


The Use of Human Sterilized Crushed Tooth Particles Compared with BTCP Biomaterial and Empty Defects in Bone Formation inside Critical Rabbit Calvaria Sites


 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Materials
2.1.1. Animals
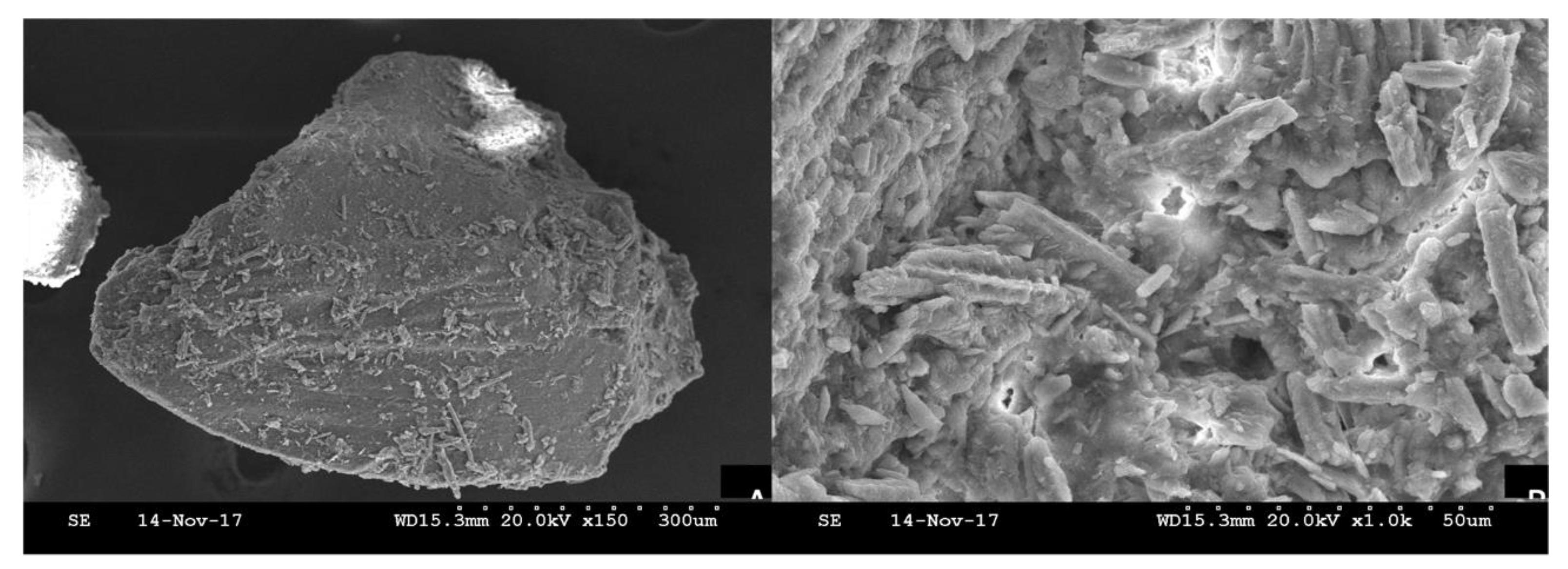
2.1.2. Biomaterials
2.1.3. Crushed Teeth
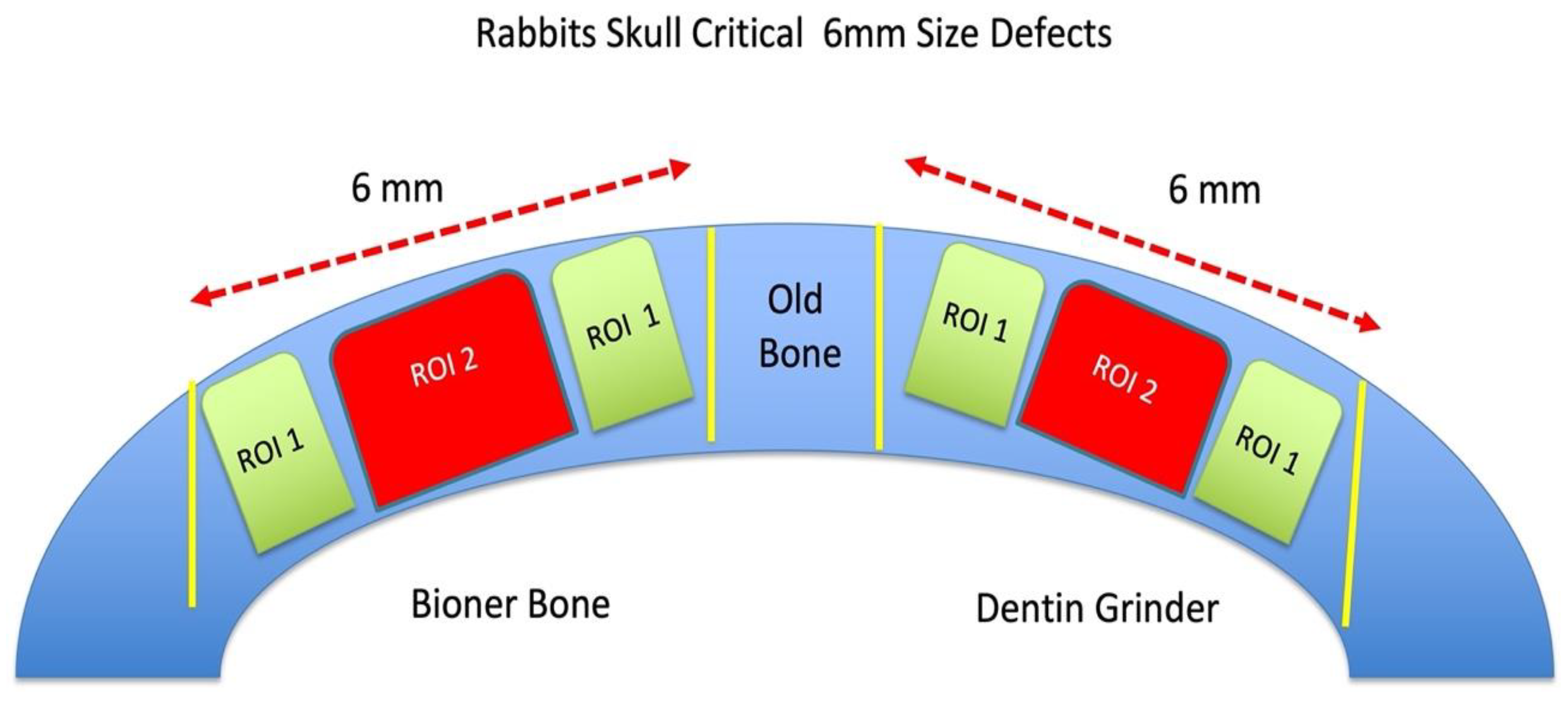
2.2. Study Design
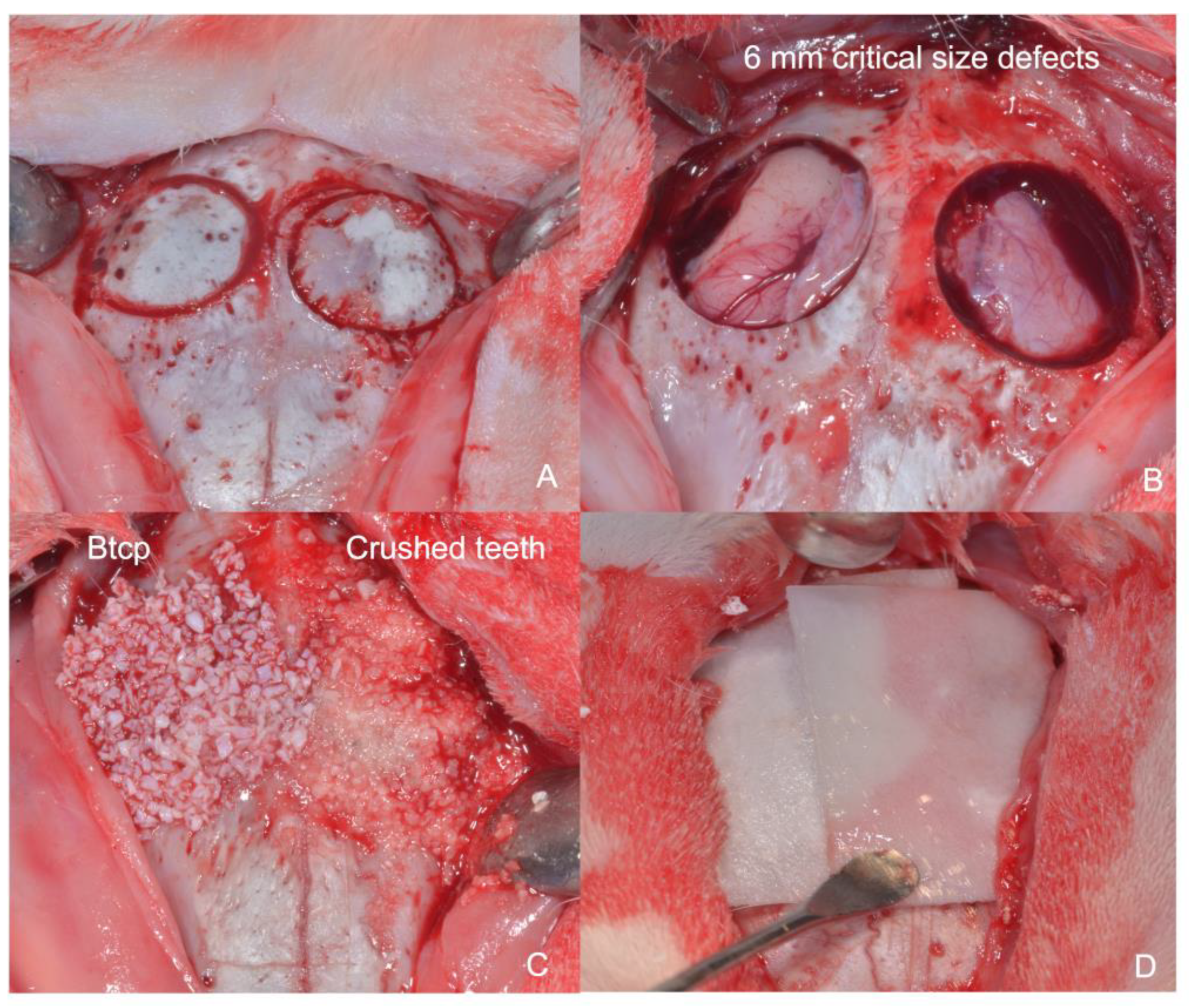
2.3. Surgical Procedure
2.4. Animal Sacrifice
2.5. Sample Processing
2.6. Histomorphometric Study
2.7. Statistical Analysis
3. Results
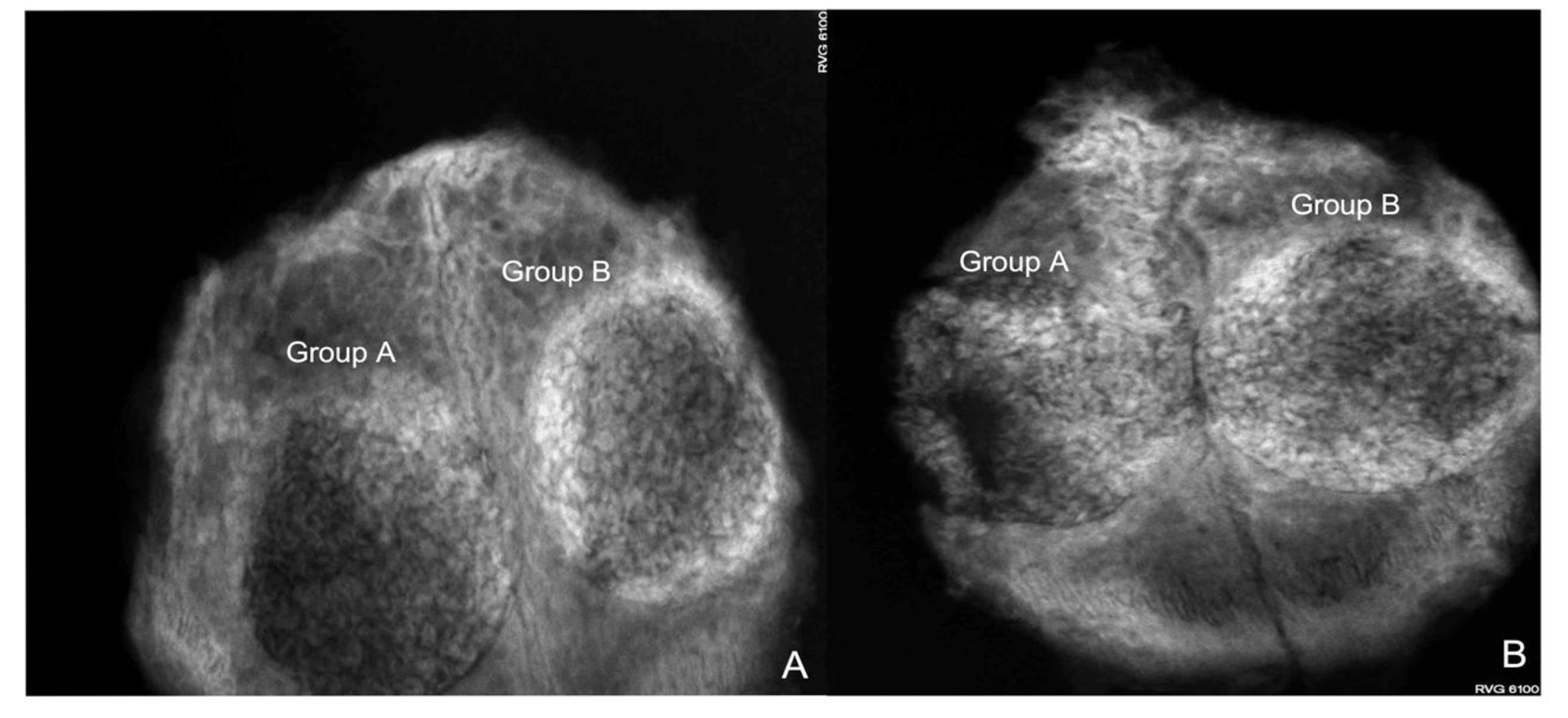
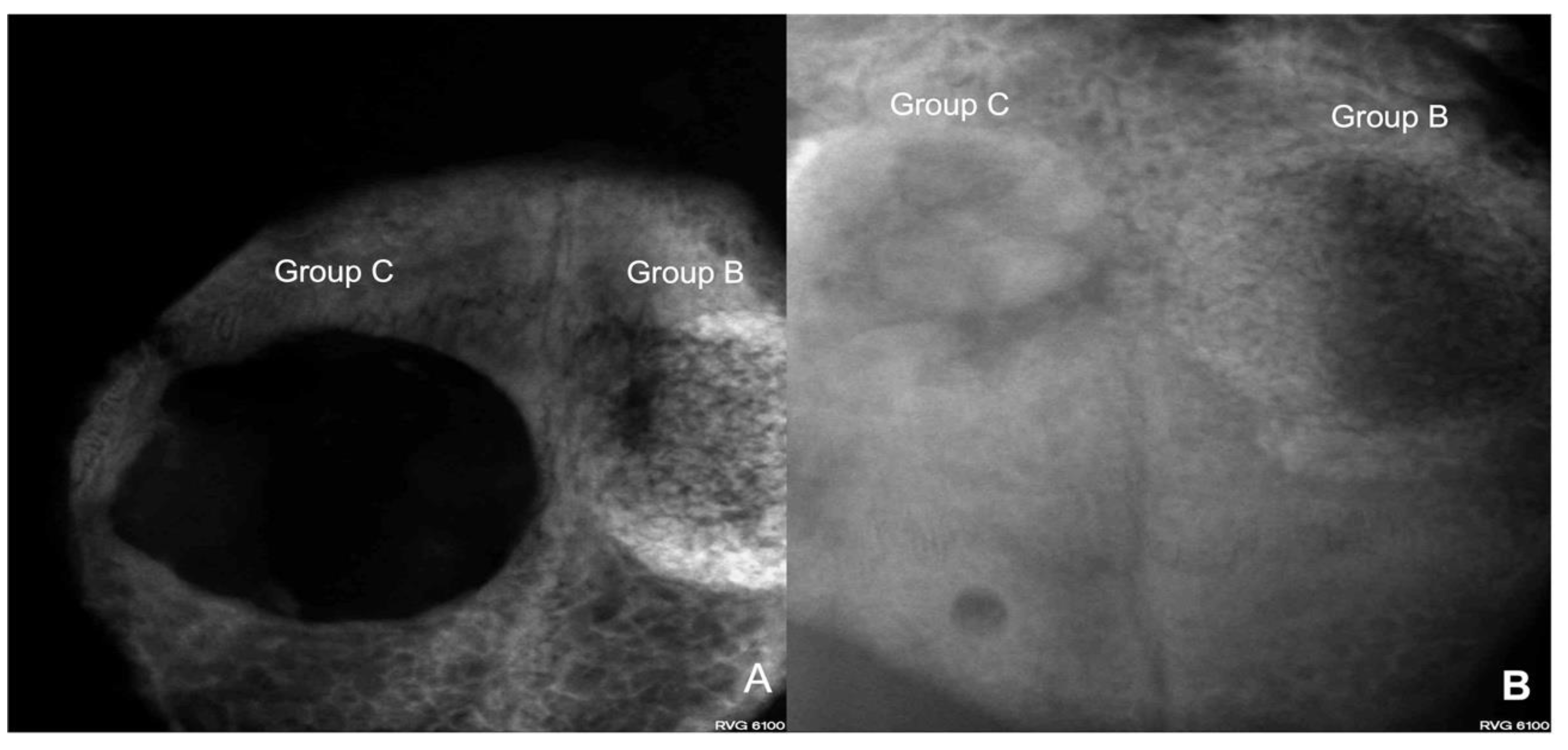
3.1. Radiovisiography
3.2. Histomorphometric Analysis
3.3. Histologic Evaluation
Four Weeks
3.4. Histomorphometric Study
3.4.1. Four Weeks
3.4.2. Eight Weeks
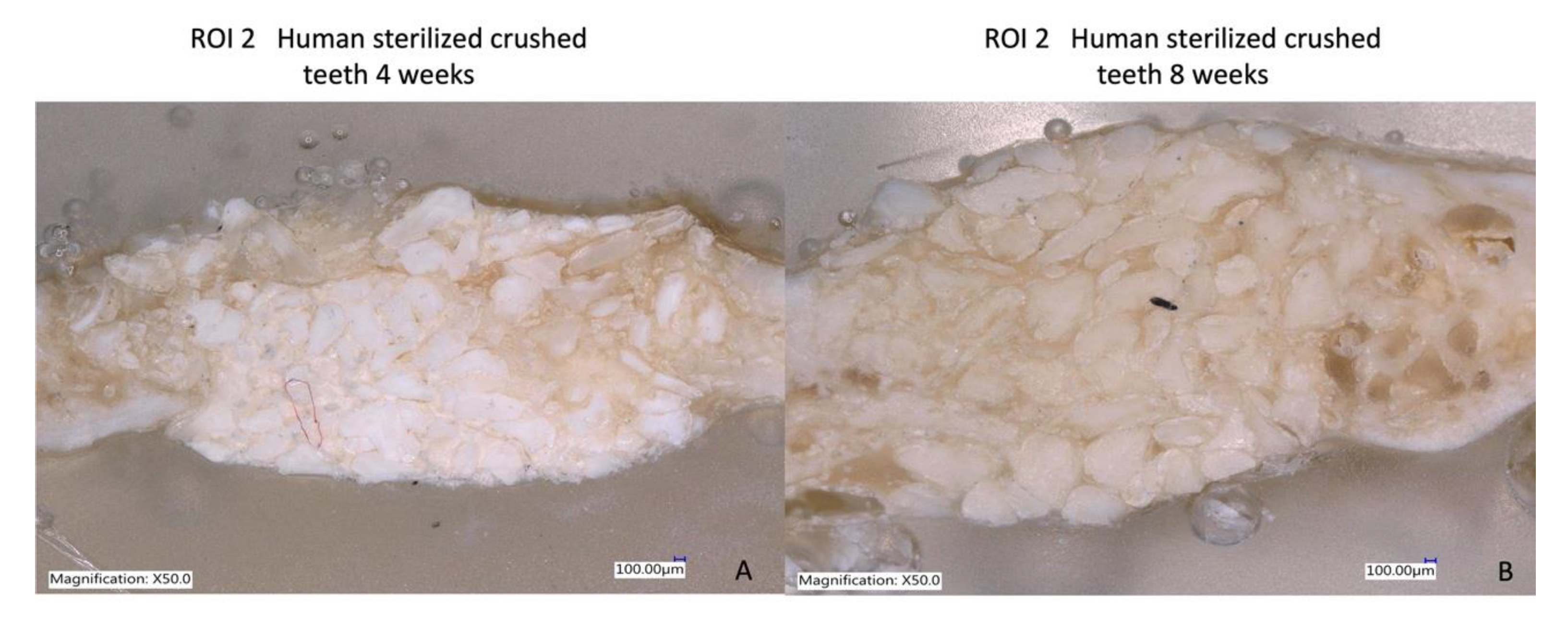
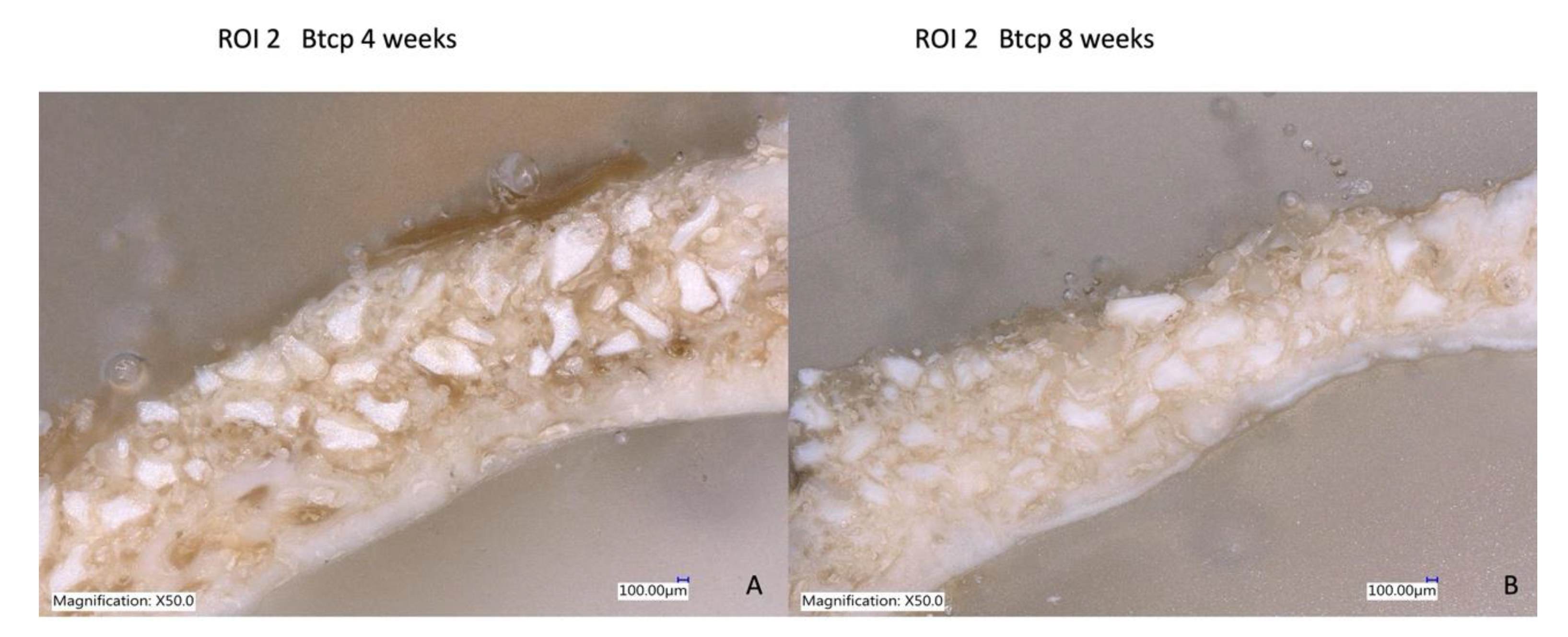
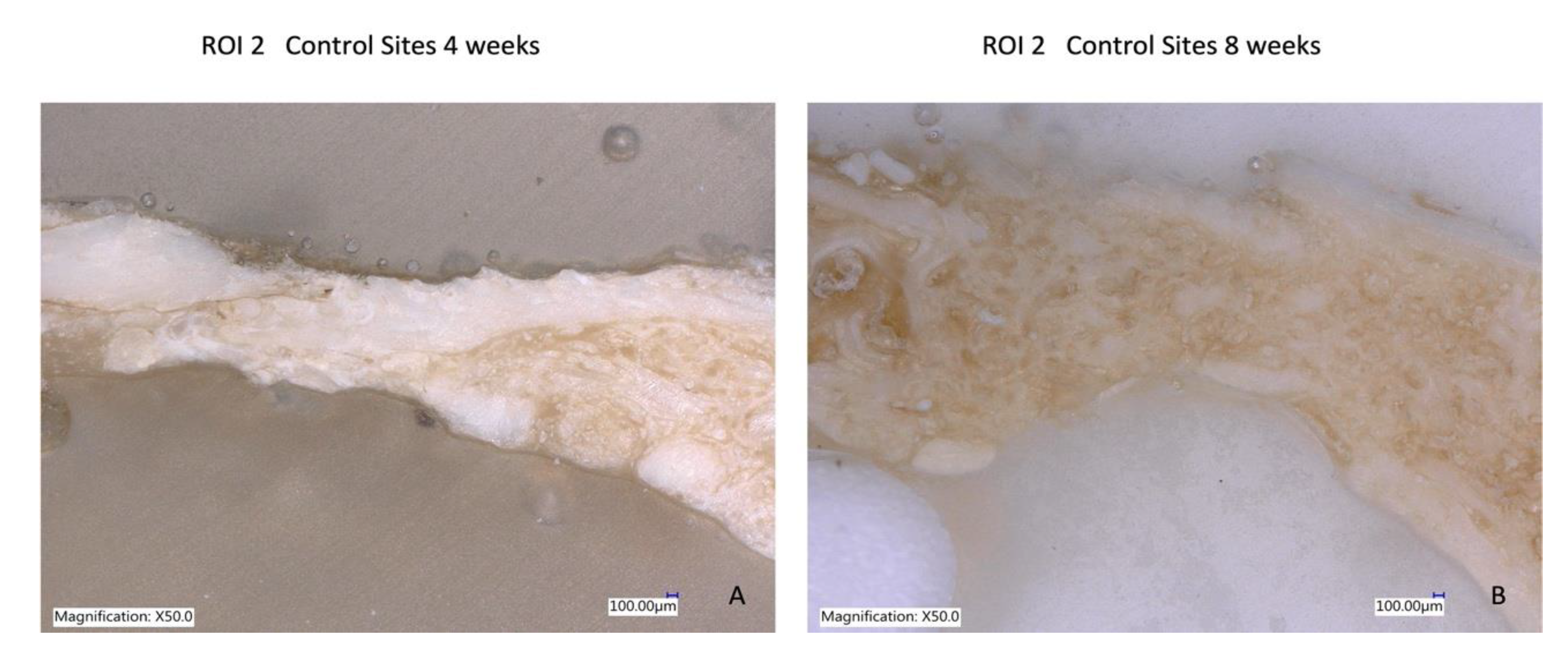
3.5. Laser Optical Microscopy
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Pelegrine, A.A.; da Costa, C.E.; Correa, M.E.; Marques, J.F., Jr. Clinical and histomorphometric evaluation of extraction sockets treated with an autologous bone marrow graft. Clin. Oral Implants Res. 2010, 21, 535–542. [Google Scholar] [CrossRef] [PubMed]
- Pelegrine, A.A.; Aloise, A.C.; Zimmermann, A.; de Mello e Oliveira, R.; Ferreira, L.M. Repair of critical-size bone defects using bone marrow stromal cells: A histomorphometric study in rabbit calvaria. Part I: Use of fresh bone marrow or bone marrow mononuclear fraction. Clin. Oral Implants Res. 2014, 25, 567–572. [Google Scholar] [CrossRef] [PubMed]
