. Surf. 2018, 16, 132–138. [Google Scholar] [CrossRef]
- Insausti, C.L.; Alcaraz, A.; García-Vizcaíno, E.M.; Mrowiec, A.; López-Martínez, M.C.; Blanquer, M.; Piñero, A.; Majado, M.J.; Moraleda, J.M.; Castellanos, G.; et al. Amniotic membrane induces epithelialization in massive posttraumatic wounds. Wound Repair. Regen. 2010, 18, 368–377. [Google Scholar] [CrossRef]
- Mao, Y.; Hoffman, T.; Dhall, S.; Singal, A.; Sathyamoorthy, M.; Danilkovitch, A.; Kohn, J. Endogenous viable cells in lyopreserved amnion retain differentiation potential and anti-fibrotic activity in vitro. Acta Biomater. 2019, 94, 330–339. [Google Scholar] [CrossRef]
- Alsina-Gibert, M.; Pedregosa-Fauste, S. Amniotic membrane transplantation in the treatment of chronic lower limb ulcers. Actas Dermosifiliogr. 2012, 103, 608–613. [Google Scholar] [CrossRef]
- Eskandarlou, M.; Azimi, M.; Rabiee, S.; Seif Rabiee, M.A. The Healing Effect of Amniotic Membrane in Burn Patients. World J. Plast. Surg. 2016, 5, 39–44. [Google Scholar]
- Navas, A.; Magaña-Guerrero, F.S.; Domínguez-López, A.; Chávez-García, C.; Partido, G.; Graue-Hernández, E.O.; Sánchez-García, F.J.; Garfias, Y. Anti-Inflammatory and Anti-Fibrotic Effects of Human Amniotic Membrane Mesenchymal Stem Cells and Their Potential in Corneal Repair. Stem Cells Transl. Med. 2018, 7, 906–917. [Google Scholar] [CrossRef]
- King, A.E.; Paltoo, A.; Kelly, R.W.; Sallenave, J.M.; Bocking, A.D.; Challis, J.R.G. Expression of Natural Antimicrobials by Human Placenta and Fetal Membranes. Placenta 2007, 28, 161–169. [Google Scholar] [CrossRef]
- Franco, G.R.; de Carvalho, A.F.; Kroon, E.G.; Lovagie, S.; Werenne, J.; Golgher, R.R.; Ferreira, P.C.P.; Bonjardim, C.A. Biological Activities of a Human Amniotic Membrane Interferon. Placenta 1999, 20, 189–196. [Google Scholar] [CrossRef]
- Koob, T.J.; Lim, J.J.; Massee, M.; Zabek, N.; Rennert, R.; Gurtner, G.; Li, W.W. Angiogenic properties of dehydrated human amnion/chorion allografts: Therapeutic potential for soft tissue repair and regeneration. Vasc. Cell 2014, 6, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Duan-Arnold, Y.; Uveges, T.E.; Gyurdieva, A.; Johnson, A.; Danilkovitch, A. Angiogenic Potential of Cryopreserved Amniotic Membrane Is Enhanced Through Retention of All Tissue Components in Their Native State. Adv. Wound Care 2015, 4, 513–522. [Google Scholar] [CrossRef]
- Shao, C.; Sima, J.; Zhang, S.X.; Jin, J.; Reinach, P.; Wang, Z.; Ma, J.-X. Suppression of Corneal Neovascularization by PEDF Release from Human Amniotic Membranes. Investig. Ophthalmol. Vis. Sci. 2004, 45, 1758–1762. [Google Scholar] [CrossRef] [PubMed]
- Yin, L.; Pi, Y.L. Effect of amnion membrane transplantation on corneal neovascularization in 10 patients with alkali burn. Int. J. Ophthalmol. 2011, 4, 110–111. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.C.; Tseng, S.C.G. The effects on inhibition of corneal neovascularization after human amniotic membrane transplantation in severely damaged rabbit corneas. Korean J. Ophthalmol. 1995, 9, 32–46. [Google Scholar] [CrossRef]
