



Recent Advances in Apical Periodontitis Treatment: A Narrative Review

 ,
,  ,
,  ,
,
Abstract
1. Introduction
Current Challenges in the Diagnosis and Treatment of Apical Periodontitis
2. Contemporary Therapies
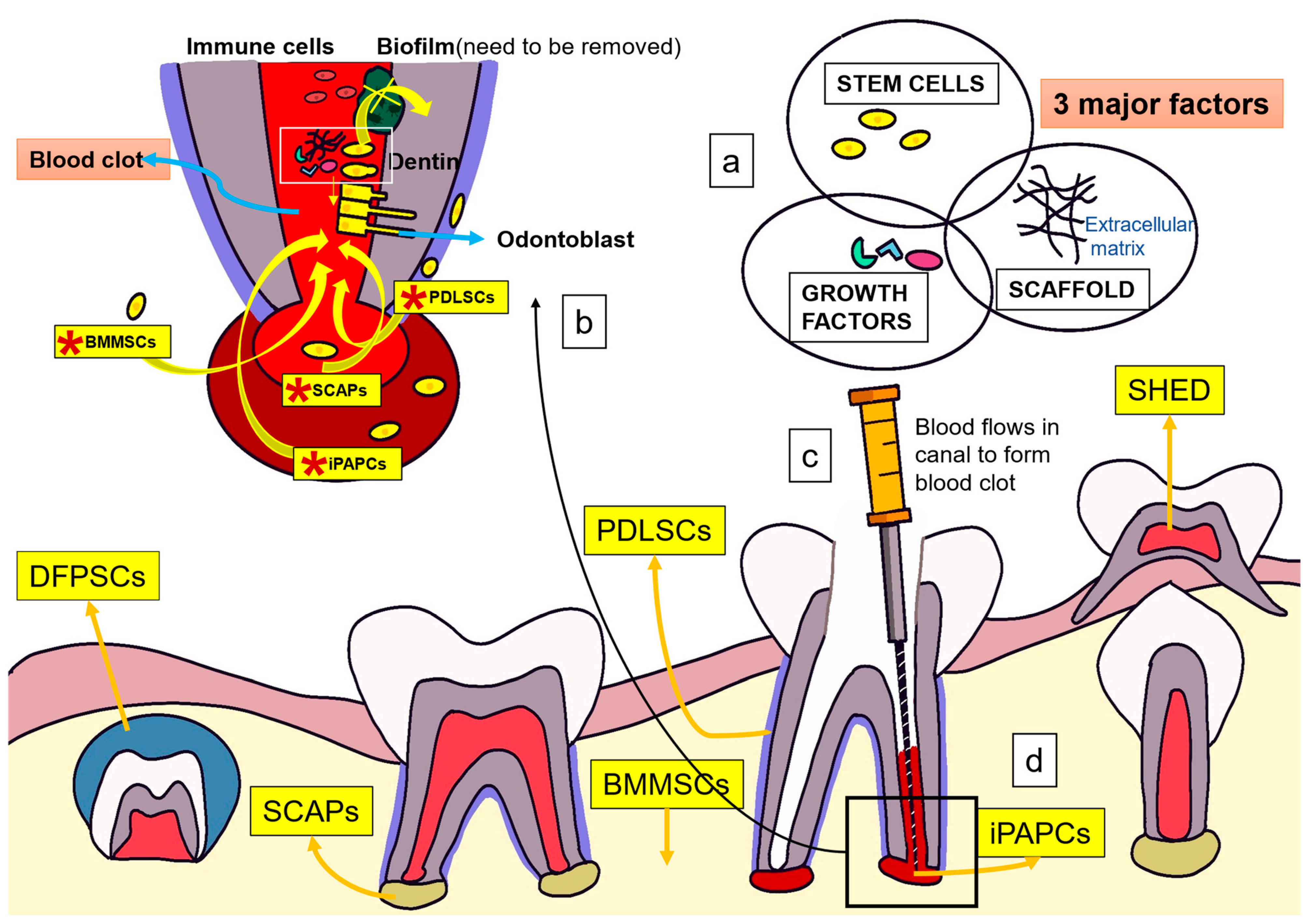
2.1. Regenerative Endodontics and Apical Periodontitis
Mechanism of Action of Tissue Engineering for the Treatment of Apical Periodontitis
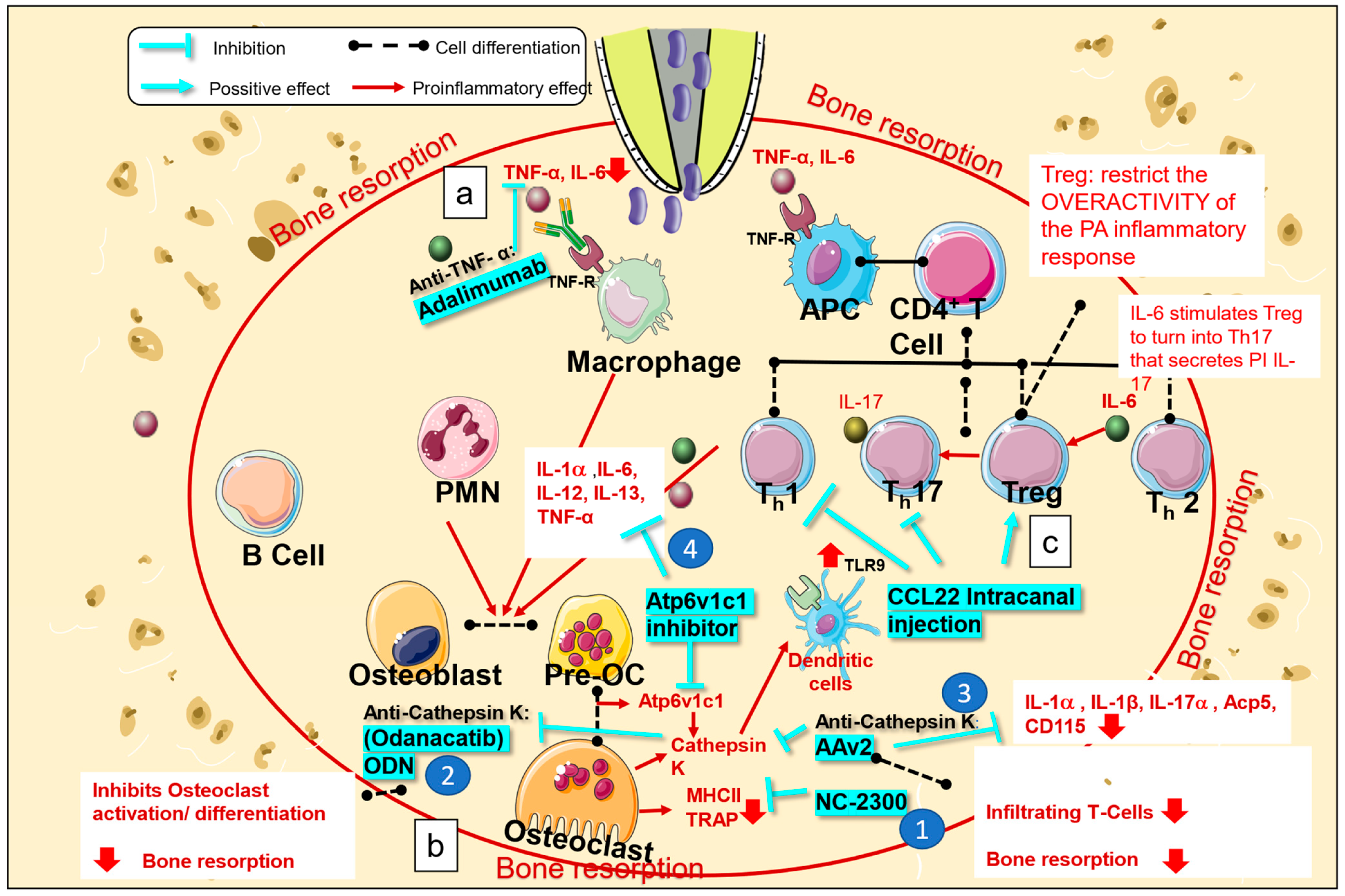
2.2. Biologic Medications for the Treatment of Apical Periodontitis
2.2.1. Mechanism of Action of Biological Medications for the Treatment of Apical Periodontitis
2.2.2. TNF-α Inhibitors
2.2.3. Treg Therapy
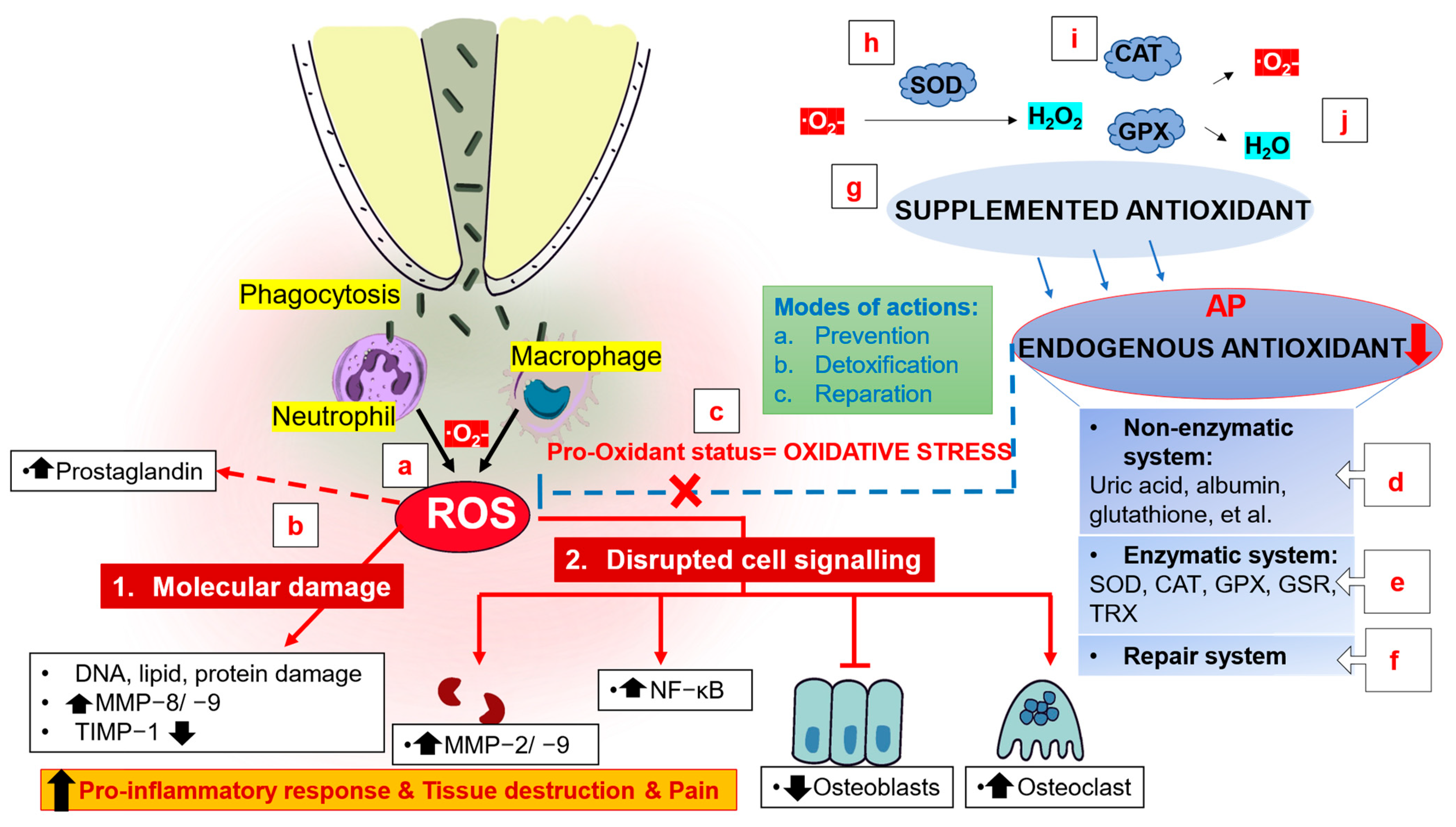
2.3. Antioxidants for the Treatment of Apical Periodontitis
2.3.1. Mechanism of Action of Antioxidants for the Treatment of Apical Periodontitis
2.3.2. NLRP3 Inflammasome Inhibitor
2.3.3. Alpha-Lipoic Acid
2.3.4. Selenium
2.4. Probiotics for the Treatment of Apical Periodontitis
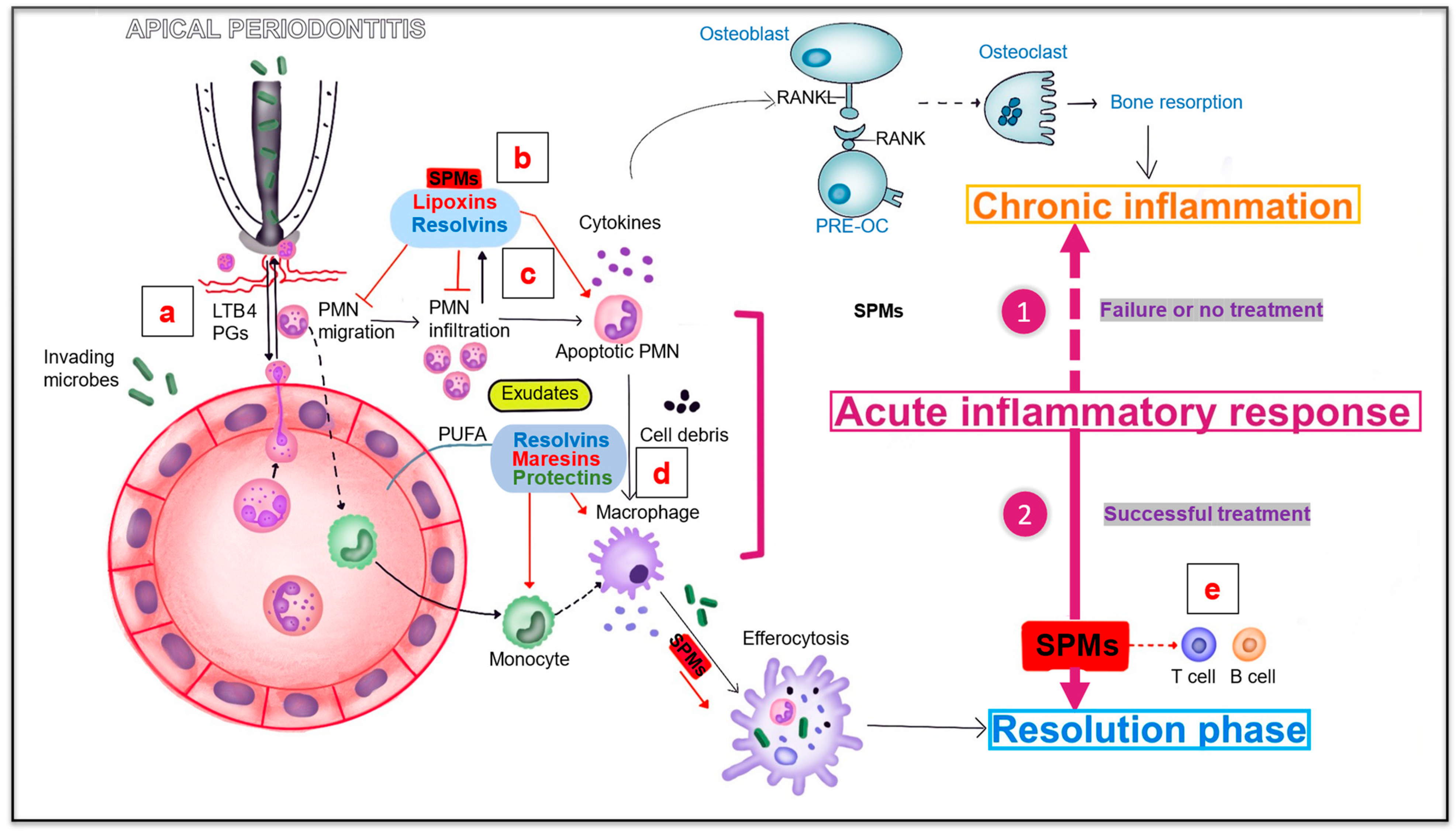
2.5. Specialized Proresolving Lipid Mediators (SPMs) and Apical Periodontitis
2.5.1. Mechanism of Action of SPMs for the Treatment of Apical Periodontitis
2.5.2. Resolvins and Apical Periodontitis
2.5.3. Omega 3 Fatty Acids and Apical Periodontitis
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tibúrcio-Machado, C.S.; Michelon, C.; Zanatta, F.B.; Gomes, M.S.; Marin, J.A.; Bier, C.A. The global prevalence of apical periodontitis: A systematic review and meta-analysis. Int. Endod. J. 2021, 54, 712–735. [Google Scholar] [CrossRef] [PubMed]
- Pereira, B.; Martins, J.N.R.; Baruwa, A.O.; Meirinhos, J.; Gouveia, J.; Quaresma, S.A.; Monroe, A.; Ginjeira, A. Association between Endodontically Treated Maxillary and Mandibular Molars with Fused Roots and Periapical Lesions: A Cone-beam Computed Tomography Cross-sectional Study. J. Endod. 2020, 46, 771–777.e771. [Google Scholar] [CrossRef] [PubMed]
- Meirinhos, J.; Martins, J.N.R.; Pereira, B.; Baruwa, A.; Gouveia, J.; Quaresma, S.A.; Monroe, A.; Ginjeira, A. Prevalence of apical periodontitis and its association with previous root canal treatment, root canal filling length and type of coronal restoration—A cross-sectional study. Int. Endod. J. 2020, 53, 573–584. [Google Scholar] [CrossRef] [PubMed]
- Jakovljevic, A.; Nikolic, N.; Jacimovic, J.; Pavlovic, O.; Milicic, B.; Beljic-Ivanovic, K.; Miletic, M.; Andric, M.; Milasin, J. Prevalence of Apical Periodontitis and Conventional Nonsurgical Root Canal Treatment in General Adult Population: An Updated Systematic Review and Meta-analysis of Cross-sectional Studies Published between 2012 and 2020. J. Endod. 2020, 46, 1371–1386.e1378. [Google Scholar] [CrossRef] [PubMed]
- Braz-Silva, P.H.; Bergamini, M.L.; Mardegan, A.P.; De Rosa, C.S.; Hasseus, B.; Jonasson, P. Inflammatory profile of chronic apical periodontitis: A literature review. Acta Odontol. Scand. 2019, 77, 173–180. [Google Scholar] [CrossRef]
- Nair, P.N. Pathogenesis of apical periodontitis and the causes of endodontic failures. Crit. Rev. Oral. Biol. Med. 2004, 15, 348–381. [Google Scholar] [CrossRef]
- Ng, Y.L.; Mann, V.; Rahbaran, S.; Lewsey, J.; Gulabivala, K. Outcome of primary root canal treatment: Systematic review of the literature—Part 1. Effects of study characteristics on probability of success. Int. Endod. J. 2007, 40, 921–939. [Google Scholar] [CrossRef]
- Galler, K.M.; Weber, M.; Korkmaz, Y.; Widbiller, M.; Feuerer, M. Inflammatory Response Mechanisms of the Dentine-Pulp Complex and the Periapical Tissues. Int. J. Mol. Sci. 2021, 22, 1480. [Google Scholar] [CrossRef]
