Intravesical Instillation of Norketamine, a Ketamine Metabolite, and Induced Bladder Functional Changes in Rats

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Experimental Animal
2.3. Intravesical Instillation of Ketamine and Norketamine
2.4. CMG Test
2.5. Hematoxylin and Eosin (H&E) Staining, Masson’s Trichrome Staining, and Evaluation of Smooth Muscles and Collagen
2.6. Statistical Analysis
3. Results
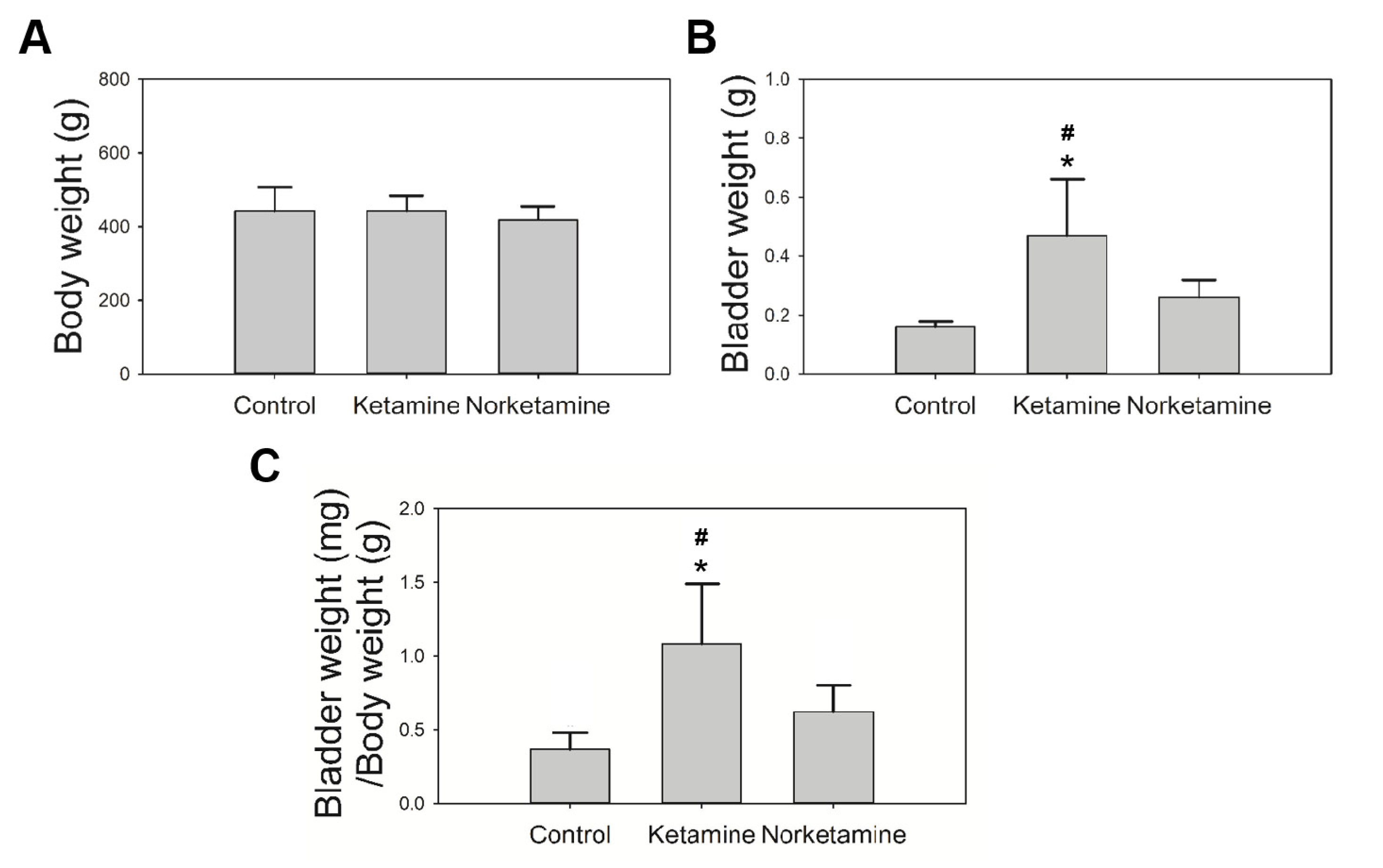
3.1. Intravesical Instillation of Ketamine or Norketamine for Four Weeks Altered the Body Weight and Bladder Weight of Rats
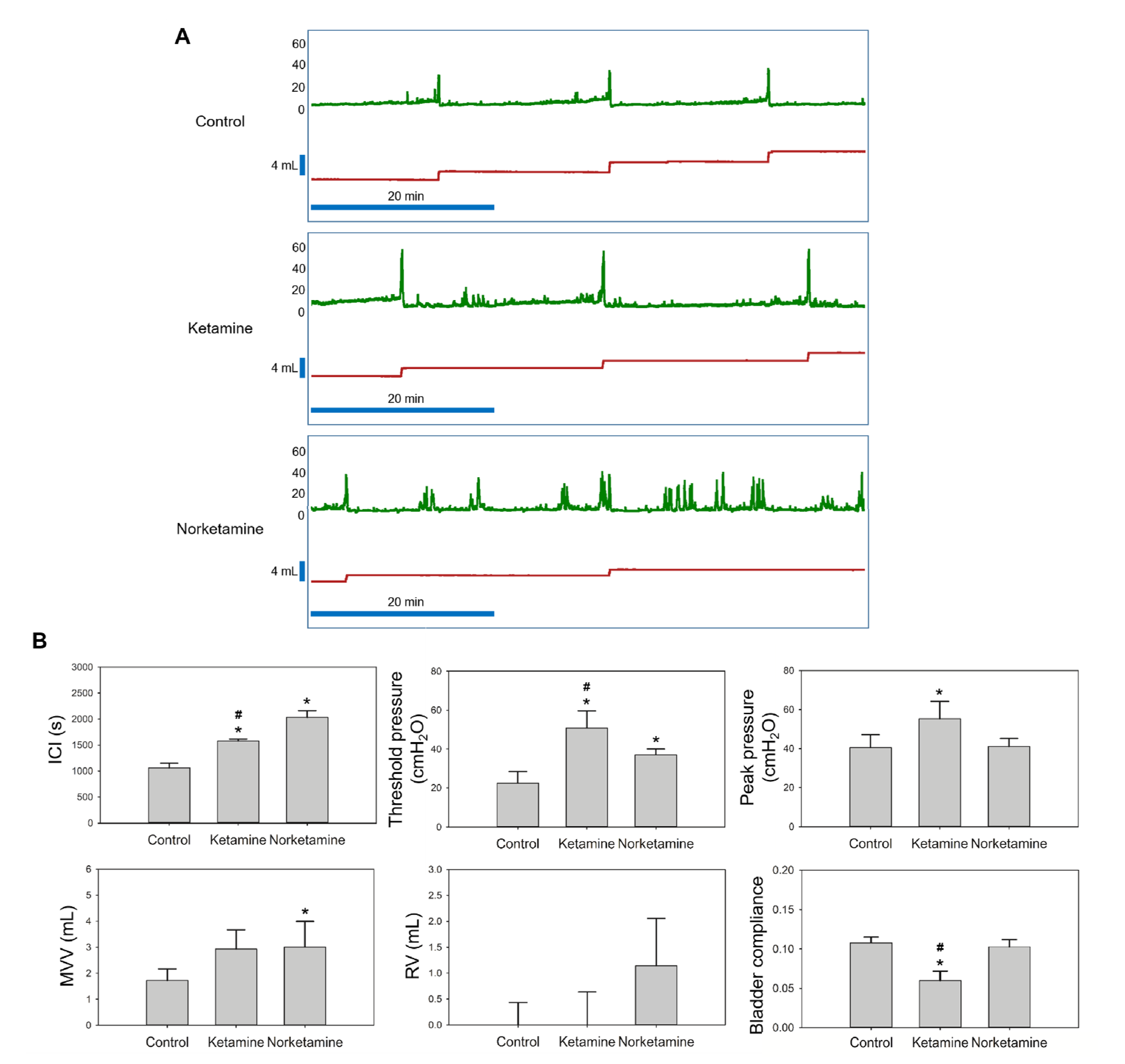
3.2. Intravesical Instillation of Ketamine or Norketamine Impaired the Bladder Function
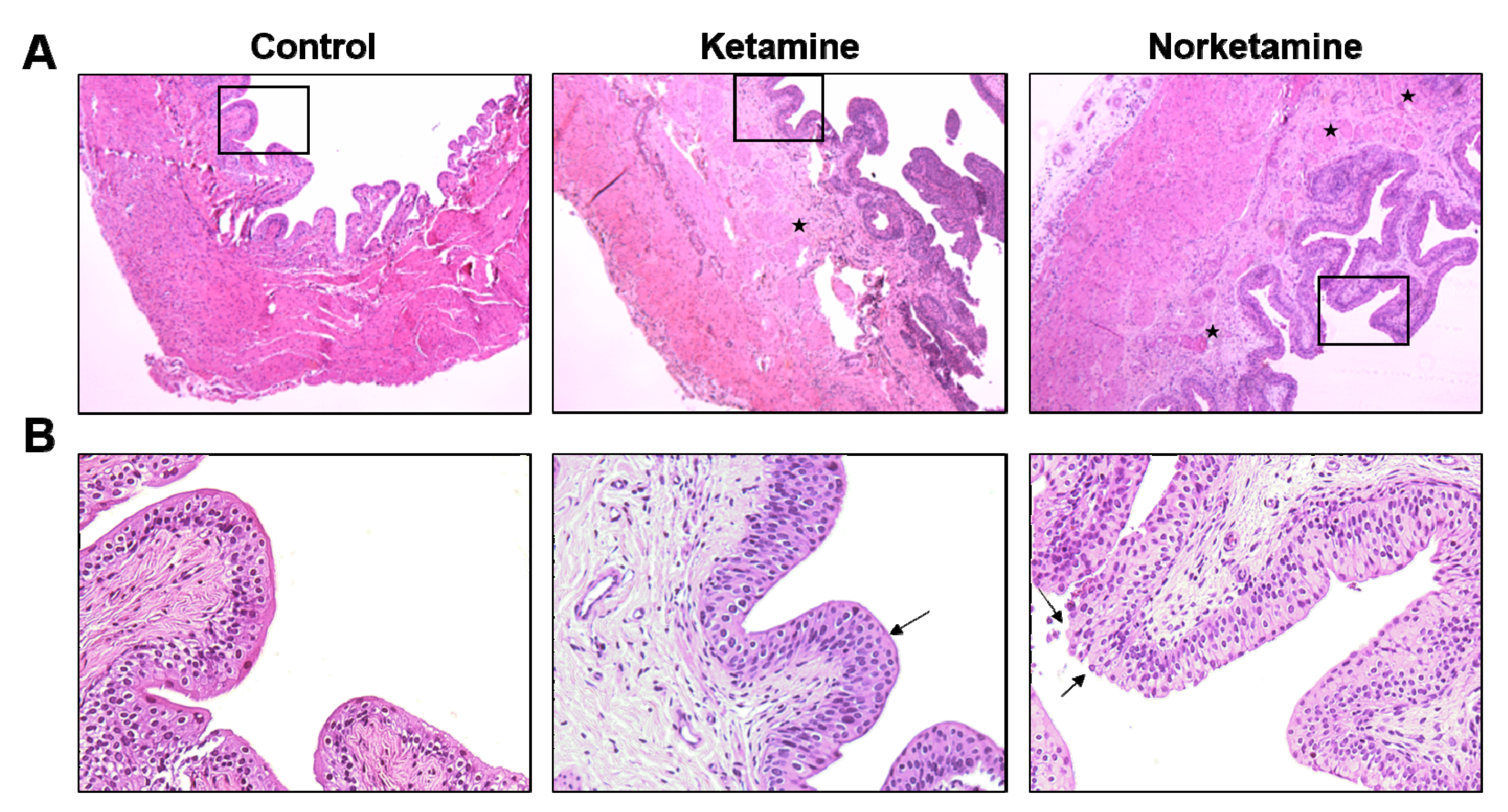
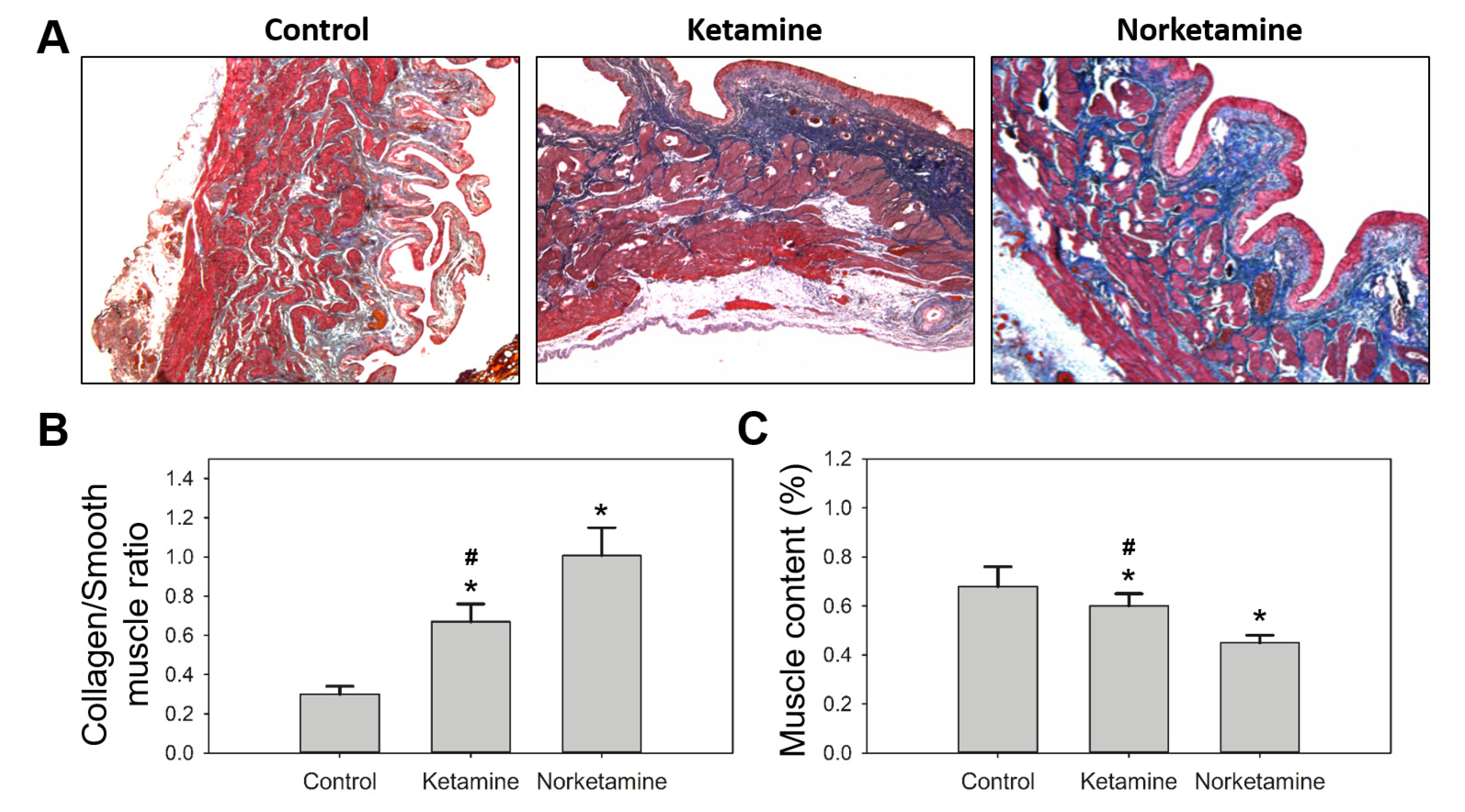
3.3. Histological Changes Corresponding to Ketamine and Norketamine-Induced Damage in Bladder
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Domino, E.F.; Chodoff, P.; Corssen, G. Pharmacologic effects of CI-581, a new dissociative anesthetic, in man. Clin. Pharmacol. Ther. 1965, 6, 279–291. [Google Scholar] [CrossRef] [Green Version]
- Grant, I.S.; Nimmo, W.S.; Clements, J.A.; Wyant, G.M. Pharmacokinetics and Analgesic Effects of I.M. and Oral Ketamine. Surv. Anesthesiol. 1982, 26, 70–810. [Google Scholar] [CrossRef]