- Lee, S.H.; Tseng, S.C. Amniotic membrane transplantation for persistent epithelial defects with ulceration. Am. J. Ophthalmol. 1997, 123, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Wang, W. Lyophilization and development of solid protein pharmaceuticals. Int. J. Pharm. 2000, 203, 1–60. [Google Scholar] [CrossRef] [PubMed]
- Lim, L.S.; Poh, R.W.; Riau, A.K.; Beuerman, R.W.; Tan, D.; Mehta, J.S. Biological and ultrastructural properties of acelagraft, a freeze-dried gamma-irradiated human amniotic membrane. Arch. Ophthalmol. 2010, 128, 1303–1310. [Google Scholar] [CrossRef]
- Paolin, A.; Trojan, D.; Leonardi, A.; Mellone, S.; Volpe, A.; Orlandi, A.; Cogliati, E. Cytokine expression and ultrastructural alterations in fresh-frozen, freeze-dried and γ-irradiated human amniotic membranes. Cell Tissue Bank 2016, 17, 399–406. [Google Scholar] [CrossRef]
- McQuilling, J.P.; Vines, J.B.; Kimmerling, K.A.; Mowry, K.C. Proteomic Comparison of Amnion and Chorion and Evaluation of the Effects of Processing on Placental Membranes. Wounds 2017, 29, E36–E40. [Google Scholar]
- Johnson, A.; Gyurdieva, A.; Dhall, S.; Danilkovitch, A.; Duan-Arnold, Y. Understanding the Impact of Preservation Methods on the Integrity and Functionality of Placental Allografts. Ann. Plast. Surg. 2017, 79, 203–213. [Google Scholar] [CrossRef] [PubMed]
- DiDomenico, L.A.; Orgill, D.P.; Galiano, R.D.; Serena, T.E.; Carter, M.J.; Kaufman, J.P.; Young, N.J.; Jacobs, A.M.; Zelen, C.M. Use of an aseptically processed, dehydrated human amnion and chorion membrane improves likelihood and rate of healing in chronic diabetic foot ulcers: A prospective, randomised, multi-centre clinical trial in 80 patients. Int. Wound J. 2018, 15, 950–957. [Google Scholar] [CrossRef] [PubMed]
- Kadkhoda, Z.; Tavakoli, A.; Chokami Rafiei, S.; Zolfaghari, F.; Akbari, S. Effect of Amniotic Membrane Dressing on Pain and Healing of Palatal Donor Site: A Randomized Controlled Trial. Int. J. Organ Transplant. Med. 2020, 11, 55–62. [Google Scholar]
- Vaheb, M.; Kohestani, B.M.; Karrabi, M.; Khosrojerdi, M.; Khajeh, M.; Shahrestanaki, E.; Sahebkar, M. Evaluation of Dried Amniotic Membrane on Wound Healing at Split-Thickness Skin Graft Donor Sites: A Randomized, Placebo-Controlled, Double-blind Trial. Adv. Ski. Wound Care 2020, 33, 636–641. [Google Scholar] [CrossRef] [PubMed]
- Tseng, S.C. HC-HA/PTX3 Purified From Amniotic Membrane as Novel Regenerative Matrix: Insight Into Relationship Between Inflammation and Regeneration. Investig. Ophthalmol. Vis. Sci. 2016, 57, ORSFh1–ORSFh8. [Google Scholar] [CrossRef]
- Talmi, Y.P.; Finkelstein, Y.; Zohar, Y. Use of human amniotic membrane as a biologic dressing. Eur. J. Plast. Surg. 1990, 13, 160–162. [Google Scholar] [CrossRef]
- Kesting, M.R.; Wolff, K.D.; Hohlweg-Majert, B.; Steinstraesser, L. The role of allogenic amniotic membrane in burn treatment. J. Burn Care Res. 2008, 29, 907–916. [Google Scholar] [CrossRef]
