
Physical Activity in the Elderly and Frailty Syndrome: A Retrospective Study in Primary Care

 ,
, 
Abstract
1. Introduction
- -
- -
- The clinical model, developed by the Canadian team at Rockwood, based on multidimensional frailty, taking into account physical, psychological and social factors, and enabling researchers to obtain a frailty index [8].
2. Patients and Methods
2.1. Type of Study
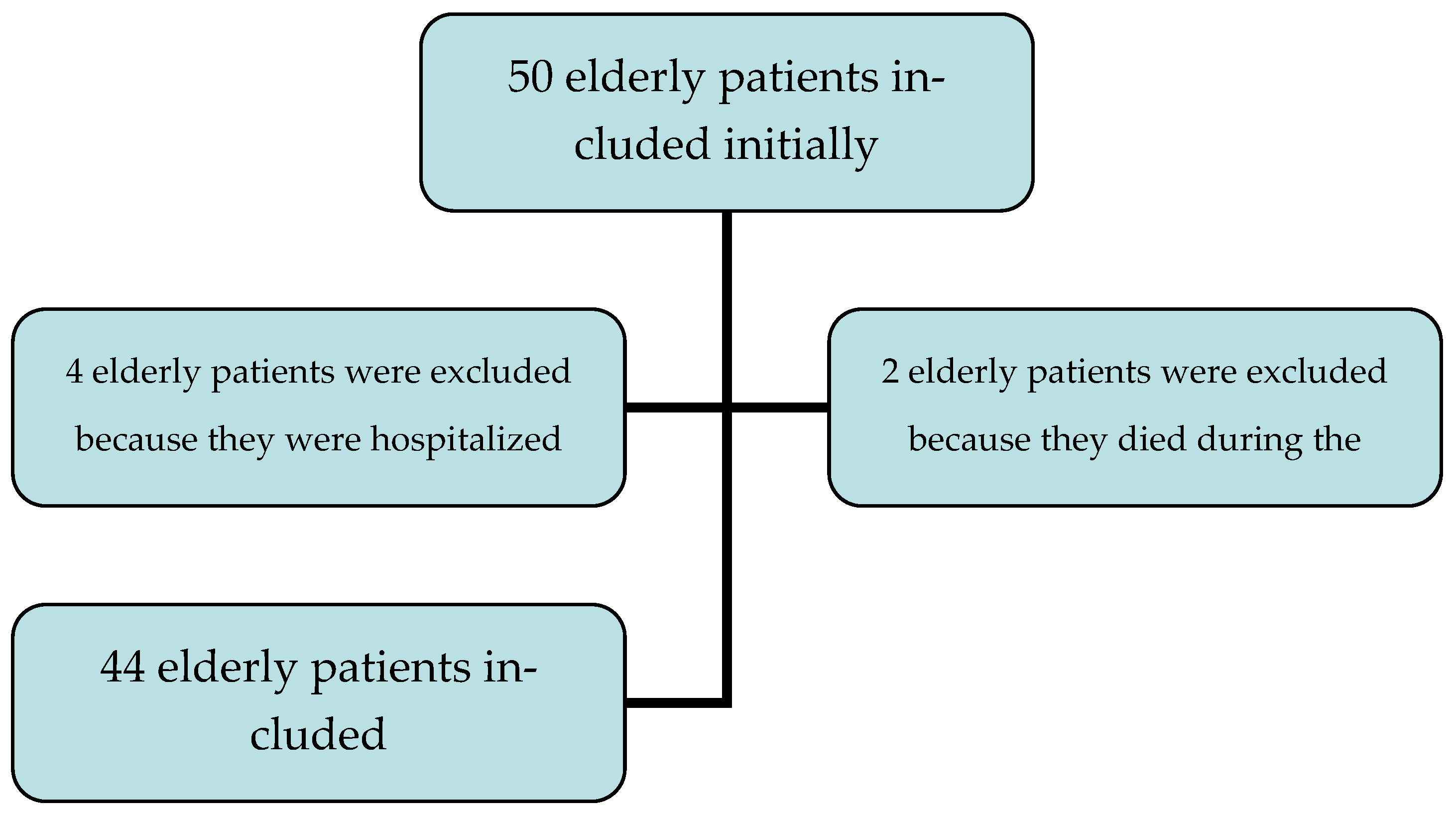
2.2. Inclusion and Exclusion Criteria
2.3. Data Collected
- -
- Sex, age, reason for consultation, medical and surgical history, marital status, professional status during their working life, presence or absence of addictive behaviors.
