
A Review of the Technology, Training, and Assessment Methods for the First Real-Time AI-Enhanced Medical Device for Endoscopy


Abstract
1. Introduction
- CADe (computer-aided detection): algorithms that are able to localize/highlight the regions of an image that may reveal specific abnormalities;
- CADx (computer-aided diagnosis): algorithms that are aimed at characterizing/assessing the disease type, severity, stage, and progression.

2. Device Overview
2.1. Regulatory Status
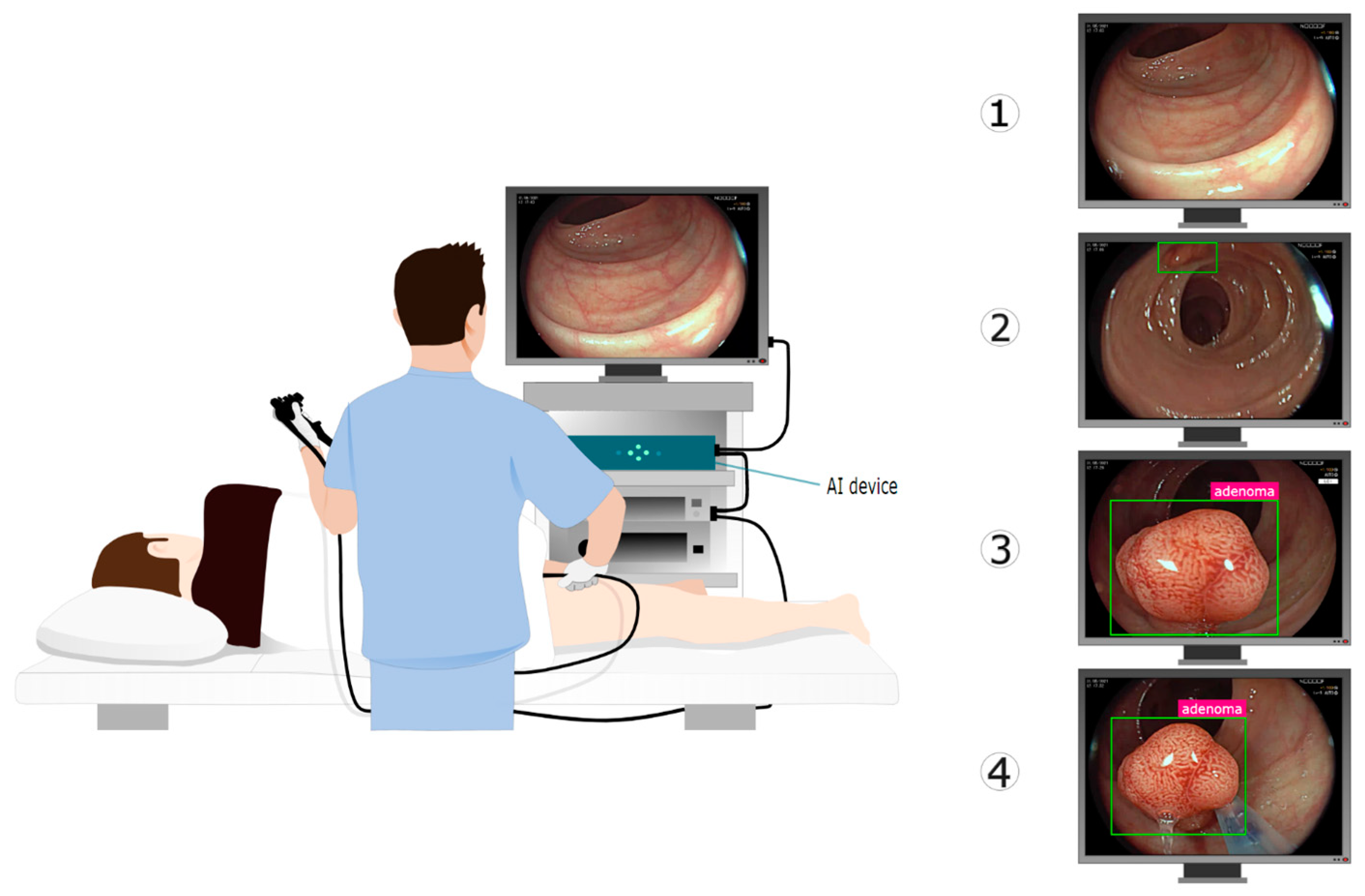
2.2. Video Flow for Real-Time Augmentation
2.3. Different Neural Networks for Different Needs