- Liu, J.; Sheha, H.; Fu, Y.; Liang, L.; Tseng, S.C. Update on amniotic membrane transplantation. Expert Rev. Ophthalmol. 2010, 5, 645–661. [Google Scholar] [CrossRef]
- ElHeneidy, H.; Omran, E.; Hieneedy, H.; Halwagy, A.; Al-Inany, H.; Al-Ansary, M.; Gad, A. Amniotic membrane can be a valid source for wound healing. Int. J. Women’s Health 2016, 8, 225–231. [Google Scholar] [CrossRef]
- Svobodova, A.; Vrkoslav, V.; Smeringaiova, I.; Jirsova, K. Distribution of an analgesic palmitoylethanolamide and other N-acylethanolamines in human placental membranes. PLoS ONE 2023, 18, e0279863. [Google Scholar] [CrossRef]
- Esposito, E.; Cuzzocrea, S. Palmitoylethanolamide is a new possible pharmacological treatment for the inflammation associated with trauma. Mini Rev. Med. Chem. 2013, 13, 237–255. [Google Scholar] [PubMed]
- Lo Verme, J.; Fu, J.; Astarita, G.; La Rana, G.; Russo, R.; Calignano, A.; Piomelli, D. The nuclear receptor peroxisome proliferator-activated receptor-alpha mediates the anti-inflammatory actions of palmitoylethanolamide. Mol. Pharmacol. 2005, 67, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Esposito, E.; Cuzzocrea, S. Palmitoylethanolamide in Homeostatic and Traumatic Central Nervous System Injuries. CNS Neurol. Disord. Drug Targets 2013, 12, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Keppel Hesselink, J.M. Professor Rita Levi-Montalcini on Nerve Growth Factor, Mast Cells and Palmitoylethanolamide, an Endogenous Anti-Inflammatory and Analgesic Compound. J. Pain Relief. 2013, 2, 1000114. [Google Scholar] [CrossRef]
- Suardiaz, M.; Estivill-Torrus, G.; Goicoechea, C.; Bilbao, A.; Rodriguez de Fonseca, F. Analgesic properties of oleoylethanolamide (OEA) in visceral and inflammatory pain. Pain 2007, 133, 99–110. [Google Scholar] [CrossRef]
- Gatti, A.; Lazzari, M.; Gianfelice, V.; Di Paolo, A.; Sabato, E.; Sabato, A.F. Palmitoylethanolamide in the treatment of chronic pain caused by different etiopathogenesis. Pain Med. 2012, 13, 1121–1130. [Google Scholar] [CrossRef]
- Di Paola, R.; Impellizzeri, D.; Fusco, R.; Cordaro, M.; Siracusa, R.; Crupi, R.; Esposito, E.; Cuzzocrea, S. Ultramicronized palmitoylethanolamide (PEA-um((R))) in the treatment of idiopathic pulmonary fibrosis. Pharmacol. Res. 2016, 111, 405–412. [Google Scholar] [CrossRef]
- Paladini, A.; Fusco, M.; Cenacchi, T.; Schievano, C.; Piroli, A.; Varrassi, G. Palmitoylethanolamide, a Special Food for Medical Purposes, in the Treatment of Chronic Pain: A Pooled Data Meta-analysis. Pain Physician 2016, 19, 11–24. [Google Scholar]
- Di Marzo, V. ’Endocannabinoids’ and other fatty acid derivatives with cannabimimetic properties: Biochemistry and possible physiopathological relevance. Biochim. Biophys. Acta 1998, 1392, 153–175. [Google Scholar] [CrossRef]
- Correia-Sa, I.B.; Carvalho, C.M.; Serrao, P.V.; Loureiro, A.I.; Fernandes-Lopes, C.; Marques, M.; Vieira-Coelho, M.A. A new role for anandamide: Defective link between the systemic and skin endocannabinoid systems in hypertrophic human wound healing. Sci. Rep. 2020, 10, 11134. [Google Scholar] [CrossRef] [PubMed]