- Yaszemski, M.J.; Payne, R.G.; Hayes, W.C.; Langer, R.; Mikos, A.G. Evolution of bone transplantation: Molecular, cellular and tissue strategies to engineer human bone. Biomaterials 1996, 17, 175–185. [Google Scholar] [CrossRef] [PubMed]
- De Aza, P.N.; Luklinska, Z.B.; Mate-Sanchez de Val, J.E.; Calvo-Guirado, J.L. Biodegradation process of α-tricalcium phosphate and α-tricalcium phosphate solid solution bioceramics In Vivo: A comparative Study. Microsc. Microanal. 2013, 19, 1350–1357. [Google Scholar] [CrossRef]
- Gallo, P.; Díaz-Báez, D.; Perdomo, S.; Aloise, A.C.; Tattan, M.; Saleh, M.H.A.; Pelegrine, A.A.; Ravidà, A.; Wang, H.L. Comparative analysis of two biomaterials mixed with autogenous bone graft for vertical ridge augmentation: A histomorphometric study in humans. Clin. Implants Dent. Relat. Res. 2022, 24, 709–719. [Google Scholar] [CrossRef]
- Schlund, M.; Depeyre, A.; Kotagudda Ranganath, S.; Marchandise, P.; Ferri, J.; Chai, F. Rabbit calvarial and mandibular critical-sized bone defects as an experimental model for the evaluation of craniofacial bone tissue regeneration. J Stomatol Oral Maxillofac Surg. 2022, 123, 601–609. [Google Scholar] [CrossRef]
- Martinez, A.; Balboa, O.; Gasamans, I.; Otero-Cepeda, X.L.; Guitian, F. Deproteinated bovine bone vs. beta-tricalcium phosphate as bone graft substitutes: Histomorphometric longitudinal study in the rabbit cranial vault. Clin. Oral Implants Res. 2015, 26, 623–632. [Google Scholar] [CrossRef]