- Dong, T.T.; Mellin-Olsen, J.; Gelb, A.W. Ketamine: A growing global health-care need. Br. J. Anaesth. 2015, 115, 491–493. [Google Scholar] [CrossRef] [Green Version]
- Wei, Y.; Chang, L.; Hashimoto, K. A historical review of antidepressant effects of ketamine and its enantiomers. Pharmacol. Biochem. Behav. 2020, 190, 172870. [Google Scholar] [CrossRef]
- Lichtwardt, J.R.; Girgis, S. Transurethral resection of prostate with intravenous sedation. Urology 1985, 26, 112–113. [Google Scholar] [CrossRef]
- Rosati, A.; De Masi, S.; Guerrini, R. Ketamine for Refractory Status Epilepticus: A Systematic Review. CNS Drugs 2018, 32, 997–1009. [Google Scholar] [CrossRef]
- Chang, C.-M.; Wu, T.L.; Ting, T.-T.; Chen, C.-Y.; Su, L.-W.; Chen, W.J. Mis-anaesthetized society: Expectancies and recreational use of ketamine in Taiwan. BMC Public Health 2019, 19, 1307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, P.S.-K.; Ma, W.-K.; Wong, S.C.-W.; Chu, R.W.-H.; Cheng, C.-H.; Wong, S.; Tse, J.M.-L.; Lau, F.-L.; Yiu, M.-K.; Man, C.-W. The destruction of the lower urinary tract by ketamine abuse: A new syndrome? BJU Int. 2008, 102, 1616–1622. [Google Scholar] [CrossRef]
- Tsai, T.-H.; Cha, T.-L.; Lin, C.-M.; Tsao, C.-W.; Tang, S.-H.; Chuang, F.-P.; Wu, S.-T.; Sun, G.-H.; Yu, D.-S.; Chang, S.-Y. Ketamine-associated bladder dysfunction. Int. J. Urol. 2009, 16, 826–829. [Google Scholar] [CrossRef]
