



A Review on the Usability, Flexibility, Affinity, and Affordability of Virtual Technology for Rehabilitation Training of Upper Limb Amputees
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Purpose of the Review
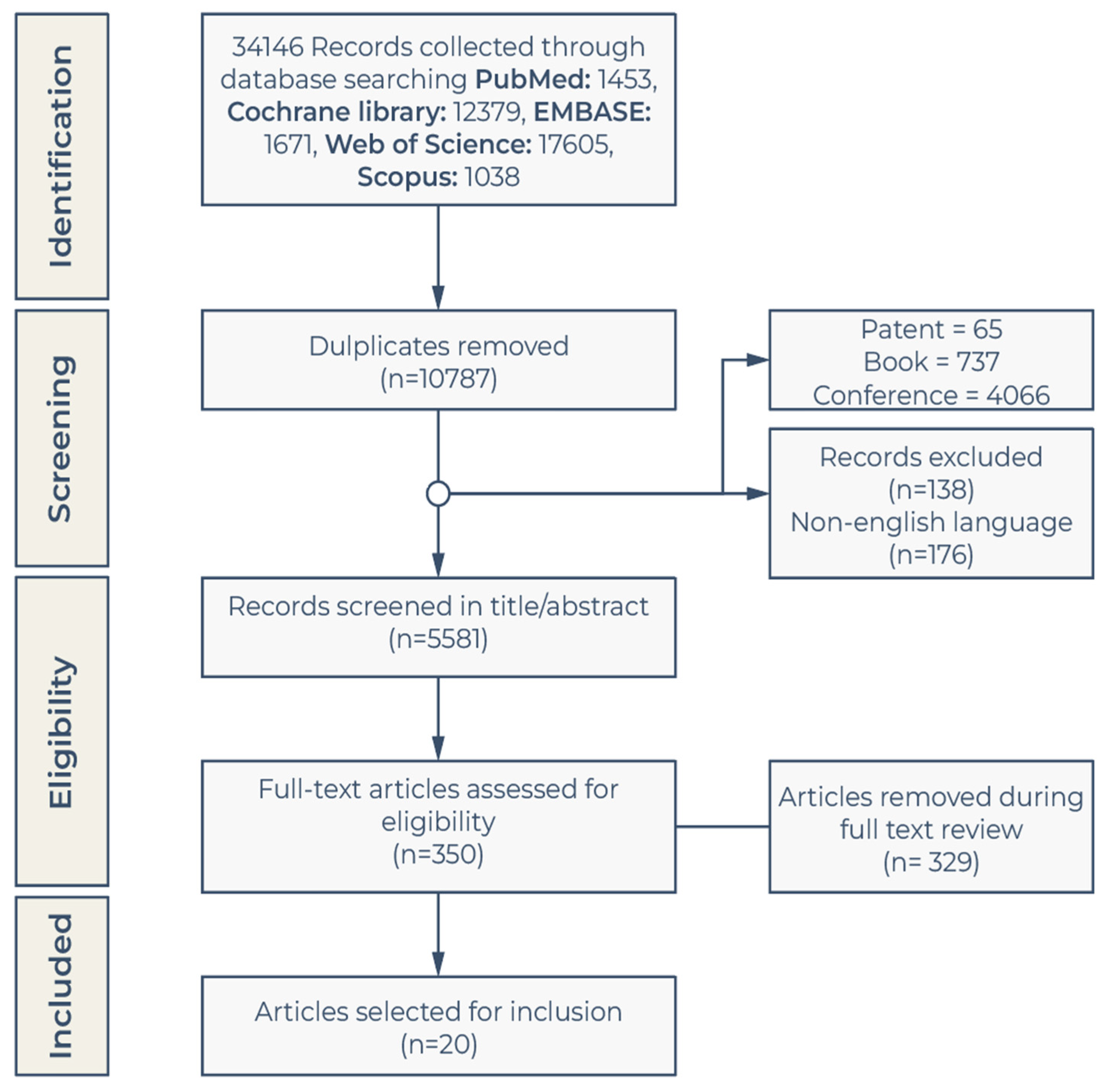
2.2. Literature Research
2.3. Inclusion and Exclusion Criteria
- The title, abstract, or keywords contain at least one of the following terms: upper limb amputation, upper extremity amputation, hand amputation, virtual reality, or video game;
- The study type is either a research paper, clinical trial, or review;
- The article is written in English.
- Other types of research include conference papers, communication, keynotes, or book chapters;
2.4. Data Analysis
- The study details an original virtual rehabilitation system devised by the author, which stands out due to its unique approach that avoids the need for participant recruitment or simulated research. This innovative system, implemented according to the CASP guidelines, brings important advancements to the field.
- After analyzing the research involving the recruited participants, we found that the selection criteria demographic or epidemiological information of the selected individuals were not discussed. We used CASP for this analysis.
- The remaining aspects of the study adhere to the STROBE guidelines.
3. Results
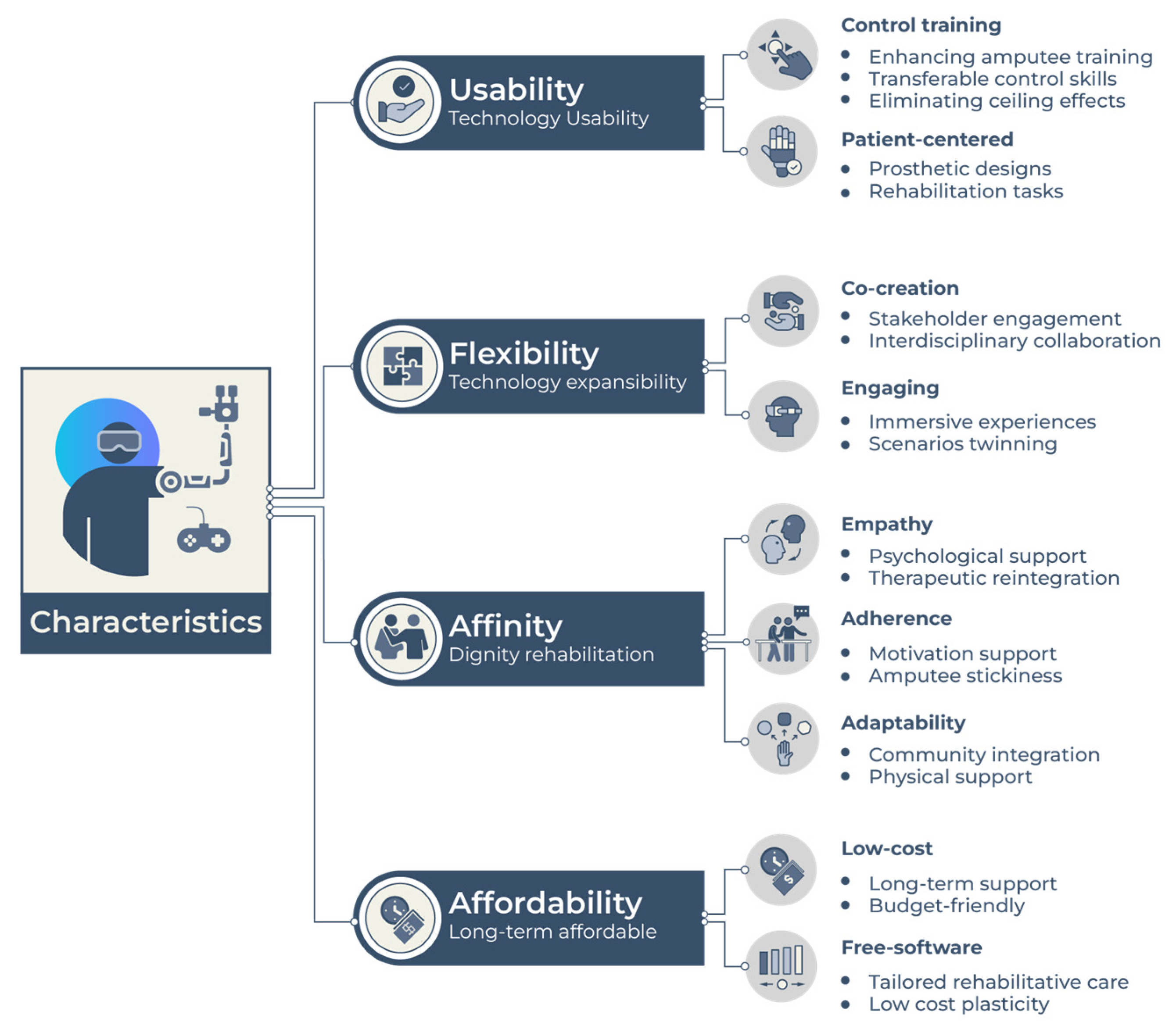
4. Discussion
4.1. Usability
4.2. Flexibility
4.3. Affinity
4.4. Affordability
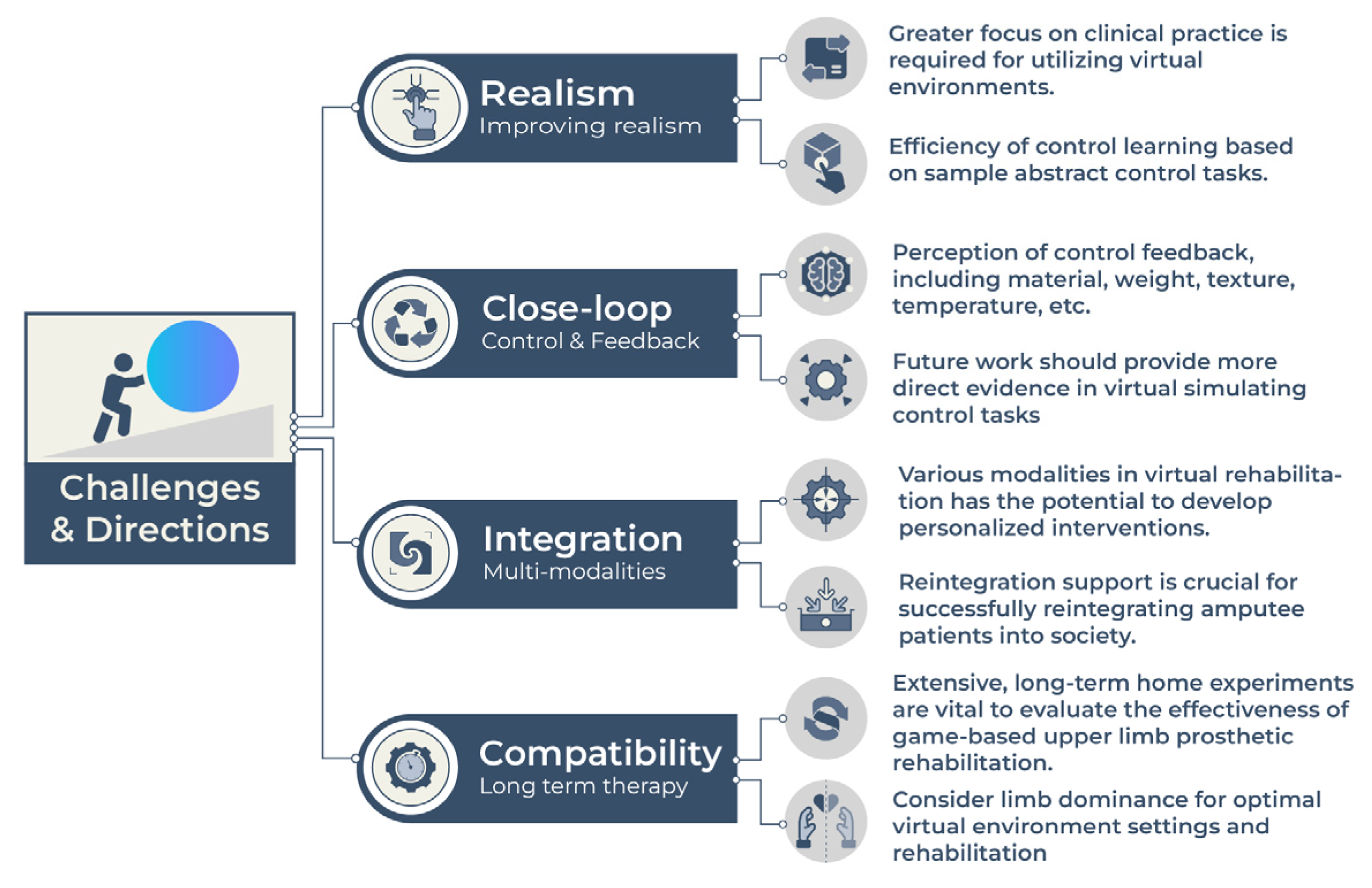
4.5. Future Challenges and Directions
- Advances in virtual prosthetic training-based prosthesis rehabilitation are predominantly limited to academic research settings, with few practical applications in clinical environments.
- We identified a need for more research focused on incorporating closed-loop control of user feedback (especially prosthetic tactile sensation, such as material, texture, temperature, etc.) into immersive virtual environments.
- One significant challenge to the widespread adoption of the technology discussed in this article lies in the limited number of amputee subjects involved in the experimental trials. Such trials pose challenges in obtaining generalizable results. As scientific knowledge advances, it becomes increasingly crucial to incorporate user-centered designs and larger sample sizes in studies related to clinical deployments. Subsequently, it becomes necessary to evaluate whether remote training options can support these studies.
- The elderly population may encounter challenges when using virtual rehabilitation technology. First, they may have deficiencies in the fundamental skills required for operating smart electronic devices. Second, the deterioration of neuromuscular function may result in the inability to operate the virtual human–machine system.