- -
- Frailty was measured by the mSEGA grid. For the mSEGA score [9], we separated the patients into three groups: non-frail patients if the score was less than 8, frail patients if the score was between 8 and 11, and very frail patients if the score was greater than 11.
- -
- The biometric level was appreciated by the use of arm circumference (normal value > 21 cm), calf circumference (normal value >31 cm), height (using heel/knee height when standing measurements were impossible), and weight. From these values, we were able to calculate the Body Mass Index (BMI) from the formula: weight (in kg)/(size2) (in m), and whose interpretation followed the values established by HAS (Haute Autorité des Soins): normal BMI if < or = 24.9 kg/m2. We also carried out the Mini Nutritional Assessment (MNA), which enabled us to define whether the patients were: not malnourished with a score > 24, at risk of malnutrition with a score between 17 and 24 or malnourished with a score < 17.
- -
- Data from the Comprehensive Geriatric Assessment (CGA) were also collected, with the single-leg support test, which was defined as positive if the single-leg support was > or equal to 5 s. Dependence was assessed using the Katz and Lawton scales (ADL and IADL). Memory disorders according to the Mini Mental State Examination (MMSE) score were found in the medical file.
- -
- The sedentary lifestyle and physical activity test was studied using the Ricci–Gagnon (R&G) scale, with 2 distinct groups: inactive (score < 18) and active (score ≥ 18).
- -
- From a biological point of view, we noted the following values dating from less than 6 months within the clinic visit: albumin (hypoalbuminemia was defined by albuminemia < 35 g/L), creatinine (kidney failure was defined by a glomerular filtration rate (GFR) < 60 mL/min/1.73 m2), hemoglobin (Hb) (anemia was defined by hemoglobinemia < 12 g/dL), vitamin D (a vitamin D deficiency corresponded to a level < 30 ng/mL).
2.4. Statistical Analysis
2.5. Administrative Elements:
3. Results
4. Discussion
Limits
5. Conclusions
- -
- Geriatric screening focused on frailty;
- -
- An evaluation of physical activity using the Ricci–Gagnon questionnaire.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hupin, D. Relation entre l’Activité Physique des Personnes Agées et le Risque de Mortalité: Revue de Littérature et Méta-analyse. Thèse d’exercice, Université Jean Monnet, Saint-Etienne, France, 2013. [Google Scholar]
- De Labra, C.; Guimaraes-Pinheiro, C.; Maseda, A.; Lorenzo, T.; Millán-Calenti, J.C. Effects of physical exercise interventions in frail older adults: A systematic review of randomized controlled trials. BMC Geriatr. 2015, 15, 1. [Google Scholar] [CrossRef] [PubMed]
- DeSouza, C.A.; Shapiro, L.F.; Clevenger, C.M.; Dinenno, F.A.; Monahan, K.D.; Tanaka, H.; Seals, D.R. Regular Aerobic Exercise Prevents and Restores Age-Related Declines in Endothelium-Dependent Vasodilation in Healthy Men. Circulation 2000, 102, 1351–1357. [Google Scholar] [CrossRef] [PubMed]
- Kelley, G.A.; Kelley, K.S.; Tran, Z. Exercise and bone mineral density in men: A meta-analysis. J. Appl. Physiol. 2000, 88, 1730–1736. [Google Scholar] [CrossRef] [PubMed]
- Lautenschlager, N.T.; Cox, K.L.; Flicker, L.; Foster, J.K.; Bockxmeer, F.M.V.; Xiao, J.; Greenop, K.R.; Almeida, O.P. Effect of Physical Activity on Cognitive Function in Older Adults at Risk for Alzheimer Disease. JAMA 2008, 300, 1027. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef] [PubMed]