- Martínez, I.M.; Velásquez, P.; De Aza, P.N. Synthesis, and stability of alpha-Tricalcium Phosphate doped with Dicalcium silicate in the system Ca3(PO4)2-Ca2SiO4. Mater. Charact. 2010, 61, 761–767. [Google Scholar] [CrossRef]
- Calvo-Guirado, J.L.; Garces, M.; Delgado-Ruiz, R.A.; Ramirez Fernandez, M.P.; Ferres-Amat, E.; Romanos, G.E. Biphasic β-TCP mixed with silicon increases bone formation in critical site defects in rabbit calvaria. Clin. Oral Implants Res. 2015, 26, 891–897. [Google Scholar] [CrossRef]
- Al-Asfour, A.; Farzad, P.; Al-Musawi, A.; Dahlin, C.; Andersson, L. Demineralized Xenogenic Dentin and Autogenous Bone as Onlay Grafts to Rabbit Tibia. Implants Dent. 2017, 26, 232–237. [Google Scholar] [CrossRef]
- Minamizato, T.; Koga, T.; Takashi, I.; Nakatani, Y.; Umebayashi, M.; Sumita, Y.; Ikeda, T.; Asahina, I. Clinical application of autogenous partially demineralized dentin matrix prepared immediately after extraction for alveolar bone regeneration in implant dentistry: A pilot study. Int. J. Oral Maxillofac. Surg. 2018, 47, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Guirado, J.L.; Garcés-Villalá, M.A.; Mahesh, L.; De Carlos-Villafranca, F.A. Effectiveness of chemical disinfection in discarding pathogenic bacteria of human particulate tooth graft: An in vitro study. Indian J. Dent. Sci. 2021, 13, 277–282. [Google Scholar] [CrossRef]
- Calvo-Guirado, J.L. Temporary implants and particulate dentin graft protecting traditional implants in severe periodontal patient: A case report. Indian J. Dent. Sci. 2021, 13, 201–204. [Google Scholar]