- Improving realism: This can be achieved by integrating novel technologies (e.g., haptic feedback-increased degrees of freedom in virtual environments) and using realistic visual cues in simulated tasks. In addition, there is a need to enhance closed-loop control to improve the accuracy of motion tracking and achieve more natural movements in virtual settings. Improvement of virtual reality environments and virtual limbs in rehabilitation paradigms has been proposed to enhance their efficacy. The modeling of virtual limbs with a higher degree of realism and movement resolution has the potential to yield substantial benefits. In addition, future research should evaluate the impact of pre-prosthetic training methods on various outcomes in amputee populations.
- Enhancing closed-loop control: Enhanced closed-loop control refers to optimizing the communication between the user and the device, allowing for more natural and intuitive movements. This can be achieved through advanced sensors, machine learning algorithms, and real-time feedback. By improving the accuracy and response speed of the device, patients may experience greater control and improved function.
- Integrating multiple modalities: Furthermore, there is a growing need to explore the use of various modalities in virtual rehabilitation. Advances in this direction can result in the development of personalized multimodal interventions tailored to individual needs and preferences. Such interventions can integrate visual, auditory, and haptic feedback to create rich and immersive training experiences.
- Supporting reintegration: Reintegration support involves providing patients with the necessary resources and support to successfully reintegrate into society following amputation and rehabilitation. This may include vocational training, peer support groups, and mental health services. By addressing the psychosocial aspects of rehabilitation, patients may enjoy more fulfilling lives.
- Persistent attention has been devoted to serious games within the realm of rehabilitative practices over an extended period. Our study delves into the utilization of game-based approaches in the context of prosthetic rehabilitation with a specific emphasis on upper limb training. To ascertain the effectiveness of games in upper limb prosthetic rehabilitation, it is imperative to prioritize extensive, long-term experiments conducted within individuals’ homes, as they yield substantial evidence of their efficacy.
- Virtual environment paradigms should consider limb dominance to optimize their settings for better performance and perceptional engagement. Adapting rehabilitation for handedness may benefit unilateral impairments [51].
5. Conclusions
- Virtual environments are effective for prosthetic rehabilitation in amputees as they can accomplish control training through virtual environments and transfer their control experience to the real prostheses.
- The technological components outlined in this study, such as signal control, sensation feedback, adaptability, and gamification, can be combined for the purpose of enhancing user engagement and facilitating autonomous learning within and beyond clinical settings.