- Vellas, B.; Cestac, P.; Morley, J.E. Implementing frailty into clinical practice: We cannot wait. J. Nutr. Health Aging 2012, 16, 599–600. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Oubaya, N.; Mahmoudi, R.; Jolly, D.; Zulfiqar, A.-A.; Quignard, E.; Cunin, C.; Nazeyrollas, P.; Novella, J.-L.; Dramé, M. Screening for frailty in elderly subjects living at home: Validation of the modified Short Emergency Geriatric Assessment (SEGAm) instrument. J. Nutr. Heal. Aging 2014, 18, 757–764. [Google Scholar] [CrossRef]
- Pavy, B.; Tisseau, A.; Caillon, M. Le patient coronarien six mois après la réadaptation cardiaque: Recherche sur l’évaluation de la réadaptation (étude RER). Ann. Cardiol. Angéiol. 2011, 60, 252–258. [Google Scholar] [CrossRef]
- Tardieu, É.; Mahmoudi, R.; Novella, J.L.; Oubaya, N.; Blanchard, F.; Jolly, D.; Drame, M. External validation of the short emergency geriatric assessment (SEGA) instrument on the SAFES cohort. Geriatr. Psychol. Neuropsychiatr. Vieil. 2016, 14, 49–55. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Heinen, M.; Borm, G.; van der Vleuten, C.; Evers, A.; Oostendorp, R.A.; van Achterberg, T. The Lively Legs self-management programme increased physical activity and reduced wound days in leg ulcer patients: Results from a randomized controlled trial. Int. J. Nurs. Stud. 2012, 49, 151–161. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, I.S.; Silva, C.D.F.R.; Ohara, D.G.; Matos, A.P.; Pinto, A.C.P.N.; Pegorari, M.S. Association between frailty syndrome and sedentary behavior among community-dwelling older adults in the Amazon region: A cross-sectional study. Sao Paulo Med. J. 2021, 139, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, R.N.; Koehler, K.M.; Gallagher, D.; Romero, L.; Heymsfield, S.B.; Ross, R.R.; Garry, P.J.; Lindeman, R.D. Epidemiology of Sarcopenia among the Elderly in New Mexico. Am. J. Epidemiol. 1998, 147, 755–763. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef]
- Santilli, V.; Bernetti, A.; Mangone, M.; Paoloni, M. Clinical definition of sarcopenia. Clin. Cases Miner. Bone Metab. 2014, 11, 3. [Google Scholar] [CrossRef]
- Bauer, J.M.; Sieber, C.C. Sarcopenia and frailty: A clinician’s controversial point of view. Exp. Gerontol. 2008, 43, 674–678. [Google Scholar] [CrossRef]
- Landi, F.; Russo, A.; Liperoti, R.; Pahor, M.; Tosato, M.; Capoluongo, E.; Bernabei, R.; Onder, G. Midarm muscle circumference, physical performance and mortality: Results from the aging and longevity study in the Sirente geographic area (ilSIRENTE study). Clin. Nutr. 2010, 29, 441–447. [Google Scholar] [CrossRef]
- Mijnarends, D.M.; Koster, A.; Schols, J.M.G.A.; Meijers, J.M.M.; Halfens, R.J.G.; Gudnason, V.; Eiriksdottir, G.; Siggeirsdottir, K.; Sigurdsson, S.; Jónsson, P.V.; et al. Physical activity and incidence of sarcopenia: The population-based AGES—Reykjavik Study. Age Ageing 2016, 45, 614–620. [Google Scholar] [CrossRef]
- Peterson, M.D.; Sen, A.; Gordon, P.M. Influence of resistance exercise on lean body mass in aging adults: A meta-analysis. Med. Sci. Sports Exerc. 2011, 43, 249. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Landi, F.; Schneider, S.M.; Zúñiga, C.; Arai, H.; Boirie, Y.; Chen, L.-K.; Fielding, R.A.; Martin, F.C.; Michel, J.-P.; et al. Prevalence of and interventions for sarcopenia in ageing adults: A systematic review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS). Age Ageing 2014, 43, 748–759. [Google Scholar] [CrossRef] [PubMed]