- Calvo-Guirado, J.L.; Cegarra Del Pino, P.; Sapoznikov, L.; Delgado Ruiz, R.A.; Fernández-Domínguez, M.; Gehrke, S.A. A new procedure for processing extracted teeth for immediate grafting in post-extraction sockets. An experimental study in American Fox Hound dogs. Ann. Anat. 2018, 217, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Guirado, J.L.; Ballester Montilla, A.; De Aza, P.N.; Fernández-Domínguez, M.; Gehrke, S.A.; Cegarra-Del Pino, P.; Mahesh, L.; Pelegrine, A.A.; Aragoneses, J.M.; Maté-Sánchez de Val, J.E. Particulated, Extracted Human Teeth Characterization by SEM⁻EDX Evaluation as a Biomaterial for Socket Preservation: An in vitro Study. Materials 2019, 12, 380. [Google Scholar] [CrossRef]
- Cervera-Maillo, J.M.; Morales-Schwarz, D.; Morales-Melendez, H.; Mahesh, L.; Calvo-Guirado, J.L. Autologous Tooth Dentin Graft: A Retrospective Study in Humans. Medicina 2021, 58, 56. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Guirado, J.L.; Carlos-Villafranca, F.D.; Garcés-Villalá, M.A.; García-Carrillo, N.; Jindal, V.; Martínez-Martinez, F. How much-disinfected ground tooth do we need to fill an empty alveolus after extraction? Experimental in vitro study. Indian J. Dent. Sci. 2022, 14, 171–177. [Google Scholar] [CrossRef]
- Calvo-Guirado, J.L.; Carlos-Villafranca Fd Garcés-Villalá, M.; García-Carrillo, N.; Jindal, V.; Martínez-Martinez, F. X-ray micro-computed tomography characterization of autologous teeth particle used in postextraction sites for bone regeneration. An experimental study in dogs. Indian J. Dent. Sci. 2022, 14, 58–67. [Google Scholar] [CrossRef]
