
Qigong Exercise May Reduce Serum TNF-α Levels and Improve Sleep in People with Parkinson’s Disease: A Pilot Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Intervention
2.3. Serum Sampling
2.4. Biomarker Assays
2.5. Sleep Quality Measurements
2.6. Statistical Analysis
3. Results
3.1. Subject’s Characteristics
3.2. Effects of Qigong Exercise on Inflammatory Status and Sleep Quality in PD
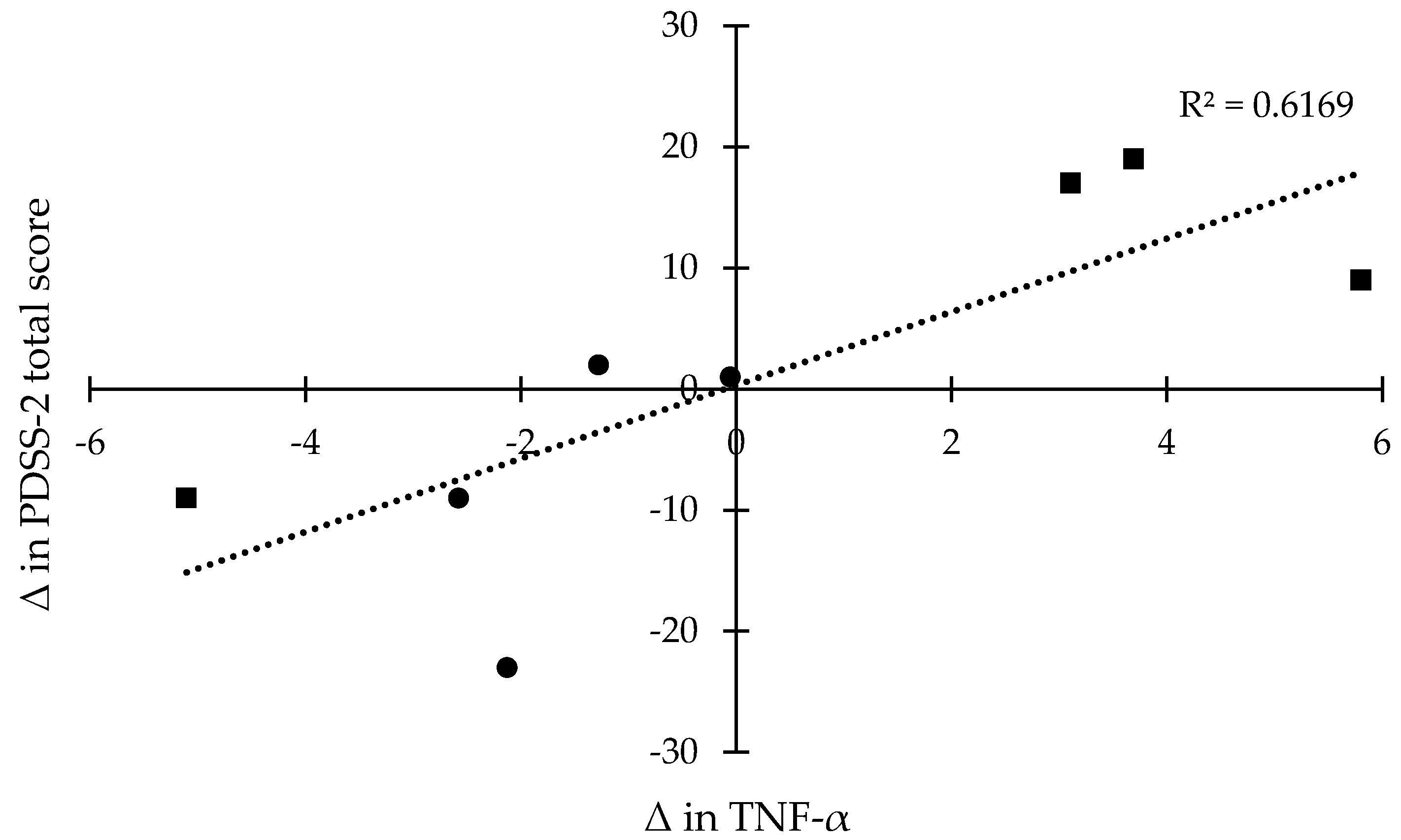
3.3. Relationships Between TNF-α Levels and Sleep Disturbances in PD
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Olanow, C.W.; Tatton, W.G. Etiology and pathogenesis of parkinson’s disease. Ann. Rev. Neurosci. 1999, 22, 123–144. [Google Scholar] [CrossRef] [PubMed]
- Jost, W.H. Costs in the treatment of parkinsonism. J. Neurol. 2000, 247, IV31–IV33. [Google Scholar] [CrossRef]
- Surmeier, D.J.; Guzman, J.N.; Sanchez-Padilla, J.; Goldberg, J.A. What causes the death of dopaminergic neurons in parkinson’s disease? Prog. Brain Res. 2010, 183, 59–77. [Google Scholar] [PubMed]
- Nagatsu, T.; Mogi, M.; Ichinose, H.; Togari, A. Cytokines in parkinson’s disease. J. Neural. Transm. Suppl. 2000, 143–151. [Google Scholar]
- Mogi, M.; Harada, M.; Narabayashi, H.; Inagaki, H.; Minami, M.; Nagatsu, T. Interleukin (il)-1 beta, il-2, il-4, il-6 and transforming growth factor-alpha levels are elevated in ventricular cerebrospinal fluid in juvenile parkinsonism and parkinson’s disease. Neurosci. Lett. 1996, 211, 13–16. [Google Scholar] [CrossRef]
- Beitz, J.M. Parkinson’s disease: A review. Front. Biosci. (Schol. Ed.) 2014, 6, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Weintraub, D.; Moberg, P.J.; Duda, J.E.; Katz, I.R.; Stern, M.B. Effect of psychiatric and other nonmotor symptoms on disability in parkinson’s disease. J. Am. Geriatr. Soc. 2004, 52, 784–788. [Google Scholar] [CrossRef] [PubMed]
- Schrempf, W.; Brandt, M.D.; Storch, A.; Reichmann, H. Sleep disorders in parkinson’s disease. J. Parkinsons Dis. 2014, 4, 211–221. [Google Scholar] [PubMed]
- Chaudhuri, K.; Pal, S.; DiMarco, A.; Whately-Smith, C.; Bridgman, K.; Mathew, R.; Pezzela, F.; Forbes, A.; Hogl, B.; Trenkwalder, C. The parkinson’s disease sleep scale: A new instrument for assessing sleep and nocturnal disability in parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2002, 73, 629–635. [Google Scholar] [CrossRef] [PubMed]
- Lieberman, A. Depression in parkinson’s disease: A review. Acta Neurol. Scand. 2006, 113, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Samii, A.; Nutt, J.G.; Ransom, B.R. Parkinson’s disease. Lancet 2004, 363, 1783–1793. [Google Scholar] [CrossRef]