- Karamifar, K.; Tondari, A.; Saghiri, M.A. Endodontic Periapical Lesion: An Overview on the Etiology, Diagnosis and Current Treatment Modalities. Eur. Endod. J. 2020, 5, 54–67. [Google Scholar] [CrossRef]
- Geibel, M.A.; Schreiber, E.; Bracher, A.K.; Hell, E.; Ulrici, J.; Sailer, L.K.; Rasche, V. Characterisation of apical bone lesions: Comparison of MRI and CBCT with histological findings—A case series. Eur. J. Oral. Implantol. 2017, 10, 197–211. [Google Scholar]
- Siqueira Junior, J.F.; Rôças, I.D.N.; Marceliano-Alves, M.F.; Pérez, A.R.; Ricucci, D. Unprepared root canal surface areas: Causes, clinical implications, and therapeutic strategies. Braz. Oral. Res. 2018, 32, e65. [Google Scholar] [CrossRef]
- Distel, J.W.; Hatton, J.F.; Gillespie, M.J. Biofilm formation in medicated root canals. J. Endod. 2002, 28, 689–693. [Google Scholar] [CrossRef]
- Deng, Z.; Lin, B.; Liu, F.; Zhao, W. Role of Enterococcus faecalis in refractory apical periodontitis: From pathogenicity to host cell response. J. Oral. Microbiol. 2023, 15, 2184924. [Google Scholar] [CrossRef]
- Haapasalo, M.; Shen, Y.; Wang, Z.; Gao, Y. Irrigation in endodontics. Br. Dent. J. 2014, 216, 299–303. [Google Scholar] [CrossRef]
- Boutsioukis, C.; Arias-Moliz, M.T. Present status and future directions-irrigants and irrigation methods. Int. Endod. J. 2022, 55 (Suppl. 3), 588–612. [Google Scholar] [CrossRef]
- Ng, Y.L.; Mann, V.; Rahbaran, S.; Lewsey, J.; Gulabivala, K. Outcome of primary root canal treatment: Systematic review of the literature—Part 2. Influence of clinical factors. Int. Endod. J. 2008, 41, 6–31. [Google Scholar] [CrossRef]
- Kim, S.G. Infection and Pulp Regeneration. Dent. J. 2016, 4, 4. [Google Scholar] [CrossRef]
- Aurora, A.B.; Olson, E.N. Immune modulation of stem cells and regeneration. Cell. Stem Cell. 2014, 15, 14–25. [Google Scholar] [CrossRef]
- Fouad, A.F. Microbial Factors and Antimicrobial Strategies in Dental Pulp Regeneration. J. Endod. 2017, 43, S46–S50. [Google Scholar] [CrossRef]
- Cooper, P.R.; McLachlan, J.L.; Simon, S.; Graham, L.W.; Smith, A.J. Mediators of inflammation and regeneration. Adv. Dent. Res. 2011, 23, 290–295. [Google Scholar] [CrossRef]
- Pulyodan, M.K.; Paramel Mohan, S.; Valsan, D.; Divakar, N.; Moyin, S.; Thayyil, S. Regenerative Endodontics: A Paradigm Shift in Clinical Endodontics. J. Pharm. Bioallied Sci. 2020, 12, S20–S26. [Google Scholar] [CrossRef] [PubMed]
- Mao, J.J.; Kim, S.G.; Zhou, J.; Ye, L.; Cho, S.; Suzuki, T.; Fu, S.Y.; Yang, R.; Zhou, X. Regenerative endodontics: Barriers and strategies for clinical translation. Dent. Clin. N. Am. 2012, 56, 639–649. [Google Scholar] [CrossRef] [PubMed]
- Kolios, G.; Moodley, Y. Introduction to stem cells and regenerative medicine. Respiration 2013, 85, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Hameed, M.H.; Gul, M.; Ghafoor, R.; Badar, S.B. Management of immature necrotic permanent teeth with regenerative endodontic procedures—A review of literature. J. Pak. Med. Assoc. 2019, 69, 1514–1520. [Google Scholar] [CrossRef]
- Roberts-Clark, D.J.; Smith, A.J. Angiogenic growth factors in human dentine matrix. Arch. Oral. Biol. 2000, 45, 1013–1016. [Google Scholar] [CrossRef]
- Friedlander, L.T.; Coates, D.; Seymour, G.; Cullinan, M.; Rich, A.M. Vascularity and VEGF/VEGFR2 Signaling in the Dentine-Pulp Complex of Immature and Mature Permanent Teeth. Eur. Endod. J. 2018, 3, 153–159. [Google Scholar] [CrossRef]