3. CADe for Polyp Detection
3.1. Dataset for AI Training and Testing
3.2. Methods for Assessing CADe Accuracy
3.2.1. Sensitivity per Frame/per Lesion
3.2.2. False-Positive Rates
4. CADx for Polyp Characterization
4.1. CADx Architecture
4.2. Details of AI Training and Polyp Classification
4.3. CADx Performance Testing
5. Discussion
5.1. Study Design and Algorithm Transparency
5.2. Why Is CADe Effective in Colonoscopy?
5.3. CADx Interactive Output
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ahmad, O.F.; Soares, A.S.; Mazomenos, E.; Brandao, P.; Vega, R.; Seward, E.; Stoyanov, D.; Chand, M.; Lovat, L.B. Artificial intelligence and computer-aided diagnosis in colonoscopy: Current evidence and future directions. Lancet Gastroenterol. Hepatol. 2019, 4, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Berzin, T.M.; Parasa, S.; Wallace, M.B.; Gross, S.A.; Repici, A.; Sharma, P. Position statement on priorities for artificial intelligence in GI endoscopy: A report by the ASGE Task Force. Gastrointest. Endosc. 2020, 92, 951–959. [Google Scholar] [CrossRef] [PubMed]
- Vulpoi, R.-A.; Luca, M.; Ciobanu, A.; Olteanu, A.; Barboi, O.-B.; Drug, V.L. Artificial Intelligence in Digestive Endoscopy—Where Are We and Where Are We Going? Diagnostics 2022, 12, 927. [Google Scholar] [CrossRef]
- Taghiakbari, M.; Mori, Y.; von Renteln, D. Artificial intelligence-assisted colonoscopy: A review of current state of practice and research. World J. Gastroenterol. 2021, 27, 8103–8122. [Google Scholar] [CrossRef] [PubMed]
- Cherubini, A.; East, J.E. Gorilla in the room: Even experts can miss polyps at colonoscopy and how AI helps complex visual perception tasks. Dig. Liver Dis. 2023, 55, 151–153. [Google Scholar] [CrossRef] [PubMed]
- Dellermann, D.; Ebel, P.; Söllner, M.; Leimeister, J.M. Hybrid Intelligence. Bus. Inf. Syst. Eng. 2019, 61, 637–643. [Google Scholar] [CrossRef]
- Benjamens, S.; Dhunnoo, P.; Meskó, B. The state of artificial intelligence-based FDA-approved medical devices and algorithms: An online database. NPJ Digit. Med. 2020, 3, 118. [Google Scholar] [CrossRef] [PubMed]
- Topol, E.J. High-performance medicine: The convergence of human and artificial intelligence. Nat. Med. 2019, 25, 44–56. [Google Scholar] [CrossRef]
- Rajpurkar, P.; Chen, E.; Banerjee, O.; Topol, E.J. AI in health and medicine. Nat. Med. 2022, 28, 31–38. [Google Scholar] [CrossRef]
- Strickland, E. IBM Watson, heal thyself: How IBM overpromised and underdelivered on AI health care. IEEE Spectr. 2019, 56, 24–31. [Google Scholar] [CrossRef]
- Esteva, A.; Robicquet, A.; Ramsundar, B.; Kuleshov, V.; DePristo, M.; Chou, K.; Cui, C.; Corrado, G.; Thrun, S.; Dean, J. A guide to deep learning in healthcare. Nat. Med. 2019, 25, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Petrick, N. Pre- and Post-Market Evaluation of Autonomous AI/ML: Lessons Learned from Prior CAD Devices. 2020. Available online: https://www.fda.gov/media/135712/download (accessed on 9 April 2021).