- Politis, M.; Niccolini, F. Serotonin in parkinson’s disease. Behav. Brain Res. 2015, 277, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Ferrer, I. Neuropathology and neurochemistry of nonmotor symptoms in parkinson’s disease. Parkinsons Dis. 2011. [Google Scholar] [CrossRef] [PubMed]
- Krueger, J.M.; Fang, J.; Taishi, P.; Chen, Z.; Kushikata, T.; Gardi, J. Sleep: A physiologic role for il-1β and tnf-α. Ann. N.Y. Acad. Sci. 1998, 856, 148–159. [Google Scholar] [CrossRef] [PubMed]
- Vgontzas, A.N.; Papanicolaou, D.A.; Bixler, E.O.; Kales, A.; Tyson, K.; Chrousos, G.P. Elevation of plasma cytokines in disorders of excessive daytime sleepiness: Role of sleep disturbance and obesity. J. Clin. Endocrinol. Metab. 1997, 82, 1313–1316. [Google Scholar] [CrossRef] [PubMed]
- Barnum, C.J.; Tansey, M.G. Neuroinflammation and non-motor symptoms: The dark passenger of parkinson’s disease? Curr. Neurol. Neurosci. Rep. 2012, 12, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Jahnke, R.; Larkey, L.; Rogers, C.; Etnier, J.; Lin, F. A comprehensive review of health benefits of qigong and tai chi. Am. J. Health Promot. 2010, 24, e1–e25. [Google Scholar] [CrossRef] [PubMed]
- Wassom, D.J.; Lyons, K.E.; Pahwa, R.; Liu, W. Qigong exercise may improve sleep quality and gait performance in parkinson’s disease: A pilot study. Int. J. Neurosci. 2014, 125, 578–584. [Google Scholar] [CrossRef] [PubMed]
- Xiao, C.-M.; Zhuang, Y.-C. Effect of health baduanjin qigong for mild to moderate parkinson’s disease. Geriatr. Gerontol. Int. 2015, 16, 911–919. [Google Scholar] [CrossRef] [PubMed]
- Manzaneque, J.M.; Vera, F.M.; Maldonado, E.F.; Carranque, G.; Cubero, V.M.; Morell, M.; Blanca, M.J. Assessment of immunological parameters following a qigong training program. Med. Sci. Monit. 2004, 10, Cr264–Cr270. [Google Scholar] [PubMed]
- Trenkwalder, C.; Kohnen, R.; Hogl, B.; Metta, V.; Sixel-Doring, F.; Frauscher, B.; Hulsmann, J.; Martinez-Martin, P.; Chaudhuri, K.R. Parkinson’s disease sleep scale—Validation of the revised version pdss-2. Mov. Disord. 2011, 26, 644–652. [Google Scholar] [CrossRef] [PubMed]
- Horváth, K.; Aschermann, Z.; Ács, P.; Deli, G.; Janszky, J.; Karádi, K.; Komoly, S.; Faludi, B.; Kovács, N. Test-retest validity of parkinson’s disease sleep scale 2nd version (pdss-2). J. Parkinsons Dis. 2014, 4, 687–691. [Google Scholar] [PubMed]
- Suzuki, K.; Miyamoto, T.; Miyamoto, M.; Numao, A.; Sakuta, H.; Fujita, H.; Watanabe, Y.; Iwanami, M.; Hirata, K. Sleep Disturbances in Patients with Parkinson’s Disease; InTech: Rijeka, Croatia, 2014. [Google Scholar]
- Suzuki, K.; Miyamoto, T.; Miyamoto, M.; Suzuki, S.; Numao, A.; Watanabe, Y.; Tatsumoto, M.; Sakuta, H.; Watanabe, Y.; Fujita, H.; et al. Evaluation of cutoff scores for the parkinson’s disease sleep scale-2. Acta Neurol. Scand. 2015, 131, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Bessler, H.; Djaldetti, R.; Salman, H.; Bergman, M.; Djaldetti, M. Il-1β, il-2, il-6 and tnf-α production by peripheral blood mononuclear cells from patients with parkinson’s disease. Biomed. Pharmacother. 1999, 53, 141–145. [Google Scholar] [CrossRef]