- Chuang, S.-M.; Liu, K.-M.; Li, Y.-L.; Jang, M.-Y.; Lee, H.-H.; Wu, W.J.; Chang, W.-C.; Levin, R.M.; Juan, Y.-S. Dual involvements of cyclooxygenase and nitric oxide synthase expressions in ketamine-induced ulcerative cystitis in rat bladder. Neurourol. Urodynamics 2013, 32, 1137–1143. [Google Scholar] [CrossRef]
- Sihra, N.; Ockrim, J.; Wood, D. The effects of recreational ketamine cystitis on urinary tract reconstruction—A surgical chal-lenge. BJU Int. 2018, 121, 458–465. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.H.; Jhang, J.F.; Hsu, Y.H.; Jiang, Y.H.; Zhai, W.J.; Kuo, H.C. Smaller bladder capacity and stronger bladder contrac-tility in patients with ketamine cystitis are associated with elevated TRPV1 and TRPV4. Sci. Rep. 2021, 11, 5200. [Google Scholar] [CrossRef]
- Wang, J.; Chen, Y.; Gu, D.; Zhang, G.; Chen, J.; Zhao, J.; Wu, P. Ketamine-induced bladder fibrosis involves epithelial-to-mesenchymal transition mediated by transforming growth factor-β1. Am. J. Physiol. Physiol. 2017, 313, F961–F972. [Google Scholar] [CrossRef] [Green Version]
- Winstock, A.R.; Mitcheson, L.; Gillatt, D.A.; Cottrell, A.M. The prevalence and natural history of urinary symptoms among recreational ketamine users. BJU Int. 2012, 110, 1762–1766. [Google Scholar] [CrossRef]