- US Food and Drug Administration. FDA Authorizes Marketing of First Device that Uses Artificial Intelligence to Help Detect Potential Signs of Colon Cancer. Available online: https://www.fda.gov/news-events/press-announcements/fda-authorizes-marketing-first-device-uses-artificial-intelligence-help-detect-potential-signs-colon (accessed on 9 April 2021).
- Hassan, C.; Wallace, M.B.; Sharma, P.; Maselli, R.; Craviotto, V.; Spadaccini, M.; Repici, A. New artificial intelligence system: First validation study versus experienced endoscopists for colorectal polyp detection. Gut 2020, 69, 799–800. [Google Scholar] [CrossRef] [PubMed]
- Repici, A.; Badalamenti, M.; Maselli, R.; Correale, L.; Radaelli, F.; Rondonotti, E.; Ferrara, E.; Spadaccini, M.; Alkandari, A.; Fugazza, A.; et al. Efficacy of Real-Time Computer-Aided Detection of Colorectal Neoplasia in a Randomized Trial. Gastroenterology 2020, 159, 512–520.e7. [Google Scholar] [CrossRef]
- Wallace, M.B.; Sharma, P.; Bhandari, P.; East, J.; Antonelli, G.; Lorenzetti, R.; Vieth, M.; Speranza, I.; Spadaccini, M.; Desai, M.; et al. Impact of Artificial Intelligence on Miss Rate of Colorectal Neoplasia. Gastroenterology 2022, 163, 295–304.e5. [Google Scholar] [CrossRef]
- Repici, A.; Spadaccini, M.; Antonelli, G.; Correale, L.; Maselli, R.; Galtieri, P.A.; Pellegatta, G.; Capogreco, A.; Milluzzo, S.M.; Lollo, G.; et al. Artificial intelligence and colonoscopy experience: Lessons from two randomised trials. Gut 2022, 71, 757–765. [Google Scholar] [CrossRef]
- Hassan, C.; Balsamo, G.; Lorenzetti, R.; Zullo, A.; Antonelli, G. Artificial Intelligence Allows Leaving-In-Situ Colorectal Polyps. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2022, 20, 2505–2513.e4. [Google Scholar] [CrossRef]
- Biffi, C.; Salvagnini, P.; Dinh, N.N.; Hassan, C.; Sharma, P.; GI Genius CADx Study Group; Cherubini, A. A novel AI device for real-time optical characterization of colorectal polyps. NPJ Digit. Med. 2022, 5, 84. [Google Scholar] [CrossRef]
- Reverberi, C.; Rigon, T.; Solari, A.; Hassan, C.; Cherubini, P.; GI Genius CADx Study Group; Cherubini, A. Experimental evidence of effective human-AI collaboration in medical decision-making. Sci. Rep. 2022, 12, 14952. [Google Scholar] [CrossRef]
- Biffi, C.; Salvagnini, P.; Dinh, N.N.; Hassan, C.; Sharma, P.; GI Genius CADx Study Group; Cherubini, A. Author Correction: A novel AI device for real-time optical characterization of colorectal polyps. NPJ Digit. Med. 2022, 5, 114. [Google Scholar] [CrossRef]
- Rex, D.K.; Mori, Y.; Sharma, P.; Lahr, R.E.; Vemulapalli, K.C.; Hassan, C. Strengths and Weaknesses of an Artificial Intelligence Polyp Detection Program as Assessed by a High-Detecting Endoscopist. Gastroenterology 2022, 163, 354–358.e1. [Google Scholar] [CrossRef] [PubMed]