- Ruhl, T.; Corsten, C.; Beier, J.P.; Kim, B.S. The immunosuppressive effect of the endocannabinoid system on the inflammatory phenotypes of macrophages and mesenchymal stromal cells: A comparative study. Pharmacol. Rep. 2021, 73, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.; Gaetani, S.; Oveisi, F.; Lo Verme, J.; Serrano, A.; Rodriguez De Fonseca, F.; Rosengarth, A.; Luecke, H.; Di Giacomo, B.; Tarzia, G.; et al. Oleylethanolamide regulates feeding and body weight through activation of the nuclear receptor PPAR-alpha. Nature 2003, 425, 90–93. [Google Scholar] [CrossRef]
- Svobodova, A.; Horvath, V.; Smeringaiova, I.; Cabral, J.V.; Zemlickova, M.; Fiala, R.; Burkert, J.; Nemetova, D.; Stadler, P.; Lindner, J.; et al. The healing dynamics of non-healing wounds using cryo-preserved amniotic membrane. Int. Wound J. 2022, 19, 1243–1252. [Google Scholar] [CrossRef] [PubMed]
- Thomasen, H.; Pauklin, M.; Noelle, B.; Geerling, G.; Vetter, J.; Steven, P.; Steuhl, K.P.; Meller, D. The effect of long-term storage on the biological and histological properties of cryopreserved amniotic membrane. Curr. Eye Res. 2011, 36, 247–255. [Google Scholar] [CrossRef]
- Dhall, S.; Sathyamoorthy, M.; Kuang, J.Q.; Hoffman, T.; Moorman, M.; Lerch, A.; Jacob, V.; Sinclair, S.M.; Danilkovitch, A. Properties of viable lyopreserved amnion are equivalent to viable cryopreserved amnion with the convenience of ambient storage. PLoS ONE 2018, 13, e0204060. [Google Scholar] [CrossRef] [PubMed]
- Merjava, S.; Neuwirth, A.; Tanzerova, M.; Jirsova, K. The spectrum of cytokeratins expressed in the adult human cornea, limbus and perilimbal conjunctiva. Histol. Histopathol. 2011, 26, 323–331. [Google Scholar] [CrossRef]
- Trosan, P.; Cabral, J.V.; Smeringaiova, I.; Studeny, P.; Jirsova, K. Interleukin-13 increases the stemness of limbal epithelial stem cells cultures. PLoS ONE 2022, 17, e0272081. [Google Scholar] [CrossRef]
- Trivedi, N.R.; Cong, Z.; Nelson, A.M.; Albert, A.J.; Rosamilia, L.L.; Sivarajah, S.; Gilliland, K.L.; Liu, W.; Mauger, D.T.; Gabbay, R.A.; et al. Peroxisome proliferator-activated receptors increase human sebum production. J. Investig. Dermatol. 2006, 126, 2002–2009. [Google Scholar] [CrossRef]
- Lam, P.M.; Marczylo, T.H.; Konje, J.C. Simultaneous measurement of three N-acylethanolamides in human bio-matrices using ultra performance liquid chromatography-tandem mass spectrometry. Anal. Bioanal. Chem. 2010, 398, 2089–2097. [Google Scholar] [CrossRef]
- Georgiadis, N.S.; Ziakas, N.G.; Boboridis, K.G.; Terzidou, C.; Mikropoulos, D.G. Cryopreserved amniotic membrane transplantation for the management of symptomatic bullous keratopathy. Clin. Exp. Ophthalmol. 2008, 36, 130–135. [Google Scholar] [CrossRef]