- Gharpure, A.S.; Bhatavadekar, N.B. Clinical Efficacy of Tooth-Bone Graft: A Systematic Review and Risk of Bias Analysis of Randomized Control Trials and Observational Studies. Implants Dent. 2018, 27, 119–134. [Google Scholar] [CrossRef] [PubMed]
- Slotte, C.; Lundgren, D.; Sennerby, L. Bone morphology and vascularization of untreated and guided bone augmentation-treated rabbit calvaria: Evaluation of an augmentation model. Clin. Oral Implants Res. 2005, 16, 228–235. [Google Scholar] [CrossRef]
- Schmitz, J.P.; Hollinger, J.O. The critical size defect as an experimental model for craniomandibulofacial nonunions. Clin. Orthop. Relat. Res. 1986, 205, 299–308. [Google Scholar] [CrossRef]
- Urist, M.R. Bone: Formation by autoinduction. Science 1965, 150, 893–899. [Google Scholar] [CrossRef] [PubMed]
- Urist, M.R.; Iwata, H.; Ceccotti, P.L.; Dorfman, R.L.; Boyd, S.D.; McDowell, R.M.; Chien, C. Bone morphogenesis in implants of insoluble bone gelatin. Proc. Nat. Acad. Sci. USA 1973, 70, 3511–3515. [Google Scholar] [CrossRef] [PubMed]
- Urist, M.R.; Mizutani, H.; Conover, M.A.; Lietze, A.; Finerman, G.A. Dentin, bone, and osteosarcoma tissue bone morphogenetic proteins. Prog. Clin. Biol. Res. 1982, 101, 61–81. [Google Scholar] [PubMed]
- Moharamzadeh, K.; Freeman, C.; Blackwood, K. Processed bovine dentine as a bone substitute. Br. J. Oral Maxillofac. Surg. 2008, 46, 110–113. [Google Scholar] [CrossRef] [PubMed]