- Li, C.-C.; Wu, S.-T.; Cha, T.-L.; Sun, G.-H.; Yu, D.-S.; Meng, E. A survey for ketamine abuse and its relation to the lower urinary tract symptoms in Taiwan. Sci. Rep. 2019, 9, 7240. [Google Scholar] [CrossRef]
- Shahani, R.; Streutker, C.; Dickson, B.; Stewart, R.J. Ketamine-Associated Ulcerative Cystitis: A New Clinical Entity. Urology 2007, 69, 810–812. [Google Scholar] [CrossRef]
- Jhang, J.-F.; Hsu, Y.-H.; Kuo, H.-C. Possible pathophysiology of ketamine-related cystitis and associated treatment strategies. Int. J. Urol. 2015, 22, 816–825. [Google Scholar] [CrossRef]
- Lee, Y.-L.; Lin, K.-L.; Chuang, S.-M.; Lee, Y.-C.; Lu, M.-C.; Wu, B.-N.; Wu, W.-J.; Yuan, S.-S.F.; Ho, W.-T.; Juan, Y.-S. Elucidating Mechanisms of Bladder Repair after Hyaluronan Instillation in Ketamine-Induced Ulcerative Cystitis in Animal Model. Am. J. Pathol. 2017, 187, 1945–1959. [Google Scholar] [CrossRef] [Green Version]
- Moore, K.A.; Sklerov, J.; Levine, B.; Jacobs, A.J. Urine concentrations of ketamine and norketamine following illegal consumption. J. Anal. Toxicol. 2001, 25, 583–588. [Google Scholar] [CrossRef] [Green Version]
- Mozayani, A. Katamine—Effects on Human Performance and Behavior. Forensic Sci. Rev. 2002, 14, 123–131. [Google Scholar]