- Dufek, M.; Hamanová, M.; Lokaj, J.; Goldemund, D.; Rektorová, I.; Michálková, Z.; Sheardová, K.; Rektor, I. Serum inflammatory biomarkers in parkinson’s disease. Parkinsonism Relat. Disord. 2009, 15, 318–320. [Google Scholar] [CrossRef] [PubMed]
- Mogi, M.; Harada, M.; Riederer, P.; Narabayashi, H.; Fujita, K.; Nagatsu, T. Tumor necrosis factor-α (tnf-α) increases both in the brain and in the cerebrospinal fluid from parkinsonian patients. Neurosci. Lett. 1994, 165, 208–210. [Google Scholar] [CrossRef]
- Koziorowski, D.; Tomasiuk, R.; Szlufik, S.; Friedman, A. Inflammatory cytokines and nt-procnp in parkinson’s disease patients. Cytokine 2012, 60, 762–766. [Google Scholar] [CrossRef] [PubMed]
- Dobbs, R.J.; Charlett, A.; Purkiss, A.G.; Dobbs, S.M.; Weller, C.; Peterson, D.W. Association of circulating tnf-α and il-6 with ageing and parkinsonism. Acta Neurol.Scand. 1999, 100, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Scalzo, P.; Kummer, A.; Cardoso, F.; Teixeira, A.L. Increased serum levels of soluble tumor necrosis factor-alpha receptor-1 in patients with parkinson’s disease. J. Neuroimmunol. 2009, 216, 122–125. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, C.C.; Tarelli, R. Parkinson’s disease and systemic inflammation. Parkinsons Dis. 2011. [Google Scholar] [CrossRef] [PubMed]
- Blum-Degen, D.; Muller, T.; Kuhn, W.; Gerlach, M.; Przuntek, H.; Riederer, P. Interleukin-1 beta and interleukin-6 are elevated in the cerebrospinal fluid of alzheimer’s and de novo parkinson’s disease patients. Neurosci. Lett. 1995, 202, 17–20. [Google Scholar] [CrossRef]
- Selikhova, M.V.; Kushlinskii, N.E.; Lyubimova, N.V.; Gusev, E.I. Impaired production of plasma interleukin-6 in patients with parkinson’s disease. Bull. Exp. Biol. Med. 2002, 133, 81–83. [Google Scholar] [CrossRef] [PubMed]
- Lindqvist, D.; Kaufman, E.; Brundin, L.; Hall, S.; Surova, Y.; Hansson, O. Non-motor symptoms in patients with parkinson’s disease—Correlations with inflammatory cytokines in serum. PLoS ONE 2012, 7. [Google Scholar] [CrossRef] [PubMed]
- Larkey, L.; Jahnke, R.; Etnier, J.; Gonzalez, J. Meditative movement as a category of exercise: Implications for research. J. Phys. Act. Health 2009, 6, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Zahner, L.; Cornell, M.; Le, T.; Ratner, J.; Wang, Y.; Pasnoor, M.; Dimachkie, M.; Barohn, R. Benefit of qigong exercise in patients with fibromyalgia: A pilot study. Int. J. Neurosci. 