- Hussain, I.; Moharamzadeh, K.; Brook, I.M.; José de Oliveira Neto, P.; Salata, L.A. Evaluation of osteoconductive and osteogenic potential of a dentin-based bone substitute using a calvarial defect model. Int. J. Dent. 2012, 2012, 396316. [Google Scholar] [CrossRef]
- Bono, N.; Tarsini, P.; Candiani, G. Demineralized dentin and enamel matrices as suitable substrates for bone regeneration. J. Appl. Biomater. Funct. Mater. 2017, 15, e236–e243. [Google Scholar] [CrossRef] [PubMed]
- Pohl, V.; Pohl, S.; Sulzbacher, I.; Fuerhauser, R.; Mailath-Pokorny, G.; Haas, R. Alveolar Ridge Augmentation Using Dystopic Autogenous Tooth: 2-Year Results of an Open Prospective Study. Int. J. Oral Maxillofac. Implants 2017, 32, 870–879. [Google Scholar] [CrossRef] [PubMed]
- Kabir, M.A.; Murata, M.; Akazawa, T.; Kusano, K.; Yamada, K.; Ito, M. Evaluation of perforated demineralized dentin scaffold on bone regeneration in critical-size sheep iliac defects. Clin. Oral Implants Res. 2017, 28, e227–e235. [Google Scholar] [CrossRef]
- Kamal, M.; Andersson, L.; Al-Asfour, A.; Bartella, A.K.; Gremse, F.; Rosenhain, S.; Gabato, S.; Hölzle, F.; Kessler, P.; Lethaus, B. Bone regeneration in rabbit calvarial critical-sized defects filled with composite in situ formed xenogenic dentin and biphasic tricalcium phosphate/hyroxyapatite mixture. J. Biomed. Mater. Res. Part B 2018, 107, 773–782. [Google Scholar] [CrossRef]