- The integration of immersive serious gaming and visual and somatosensory feedback using virtual technology, in particular, holds immense potential for promoting prosthetic embodiment within the virtual space.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Supplementary Information for the Reviewed 17 Articles

{kind=link}
{kind=link}
{kind=link}
| Author | Year | Article Type | Participants Scale | UL Amputation | Age Range/Age Mean (SD) | Study Purpose | Methods and Tools | Relevant Conclusion | Treatment Effects | Paper Quality |
|---|---|---|---|---|---|---|---|---|---|---|
| Simon et al. [37]. | 2011 | Research articles | Five upper limb amputees | Three right trans-radial amputations; One left trans-radial amputation; Two bilateral amputations | 24–62 (45.2 ± 16.3) | The study aimed to assess the performance of individuals with trans-radial amputations using myoelectric pattern recognition with proportional control in a virtual prosthesis, specifically evaluating the effects of classifiers and task complexities on completion time and path efficiency. | The study utilized myoelectric pattern recognition with proportional control and a virtual prosthesis to assess the performance of individuals with trans-radial amputations, using a Target Achievement Control test with varying classifiers and task complexities. | The study concluded that the Target Achievement Control (TAC) test in a virtual reality environment provides a valuable platform for assessing user myoelectric control and pattern recognition algorithms, offering more comprehensive control information than existing offline measures and simplified virtual performance tests. | Subjects controlled seven motion classes of a virtual prosthesis with an average classification accuracy of 94.0 ± 3.1 percent in the TAC test. The TAC test also allows subjects to control the speed of the virtual prosthesis based on their muscle contraction intensity. | CASP |
| Rahman Davoodi and Gerald E. Loeb [38] | 2012 | Research articles | One upper limb amputee | Shoulder disarticulation amputation | - | The study aims to develop a physics-based target shooting game as a virtual training environment for upper limb amputees to practice and learn the control of a multi-joint prosthesis, with a focus on realistic simulations and user immersion. | The study developed a physics-based target shooting game using freely available software tools to train upper limb amputees in operating multi-joint neural prostheses in a realistic and engaging virtual environment. | The target shooting game is designed to help amputees practice and learn the control of a multi-joint prosthesis in a virtual simulation environment, providing realistic movement and interactions with objects. | The virtual target shooting game provides upper limb amputees with a realistic and immersive training environment, thanks to its ability to perform real-time computations, smooth control of virtual arm and finger movement, execution within allowable integration time steps, efficient rendering time, and low loop latency resulting in real-time update rates. | CASP |
| RR Kaliki et al. [39]. | 2013 | Research articles | Eight non-disabled participants | - | - | The purpose of the study was to evaluate the performance of a non-invasive command scheme for upper limb prostheses in a virtual reality task. | The study used an anthropomorphic arm model and artificial neural networks to develop a non-invasive command scheme for upper limb prostheses, analyzing spatial variability in performance over sessions and comparing differences in performance between groups. | The study found that subjects using the non-invasive command scheme for upper limb prostheses showed progressive improvement in completing a reach and grasp task in virtual technologies, with a high completion percentage achieved after multiple sessions, indicating the potential effectiveness of the control paradigm. | VR has shown potential in improving motor function, sensory feedback integration, patient engagement, realistic simulations, and customization in prosthetic rehabilitation, as evidenced by studies comparing VR to traditional methods and measuring various outcomes. | CASP STROBE |
| MA Powell et al. [40]. | 2013 | Research articles | Four trans-radial amputees | Trans-radial amputation | - | The study aims to investigate the effectiveness of using virtual technology for pattern recognition training in individuals with limb loss. | The study methods involved an initial supervised testing session followed by at-home training using a pattern recognition training system, with the use of detailed written instructions and supervised practice to ensure familiarity and proficiency with the software and equipment. | The conclusion of the study is that pattern recognition training can be effective in enabling amputees to control a virtual prosthesis using muscle activity from their intact limb, leading to improved movement distinguishability and a sense of naturalness in performing various hand and wrist movements. | Virtual technologies offer improved initial control and awareness of virtual prostheses, potential benefits for previous myoelectric prosthesis users, reversal of cortical reorganization through training, reduced phantom limb pain, favorable functional outcomes, enhanced rehabilitation and training experience, and the potential for further advancements in research and development. | CASP |
| NE Bunderson [41]. | 2014 | Research articles | Four non-upper limb amputees and one shoulder disarticulation patient | One patient with shoulder disarticulation | - | The purpose of this study was to assess the performance and control strategies of an impulsive virtual prosthesis in a Box and Block Test and compare it to physical prostheses. | This study used an impulsive virtual environment with an eight-degree-of-freedom prosthesis controlled through EMG pattern recognition to perform a Box and Block Test, demonstrating the feasibility of this approach for upper limb prostheses. | The study demonstrated the use of a virtual environment with an eight-degree-of-freedom prosthesis controlled through EMG pattern recognition, showing promise for evaluating prosthetic control strategies and potentially improving physical prosthesis design and use. | Virtual environment improved completion time by 29% for non-amputees and 31% for shoulder disarticulation subjects, with a grip force of approximately 70N, exceeding the average pinch force of 60N, and Endpoint In being the most frequently selected class. Elbow flex/extension distance showed the strongest correlation with completion time, while wrist flex/extension had the weakest correlation. | CASP STROBE |
| D. Blana et al. [42]. | 2016 | Research articles | 10 (seven male, three female) | - | 22–35 | The purpose of the study was to test the feasibility of using a virtual reality environment to simulate prosthesis control and evaluate the performance of a novel controller that combines EMG and kinematic signals for predicting forearm movement. | The study utilized a virtual reality environment and a combination of electromyography (EMG) and kinematic signals to train and test an artificial neural network (ANN) for prosthesis control. | The study used a virtual reality environment to evaluate the feasibility of using combined EMG and kinematic signals for prosthesis control and found that participants were able to achieve the required accuracy with the trained artificial neural network, although online performance showed larger prediction errors. | Virtual reality offers advantages for upper limb amputees through data collection, model-based training, and control of simulated prosthetic devices using kinematic and muscle activity signals. Testing with amputee participants shows the effectiveness of this approach, achieving high path efficiency (78%) and minimal overshoot while providing valuable data on controller performance. | CASP |
| Kurzynski et al. [43]. | 2017 | Research articles | One | One participant with bilateral upper limb congenital amputation (no upper extremities from glenohumeral joints level) | 30 years old woman | The purpose of this study is to investigate the potential benefits of computer-aided mental training in promoting motor function learning in individuals before upper limb transplantation. | The study utilized a computer-aided training (CAT) system, which included a virtual hand with visual and sensory feedback, along with EEG recordings, to investigate the effects of mental training on motor function learning before upper limb transplantation. | The study presented a computer-aided training system using virtual reality and sensory feedback to facilitate structural and functional reorganization of the brain, leading to improved motor function in patients before upper limb transplantation. | The study found that using virtual reality and sensory feedback in pre-transplantation training for upper limb transplantation led to positive changes in cortical activity, highlighting the potential of virtual technologies in enhancing motor function learning and suggesting the use of biosignal analysis for future improvements. | CASP |