- Angelopoulos, I.; Trigo, C.; Ortuzar, M.I.; Cuenca, J.; Brizuela, C.; Khoury, M. Delivery of affordable and scalable encapsulated allogenic/autologous mesenchymal stem cells in coagulated platelet poor plasma for dental pulp regeneration. Sci. Rep. 2022, 12, 435. [Google Scholar] [CrossRef]
- Altaii, M.; Kaidonis, X.; Koblar, S.; Cathro, P.; Richards, L. Platelet rich plasma and dentine effect on sheep dental pulp cells regeneration/revitalization ability (in vitro). Aust. Dent. J. 2017, 62, 39–46. [Google Scholar] [CrossRef]
- Lee, U.L.; Jeon, S.H.; Park, J.Y.; Choung, P.H. Effect of platelet-rich plasma on dental stem cells derived from human impacted third molars. Regen. Med. 2011, 6, 67–79. [Google Scholar] [CrossRef]
- Fang, Y.; Wang, X.; Zhu, J.; Su, C.; Yang, Y.; Meng, L. Influence of Apical Diameter on the Outcome of Regenerative Endodontic Treatment in Teeth with Pulp Necrosis: A Review. J. Endod. 2018, 44, 414–431. [Google Scholar] [CrossRef]
- Lenzi, R.; Hernández, S.R.; Alves, F.R.F.; Rôças, I.N.; Siqueira, J.F. Regenerative Endodontic Therapy for Management of an Immature Permanent Tooth with Recurrent Post-treatment Apical Periodontitis: A Case Report. J. Int. Soc. Prev. Community Dent. 2022, 12, 468–473. [Google Scholar] [CrossRef]
- Cotti, E.; Mereu, M.; Lusso, D. Regenerative treatment of an immature, traumatized tooth with apical periodontitis: Report of a case. J. Endod. 2008, 34, 611–616. [Google Scholar] [CrossRef]
- Kumar, J.K.; Surendranath, P.; Eswaramoorthy, R. Regeneration of immature incisor using platelet rich fibrin: Report of a novel clinical application. BMC Oral. Health 2023, 23, 69. [Google Scholar] [CrossRef]
- Cordero, C.B.; Santander, G.M.; González, D.U.; Quezada, A.; Silva, C.I.; Vásquez, C.; Jara, R.; Jara, D.; Khoury, M. Allogeneic Cellular Therapy in a Mature Tooth with Apical Periodontitis and Accidental Root Perforation: A Case Report. J. Endod. 2020, 46, 1920–1927.e1921. [Google Scholar] [CrossRef]
- Marending, M.; Peters, O.A.; Zehnder, M. Factors affecting the outcome of orthograde root canal therapy in a general dentistry hospital practice. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2005, 99, 119–124. [Google Scholar] [CrossRef]
- Wang, S.; Wang, X.; Bai, F.; Shi, X.; Zhou, T.; Li, F. Effect of endodontic treatment on clinical outcome in type 2 diabetic patients with apical periodontitis. Heliyon 2023, 9, e13914. [Google Scholar] [CrossRef]
- Dill, A.; Letra, A.; Chaves de Souza, L.; Yadlapati, M.; Biguetti, C.C.; Garlet, G.P.; Vieira, A.R.; Silva, R.M. Analysis of multiple cytokine polymorphisms in individuals with untreated deep carious lesions reveals IL1B (rs1143643) as a susceptibility factor for periapical lesion development. J. Endod. 2015, 41, 197–200. [Google Scholar] [CrossRef]
- Petean, I.B.F.; Küchler, E.C.; Soares, I.M.V.; Segato, R.A.B.; Silva, L.A.B.D.; Antunes, L.A.A.; Salles, A.G.; Antunes, L.S.; Sousa-Neto, M.D. Genetic Polymorphisms in RANK and RANKL are Associated with Persistent Apical Periodontitis. J. Endod. 2019, 45, 526–531. [Google Scholar] [CrossRef]
- Xiao, T.S. Innate immunity and inflammation. Cell. Mol. Immunol. 2017, 14, 1–3. [Google Scholar] [CrossRef]
- Radu, A.F.; Bungau, S.G. Management of Rheumatoid Arthritis: An Overview. Cells 2021, 10, 2857. [Google Scholar] [CrossRef]
- O’Neill, I.D.; Scully, C. Biologics in oral medicine: Principles of use and practical considerations. Oral Dis. 2012, 18, 525–536. [Google Scholar] [CrossRef] [PubMed]
- Pan, W.; Wang, Q.; Chen, Q. The cytokine network involved in the host immune response to periodontitis. Int. J. Oral Sci. 2019, 11, 30. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Guo, J.; Jia, R. Treg: A Promising Immunotherapeutic Target in Oral Diseases. Front. Immunol. 2021, 12, 667862. [Google Scholar] [CrossRef] [PubMed]