- Romanos, G.E.; Delgado-Ruiz, R.A.; Gómez-Moreno, G.; López-López, P.J.; Mate Sanchez de Val, J.E.; Calvo-Guirado, J.L. Role of mechanical compression on bone regeneration around a particulate bone graft material: An experimental study in rabbit calvaria. Clin. Oral Implants Res. 2018, 29, 612–619. [Google Scholar] [CrossRef] [PubMed]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| GROUPS | Cortical Defect Closure (C.D.C.) % | Residual Graft Material (R.G.M.) % | Connective Tissue (C.T.) % | |||
|---|---|---|---|---|---|---|
| R.O.I. 1 | R.O.I. 2 | R.O.I. 1 | R.O.I. 2 | R.O.I. 1 | R.O.I. 2 | |
| Group A | 10.9% ± 1.2% | 20.6% ± 0.18% | 45.7% ± 10.6% | 31.9% ± 0.2% | 43.4% ± 0.8% * | 47.6% ± 1.1% * |
| Group B | 26.9% ± 0.6% * | 51.4% ± 0.7% * | 53.7% ± 1.3% | 36.8% ± 0.5% | 19.4% ± 1.2% | 11.8% ± 0.7% |
| Group C | 0.8% ± 1.1% | 11.2% ± 0.2% | 0.0% ± 0.0% | 0.0% ± 0.0% | 99.2% ± 0.3% | 88.8% ± 0.7% |
| GROUPS | Cortical Defect Closure (C.D.C.) % | Residual Graft Material (R.G.M.) % | Connective Tissue (C.T.) % | |||
|---|---|---|---|---|---|---|
| R.O.I. 1 | R.O.I. 2 | R.O.I. 1 | R.O.I. 2 | R.O.I. 1 | R.O.I. 2 | |
| Group A | 27.6% ± 0.2% | 38.2% ± 0.11% | 21.3% ± 1.7% | 15.6% ± 0.2% | 51.1% ± 0.3% * | 46.2% ± 1.6% * |
| Group B | 31.5% ± 0.4% * | 61.3% ± 1.6% * | 41.8% ± 1.5% | 21.9% ± 1.5% | 26.7% ± 1.4% | 16.8% ± 1.9% |
| Group C | 11.2% ± 0.3% | 18.3% ± 0.17% | 0.0% ± 0.0% | 0.0% ± 0.0% | 88.8% ± 1.2% | 81.7% ± 0.7% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calvo-Guirado, J.L.; Cabo-Pastor, M.B.; Martínez-Martínez, F.; Garcés-Villalá, M.