| N A Hashim et al. [44]. | 2018 | Case–control study | 10 (five amputees and five non-disabled) | Trans-radial amputation | 26.3 (±4.47) | The purpose of the study was to investigate the impact of incorporating video games into the rehabilitation protocol for upper limb amputees, with a focus on functional outcomes, patient motivation, and muscle control. | The study utilized a Myo armband connected via Bluetooth and commercially available equipment to assess the impact of incorporating video games into the rehabilitation protocol for upper limb amputees, with assessments including the Box and Block Test, electromyography (EMG) readings, and modified Intrinsic Motivation Inventory (IMI) questionnaires. | The study concluded that incorporating video games into the upper limb amputee rehabilitation protocol resulted in improved motor coordination, muscle strength, and patient motivation, suggesting the potential benefits of video game-based rehabilitation for this population. The results show a significant positive association between the training period and the Box and Block Test score (r8 = 0.95, p < 0.001) | The study’s quantitative results showed that amputee participants enjoyed the game (p < 0.001) Crate Whacker less than able-bodied participants while also reporting improvements in muscle strength and positive motivational aspects of training gamification through an IMI questionnaire. | CASP STROBE |
| C Prahm et al. [45]. | 2018 | Control group study | 14 participants | Traumatic trans-radial or trans-humeral upper limb amputees | - | The study aimed to investigate the effectiveness of game-based interventions and virtual technologies in improving EMG control, muscle separation, and endurance in individuals with upper limb amputation, as well as assessing user experience and satisfaction with the interventions. | The study utilized game-based interventions, virtual technologies, and EMG assessments to evaluate the effectiveness of training upper limb amputees in muscle control and endurance. | The study found that integrating game-based interventions into rehabilitation protocols for upper limb amputees can lead to improved muscle control, endurance, and engagement, suggesting the potential for more effective and enjoyable rehabilitation methods. | The study found improvements in proportional precision control, muscle separation, endurance control, and MVC values among participants, who enjoyed playing the games more than using the MyoBoy and rated the rhythm and racing games highly for input, game controls, fun, and motivation. | STROBE |
| BN Perry et al. [46]. | 2018 | Quantitative research | 13 participants | Military upper extremity amputation | 26.2 (±3.76) | The purpose of the study was to evaluate the effectiveness of virtual training using the Virtual Integration Environment (VIE) platform for individuals with upper limb amputation in improving their motor control and prosthetic limb functionality. | The study utilized the Virtual Integration Environment (VIE) platform to provide virtual training and assess motor control using surface electromyography (sEMG) data collected from participants with upper limb amputation. | The study found that participants were able to effectively control a virtual limb using pattern recognition software, achieving high accuracy scores for various upper limb movements, indicating the potential for using virtual integration environments as prosthetic limb trainers. | Passive motor training had 43.8% ± 10.7% accuracy, while >95% accuracy was achieved in Basic sets and 50% in Advanced and Digit sets during active motor sessions; significant improvement in active motor scores in Basic and Advanced sets and a trend towards significance in Digit sets shows the effectiveness of a virtual reality training platform for upper limb amputees and supports pattern recognition feedback in advanced myoelectric prostheses. | CASP STROBE |
| L Hargrove et al. [46]. | 2018 | Quantitative research | Nine trans-humeral amputees with targeted muscle reinnervation surgery and fitted with a myoelectric prosthesis | Trans-humeral amputees | 38.8 (±11.89) | The purpose of this study was to determine the relationship between performance on a virtual test and performance with a physical prosthesis, as well as to assess the potential improvement in functional outcomes after a 6-week home trial using pattern recognition-controlled prosthetic arms. | The study utilized a sample of individuals with trans-humeral-level amputations who had undergone targeted muscle reinnervation surgery to investigate the relationship between performance on a virtual test (Target Achievement Control test) and performance with a physical prosthesis, as well as the potential improvement in functional outcomes after a 6-week home trial using pattern recognition-controlled prosthetic arms. | The study found that using virtual tests, such as the Target Achievement Control (TAC) test, can be correlated with physical outcome measures in individuals with trans-humeral-level amputations using pattern recognition-controlled prosthetic arms, suggesting the potential for virtual environments to assess and improve functional outcomes in upper limb prosthetics. | Pattern recognition-controlled prostheses in a home trial showed promising results, including reduced TAC completion time (p = 0.007), improved performance in SHAP and Box and Block Tests (p = 0.001 and p = 0.03, respectively), strong correlations between TAC completion time and physical measures, and a correlation between classification error rate and performance in Clothespin Relocation task (p = 0.018), suggesting potential translation of virtual performance into functional outcomes. | CASP STROBE |
| BD. Winslow et al. [11]. | 2018 | Quantitative research | 12 non-disabled participants | - | 30.6 (±6) | The purpose of the study was to evaluate the effectiveness and user experience of a mobile game-based prosthesis training system for individuals with upper limb amputation. | The study utilized a mobile game-based prosthesis training system called ADAPT-MP, which included four training games (Dino Sprint, Dino Feast, Volcanic Crush, and Dino Claw), and collected data through user evaluation surveys (UES), Intrinsic Motivation Inventory (IMI), system usability scale (SUS), and EMG measurements. | The study demonstrated that a mobile game-based prosthesis training system called ADAPT-MP led to rapid improvements in wrist flexor/extensor control and EMG levels, increased motivation, and positive user experiences, suggesting its potential as an effective pre-prosthetic training tool. | Virtual technologies have the potential to enhance rehabilitation success rates by providing engaging and mobile training outside the clinic, addressing current issues in onsite training, and allowing for remote monitoring through cloud- and web-based data communication | CASP STROBE |
| DT. Kluger et al. [48]. | 2019 | Quantitative research | Two trans-radial amputees (intramuscular EMG) | Trans-radial amputees | - | The study aimed to assess the effectiveness of virtual reality technologies in functional evaluations for individuals with upper limb amputation, specifically focusing on sensory feedback and motor performance using virtual prosthetic hands in virtual reality environments during activities of daily life tasks. | The study utilized virtual reality environments and virtual prosthetic hands controlled by intraneural microstimulation to assess sensory feedback, motor performance, and functional evaluations for individuals with upper limb amputation. | The study demonstrated that closed-loop control of a virtual prosthetic hand in a virtual reality environment, combined with sensory feedback through intraneural microstimulation, enabled individuals with upper limb amputations to successfully perform tasks related to texture identification, size and compliance discrimination, and activities of daily life. | Using virtual reality environments (VREs) with embedded physics engines and virtual prosthetic hands (VPHs) offers a cost-effective alternative to physical prosthetics, eliminates physical constraints and secondary sensory cues, provides repeatability and standardization, enables real-time analysis, enhances control and sensory feedback, and holds predictive value for physical prostheses. | CASP STROBE |