- Longo, D.; Fauci, A.; Kasper, D.; Hauser, S.; Jameson, J.; Loscalzo, J. Harrison’s Principles of Internal Medicine, 18th ed.; McGraw-Hill Professional: New York, NY, USA, 2012. [Google Scholar]
- Georgakopoulou, E.; Scully, C. Biological agents: What they are, how they affect oral health and how they can modulate oral healthcare. Br. Dent. J. 2015, 218, 671–677. [Google Scholar] [CrossRef]
- De Smit, M.J.; Westra, J.; Posthumus, M.D.; Springer, G.; van Winkelhoff, A.J.; Vissink, A.; Brouwer, E.; Bijl, M. Effect of Anti-Rheumatic Treatment on the Periodontal Condition of Rheumatoid Arthritis Patients. Int. J. Environ. Res. Public. Health 2021, 18, 2529. [Google Scholar] [CrossRef]
- Delima, A.J.; Oates, T.; Assuma, R.; Schwartz, Z.; Cochran, D.; Amar, S.; Graves, D.T. Soluble antagonists to interleukin-1 (IL-1) and tumor necrosis factor (TNF) inhibits loss of tissue attachment in experimental periodontitis. J. Clin. Periodontol. 2001, 28, 233–240. [Google Scholar] [CrossRef]
- Cotti, E.; Abramovitch, K.; Jensen, J.; Schirru, E.; Rice, D.D.; Oyoyo, U.; Torabinejad, M. The Influence of Adalimumab on the Healing of Apical Periodontitis in Ferrets. J. Endod. 2017, 43, 1841–1846. [Google Scholar] [CrossRef]
- Asagiri, M.; Hirai, T.; Kunigami, T.; Kamano, S.; Gober, H.J.; Okamoto, K.; Nishikawa, K.; Latz, E.; Golenbock, D.T.; Aoki, K.; et al. Cathepsin K-dependent toll-like receptor 9 signaling revealed in experimental arthritis. Science 2008, 319, 624–627. [Google Scholar] [CrossRef]
- Latz, E.; Schoenemeyer, A.; Visintin, A.; Fitzgerald, K.A.; Monks, B.G.; Knetter, C.F.; Lien, E.; Nilsen, N.J.; Espevik, T.; Golenbock, D.T. TLR9 signals after translocating from the ER to CpG DNA in the lysosome. Nat. Immunol. 2004, 5, 190–198. [Google Scholar] [CrossRef]
- Suzuki, N.; Takimoto, K.; Kawashima, N. Cathepsin K Inhibitor Regulates Inflammation and Bone Destruction in Experimentally Induced Rat Periapical Lesions. J. Endod. 2015, 41, 1474–1479. [Google Scholar] [CrossRef]
- Hao, L.; Chen, W.; McConnell, M.; Zhu, Z.; Li, S.; Reddy, M.; Eleazer, P.D.; Wang, M.; Li, Y.P. A small molecule, odanacatib, inhibits inflammation and bone loss caused by endodontic disease. Infect. Immun. 2015, 83, 1235–1245. [Google Scholar] [CrossRef]
- Gao, B.; Chen, W.; Hao, L.; Zhu, G.; Feng, S.; Ci, H.; Zhou, X.; Stashenko, P.; Li, Y.P. Inhibiting periapical lesions through AAV-RNAi silencing of cathepsin K. J. Dent. Res. 2013, 92, 180–186. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, W.; Hao, L.; McVicar, A.; Wu, J.; Gao, N.; Liu, Y.; Li, Y.P. C1 Silencing Attenuates Inflammation and Alveolar Bone Resorption in Endodontic Disease. J. Endod. 2019, 45, 898–906. [Google Scholar] [CrossRef]
- Liu, X.M.; Liu, Y.; Yu, S.; Jiang, L.M.; Song, B.; Chen, X. Potential immunomodulatory effects of stem cells from the apical papilla on Treg conversion in tissue regeneration for regenerative endodontic treatment. Int. Endod. J. 2019, 52, 1758–1767. [Google Scholar] [CrossRef]
- Francisconi, C.F.; Vieira, A.E.; Biguetti, C.C.; Glowacki, A.J.; Trombone, A.P.; Letra, A.; Menezes Silva, R.; Sfeir, C.S.; Little, S.R.; Garlet, G.P. Characterization of the Protective Role of Regulatory T Cells in Experimental Periapical Lesion Development and Their Chemoattraction Manipulation as a Therapeutic Tool. J. Endod. 2016, 42, 120–126. [Google Scholar] [CrossRef]