- Wang, K.-C.; Shih, T.-S.; Cheng, S.-G. Use of SPE and LC/TIS/MS/MS for rapid detection and quantitation of ketamine and its metabolite, norketamine, in urine. Forensic Sci. Int. 2005, 147, 81–88. [Google Scholar] [CrossRef]
- Wu, G.-J.; Chan, H.; Lee, M.-R.; Chen, C.-Y.; Yang, D.-Y.; Cheng, F.-C. Simultaneous measurement of urinary ketamine, nor-ketamine, and dehydronorketamine by liquid chromatography-atmospheric pressure chemical ionization mass spectrometry. J. Chin. Chem. Soc. 2007, 54, 351–355. [Google Scholar] [CrossRef]
- Kim, E.-M.; Lee, J.-S.; Choi, S.-K.; Lim, M.-A.; Chung, H.-S. Analysis of ketamine and norketamine in urine by automatic solid-phase extraction (SPE) and positive ion chemical ionization–gas chromatography–mass spectrometry (PCI–GC–MS). Forensic Sci. Int. 2008, 174, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Zanos, P.; Moaddel, R.; Morris, P.J.; Riggs, L.M.; Highland, J.N.; Georgiou, P.; Pereira, E.F.R.; Albuquerque, E.X.; Thomas, C.J., Jr.; Gould, T.D.; et al. Ketamine and Ketamine Metabolite Pharmacology: Insights into Therapeutic Mechanisms. Pharmacol. Rev. 2018, 70, 621–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, C.-C.; Lin, A.T.-L.; Yang, A.-H.; Chen, K.-K. Microvascular Injury in Ketamine-Induced Bladder Dysfunction. PLoS ONE 2016, 11, e0160578. [Google Scholar] [CrossRef]