| Manabu Yoshimura et al. [49]. | 2020 | Quantitative research | 40 right-handed participants (20 male and 20 female) | - | 21–40 | The purpose of this study was to investigate the effectiveness of virtual reality (VR) technology in improving bilateral prosthetic control skills in individuals with upper limb amputation. | The study utilized a combination of the Box and Block Test (BBT), the bowknot task (BKT), and virtual reality (VR) technology to evaluate and improve bilateral prosthetic control skills in individuals with upper limb amputation. | The study found that using virtual reality (VR) for action observation (AO) was more effective in improving bilateral prosthetic control skills compared to a control group, and higher immersion scores in VR were associated with better acquisition of these skills. | Virtual reality environments enhance motor skill learning and provide increased motivation and engagement in rehabilitation therapy, integrating multiple sensory processes and offering personalized training with real-time feedback in a safe and controlled environment; these benefits transfer to real-world tasks and make rehabilitation more cost-effective and accessible. | CASP STROBE |
| Brian Kaluf et al. [50]. | 2021 | Scientific research | Seven participants | Congenital trans-radial amputation | 9–62 | The purpose of the study was to evaluate the ability of individuals with congenital trans-radial amputation to control a multi-DOF upper limb prosthesis using a pattern recognition control algorithm and to examine the effects of potential confounders such as age and previous prosthetic experience. | The study utilized the Coapt Engineering Complete Control handheld evaluation unit and graphical user interface software to assess myoelectric control in participants with congenital trans-radial amputation, allowing direct application of electrodes to the residual limb for calibration and evaluation of multi-DOF upper limb prosthesis control. | The study concluded that individuals with congenital trans-radial amputation could effectively control a multi-DOF upper limb prosthesis using a pattern recognition (PR) control algorithm, with comparable proficiency to their sound limb, and that age and previous prosthesis experience did not significantly impact performance. | The study included seven participants with congenital limb amputation, measuring calibration accuracy, completion rates, and differentiation between grip patterns for different levels of complexity. Results showed successful calibration with residual limbs, similar accuracy between sound and residual limbs, challenges in differentiating grips at the highest complexity level, and suggested a learning effect. These insights inform prosthetists in designing myoelectric prostheses for this population. | CASP STROBE |
| CA. Garske et al. [10]. | 2021 | Survey (questionnaire) | 26 (14 patients, 12 researchers) | 12 above- or below-the-elbow amputees; One shoulder amputee; One wrist amputee | Patients: 31–40, 41–50, 51–60, 61–70; Researchers: 20–30, 31–40, 41–50; | The purpose of the study is to determine the preferences, expectations, and views of both researchers and people with limb differences on game-based prosthetic training. | The study utilized a survey to gather insights from researchers and participants with limb differences, focusing on their preferences and expectations regarding game design and the incorporation of game-based prosthetic training tools. | The study concluded that game-based prosthetic training tools should prioritize ease of use, immersion in gameplay, and long-term engagement to enhance motivation and motor learning while also considering the preferences and needs of both users with limb differences and clinicians. | The study found a significant difference in user types between people with limb differences and researchers, with both groups significantly different from the control group. Participants with limb differences showed more similarity to the sample population in a previous study. Survey data revealed main themes of usability, training, game design, and challenges. Participants expected muscle development, improved prosthetic ability, and pain reduction. Game design focused on engagement and stakeholder involvement. Researchers mentioned challenges related to justification, study design, and knowledge sharing for Myo games. | STROBE |
| R.Nataraj et al. [51]. | 2022 | Quantitative research | 16 (12 males, four females) | - | 21 (±3) | The purpose of the study was to examine the effects of different control modes on performance and time perception in a virtual reach-to-grasp task, with the aim of understanding the potential implications for motor rehabilitation. | The study utilized a virtual reach-to-grasp task with variations in control modes, including speed changes, noise interference, and automation, to assess performance, performance efficiency, time perception (intentional binding), and explicit agency measures in participants’ dominant and non-dominant hands. | The study found significant variations in performance and perception (relative binding) of a reach-to-grasp task based on control modes and hand dominance, suggesting the potential for perception-based motor rehabilitation with virtual reality to enhance functional outcomes. | The study suggests that control modes, such as speed changes, noise interference, and automated assistance when adjusted for assistive devices, can improve performance and cognition during training. These modes significantly impacted performance and perception metrics, indicating their potential to enhance the effectiveness of virtual technologies in rehabilitation protocols. | CASP STROBE |
| Lucas EI Raghibi et al. [52] | 2022 | Quantitative research | 12 (one trans-radial amputee) | Trans-radial amputation | 18–40 | The purpose of the study was to assess the usability and performance of different virtualized prostheses in a VR environment and to determine the impact of VR testing on participants’ device preferences. | The study implemented a virtual reality environment to assess the usability and performance of different myoelectric prostheses, finding that participants’ perceived usability correlated with their objective performance in controlling the prostheses. | The developed VR system effectively facilitated the learning phase of myoelectric prostheses and allowed for a better-informed selection process. Participants’ perceived usability of the virtual prostheses correlated with their objective performance, and more than half of the participants changed their preferred device after testing in VR. | The study demonstrated that the VR environment effectively supported the learning phase of myoelectric prostheses, influenced participants’ device preferences based on perceived usability and other factors, and facilitated a more informed device selection process. | STROBE |
| Effie Segas et al. [53] | 2023 | Quantitative research | 29 (seven above-elbow amputees) | Elbow amputation | Group 1: 27.3 (±6) Group 2: 24.1 (±4.4) Group 3: 40.4 (±4.4) | The purpose of the study was to develop and evaluate a movement-based control system for prosthetic arms that allows users to reach and grasp objects in a natural and intuitive manner. | The study involved three experimental phases: familiarization, initial acquisition, and test, where participants familiarized themselves with the apparatus, performed natural arm movements to train their own artificial neural network (ANN), and compared performances using a hybrid arm controlled by the ANN and a virtual arm. | The study demonstrated that a movement-based control system, utilizing artificial neural networks and natural arm movements, enabled participants, including amputees, to achieve comparable reaching performance to their natural arm, highlighting the potential for daily life applications of this approach to prosthetic control. | The study showcased the effectiveness of virtual arm control methods, such as the Hybrid Arm control and Virtual Arm control, in achieving high success rates and efficient movement times comparable to participants’ own arm movements. Additionally, the use of a generic model trained on data from other participants proved promising, allowing new participants to achieve similar results. The validation with unilateral amputees further demonstrated the efficacy of these virtual technologies for individuals with limb loss, highlighting their positive treatment effects in terms of accuracy and efficiency. | CASP |
| Christopher L. Hunt [54] | 2023 | Quantitative research | 12 (seven males, five females) | - | 18–31 | The purpose of the study was to compare the effectiveness of augmented reality (AR) training with a loaded prosthesis to traditional muscle strengthening training in improving dexterous functionality and motor skills in individuals with upper limb loss. | The study used an augmented reality platform to train participants in object manipulation tasks using a virtual prosthesis and compared their performance to that of participants who underwent muscle strengthening exercises with a non-operational physical prosthesis. | The study found that training with an augmented reality prosthesis, with or without a load applied to the limb, led to greater improvement in dexterous functionality with a physical prosthesis compared to traditional muscle training alone. | The study demonstrated that VR training with physics simulation and robotic force interaction enhanced dexterous functionality with a physical prosthesis more than traditional muscle training or VR training without force interaction; AR training facilitated skill transference between augmented and physical reality tasks using EMG signals, limb loading improved proficiency in virtual object interactions, and objective measures of motor strategy execution were more indicative of real-world task performance than offline training accuracy. | CASP STROBE |