2012, 122, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Lynch, M.; Sawynok, J.; Hiew, C.; Marcon, D. A randomized controlled trial of qigong for fibromyalgia. Arthritis Res. Ther. 2012, 14. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.S.M.; Ho, R.T.H.; Chung, K.-f.; Wang, C.-w.; Yao, T.-j.; Ng, S.-m.; Chan, C.L.W. Qigong exercise alleviates fatigue, anxiety, and depressive symptoms, improves sleep quality, and shortens sleep latency in persons with chronic fatigue syndrome-like illness. Evid. Based Complement. Alternat. Med. 2014. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Fisher, K.J.; Harmer, P.; Irbe, D.; Tearse, R.G.; Weimer, C. Tai chi and self-rated quality of sleep and daytime sleepiness in older adults: A randomized controlled trial. J. Am. Geriatr. Soc. 2004, 52, 892–900. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Sawada, M.; Noriyama, Y.; Arita, K.; Ota, T.; Sadamatsu, M.; Kiyotou, R.; Hirai, M.; Kishimoto, T. Tai chi exercise versus rehabilitation for the elderly with cerebral vascular disorder: A single-blinded randomized controlled trial. Psychogeriatrics 2010, 10, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Black, D.S.; O’Reilly, G.A.; Olmstead, R.; Breen, E.C.; Irwin, M.R. Mindfulness meditation and improvement in sleep quality and daytime impairment among older adults with sleep disturbances: A randomized clinical trial. JAMA Intern. Med. 2015, 175, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Carlson, L.E.; Garland, S.N. Impact of mindfulness-based stress reduction (mbsr) on sleep, mood, stress and fatigue symptoms in cancer outpatients. Intern. J. Behav. Med. 2005, 12, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, S.L.; Bootzin, R.R.; Figueredo, A.J.; Lopez, A.M.; Schwartz, G.E. The efficacy of mindfulness-based stress reduction in the treatment of sleep disturbance in women with breast cancer: An exploratory study. J. Psychosom. Res. 2003, 54, 85–91. [Google Scholar] [CrossRef]
- Menza, M.; DeFronzo Dobkin, R.; Marin, H.; Mark, M.H.; Gara, M.; Bienfait, K.; Dicke, A.; Kusnekov, A. The role of inflammatory cytokines in cognition and other non-motor symptoms of parkinson’s disease. Psychosomatics 2010, 51, 474–479. [Google Scholar] [PubMed]
- Zoladz, J.A.; Majerczak, J.; Zeligowska, E.; Mencel, J.; Jaskolski, A.; Jaskolska, A.; Marusiak, J. Moderate-intensity interval training increases serum brain-derived neurotrophic factor level and decreases inflammation in parkinson’s disease patients. J. Physiol. Pharmacol. 2014, 65, 441–448. [Google Scholar] [PubMed]