- Gu, D.; Huang, J.; Yin, Y.; Shan, Z.; Zheng, S.; Wu, P. Long-term ketamine abuse induces cystitis in rats by impairing the bladder epithelial barrier. Mol. Biol. Rep. 2014, 41, 7313–7322. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.; Yang, J.R.; Yin, Z.; Guo, Q.; Liang, B.L.; Zhou, K.Q. Genitourinary toxicity of ketamine. Hong Kong Med. J. 2013, 19, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Vandorpe, D.H.; Xie, X.; Alper, S.L.; Zeidel, M.L.; Yu, W. Disruption of Cav1.2-mediated signaling is a pathway for ketamine-induced pathology. Nat. Commun. 2020, 11, 4328. [Google Scholar] [CrossRef]
- Riedl, C.R.; Engelhardt, P.F.; Daha, K.L.; Morakis, N.; Pflüger, H. Hyaluronan treatment of interstitial cystitis/painful bladder syndrome. Int. Urogynecol. J. Pelvic Floor Dysfunct. 2008, 19, 717–721. [Google Scholar] [CrossRef]
- Tan, S.; Chan, W.; Wai, M.S.; Hui, L.K.; Hui, V.W.; James, A.E.; Yeung, L.; Yew, D. Ketamine effects on the urogenital system-changes in the urinary bladder and sperm motility. Microsc. Res. Tech. 2011, 74, 1192–1198. [Google Scholar] [CrossRef] [PubMed]
- Rajandram, R.; Ong, T.A.; Razack, A.H.A.; Maciver, B.; Zeidel, M.; Yu, W. Intact urothelial barrier function in a mouse model of ketamine-induced voiding dysfunction. Am. J. Physiol. Physiol. 2016, 310, F885–F894. [Google Scholar] [CrossRef] [Green Version]