- Suzen, S.; Gurer-Orhan, H.; Saso, L. Detection of Reactive Oxygen and Nitrogen Species by Electron Paramagnetic Resonance (EPR) Technique. Molecules 2017, 22, 181. [Google Scholar] [CrossRef]
- Barcelos, R.C.S.; Rosa, H.Z.; Roversi, K.; Tibúrcio-Machado, C.D.S.; Inchaki, P.T.; Burger, M.E.; Bier, C.A.S. Apical periodontitis induces changes on oxidative stress parameters and increases Na+/K+-ATPase activity in adult rats. Arch. Oral Biol. 2020, 118, 104849. [Google Scholar] [CrossRef]
- Georgiou, A.C.; Cornejo Ulloa, P.; Van Kessel, G.M.H.; Crielaard, W.; Van der Waal, S.V. Reactive oxygen species can be traced locally and systemically in apical periodontitis: A systematic review. Arch. Oral Biol. 2021, 129, 105167. [Google Scholar] [CrossRef]
- Hernández-Ríos, P.; Pussinen, P.J.; Vernal, R.; Hernández, M. Oxidative Stress in the Local and Systemic Events of Apical Periodontitis. Front. Physiol. 2017, 8, 869. [Google Scholar] [CrossRef]
- Vo, T.T.T.; Chu, P.M.; Tuan, V.P.; Te, J.S.; Lee, I.T. The Promising Role of Antioxidant Phytochemicals in the Prevention and Treatment of Periodontal Disease via the Inhibition of Oxidative Stress Pathways: Updated Insights. Antioxidants 2020, 9, 1211. [Google Scholar] [CrossRef]
- Wang, L.; Jin, H.; Ye, D.; Wang, J.; Ao, X.; Dong, M.; Niu, W. Enterococcus faecalis Lipoteichoic Acid-induced NLRP3 Inflammasome via the Activation of the Nuclear Factor Kappa B Pathway. J. Endod. 2016, 42, 1093–1100. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Zheng, Y.; Jin, S.; Fu, Y.; Liu, Y. Dioscin Protects against Cisplatin-Induced Acute Kidney Injury by Reducing Ferroptosis and Apoptosis through Activating Nrf2/HO-1 Signaling. Antioxidants 2022, 11, 2443. [Google Scholar] [CrossRef] [PubMed]
- Yin, W.; Liu, S.; Dong, M.; Liu, Q.; Shi, C.; Bai, H.; Wang, Q.; Yang, X.; Niu, W.; Wang, L. A New NLRP3 Inflammasome Inhibitor, Dioscin, Promotes Osteogenesis. Small 2020, 16, e1905977. [Google Scholar] [CrossRef] [PubMed]
- Odabasoglu, F.; Halici, Z.; Aygun, H.; Halici, M.; Atalay, F.; Cakir, A.; Cadirci, E.; Bayir, Y.; Suleyman, H. α-Lipoic acid has anti-inflammatory and anti-oxidative properties: An experimental study in rats with carrageenan-induced acute and cotton pellet-induced chronic inflammations. Br. J. Nutr. 2011, 105, 31–43. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Fu, J.; Zhao, Y.; Ji, K.; Luan, T.; Zang, B. Alpha-lipoic acid exerts anti-inflammatory effects on lipopolysaccharide-stimulated rat mesangial cells via inhibition of nuclear factor kappa B (NF-κB) signaling pathway. Inflammation 2015, 38, 510–519. [Google Scholar] [CrossRef]
- Aksoy, U.; Savtekin, G.; Şehirli, A.; Kermeoğlu, F.; Kalender, A.; Özkayalar, H.; Sayıner, S.; Orhan, K. Effects of alpha-lipoic acid therapy on experimentally induced apical periodontitis: A biochemical, histopathological and micro-CT analysis. Int. Endod. J. 2019, 52, 1317–1326. [Google Scholar] [CrossRef]
- Razaghi, A.; Poorebrahim, M.; Sarhan, D.; Björnstedt, M. Selenium stimulates the antitumour immunity: Insights to future research. Eur. J. Cancer 2021, 155, 256–267. [Google Scholar] [CrossRef]
- Espaladori, M.C.; Diniz, J.M.B.; de Brito, L.C.N.; Tavares, W.L.F.; Kawai, T.; Vieira, L.Q.; Sobrinho, A.P.R. Selenium intracanal dressing: Effects on the periapical immune response. Clin. Oral Investig. 2021, 25, 2951–2958. [Google Scholar] [CrossRef]
- Suez, J.; Zmora, N.; Segal, E.; Elinav, E. The pros, cons, and many unknowns of probiotics. Nat. Med. 2019, 25, 716–729. [Google Scholar] [CrossRef]