Á.; de Carlos-Villafranca, F.; García-Carrillo, N.; Fernández-Domínguez, M. The Use of Human Sterilized Crushed Tooth Particles Compared with BTCP Biomaterial and Empty Defects in Bone Formation inside Critical Rabbit Calvaria Sites. Bioengineering 2023, 10, 638. https://doi.org/10.3390/bioengineering10060638
Calvo-Guirado JL, Cabo-Pastor MB, Martínez-Martínez F, Garcés-Villalá MÁ, de Carlos-Villafranca F, García-Carrillo N, Fernández-Domínguez M. The Use of Human Sterilized Crushed Tooth Particles Compared with BTCP Biomaterial and Empty Defects in Bone Formation inside Critical Rabbit Calvaria Sites. Bioengineering. 2023; 10(6):638. https://doi.org/10.3390/bioengineering10060638
Chicago/Turabian StyleCalvo-Guirado, José Luis, Marta Belén Cabo-Pastor, Francisco Martínez-Martínez, Miguel Ángel Garcés-Villalá, Félix de Carlos-Villafranca, Nuria García-Carrillo, and Manuel Fernández-Domínguez. 2023. "The Use of Human Sterilized Crushed Tooth Particles Compared with BTCP Biomaterial and Empty Defects in Bone Formation inside Critical Rabbit Calvaria Sites" Bioengineering 10, no. 6: 638. https://doi.org/10.3390/bioengineering10060638
APA StyleCalvo-Guirado, J. L., Cabo-Pastor, M. B., Martínez-Martínez, F., Garcés-Villalá, M. Á., de Carlos-Villafranca, F., García-Carrillo, N., & Fernández-Domínguez, M. (2023). The Use of Human Sterilized Crushed Tooth Particles Compared with BTCP Biomaterial and Empty Defects in Bone Formation inside Critical Rabbit Calvaria Sites. Bioengineering, 10(6), 638. https://doi.org/10.3390/bioengineering10060638