| CASP Questions | Rahman Davoodi and Gerald E. Loeb, 2012 [38] | Simon. et al., 2011 [37] | MA Powell. et al., 2013 [40] | RR Kaliki et al., 2013 [39] | NE Bunderson, 2014 [41] | D.Blana. et al., 2016 [42] | Kurzynski et al., 2017 [43] | N A Hashim. et al., 2018 [44] | DT.Kluger. et al., 2019 [48] | Effie Segas et al., 2023 [53] |
|---|---|---|---|---|---|---|---|---|---|---|
| Was there a clear statement of the aims of the research? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Is a qualitative methodology appropriate? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Was the research design appropriate to address the aims of the research? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Was the recruitment strategy appropriate to the aims of the research? | NA | NA | NA | NA | Yes | NA | Yes | Yes | Yes | No |
| Was the data collected in a way that addressed the research issue? | NA | Yes | Yes | Yes | Yes | NA | Yes | Yes | Yes | Yes |
| Has the relationship between the researcher and participants been adequately considered? | NA | No | No | No | No | NA | No | No | No | No |
| Have ethical issues been taken into consideration? | NA | No | No | No | Yes | NA | Yes | No | Yes | Yes |
| Was the data analysis sufficiently rigorous? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Is there a clear statement of findings? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Is the research sufficiently valuable? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Total score | 6 | 7 | 7 | 7 | 9 | 6 | 9 | 8 | 9 | 8 |
| STROBE Questions | NE Bunderson, 2014 [41] | C Prahm. et al., 2018 [45] | Brian Kaluf. et al., 2021 [50] | R.Nataraj et al., 2022 [51] | Lucas EI Raghibi et al., 2022 [52] | BN Perry et al., 2018 [46] | L Hargove. et al., 2018 [47] | BD.Winslow. et al., 2018 [11] | Manabu Yoshimura. et al., 2020 [49] | CA.Garske et al., 2021 [10] | Christopher L. Hunt et al., 2023 [54] |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Does the title and abstract clearly indicate the study’s design with commonly used terms? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Does the abstract provide an informative and balanced summary of what was executed and what was found? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Does the introduction explain the scientific background and rationale for the investigation being reported? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Were specific objectives stated, including any prespecified hypotheses? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Were key elements of the study design presented early in the paper? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Were the setting, locations, and relevant dates described, including periods of recruitment, exposure, follow-up, and data collection? | No | No | No | No | No | No | No | No | No | No | No |
| Did the methods give the eligibility criteria for, and the sources and methods of, the selection of participants? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Did the methods give matching criteria, and the number of exposed and unexposed, for the matched studies? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Were all outcomes, exposures, predictors, potential confounders, and effect modifiers clearly defined? | No | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
| Were sources of data and details of methods of assessment (measurement) given for each variable of interest? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Were there any efforts to address potential sources of bias? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Is there any explanation of how the study size was chosen? | No | No | No | No | No | No | No | No | No | No | No |
| Is there any explanation of how quantitative variables were handled in the analyses? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Were all statistical methods described, including those used as controls for confounding? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Were any methods used to examine subgroups and their interactions? | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Is there any explanation of how missing data were addressed? | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| For the cohort study, is there any explanation of how failures to follow up were addressed? For the case–control study, is there any explanation of how the matching of cases and controls was addressed? For the cross-sectional study, is there any description of the analytical methods taking account of the sampling strategy? | No | Yes | NA | NA | NA | NA | NA | NA | NA | NA | Yes |
| Was any sensitivity analysis described? | No | No | No | No | No | No | No | No | No | No | No |
| Was the number of individuals reported at each stage of the study—e.g., number of individuals potentially eligible, examined for eligibility, confirmed eligible, and included in the study, and number of individuals who completed the follow-up, and were analyzed? | No | No | No | No | No | No | No | No | No | No | No |
| Were reasons for non-participation stated at each stage? | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Was a flow diagram used to report the choices of individuals in each stage of the study? | No | No | No | No | No | No | No | No | No | No | No |
| Were characteristics of the study’s participants (e.g., demographic, clinical, social) and information on exposures and potential confounders given? | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Was the number of participants with missing data indicated for each variable of interest? | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Was a follow-up time summarized for the cohort study? | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| For the cohort study, was the number of outcome events or summary measures reported over time? For the case–control study, were the numbers in each exposure category or summary measures of exposure reported? For the cross-sectional study, was the number of outcome events or summary measures reported? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Were unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (e.g., 95% confidence interval) given? | No | No | No | Yes | Yes | No | No | No | No | No | No |
| Were the category boundaries being reported when continuous variables were categorized? | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Were other analyses reported—eg, the analyses of subgroups and interactions, and sensitivity analyses? | No | No | No | Yes | No | No | No | No | No | No | No |
| Were key results with reference to study objectives summarized? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Were limitations of the study discussed (and both the direction and magnitude of any potential bias), taking into account sources of potential bias or imprecisions? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Was a cautious overall interpretation of results given, considering objectives, limitations, multiplicity of analyses, results from similar studies, and other relevant evidence? | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Was the generalizability (external validity) of the study results discussed? | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Were the sources of funding and the role of the funders given for the present study and, if applicable, for the original study on which the present article is based? | Yes | Yes | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes |
| Total score | 15 | 18 | 18 | 20 | 18 | 19 | 19 | 19 | 19 | 19 | 20 |
References
- Shahsavari, H.; Matourypour, P.; Ghiyasvandian, S.; Ghorbani, A.; Bakhshi, F.; Mahmoudi, M.; Golestannejad, M. Upper Limb Amputation; Care Needs for Reintegration to Life: An Integrative Review. Int. J. Orthop. Trauma Nurs. 2020, 38, 100773. [Google Scholar] [CrossRef]
- Cordella, F.; Ciancio, A.L.; Sacchetti, R.; Davalli, A.; Cutti, A.G.; Guglielmelli, E.; Zollo, L. Literature Review on Needs of Upper Limb Prosthesis Users. Front. Neurosci. 2016, 10, 209. [Google Scholar] [CrossRef]
- Gallagher, P.; O’Donovan, M.-A.; Doyle, A.; Desmond, D. Environmental Barriers, Activity Limitations and Participation Restrictions Experienced by People with Major Limb Amputation. Prosthet. Orthot. Int. 2011, 35, 278–284. [Google Scholar] [CrossRef]
- Resnik, L.; Borgia, M.; Silver, B.; Cancio, J. Systematic Review of Measures of Impairment and Activity Limitation for Persons with Upper Limb Trauma and Amputation. Arch. Phys. Med. Rehabil. 2017, 98, 1863–1892.e14. [Google Scholar] [CrossRef]
- Jang, C.H.; Yang, H.S.; Yang, H.E.; Lee, S.Y.; Kwon, J.W.; Yun, B.D.; Choi, J.Y.; Kim, S.N.; Jeong, H.W. A Survey on Activities of Daily Living and Occupations of Upper Extremity Amputees. Ann. Rehabil. Med. 2011, 35, 907. [Google Scholar] [CrossRef]