- Sharma, N.; Singh, D.; Maharana, P.K.; Kriplani, A.; Velpandian, T.; Pandey, R.M.; Vajpayee, R.B. Comparison of Amniotic Membrane Transplantation and Umbilical Cord Serum in Acute Ocular Chemical Burns: A Randomized Controlled Trial. Am. J. Ophthalmol. 2016, 168, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Loeffelbein, D.J.; Rohleder, N.H.; Eddicks, M.; Baumann, C.M.; Stoeckelhuber, M.; Wolff, K.D.; Drecoll, E.; Steinstraesser, L.; Hennerbichler, S.; Kesting, M.R. Evaluation of human amniotic membrane as a wound dressing for split-thickness skin-graft donor sites. Biomed. Res. Int. 2014, 2014, 572183. [Google Scholar] [CrossRef] [PubMed]
- Zidan, S.M.; Eleowa, S.A.; Nasef, M.A.; Abd-Almoktader, M.A.; Elbatawy, A.M.; Borhamy, A.G.; Aboliela, M.A.; Ali, A.M.; Algamal, M.R. Maximizing the safety of glycerol preserved human amniotic membrane as a biological dressing. Burns 2015, 41, 1498–1503. [Google Scholar] [CrossRef] [PubMed]
- Rankin, L.; Fowler, C.J. The Basal Pharmacology of Palmitoylethanolamide. Int. J. Mol. Sci. 2020, 21, 7942. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Samples | Fresh | Deco | Cryo 6 m | Cryo 1 y | Cryo 4 y | Cryo 10 y | F-Dry 1 y |
|---|---|---|---|---|---|---|---|
| PEA (AV) | 323.85 | 1241.76 | 806.26 | 812.86 | 497.16 | 561.16 | 1121.76 |
| PEA (SD) | 202.68 | 245.07 | 485.69 | 403.27 | 285.76 | 248.25 | 692.50 |
| OEA (AV) | 106.56 | 320.42 | 314.30 | 280.56 | 227.87 | 293.77 | 440.25 |
| OEA (SD) | 55.68 | 123.26 | 175.76 | 136.40 | 106.84 | 127.06 | 258.60 |
| AEA (AV) | 14.87 | 43.58 | 43.19 | 43.70 | 21.31 | 39.76 | 160.00 |
| AEA (SD) | 5.82 | 26.02 | 32.75 | 24.09 | 10.74 | 14.39 | 134.99 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vrkoslav, V.; Smeringaiova, I.; Smorodinova, N.; Svobodova, A.; Strnad, S.; Jackson, C.J.; Burkert, J.; Jirsova, K. Quantification of Analgesic and Anti-Inflammatory Lipid Mediators in Long-Term Cryopreserved and Freeze-Dried Preserved Human Amniotic Membrane. Bioengineering 2023, 10, 740. https://doi.org/10.3390/bioengineering10060740
Vrkoslav V, Smeringaiova I, Smorodinova N, Svobodova A, Strnad S, Jackson CJ, Burkert J, Jirsova K. Quantification of Analgesic and Anti-Inflammatory Lipid Mediators in Long-Term Cryopreserved and Freeze-Dried Preserved Human Amniotic Membrane. Bioengineering. 2023; 10(6):740. https://doi.org/10.3390/bioengineering10060740
Chicago/Turabian StyleVrkoslav, Vladimir, Ingrida Smeringaiova, Natalia Smorodinova, Alzbeta Svobodova, Stepan Strnad, Catherine Joan Jackson, Jan Burkert, and Katerina Jirsova. 2023. "Quantification of Analgesic and Anti-Inflammatory Lipid Mediators in Long-Term Cryopreserved and Freeze-Dried Preserved Human Amniotic Membrane" Bioengineering 10, no. 6: 740. https://doi.org/10.3390/bioengineering10060740
APA StyleVrkoslav, V., Smeringaiova, I., Smorodinova, N., Svobodova, A., Strnad, S., Jackson, C. J., Burkert, J., & Jirsova, K. (2023). Quantification of Analgesic and Anti-Inflammatory Lipid Mediators in Long-Term Cryopreserved and Freeze-Dried Preserved Human Amniotic Membrane. Bioengineering, 10(6), 740. https://doi.org/10.3390/bioengineering10060740