- Hassan, C.; Badalamenti, M.; Maselli, R.; Correale, L.; Iannone, A.; Radaelli, F.; Rondonotti, E.; Ferrara, E.; Spadaccini, M.; Alkandari, A.; et al. Computer-aided detection-assisted colonoscopy: Classification and relevance of false positives. Gastrointest. Endosc. 2020, 92, 900–904.e4. [Google Scholar] [CrossRef] [PubMed]
- Ladabaum, U.; Shepard, J.; Weng, Y.; Desai, M.; Singer, S.J.; Mannalithara, A. Computer-aided Detection of Polyps Does Not Improve Colonoscopist Performance in a Pragmatic Implementation Trial. Gastroenterology 2022, 164, 481–483.e6. [Google Scholar] [CrossRef] [PubMed]
- Nehme, F.; Coronel, E.; Barringer, D.A.; Romero, L.; Shafi, M.A.; Ross, W.A.; Ge, P.S. Performance and Attitudes Toward Real-time Computer-aided Polyp Detection during Colonoscopy in a Large Tertiary Referral Center in the United States. Gastrointest. Endosc. 2023, S0016510723002638. [Google Scholar] [CrossRef] [PubMed]
- Levy, I.; Bruckmayer, L.; Klang, E.; Ben-Horin, S.; Kopylov, U. Artificial intelligence- aided colonoscopy does not increase adenoma detection rate in routine clinical practice. Am. J. Gastroenterol. 2022, 117, 1871–1873. [Google Scholar] [CrossRef]
- Koh, F.H.; Ladlad, J.; SKH Endoscopy Centre; Foo, F.-J.; Tan, W.J.; Sivarajah, S.S.; Ho, L.M.L.; Ng, J.-L.; Koh, F.H.; Chong, C.; et al. Real-time artificial intelligence (AI)-aided endoscopy improves adenoma detection rates even in experienced endoscopists: A cohort study in Singapore. Surg. Endosc. 2022, 37, 165–171. [Google Scholar] [CrossRef]
- Biscaglia, G.; Cocomazzi, F.; Gentile, M.; Loconte, I.; Mileti, A.; Paolillo, R.; Marra, A.; Castellana, S.; Mazza, T.; Di Leo, A.; et al. Real-time, computer-aided, detection-assisted colonoscopy eliminates differences in adenoma detection rate between trainee and experienced endoscopists. Endosc. Int. Open 2022, 10, E616–E621. [Google Scholar] [CrossRef]
- Spadaccini, M.; Iannone, A.; Maselli, R.; Badalamenti, M.; Desai, M.; Chandrasekar, V.T.; Patel, H.K.; Fugazza, A.; Pellegatta, G.; Galtieri, P.A.; et al. Computer-aided detection versus advanced imaging for detection of colorectal neoplasia: A systematic review and network meta-analysis. Lancet Gastroenterol. Hepatol. 2021, 6, 793–802. [Google Scholar] [CrossRef]
- Vokinger, K.N.; Gasser, U. Regulating AI in medicine in the United States and Europe. Nat. Mach. Intell. 2021, 3, 738–739. [Google Scholar] [CrossRef]
- Muehlematter, U.J.; Daniore, P.; Vokinger, K.N. Approval of artificial intelligence and machine learning-based medical devices in the USA and Europe (2015–20): A comparative analysis. Lancet Digit. Health 2021, 3, e195–e203. [Google Scholar] [CrossRef]
- Wolfe, J.M.; Kluender, K.R.; Levi, D.M.; Bartoshuk, L.M. Sensation & Perception; Sinauer Associates: Franklin County, MA, USA, 2006; ISBN 978-0-87893-938-1. [Google Scholar]
- Jiao, L.; Zhang, R.; Liu, F.; Yang, S.; Hou, B.; Li, L.; Tang, X. New Generation Deep Learning for Video Object Detection: A Survey. IEEE Trans. Neural Netw. Learn. Syst. 2022, 33, 3195–3215. [Google Scholar] [CrossRef] [PubMed]