- Bouwsema, H. Learning to Handle a Myoelectric Upper-Limb Prosthesis: The Development of an Evidence-Based Guideline for Training, [H. Bouwsema]; University of Groningen: Groningen, The Netherlands, 2014. [Google Scholar]
- Salminger, S.; Stino, H.; Pichler, L.H.; Gstoettner, C.; Sturma, A.; Mayer, J.A.; Szivak, M.; Aszmann, O.C. Current Rates of Prosthetic Usage in Upper-Limb Amputees-Have Innovations Had an Impact on Device Acceptance? Disabil. Rehabil. 2020, 44, 3708–3713. [Google Scholar] [CrossRef] [PubMed]
- Biddiss, E.; Beaton, D.; Chau, T. Consumer Design Priorities for Upper Limb Prosthetics. Disabil. Rehabil. Assist. Technol. 2007, 2, 346–357. [Google Scholar] [CrossRef] [PubMed]
- Weiss, P.L.; Jessel, A.S. Virtual Reality Applications to Work. Work 1998, 11, 277–293. [Google Scholar] [CrossRef]
- Garske, C.A.; Dyson, M.; Dupan, S.; Nazarpour, K. Perception of Game-Based Rehabilitation in Upper Limb Prosthetic Training: Survey of Users and Researchers. JMIR Serious Games 2021, 9, e23710. [Google Scholar] [CrossRef]
- Winslow, B.D.; Ruble, M.; Huber, Z. Mobile, Game-Based Training for Myoelectric Prosthesis Control. Front. Bioeng. Biotechnol. 2018, 6, 94. [Google Scholar] [CrossRef] [PubMed]
- Prahm, C.; Kayali, F.; Vujaklija, I.; Sturma, A.; Aszmann, O. Increasing Motivation, Effort and Performance through Game-Based Rehabilitation for Upper Limb Myoelectric Prosthesis Control. In Proceedings of the 2017 International Conference on Virtual Rehabilitation (ICVR), Montreal, QC, Canada, 19–22 June 2017; pp. 1–6. [Google Scholar]
- Melero, M.; Hou, A.; Cheng, E.; Tayade, A.; Lee, S.C.; Unberath, M.; Navab, N. Upbeat: Augmented Reality-Guided Dancing for Prosthetic Rehabilitation of Upper Limb Amputees. J. Healthc. Eng. 2019, 2019, 2163705. [Google Scholar] [CrossRef]
- Donnelley, C.A.; Shirley, C.; Von Kaeppler, E.P.; Hetherington, A.; Albright, P.D.; Morshed, S.; Shearer, D.W. Cost Analyses of Prosthetic Devices: A Systematic Review. Arch. Phys. Med. Rehabil. 2021, 102, 1404–1415.e2. [Google Scholar] [CrossRef]
- Ligthelm, E.J.; Wright, S.C.D. Lived Experience of Persons with an Amputation of the Upper Limb. Int. J. Orthop. Trauma Nurs. 2014, 18, 99–106. [Google Scholar] [CrossRef]
- Resnik, L.; Huang, H.H.; Winslow, A.; Crouch, D.L.; Zhang, F.; Wolk, N. Evaluation of EMG Pattern Recognition for Upper Limb Prosthesis Control: A Case Study in Comparison with Direct Myoelectric Control. J. Neuroeng. Rehabil. 2018, 15, 23. [Google Scholar] [CrossRef]
- Fougner, A.; Stavdahl, O.; Kyberd, P.J.; Losier, Y.G.; Parker, P.A. Control of Upper Limb Prostheses: Terminology and Proportional Myoelectric Control—A Review. IEEE Trans. Neural Syst. Rehabil. Eng. 2012, 20, 663–677. [Google Scholar] [CrossRef]
- Van Dijk, L.; Van Der Sluis, C.K.; Van Dijk, H.W.; Bongers, R.M. Task-Oriented Gaming for Transfer to Prosthesis Use. IEEE Trans. Neural Syst. Rehabil. Eng. 2016, 24, 1384–1394. [Google Scholar] [CrossRef] [PubMed]
- Bouwsema, H.; Van Der Sluis, C.K.; Bongers, R.M. Learning to Control Opening and Closing a Myoelectric Hand. Arch. Phys. Med. Rehabil. 2010, 91, 1442–1446. [Google Scholar] [CrossRef]
- Radhakrishnan, M.; Smailagic, A.; French, B.; Siewiorek, D.P.; Balan, R.K. Design and Assessment of Myoelectric Games for Prosthesis Training of Upper Limb Amputees. In Proceedings of the 2019 IEEE International Conference on Pervasive Computing and Communications Workshops (PerCom Workshops), Kyoto, Japan, 11–15 March 2019; pp. 151–157. [Google Scholar]
- Deans, S.; Burns, D.; McGarry, A.; Murray, K.; Mutrie, N. Motivations and Barriers to Prosthesis Users Participation in Physical Activity, Exercise and Sport: A Review of the Literature. Prosthet. Orthot. Int. 2012, 36, 260–269. [Google Scholar] [CrossRef]
- Yu, K.E.; Perry, B.N.; Moran, C.W.; Armiger, R.S.; Johannes, M.S.; Hawkins, A.; Stentz, L.; Vandersea, J.; Tsao, J.W.; Pasquina, P.F. Clinical Evaluation of the Revolutionizing Prosthetics Modular Prosthetic Limb System for Upper Extremity Amputees. Sci. Rep. 2021, 11, 954. [Google Scholar] [CrossRef]
- Cho, S.; Ku, J.; Cho, Y.K.; Kim, I.Y.; Kang, Y.J.; Jang, D.P.; Kim, S.I. Development of Virtual Reality Proprioceptive Rehabilitation System for Stroke Patients. Comput. Methods Programs Biomed. 2014, 113, 258–265. [Google Scholar] [CrossRef]
- Bashiri, A.; Ghazisaeedi, M.; Shahmoradi, L. The Opportunities of Virtual Reality in the Rehabilitation of Children with Attention Deficit Hyperactivity Disorder: A Literature Review. Korean J. Pediatr. 2017, 60, 337. [Google Scholar] [CrossRef]
- Perez-Marcos, D.; Bieler-Aeschlimann, M.; Serino, A. Virtual Reality as a Vehicle to Empower Motor-Cognitive Neurorehabilitation. Front. Psychol. 2018, 9, 2120. [Google Scholar] [CrossRef]
- Li, K.; Boyd, P.; Zhou, Y.; Ju, Z.; Liu, H. Electrotactile Feedback in a Virtual Hand Rehabilitation Platform: Evaluation and Implementation. IEEE Trans. Automat. Sci. Eng. 2019, 16, 1556–1565. [Google Scholar] [CrossRef]
- Engdahl, S.; Dhawan, A.; Bashatah, A.; Diao, G.; Mukherjee, B.; Monroe, B.; Holley, R.; Sikdar, S. Classification Performance and Feature Space Characteristics in Individuals With Upper Limb Loss Using Sonomyography. IEEE J. Transl. Eng. Health Med. 2022, 10, 2100311. [Google Scholar] [CrossRef]
- Wand, M.; Kristoffersen, M.B.; Franzke, A.W.; Schmidhuber, J. Analysis of Neural Network Based Proportional Myoelectric Hand Prosthesis Control. IEEE Trans. Biomed. Eng. 2022, 69, 2283–2293. [Google Scholar] [CrossRef]
- Putrino, D.; Wong, Y.T.; Weiss, A.; Pesaran, B. A Training Platform for Many-Dimensional Prosthetic Devices Using a Virtual Reality Environment. J. Neurosci. Methods 2015, 244, 68–77. [Google Scholar] [CrossRef]
- Gaballa, A.; Cavalcante, R.S.; Lamounier, E.; Soares, A.; Cabibihan, J.-J. Extended Reality “X-Reality” for Prosthesis Training of Upper-Limb Amputees: A Review on Current and Future Clinical Potential. IEEE Trans. Neural Syst. Rehabil. Eng. 2022, 30, 1652–1663. [Google Scholar] [CrossRef]
- Whittemore, R.; Knafl, K. The Integrative Review: Updated Methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D. Evaluations of the Uptake and Impact of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement and Extensions: A Scoping Review. Syst. Rev. 2017, 6, 263. [Google Scholar] [CrossRef]
- Caulley, L.; Cheng, W.; Catalá-López, F.; Whelan, J.; Khoury, M.; Ferraro, J.; Husereau, D.; Altman, D.G.; Moher, D. Citation Impact Was Highly Variable for Reporting Guidelines of Health Research: A Citation Analysis. J. Clin. Epidemiol. 2020, 127, 96–104. [Google Scholar] [CrossRef]
- Cuschieri, S. The STROBE Guidelines. Saudi J. Anaesth. 2019, 13, 31. [Google Scholar] [CrossRef] [PubMed]
- Brice, R.; Casp Checklists. CASP-Critical Appraisal Skills Programme. Available online: https://casp-uk.net/how-to-use-checklist/ (accessed on 8 August 2023).
- Simon, A.M.; Hargrove, L.J.; Lock, B.A.; Kuiken, T.A. Target Achievement Control Test: Evaluating Real-Time Myoelectric Pattern-Recognition Control of Multifunctional Upper-Limb Prostheses. J. Rehabil. Res. Dev. 2011, 48, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Davoodi, R.; Loeb, G.E. Development of a Physics-Based Target Shooting Game to Train Amputee Users of Multijoint Upper Limb Prostheses. Presence Teleoperators Virt. Environ. 2012, 21, 85–95. [Google Scholar] [CrossRef]
- Kaliki, R.R.; Davoodi, R.; Loeb, G.E. Evaluation of a Noninvasive Command Scheme for Upper-Limb Prostheses in a Virtual Reality Reach and Grasp Task. IEEE Trans. Biomed. Eng. 2013, 60, 792–802. [Google Scholar] [CrossRef]
- Powell, M.A.; Thakor, N.V. A Training Strategy for Learning Pattern Recognition Control for Myoelectric Prostheses. J. Prosthet. Orthot. 2013, 25, 30–41. [Google Scholar] [CrossRef] [PubMed]
- Bunderson, N.E. Real-Time Control of an Interactive Impulsive Virtual Prosthesis. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Blana, D.; Kyriacou, T.; Lambrecht, J.M.; Chadwick, E.K. Feasibility of Using Combined EMG and Kinematic Signals for Prosthesis Control: A Simulation Study Using a Virtual Reality Environment. J. Electromyogr. Kinesiol. 2016, 29, 21–27. [Google Scholar] [CrossRef]
- Kurzynski, M.; Jaskolska, A.; Marusiak, J.; Wolczowski, A.; Bierut, P.; Szumowski, L.; Witkowski, J.; Kisiel-Sajewicz, K. Computer-Aided Training Sensorimotor Cortex Functions in Humans before the Upper Limb Transplantation Using Virtual Reality and Sensory Feedback. Comput. Biol. Med. 2017, 87, 311–321. [Google Scholar] [CrossRef]
- Hashim, N.A.; Abd Razak, N.A.; Gholizadeh, H.; Abu Osman, N.A. Video Game-Based Rehabilitation Approach for Individuals Who Have Undergone Upper Limb Amputation: Case-Control Study. JMIR Serious Games 2021, 9, e17017. [Google Scholar] [CrossRef] [PubMed]
- Prahm, C.; Kayali, F.; Sturma, A.; Aszmann, O. PlayBionic: Game-Based Interventions to Encourage Patient Engagement and Performance in Prosthetic Motor Rehabilitation. PMR 2018, 10, 1252–1260. [Google Scholar] [CrossRef]