- Chudzik, A.; Orzyłowska, A.; Rola, R.; Stanisz, G.J. Probiotics, Prebiotics and Postbiotics on Mitigation of Depression Symptoms: Modulation of the Brain-Gut-Microbiome Axis. Biomolecules 2021, 11, 1000. [Google Scholar] [CrossRef]
- Gatej, S.; Gully, N.; Gibson, R.; Bartold, P.M. Probiotics and Periodontitis-A Literature Review. J. Int. Acad. Periodontol. 2017, 19, 42–50. [Google Scholar]
- Ranjith, A.; Nazimudeen, N.B.; Baiju, K.V. Probiotic mouthwash as an adjunct to mechanical therapy in the treatment of stage II periodontitis: A randomized controlled clinical trial. Int. J. Dent. Hyg. 2022, 20, 415–421. [Google Scholar] [CrossRef]
- Invernici, M.M.; Salvador, S.L.; Silva, P.H.F.; Soares, M.S.M.; Casarin, R.; Palioto, D.B.; Souza, S.L.S.; Taba, M.; Novaes, A.B.; Furlaneto, F.A.C.; et al. Effects of Bifidobacterium probiotic on the treatment of chronic periodontitis: A randomized clinical trial. J. Clin. Periodontol. 2018, 45, 1198–1210. [Google Scholar] [CrossRef]
- Invernici, M.M.; Furlaneto, F.A.C.; Salvador, S.L.; Ouwehand, A.C.; Salminen, S.; Mantziari, A.; Vinderola, G.; Ervolino, E.; Santana, S.I.; Silva, P.H.F.; et al. Bifidobacterium animalis subsp lactis HN019 presents antimicrobial potential against periodontopathogens and modulates the immunological response of oral mucosa in periodontitis patients. PLoS ONE 2020, 15, e0238425. [Google Scholar] [CrossRef]
- Cosme-Silva, L.; Dal-Fabbro, R.; Cintra, L.T.A.; Dos Santos, V.R.; Duque, C.; Ervolino, E.; Mogami Bomfim, S.; Gomes-Filho, J.E. Systemic administration of probiotics reduces the severity of apical periodontitis. Int. Endod. J. 2019, 52, 1738–1749. [Google Scholar] [CrossRef]
- Cosme-Silva, L.; Dal-Fabbro, R.; Cintra, L.T.A.; Ervolino, E.; Prado, A.S.D.; Oliveira, D.P.; Marcelos, P.; Gomes-Filho, J.E. Dietary supplementation with multi-strain formula of probiotics modulates inflammatory and immunological markers in apical periodontitis. J. Appl. Oral. Sci. 2021, 29, e20210483. [Google Scholar] [CrossRef]
- Cosme-Silva, L.; Dal-Fabbro, R.; Cintra, L.; Ervolino, E.; Plazza, F.; Mogami Bomfim, S.; Duarte, P.; Junior, V.; Gomes-Filho, J. Reduced bone resorption and inflammation in apical periodontitis evoked by dietary supplementation with probiotics in rats. Int. Endod. J. 2020, 53, 1084–1092. [Google Scholar] [CrossRef]
- Oishi, Y.; Manabe, I. Macrophages in inflammation, repair and regeneration. Int. Immunol. 2018, 30, 511–528. [Google Scholar] [CrossRef]
- Serhan, C.N.; Clish, C.B.; Brannon, J.; Colgan, S.P.; Chiang, N.; Gronert, K. Novel functional sets of lipid-derived mediators with antiinflammatory actions generated from omega-3 fatty acids via cyclooxygenase 2-nonsteroidal antiinflammatory drugs and transcellular processing. J. Exp. Med. 2000, 192, 1197–1204. [Google Scholar] [CrossRef]
- Huang, J.; Cai, X.; Ou, Y.; Zhou, Y.; Wang, Y. Resolution of inflammation in periodontitis: A review. Int. J. Clin. Exp. Pathol. 2018, 11, 4283–4295. [Google Scholar]
- Serhan, C.N.; Hong, S.; Gronert, K.; Colgan, S.P.; Devchand, P.R.; Mirick, G.; Moussignac, R.L. Resolvins: A family of bioactive products of omega-3 fatty acid transformation circuits initiated by aspirin treatment that counter proinflammation signals. J. Exp. Med. 2002, 196, 1025–1037. [Google Scholar] [CrossRef] [PubMed]
- Serhan, C.N.; Chiang, N.; Dalli, J.; Levy, B.D. Lipid mediators in the resolution of inflammation. Cold Spring Harb. Perspect. Biol. 2014, 7, a016311. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, I.; Falcato, F.; Bandarra, N.; Rauter, A.P. Resolvins, Protectins, and Maresins: DHA-Derived Specialized Pro-Resolving Mediators, Biosynthetic Pathways, Synthetic Approaches, and Their Role in Inflammation. Molecules 2022, 27, 1677. [Google Scholar] [CrossRef] [PubMed]