- Vasey, B.; Nagendran, M.; Campbell, B.; Clifton, D.A.; Collins, G.S.; Denaxas, S.; Denniston, A.K.; Faes, L.; Geerts, B.; Ibrahim, M.; et al. Reporting guideline for the early-stage clinical evaluation of decision support systems driven by artificial intelligence: DECIDE-AI. Nat. Med. 2022, 28, 924–933. [Google Scholar] [CrossRef] [PubMed]
- Sounderajah, V.; Ashrafian, H.; Aggarwal, R.; De Fauw, J.; Denniston, A.K.; Greaves, F.; Karthikesalingam, A.; King, D.; Liu, X.; Markar, S.R.; et al. Developing specific reporting guidelines for diagnostic accuracy studies assessing AI interventions: The STARD-AI Steering Group. Nat. Med. 2020, 26, 807–808. [Google Scholar] [CrossRef] [PubMed]
- Cruz Rivera, S.; Liu, X.; Chan, A.-W.; Denniston, A.K.; Calvert, M.J.; The SPIRIT-AI and CONSORT-AI Working Group; SPIRIT-AI and CONSORT-AI Steering Group; Darzi, A.; Holmes, C.; Yau, C.; et al. Guidelines for clinical trial protocols for interventions involving artificial intelligence: The SPIRIT-AI extension. Nat. Med. 2020, 26, 1351–1363. [Google Scholar] [CrossRef]
- Ahmad, O.F.; Mori, Y.; Misawa, M.; Kudo, S.; Anderson, J.T.; Bernal, J.; Berzin, T.M.; Bisschops, R.; Byrne, M.F.; Chen, P.-J.; et al. Establishing key research questions for the implementation of artificial intelligence in colonoscopy: A modified Delphi method. Endoscopy 2021, 53, 893–901. [Google Scholar] [CrossRef] [PubMed]
- Bilal, M.; Brown, J.R.G.; Berzin, T.M. Incorporating standardised reporting guidelines in clinical trials of artificial intelligence in gastrointestinal endoscopy. Lancet Gastroenterol. Hepatol. 2020, 5, 962–964. [Google Scholar] [CrossRef]
- Repici, A.; Wallace, M.B.; East, J.E.; Sharma, P.; Ramirez, F.C.; Bruining, D.H.; Young, M.; Gatof, D.; Irene (Mimi) Canto, M.; Marcon, N.; et al. Efficacy of Per-oral Methylene Blue Formulation for Screening Colonoscopy. Gastroenterology 2019, 156, 2198–2207.e1. [Google Scholar] [CrossRef]
- Parasa, S.; Repici, A.; Berzin, T.; Leggett, C.; Gross, S.A.; Sharma, P. Framework and metrics for the clinical use and implementation of artificial intelligence algorithms into endoscopy practice: Recommendations from the American Society for Gastrointestinal Endoscopy Artificial Intelligence Task Force. Gastrointest. Endosc. 2023, S0016510722020521. [Google Scholar] [CrossRef]
- Xu, Y.; Ding, W.; Wang, Y.; Tan, Y.; Xi, C.; Ye, N.; Wu, D.; Xu, X. Comparison of diagnostic performance between convolutional neural networks and human endoscopists for diagnosis of colorectal polyp: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0246892. [Google Scholar] [CrossRef]
- Holzwanger, E.A.; Bilal, M.; Glissen Brown, J.R.; Singh, S.; Becq, A.; Ernest-Suarez, K.; Berzin, T.M. Benchmarking definitions of false-positive alerts during computer-aided polyp detection in colonoscopy. Endoscopy 2021, 53, 937–940. [Google Scholar] [CrossRef]