- Kiecolt-Glaser, J.K.; Bennett, J.M.; Andridge, R.; Peng, J.; Shapiro, C.L.; Malarkey, W.B.; Emery, C.F.; Layman, R.; Mrozek, E.E.; Glaser, R. Yoga’s impact on inflammation, mood, and fatigue in breast cancer survivors: A randomized controlled trial. J. Clin. Oncol. 2014, 32, 1040–1049. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.; Steensberg, A.; Fischer, C.; Keller, C.; Keller, P.; Plomgaard, P.; Wolsk-Petersen, E.; Febbraio, M. The metabolic role of il-6 produced during exercise: Is il-6 an exercise factor? Proc. Nutr. Soc. 2004, 63, 263–267. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Movement | Sound | Body Movement and Breathing |
|---|---|---|
| Adjusting movement | No sound | When inhaling, lift up both arms/hands with elbows fully extended from two sides to the shoulder level, move both arms/hands horizontally to the front and then towards the chest. Exhale as arms/hands move down slowly till the end of exhalation. Repeat the breath and body movement three times in a complete adjusting breath. Perform this movement before Movement 1, between each movement, and after Movement 6 (a total of seven times throughout the exercise). |
| Movement 1 | Hsu [shh] | When inhaling, lift up both arms/hands the body to chest level, with the palms facing up and elbow joints fully extended, and then move the hands towards the chest. Exhale as the arms/hands move down. During the slow exhalation, chant “shh.” Repeat the sound and movement six times. |
| Movement 2 | Her [her] | When inhaling, lift up both arms/hands near the body to the chest level with the palms facing up. Begin to exhale. During exhalation, chant “her” and continue to slowly move arms/hands up up to the eyebrow level. Inhale while moving arms/hands down. Convert to exhalation when the hands pass the chest level and continue to move arms/hands down. Repeat the sound and movement six times. |
| Movement 3 | Hoo [who] | When inhaling, lift up both arms/hands near the body to chest level with palms facing up. Then, begin to exhale and chant “who” while slowly moving your left hand up and right hand down in a diagonal direction until the end of exhalation. Inhale and move left hand down and right hand up to the chest level again. Convert to exhalation and chant “who” while slowly moving the left hand up and the right hand down in a diagonal direction until the end of exhalation. Repeat the sound and movement three times. |
| Movement 4 | Sss [sss] | When inhaling, lift up both arms/hands to the chest level with palms facing up. Begin to exhale. During exhalation, chant “sss” while slowly pushing the hands forward and then down to both sides until the end of exhalation. Repeat the sound and movement six times. |
| Movement 5 | Chway [ch-way] | When inhaling, lift up both arms/hands through the back of trunk to the front of the chest as if holding a large ball. Begin to exhale. During exhalation, chant “chway” while slowly moving both hands down over an imaginary ball until touching the thighs. Bend both knees down slightly while you circle your hands down over the ball. Repeat the sound and movement six times. |