- Arnardottir, H.; Orr, S.K.; Dalli, J.; Serhan, C.N. Human milk proresolving mediators stimulate resolution of acute inflammation. Mucosal Immunol. 2016, 9, 757–766. [Google Scholar] [CrossRef]
- Kytikova, O.; Novgorodtseva, T.; Denisenko, Y.; Antonyuk, M.; Gvozdenko, T. Pro-Resolving Lipid Mediators in the Pathophysiology of Asthma. Medicina 2019, 55, 284. [Google Scholar] [CrossRef]
- Arita, M.; Ohira, T.; Sun, Y.P.; Elangovan, S.; Chiang, N.; Serhan, C.N. Resolvin E1 selectively interacts with leukotriene B4 receptor BLT1 and ChemR23 to regulate inflammation. J. Immunol. 2007, 178, 3912–3917. [Google Scholar] [CrossRef]
- Chiang, N.; Dalli, J.; Colas, R.A.; Serhan, C.N. Identification of resolvin D2 receptor mediating resolution of infections and organ protection. J. Exp. Med. 2015, 212, 1203–1217. [Google Scholar] [CrossRef]
- Aubeux, D.; Peters, O.A.; Hosseinpour, S.; Tessier, S.; Geoffroy, V.; Pérez, F.; Gaudin, A. Specialized pro-resolving lipid mediators in endodontics: A narrative review. BMC Oral Health 2021, 21, 276. [Google Scholar] [CrossRef]
- Serhan, C.N. Treating inflammation and infection in the 21st century: New hints from decoding resolution mediators and mechanisms. FASEB J. 2017, 31, 1273–1288. [Google Scholar] [CrossRef]
- Ali, M.; Yang, F.; Plachokova, A.S.; Jansen, J.A.; Walboomers, X.F. Application of specialized pro-resolving mediators in periodontitis and peri-implantitis: A review. Eur. J. Oral Sci. 2021, 129, e12759. [Google Scholar] [CrossRef]
- Perez-Hernandez, J.; Chiurchiù, V.; Perruche, S.; You, S. Regulation of T-Cell Immune Responses by Pro-Resolving Lipid Mediators. Front. Immunol. 2021, 12, 768133. [Google Scholar] [CrossRef]
- Scarparo, R.K.; Dondoni, L.; Böttcher, D.E.; Grecca, F.S.; Figueiredo, J.A.; Kantarci, A.; Van Dyke, T.E.; Batista, E.L. Intracanal delivery of Resolvin E1 controls inflammation in necrotic immature rat teeth. J. Endod. 2014, 40, 678–682. [Google Scholar] [CrossRef]
- Siddiqui, Y.D.; Omori, K.; Ito, T.; Yamashiro, K.; Nakamura, S.; Okamoto, K.; Ono, M.; Yamamoto, T.; Van Dyke, T.E.; Takashiba, S. Resolvin D2 Induces Resolution of Periapical Inflammation and Promotes Healing of Periapical Lesions in Rat Periapical Periodontitis. Front. Immunol. 2019, 10, 307. [Google Scholar] [CrossRef]
- Corazza, B.J.M.; Martinho, F.C.; Khoury, R.D.; Toia, C.C.; Orozco, E.I.F.; Prado, R.F.; Machado, F.P.; Valera, M.C. Clinical influence of calcium hydroxide and N-acetylcysteine on the levels of resolvins E1 and D2 in apical periodontitis. Int. Endod. J. 2021, 54, 61–73. [Google Scholar] [CrossRef]
- Serhan, C.N.; Savill, J. Resolution of inflammation: The beginning programs the end. Nat. Immunol. 2005, 6, 1191–1197. [Google Scholar] [CrossRef]
- Sears, B.; Saha, A.K. Dietary Control of Inflammation and Resolution. Front. Nutr. 2021, 8, 709435. [Google Scholar] [CrossRef]
- Yan, Y.; Jiang, W.; Spinetti, T.; Tardivel, A.; Castillo, R.; Bourquin, C.; Guarda, G.; Tian, Z.; Tschopp, J.; Zhou, R. Omega-3 fatty acids prevent inflammation and metabolic disorder through inhibition of NLRP3 inflammasome activation. Immunity 2013, 38, 1154–1163. [Google Scholar] [CrossRef]
- Azuma, M.M.; Gomes-Filho, J.E.; Ervolino, E.; Pipa, C.B.; Cardoso, C.B.M.; Andrada, A.C.; Kawai, T.; Cintra, L.T.A. Omega 3 Fatty Acids Reduce Bone Resorption While Promoting Bone Generation in Rat Apical Periodontitis. J. Endod. 2017, 43, 970–976. [Google Scholar] [CrossRef]