- Tajbakhsh, N.; Gurudu, S.R.; Liang, J. Automated Polyp Detection in Colonoscopy Videos Using Shape and Context Information. IEEE Trans. Med. Imaging 2015, 35, 630–644. [Google Scholar] [CrossRef] [PubMed]
- Rex, D.K.; Boland, R.C.; Dominitz, J.A.; Giardiello, F.M.; Johnson, D.A.; Kaltenbach, T.; Levin, T.R.; Lieberman, D.; Robertson, D.J. Colorectal Cancer Screening: Recommendations for Physicians and Patients from the U.S. Multi-Society Task Force on Colorectal Cancer. Am. J. Gastroenterol. 2017, 112, 1016–1030. [Google Scholar] [CrossRef] [PubMed]
- Bisschops, R.; East, J.E.; Hassan, C.; Hazewinkel, Y.; Kamiński, M.F.; Neumann, H.; Pellisé, M.; Antonelli, G.; Bustamante Balen, M.; Coron, E.; et al. Advanced imaging for detection and differentiation of colorectal neoplasia: European Society of Gastrointestinal Endoscopy (ESGE) Guideline—Update 2019. Endoscopy 2019, 51, 1155–1179. [Google Scholar] [CrossRef] [PubMed]
- Nogueira-Rodríguez, A.; Domínguez-Carbajales, R.; López-Fernández, H.; Iglesias, Á.; Cubiella, J.; Fdez-Riverola, F.; Reboiro-Jato, M.; Glez-Peña, D. Deep Neural Networks approaches for detecting and classifying colorectal polyps. Neurocomputing 2021, 423, 721–734. [Google Scholar] [CrossRef]
- Mori, Y.; Kudo, S.; Misawa, M.; Saito, Y.; Ikematsu, H.; Hotta, K.; Ohtsuka, K.; Urushibara, F.; Kataoka, S.; Ogawa, Y.; et al. Real-Time Use of Artificial Intelligence in Identification of Diminutive Polyps During Colonoscopy: A Prospective Study. Ann. Intern. Med. 2018, 169, 357. [Google Scholar] [CrossRef]
- Schlemper, R.J.; Riddell, R.H.; Kato, Y.; Borchard, F.; Cooper, H.S.; Dawsey, S.M.; Dixon, M.F.; Fenoglio-Preiser, C.M.; Fléjou, J.-F.; Geboes, K.; et al. The Vienna classification of gastrointestinal epithelial neoplasia. Gut 2000, 47, 251–255. [Google Scholar] [CrossRef]
- Rex, D.K.; Hassan, C.; Bourke, M.J. The colonoscopist’s guide to the vocabulary of colorectal neoplasia: Histology, morphology, and management. Gastrointest. Endosc. 2017, 86, 253–263. [Google Scholar] [CrossRef]
- Rex, D.K.; Kahi, C.; O’Brien, M.; Levin, T.R.; Pohl, H.; Rastogi, A.; Burgart, L.; Imperiale, T.; Ladabaum, U.; Cohen, J.; et al. The American Society for Gastrointestinal Endoscopy PIVI (Preservation and Incorporation of Valuable Endoscopic Innovations) on real-time endoscopic assessment of the histology of diminutive colorectal polyps. Gastrointest. Endosc. 2011, 73, 419–422. [Google Scholar] [CrossRef]
- Seager, A.; Sharp, L.; Hampton, J.S.; Neilson, L.J.; Lee, T.J.W.; Brand, A.; Evans, R.; Vale, L.; Whelpton, J.; Rees, C.J. Trial protocol for COLO-DETECT: A randomized controlled trial of lesion detection comparing colonoscopy assisted by the GI GeniusTM artificial intelligence endoscopy module with standard colonoscopy. Color. Dis. 2022, 24, 1227–1237. [Google Scholar] [CrossRef]
- Plana, D.; Shung, D.L.; Grimshaw, A.A.; Saraf, A.; Sung, J.J.Y.; Kann, B.H. Randomized Clinical Trials of Machine Learning Interventions in Health Care: A Systematic Review. JAMA Netw. Open 2022, 5, e2233946. [Google Scholar] [CrossRef]