- Van de Rest, O.; van der Zwaluw, N.L.; Tieland, M.; Adam, J.J.; Hiddink, G.J.; van Loon, L.J.; de Groot, L.C. Effect of resistance-type exercise training with or without protein supplementation on cognitive functioning in frail and pre-frail elderly: Secondary analysis of a randomized, double-blind, placebo-controlled trial. Mech. Ageing Develop. 2014, 136, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.; Ying, Z.; Gomez-Pinilla, F. Docosahexaenoic acid dietary supplementation enhances the effects of exercise on synaptic plasticity and cognition. Neuroscience 2008, 155, 751–759. [Google Scholar] [CrossRef]
- Bobeuf, F.; Labonte, M.; Dionne, I.J.; Khalil, A. Combined effect of antioxidant supplementation and resistance training on oxidative stress markers, muscle and body composition in an elderly population. J. Nutr. Health Aging 2011, 15, 883–889. [Google Scholar] [CrossRef] [PubMed]
- Freiberger, E.; Goisser, S.; Porzel, S.; Volkert, D.; Kemmler, W.; Sieber, C.; Bollheimer, C. Sarcopenic obesity and complex interventions with nutrition and exercise in community-dwelling older persons—A narrative review. Clin. Interv. Aging 2015, 10, 1267–1282. [Google Scholar] [CrossRef]
- Welch, A.A. Nutritional influences on age-related skeletal muscle loss. Proc. Nutr. Soc. 2014, 73, 16–33. [Google Scholar] [CrossRef]
- Ng, T.P.; Feng, L.; Nyunt, M.S.Z.; Feng, L.; Niti, M.; Tan, B.Y.; Chan, G.; Khoo, S.A.; Chan, S.M.; Yap, P.; et al. Nutritional, Physical, Cognitive, and Combination Interventions and Frailty Reversal Among Older Adults: A Randomized Controlled Trial. Am. J. Med. 2015, 128, 1225–1236.e1. [Google Scholar] [CrossRef]
- Buntinx, F.; Niclaes, L.; Suetens, C.; Jans, B.; Mertens, R.; van den Akker, M. Evaluation of Charlson’s comorbidity index in elderly living in nursing homes. J. Clin. Epidemiol. 2002, 55, 1144–1147. [Google Scholar] [CrossRef]
- Lin, C.Y.; Gentile, N.L.; Bale, L.; Rice, M.; Lee, E.S.; Ray, L.S.; Ciol, M.A. Implementation of a Physical Activity Vital Sign in Primary Care: Associations Between Physical Activity, Demographic Characteristics, and Chronic Disease Burden. Prev. Chronic Dis. 2022, 19, E33. [Google Scholar] [CrossRef]
- Vuillemin, A.; Speyer, E.; Simon, C.; Ainsworth, B.; Paineau, D. Revue critique des questionnaires d’activité physique administrés en population française et perspectives de développement. Cah. Nutr. Diététique 2012, 47, 234–241. [Google Scholar] [CrossRef]
- Réseaux de Santé de Chamapgne-Ardenne. Les Parcours Sport Santé du RSSBE en Champagne-Ardenne. Available online: http://reseaux-sante-ca.org/spip.php?article779&var_mode=calcul (accessed on 16 December 2016).


{kind=link}
| n = 44 | ||
|---|---|---|
| Sex, n (%) | Female | 26 (59.1) |
| Male | 18 (40.9) | |
| Age, m | 75 (65–93) | |
| Charlson, out of 24, m (sd) | 2.8 (0–7) | |
| Marital status | ||
| Married | 30 (68%) | |
| Divorced | 4 (9%) | |
| Widowed | 10 (23%) | |
| Addictive behaviors | ||
| Tobacco | 16 (36.36%) | |
| Alcohol | 30 (68.18%) | |
| Medical history | ||
| Arthrosis | 27 (61.4%) | |
| Hypertension | 22 (50%) | |
| Obesity | 14 (31.8%) | |
| Pulmonary disease | 12 (27.2%) | |
| Heart deficiency (defined by left ventricular ejection fraction <50%) | 10 (22.7%) | |
| Diabetes | 9 (20.45%) | |
| Atrial fibrillation | 8 (18.2%) | |
| Neoplasms | 6 (13.6%) | |
| Prothesis | 6 (13.6%) | |
| Stroke | 4 (9%) | |
| Renal deficiency (defined by a glomerular filtration rate (GFR) <60 mL/min/1.73 m2) | 4 (9%) | |