- Perry, B.N.; Armiger, R.S.; Yu, K.E.; Alattar, A.A.; Moran, C.W.; Wolde, M.; McFarland, K.; Pasquina, P.F.; Tsao, J.W. Virtual Integration Environment as an Advanced Prosthetic Limb Training Platform. Front. Neurol. 2018, 9, 785. [Google Scholar] [CrossRef] [PubMed]
- Hargrove, L.; Miller, L.; Turner, K.; Kuiken, T. Control within a Virtual Environment Is Correlated to Functional Outcomes When Using a Physical Prosthesis. J. Neuroeng. Rehabil. 2018, 15, 60. [Google Scholar] [CrossRef] [PubMed]
- Kluger, D.T.; Joyner, J.S.; Wendelken, S.M.; Davis, T.S.; George, J.A.; Page, D.M.; Hutchinson, D.T.; Benz, H.L.; Clark, G.A. Virtual Reality Provides an Effective Platform for Functional Evaluations of Closed-Loop Neuromyoelectric Control. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 876–886. [Google Scholar] [CrossRef]
- Yoshimura, M.; Kurumadani, H.; Hirata, J.; Osaka, H.; Senoo, K.; Date, S.; Ueda, A.; Ishii, Y.; Kinoshita, S.; Hanayama, K.; et al. Virtual Reality-Based Action Observation Facilitates the Acquisition of Body-Powered Prosthetic Control Skills. J. Neuroeng. Rehabil. 2020, 17, 113. [Google Scholar] [CrossRef] [PubMed]
- Kaluf, B.; Gart, M.S.; Loeffler, B.J.; Gaston, G. Evaluating the Ability of Congenital Upper Extremity Amputees to Control a Multi-Degree of Freedom Myoelectric Prosthesis. J. Hand Surg. 2021, 47, 1019. [Google Scholar] [CrossRef] [PubMed]
- Nataraj, R.; Sanford, S.; Liu, M.; Harel, N.Y. Hand Dominance in the Performance and Perceptions of Virtual Reach Control. Acta Psychol. 2022, 223, 103494. [Google Scholar] [CrossRef]
- Raghibi, L.E.; Muhoza, A.P.; Evrard, J.; Ghazi, H.; Van Oldeneel Tot Oldenzeel, G.; Sonneville, V.; Macq, B.; Ronsse, R. Virtual Reality Can Mediate the Learning Phase of Upper Limb Prostheses Supporting a Better-Informed Selection Process. J. Multimodal User Interfaces 2023, 17, 33–46. [Google Scholar] [CrossRef]
- Segas, E.; Mick, S.; Leconte, V.; Dubois, O.; Klotz, R.; Cattaert, D.; De Rugy, A. Intuitive Movement-Based Prosthesis Control Enables Arm Amputees to Reach Naturally in Virtual Reality. eLife 2023, 12, RP87317. [Google Scholar] [CrossRef] [PubMed]
- Hunt, C.L.; Sun, Y.; Wang, S.; Shehata, A.W.; Hebert, J.S.; Gonzalez-Fernandez, M.; Kaliki, R.R.; Thakor, N.V. Limb Loading Enhances Skill Transfer between Augmented and Physical Reality Tasks during Limb Loss Rehabilitation. J. NeuroEng. Rehabil. 2023, 20, 16. [Google Scholar] [CrossRef] [PubMed]
- Baur, K.; Schättin, A.; de Bruin, E.D.; Riener, R.; Duarte, J.E.; Wolf, P. Trends in Robot-Assisted and Virtual Reality-Assisted Neuromuscular Therapy: A Systematic Review of Health-Related Multiplayer Games. J. NeuroEng. Rehabil. 2018, 15, 107. [Google Scholar] [CrossRef]
- Lohse, K.; Shirzad, N.; Verster, A.; Hodges, N.; Van der Loos, H.F.M. Video Games and Rehabilitation: Using Design Principles to Enhance Engagement in Physical Therapy. J. Neurol. Phys. Ther. 2013, 37, 166–175. [Google Scholar] [CrossRef]
- Sluijs, E.M.; Knibbe, J.J. Patient Compliance with Exercise: Different Theoretical Approaches to Short-Term and Long-Term Compliance. Patient Educ. Couns. 1991, 17, 191–204. [Google Scholar] [CrossRef]
- De La Rosa, R.; Alonso, A.; De La Rosa, S.; Abasolo, D. Myo-Pong: A Neuromuscular Game for the UVa-Neuromuscular Training System Platform. In Proceedings of the 2008 Virtual Rehabilitation; IEEE: Vancouver, BC, Canada, 2008; p. 61. [Google Scholar]
- Garcia-Hernandez, N.; Garza-Martinez, K.; Parra-Vega, V. Electromyography Biofeedback Exergames to Enhance Grip Strength and Motivation. Games Health J. 2018, 7, 75–82. [Google Scholar] [CrossRef]
- Anderson, F.; Bischof, W.F. Augmented Reality Improves Myoelectric Prosthesis Training. Int. J. Disabil. Hum. Dev. 2014, 13, 349–354. [Google Scholar] [CrossRef]
- Hu, F.; Lu, J.; Zhang, T. (Eds.) Virtual Reality Enhanced Robotic Systems for Disability Rehabilitation; Advances in Medical Technologies and Clinical Practice; IGI Global: Hershey, PA, USA, 2016; ISBN 978-1-4666-9740-9. [Google Scholar]
- Oppenheim, H.; Armiger, R.S.; Vogelstein, R.J. WiiEMG: A Real-Time Environment for Control of the Wii with Surface Electromyography. In Proceedings of the 2010 IEEE International Symposium on Circuits and Systems, Paris, France, 30 May–2 June 2010; pp. 957–960. [Google Scholar]
- Hargrove, L.; Losier, Y.; Lock, B.; Englehart, K.; Hudgins, B. A Real-Time Pattern Recognition Based Myoelectric Control Usability Study Implemented in a Virtual Environment. In Proceedings of the 2007 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 22–26 August 2007; pp. 4842–4845. [Google Scholar]
- Kuiken, T.A.; Li, G.; Lock, B.A.; Lipschutz, R.D.; Miller, L.A.; Stubblefield, K.A.; Englehart, K.B. Targeted Muscle Reinnervation for Real-Time Myoelectric Control of Multifunction Artificial Arms. JAMA 2009, 301, 619–628. [Google Scholar] [CrossRef]
- Anderson, J.G. Social, Ethical and Legal Barriers to e-Health. Int. J. Med. Inform. 2007, 76, 480–483. [Google Scholar]
- Caro, J.J.; Brazier, J.E.; Karnon, J.; Kolominsky-Rabas, P.; McGuire, A.J.; Nord, E.; Schlander, M. Determining Value in Health Technology Assessment: Stay the Course or Tack Away? Pharmacoeconomics 2019, 37, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Wasiak, R.; Young, A.E.; Roessler, R.T.; McPherson, K.M.; van Poppel, M.N.M.; Anema, J.R. Measuring Return to Work. J. Occup. Rehabil. 2007, 17, 766–781. [Google Scholar] [CrossRef] [PubMed]
- Tatla, S.K.; Shirzad, N.; Lohse, K.R.; Virji-Babul, N.; Hoens, A.M.; Holsti, L.; Li, L.C.; Miller, K.J.; Lam, Y. Therapists’ Perceptions of Social Media and Video Game Technologies in Upper Limb Rehabilitation. JMIR Serious Games 2015, 10, e2. [Google Scholar] [CrossRef]
- Godwin, K.M.; Wasserman, J.; Ostwald, S.K. Cost Associated with Stroke: Outpatient Rehabilitative Services and Medication. Top. Stroke Rehabil. 2011, 18, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Lloréns, R.; Noé, E.; Colomer, C.; Alcañiz, M. Effectiveness, Usability, and Cost-Benefit of a Virtual Reality–Based Telerehabilitation Program for Balance Recovery after Stroke: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2015, 96, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Franzò, M.; Pica, A.; Pascucci, S.; Marinozzi, F.; Bini, F. Hybrid System Mixed Reality and Marker-Less Motion Tracking for Sports Rehabilitation of Martial Arts Athletes. Appl. Sci. 2023, 13, 2587. [Google Scholar] [CrossRef]
| Strategy | PubMed | Cochrane Library | EMBASE | Web of Science | Scopus |
|---|---|---|---|---|---|
| ((Upper limb amput*)) OR ((Hand amput*)) OR ((Upper extremity amput*)) AND ((Prosthetic training)) OR ((Rehabilitation)) AND ((Control)) AND ((Virtual reality)) NOT ((Stroke)) NOT ((Parkinson)) NOT ((Cerebral palsy)) | 859 | 843 trials | 1209 | 9113 (6757 articles, 1016 reviews, 302 trials) | 679 |
| ((Upper limb amput*)) OR ((Hand amput*)) OR ((Upper extremity amput*)) AND ((Prosthetic training)) OR ((Rehabilitation)) AND ((Control)) AND ((Video game)) NOT ((Stroke)) NOT ((Parkinson)) NOT ((Cerebral palsy)) | 542 | 638 trials | 418 | 7927 (6014 articles, 845 reviews, 265 trials) | 91 |
| ((Reintegration to normal live)) OR ((Reintegration to normal living)) AND ((Upper)) AND ((Amputation)) NOT ((Stroke)) NOT ((Parkinson)) NOT ((Cerebral palsy)) | 3 | 51 trials | 1 | 160 (139 articles, 7 reviews, 7 trials) | 23 |
| ((Reintegration to occupation)) OR ((Reintegration to work)) AND ((Upper)) AND ((Amputation)) NOT ((Stroke)) NOT ((Parkinson)) NOT ((Cerebral palsy)) | 7 | 61 trials | 9 | 122 (106 articles, 11 reviews, 4 trials) | 95 |
| ((Reintegration to daily life)) OR ((Self-care)) AND ((Upper)) AND ((Amputation)) NOT ((Stroke)) NOT ((Parkinson)) NOT ((Cerebral palsy)) | 42 | 10,786 trials | 34 | 283 (241 articles, 34 reviews, 7 trials) | 150 |
| Total | 1453 | 12,379 | 1671 | 17,605 | 1038 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, X.; Zhang, D.; Miao, K.; Guo, Y.; Jiang, X.; Zhang, X.; Jia, F.; Tang, H.; Dai, C. A Review on the Usability, Flexibility, Affinity, and Affordability of Virtual Technology for Rehabilitation Training of Upper Limb Amputees. Bioengineering 2023, 10, 1301. https://doi.org/10.3390/bioengineering10111301
Liu X, Zhang D, Miao K, Guo Y, Jiang X, Zhang X, Jia F, Tang H, Dai C. A Review on the Usability, Flexibility, Affinity, and Affordability of Virtual Technology for Rehabilitation Training of Upper Limb Amputees. Bioengineering. 2023; 10(11):1301. https://doi.org/10.3390/bioengineering10111301
Chicago/Turabian StyleLiu, Xiangyu, Di Zhang, Ke Miao, Yao Guo, Xinyu Jiang, Xi Zhang, Fumin Jia, Hao Tang, and Chenyun Dai. 2023. "A Review on the Usability, Flexibility, Affinity, and Affordability of Virtual Technology for Rehabilitation Training of Upper Limb Amputees" Bioengineering 10, no. 11: 1301. https://doi.org/10.3390/bioengineering10111301
APA StyleLiu, X., Zhang, D., Miao, K., Guo, Y., Jiang, X., Zhang, X., Jia, F., Tang, H., & Dai, C. (2023). A Review on the Usability, Flexibility, Affinity, and Affordability of Virtual Technology for Rehabilitation Training of Upper Limb Amputees. Bioengineering, 10(11), 1301. https://doi.org/10.3390/bioengineering10111301