- Hassan, C.; Mori, Y.; Sharma, P.; Spadaccini, M.; Repici, A. Detrimental Detection of Advanced Lesions with AI: False-confidence or Prevalence Bias? Am. J. Gastroenterol. 2022, 117, 2088–2089. [Google Scholar] [CrossRef] [PubMed]
- Barua, I.; Wieszczy, P.; Kudo, S.; Misawa, M.; Holme, Ø.; Gulati, S.; Williams, S.; Mori, K.; Itoh, H.; Takishima, K.; et al. Real-Time Artificial Intelligence–Based Optical Diagnosis of Neoplastic Polyps during Colonoscopy. NEJM Evid. 2022, 1, EVIDoa2200003. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Training/Validation (568 Subjects) | Holdout Test Set (150 Subjects) | Overall (718 Subjects) | ||||
|---|---|---|---|---|---|---|
| Mean Age, years (SD) | 61.6 | (6.58) | 61.5 | (6.32) | 61.6 | (6.59) |
| Sex, N (%) | ||||||
| Male | 370 | (65.1%) | 93 | (62.0%) | 463 | (64.5%) |
| Female | 198 | (34.9%) | 57 | (38.0%) | 255 | (35.5%) |
| Indication for Colonoscopy, N (%) | ||||||
| Screening | 270 | (47.5%) | 73 | (46.7%) | 343 | (47.8%) |
| Surveillance ≤ 2 years | 43 | (7.6%) | 7 | (4.7%) | 50 | (7.0%) |
| Surveillance > 2 years | 255 | (44.9%) | 70 | (48.7%) | 325 | (45.3%) |
| Race/Ethnicity | ||||||
| White or Caucasian | 522 | (91.9%) | 141 | (94.0%) | 663 | (92.3%) |
| Black or African American | 34 | (6.0%) | 5 | (3.3%) | 39 | (5.4%) |
| Hispanic or Latino | 7 | (1.2%) | 0 | (0%) | 7 | (1.0%) |
| Asian | 3 | (0.5%) | 3 | (2.0%) | 6 | (0.8%) |
| Native Hawaiian or other Pacific Islander | 1 | (0.2%) | 1 | (0.7%) | 2 | (0.3%) |
| GI Genius CADe v1 | GI Genius CADe v2 | |||
|---|---|---|---|---|
| Label | Overall FP | FP per Patient | Overall FP | FP per Patient |
| Bin 1: <500 ms | 21,962 | 146.41 | 15,903 | 106.02 |
| Bin 2: ≥500 ms <1000 ms | 896 | 5.97 | 907 | 6.05 |
| Bin 3: ≥1000 ms <1500 ms | 283 | 1.89 | 303 | 2.02 |
| Bin 4: ≥1500 ms <2000 ms | 118 | 0.79 | 154 | 1.03 |
| Bin 5: ≥2000 ms | 187 | 1.25 | 269 | 1.79 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cherubini, A.; Dinh, N.N. A Review of the Technology, Training, and Assessment Methods for the First Real-Time AI-Enhanced Medical Device for Endoscopy. Bioengineering 2023, 10, 404. https://doi.org/10.3390/bioengineering10040404
Cherubini A, Dinh NN. A Review of the Technology, Training, and Assessment Methods for the First Real-Time AI-Enhanced Medical Device for Endoscopy. Bioengineering. 2023; 10(4):404. https://doi.org/10.3390/bioengineering10040404
Chicago/Turabian StyleCherubini, Andrea, and Nhan Ngo Dinh. 2023. "A Review of the Technology, Training, and Assessment Methods for the First Real-Time AI-Enhanced Medical Device for Endoscopy" Bioengineering 10, no. 4: 404. https://doi.org/10.3390/bioengineering10040404
APA StyleCherubini, A., & Dinh, N. N. (2023). A Review of the Technology, Training, and Assessment Methods for the First Real-Time AI-Enhanced Medical Device for Endoscopy. Bioengineering, 10(4), 404. https://doi.org/10.3390/bioengineering10040404