| Cognitive disorders | 3 (6.8%) | |
| Nutritional status | ||
| Undernourishment according to albumin | 3 (8.82%) | |
| Undernourishment according to Body Mass Index | 11 (25%) | |
| Undernourishment according to Mini Nutritional Assessment | 6 (13.64%) | |
| Biological measurement | ||
| Anemia | 1 (6.3%) | |
| Vitamin D deficiency | 34 (85%) | |
| Frailty status | ||
| Modified SEGA | 7 (15.91) | |
| Inactive Physical status | ||
| According to Ricci–Gagnon scale | 10 (22.73%) | |
| Collective sport activity | 6 (13.64%) |
| Parameters | n | Mean | Standard Deviation | Median | Minimum | Maximum |
|---|---|---|---|---|---|---|
| Age (years) | 44 | 75.0 | 7.1 | 73.5 | 65.0 | 93.0 |
| Weight (kg) | 44 | 72.5 | 13.6 | 70.5 | 47 | 117 |
| Height (cm) | 44 | 162.7 | 8.5 | 163 | 145 | 180 |
| BMI (kg/m2) | 44 | 27.4 | 5.1 | 26.2 | 20.8 | 43 |
| Arm Circumference (cm) | 44 | 31.6 | 3.8 | 31.5 | 23.5 | 43.5 |
| Thigh Circumference (cm) | 44 | 53.5 | 5.6 | 53.5 | 43.5 | 69.5 |
| Calf Circumference (cm) | 44 | 36.6 | 2.9 | 35.8 | 31 | 44.5 |
| Abdominal Perimeter (cm) | 44 | 101.6 | 11.7 | 101.5 | 81 | 138.5 |
| Charlson | 44 | 2.8 | 1.8 | 2 | 0 | 7 |
| MMSE | 44 | 25.4 | 3.3 | 26 | 18 | 30 |
| mSEGA | 44 | 5.3 | 2.9 | 5.0 | 1.0 | 12.0 |
| IADL | 44 | 6.7 | 1.6 | 7 | 1 | 8 |
| ADL | 44 | 5.8 | 0.4 | 6 | 4 | 6 |
| Ricci Gagnon | 44 | 22.6 | 6.3 | 22 | 9 | 34 |
| Hb (g/dL) (missing data for one patient) | 43 | 14 | 1.3 | 14.2 | 11.2 | 16.8 |
| Glomerular filtration rate (mL/min/1.73 m2) | 44 | 76.5 | 21.2 | 78.5 | 16 | 133 |
| Albumin (g /L) (missing data for 10 patients) | 34 | 38.4 | 3.2 | 38 | 31.3 | 45 |
| Vitamin D (ng/mL) (missing data for 10 patients) | 30 | 20.6 | 9 | 20 | 5 | 46 |
| MNA | 44 | 26.2 | 2.3 | 26.5 | 20 | 30 |
| Parameter Correlation | Frailty According to mSEGA |
| Inactive according to Ricci–Gagnon | p = 0.68 |
| Pathological monopodal support test | p = 0.083 |
| Collective sport | p = 0.25 |
| Undernourishment BMI | p = 0.47 |
| Undernourishment MNA | p = 0.21 |
| Undernourishment Albumin | p = 0.002 |
| Charlson score | p = 0.07 |
| MMSE | p = 0.48 |
| Parameter Correlation | Inactive According to Ricci–Gagnon |
| Pathological monopodal support test | p = 0.014 |
| Age | p = 0.06 |
| Undernourishment BMI | p = 0.68 |
| Undernourishment MNA | p = 0.0057 |
| Undernourishment Albumin | p = 0.3 |
| Charlson score | p = 0.027 |
| Vitamin D deficiency | p = 0.61 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zulfiqar, A.-A.; Habchi, H.; Habchi, P.; Dembele, I.A.; Andres, E. Physical Activity in the Elderly and Frailty Syndrome: A Retrospective Study in Primary Care. Medicines 2022, 9, 51. https://doi.org/10.3390/medicines9100051
Zulfiqar A-A, Habchi H, Habchi P, Dembele IA, Andres E. Physical Activity in the Elderly and Frailty Syndrome: A Retrospective Study in Primary Care. Medicines. 2022; 9(10):51. https://doi.org/10.3390/medicines9100051
Chicago/Turabian StyleZulfiqar, Abrar-Ahmad, Habib Habchi, Perla Habchi, Ibrahima Amadou Dembele, and Emmanuel Andres. 2022. "Physical Activity in the Elderly and Frailty Syndrome: A Retrospective Study in Primary Care" Medicines 9, no. 10: 51. https://doi.org/10.3390/medicines9100051
APA StyleZulfiqar, A.-A., Habchi, H., Habchi, P., Dembele, I. A., & Andres, E. (2022). Physical Activity in the Elderly and Frailty Syndrome: A Retrospective Study in Primary Care. Medicines, 9(10), 51. https://doi.org/10.3390/medicines9100051