- Azuma, M.M.; Gomes-Filho, J.E.; Cardoso, C.B.M.; Pipa, C.B.; Narciso, L.G.; Bomfim, S.R.M.; Jacinto, R.C.; Cintra, L.T.A. Omega 3 Fatty Acids Reduce the Triglyceride Levels in Rats with Apical Periodontitis. Braz. Dent. J. 2018, 29, 173–178. [Google Scholar] [CrossRef]
- Azuma, M.M.; Cardoso, C.B.M.; Samuel, R.O.; Pipa, C.B.; Bomfim, S.R.M.; Narciso, L.G.; Gomes-Filho, J.E.; Cintra, L.T.A. Omega-3 Fatty Acids Alter Systemic Inflammatory Mediators Caused by Apical Periodontitis. J. Endod. 2021, 47, 272–277. [Google Scholar] [CrossRef]
- Shaddox, L.M.; Walker, C.B. Treating chronic periodontitis: Current status, challenges, and future directions. Clin. Cosmet. Investig. Dent. 2010, 2, 79–91. [Google Scholar] [CrossRef] [PubMed]
- Aimetti, M. Nonsurgical periodontal treatment. Int. J. Esthet. Dent. 2014, 9, 251–267. [Google Scholar] [PubMed]
- Cotti, E.; Careddu, R.; Schirru, E.; Marongiu, S.; Barca, M.P.; Manconi, P.E.; Mercuro, G. A case of SAPHO syndrome with endodontic implications and treatment with biologic drugs. J. Endod. 2015, 41, 1565–1570. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment | Key Treatment Strategies | Study Subjects | References (Available Articles) |
|---|---|---|---|
| Regenerative endodontics | Scaffolds with blood-clot; platelet-rich plasma; platelet-rich fibrin Apical papilla stem cell stimulation (root canal application) | Human Dogs | [30] [55] |
| Adalimumab | Anti-tumor necrosis factor alpha (local and systemic administration) | Ferret Human | [48,104] |
| NC-2300 | Cathepsin K inhibitor (oral administration) | Rats | [51] |
| Odanacatib | Cathepsin K inhibitor | Mice | [52] |
| AAV2 | Cathepsin K knockdown vector (root canal application) | Mice | [53] |
| AAV-sh-Atp6v1c1 | Recombinant adeno-associated virus-mediated Atp6v1c1 | Mice | [54] |
| Treg-cell therapy CCL22 | Targeting Treg cells Th1 & Th17 downregulation (root canal application) | Mice | [56] |
| Alpha-lipoic acid | Antioxidant (intraperitoneal injection) | Rats | [67] |
| Selenium | Antioxidant (root canal application) | Rats | [69] |
| Microbes | Probiotics (systemic administration) | Rats | [76] |
| Microbes | Probiotics (systemic administration) | Rats | [77] |
| Microbes | Probiotics (systemic administration) | Rats | [78] |
| Omega-3 fatty acid | Resolution of inflammation (systemic administration) | Rats | [99,100,101] |
| RVE1 | Resolution of inflammation (intracanal application) | Rats | [93] |
| RVD2 | Resolution of inflammation (intracanal application) | Rats | [94] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arias, Z.; Nizami, M.Z.I.; Chen, X.; Chai, X.; Xu, B.; Kuang, C.; Omori, K.; Takashiba, S. Recent Advances in Apical Periodontitis Treatment: A Narrative Review. Bioengineering 2023, 10, 488. https://doi.org/10.3390/bioengineering10040488
Arias Z, Nizami MZI, Chen X, Chai X, Xu B, Kuang C, Omori K, Takashiba S. Recent Advances in Apical Periodontitis Treatment: A Narrative Review. Bioengineering. 2023; 10(4):488. https://doi.org/10.3390/bioengineering10040488
Chicago/Turabian StyleArias, Zulema, Mohammed Zahedul Islam Nizami, Xiaoting Chen, Xinyi Chai, Bin Xu, Canyan Kuang, Kazuhiro Omori, and Shogo Takashiba. 2023. "Recent Advances in Apical Periodontitis Treatment: A Narrative Review" Bioengineering 10, no. 4: 488. https://doi.org/10.3390/bioengineering10040488
APA StyleArias, Z., Nizami, M. Z. I., Chen, X., Chai, X., Xu, B., Kuang, C., Omori, K., & Takashiba, S. (2023). Recent Advances in Apical Periodontitis Treatment: A Narrative Review. Bioengineering, 10(4), 488. https://doi.org/10.3390/bioengineering10040488