| Movement 6 | See [see] | When inhaling, lift up both arms/hands near the body to the chest level with palms facing up. Begin to exhale. During exhalation, chant “see” and continue to slowly lift up hands above the head until the end of exhalation. Begin to inhale while slowly moving down arms/hands along the same path. Begin to exhale again when the hands pass the chest and continue to move arms/hands down until the end of exhalation. Repeat the sound and movement six times. |
| Throughout the entire exercise sequence, focus your mind on an important focal point, the so-called “Dan Tian” acupuncture point, which is located in the abdomen three finger widths below your belly button to establish and maintain the mind emptiness status. | ||
| Characteristic | Experimental | Control |
|---|---|---|
| Age, y | 61.8 ± 5.7 | 68.0 ± 5.3 |
| Disease duration, y | 8.0 ± 3.6 | 13.3 ± 3.6 |
| Symptom duration, y | 9.3 ± 4.2 | 13.9 ± 8.6 |
| HY stage | 2.7 ± 0.3 | 2.4 ± 0.5 |
| Assessment | TNF-α. pg/mL | |
|---|---|---|
| Experimental | Control | |
| Pre-intervention | 13.8 ± 0.6 | 13.3 ± 3.3 |
| Post-intervention | 12.3 ± 1.6 * | 15.1 ± 2.3 |
| PDSS-2 | Baseline | Mean Change (Δ) | ||
|---|---|---|---|---|
| Experimental | Control | Experimental | Control | |
| Motor symptoms at night | 4.5 ± 4.7 | 3.0 ± 2.5 | −2.3 ± 4.6 | 2.8 ± 2.8 |
| PD symptoms at night | 6.0 ± 3.2 | 2.8 ± 2.2 | −2.5 ± 3.8 * | 2.3 ± 4.1 |
| Disturbed sleep | 8.3 ± 3.4 | 8.3 ± 5.3 | −2.5 ± 4.1 | 4.0 ± 9.1 |
| PDSS-2 total score | 18.8 ± 8.1 | 14.0 ± 9.8 | −7.3 ± 11.6 ** | 9.0 ± 12.8 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moon, S.; Schmidt, M.; Smirnova, I.V.; Colgrove, Y.; Liu, W. Qigong Exercise May Reduce Serum TNF-α Levels and Improve Sleep in People with Parkinson’s Disease: A Pilot Study. Medicines 2017, 4, 23. https://doi.org/10.3390/medicines4020023
Moon S, Schmidt M, Smirnova IV, Colgrove Y, Liu W. Qigong Exercise May Reduce Serum TNF-α Levels and Improve Sleep in People with Parkinson’s Disease: A Pilot Study. Medicines. 2017; 4(2):23. https://doi.org/10.3390/medicines4020023
Chicago/Turabian StyleMoon, Sanghee, Marshall Schmidt, Irina V. Smirnova, Yvonne Colgrove, and Wen Liu. 2017. "Qigong Exercise May Reduce Serum TNF-α Levels and Improve Sleep in People with Parkinson’s Disease: A Pilot Study" Medicines 4, no. 2: 23. https://doi.org/10.3390/medicines4020023
APA StyleMoon, S., Schmidt, M., Smirnova, I. V., Colgrove, Y., & Liu, W. (2017). Qigong Exercise May Reduce Serum TNF-α Levels and Improve Sleep in People with Parkinson’s Disease: A Pilot Study. Medicines, 4(2), 23. https://doi.org/10.3390/medicines4020023