- Uvin, P.; Everaerts, W.; Pinto, S.; Alpizar, Y.A.; Boudes, M.; Gevaert, T.; Voets, T.; Nilius, B.; Talavera, K.; De Ridder, D. The Use of Cystometry in Small Rodents: A Study of Bladder Chemosensation. J. Vis. Exp. 2012, 66, e3869. [Google Scholar] [CrossRef] [Green Version]
- Chu, P.S.; Kwok, S.C.; Lam, K.M.; Chu, T.Y.; Chan, S.W.; Man, C.W.; Ma, W.K.; Chui, K.L.; Tse, M.L.; Lau, F.L. ‘Street ketamine’-associated bladder dysfunction: A report of ten cases. Hong Kong Med. J. 2007, 13, 311–313. [Google Scholar]
- Wu, Z.-G.; Chen, F.; Wu, H.; Chen, J.-X.; Wei, Q.-T.; Fu, Y.-Q.; Lu, X.; Ye, Y.; Yan, Y.-Y.; Liao, L.-C. Urinary metabonomics of rats with ketamine-induced cystitis using GC-MS spectroscopy. Int. J. Clin. Exp. Pathol. 2018, 11, 558–567. [Google Scholar]
- Shen, C.-H.; Wang, S.-T.; Wang, S.-C.; Lin, S.-M.; Lin, L.-C.; Dai, Y.C.; Liu, Y.W. Ketamine-induced bladder dysfunction is associated with extracellular matrix ac-cumulation and impairment of calcium signaling in a mouse model. Mol. Med. Rep. 2019, 19, 2716–2728. [Google Scholar]
- Kim, A.; Yu, H.Y.; Heo, J.; Song, M.; Shin, J.-H.; Lim, J.; Yoon, S.-J.; Kim, Y.; Lee, S.; Kim, S.W.; et al. Mesenchymal stem cells protect against the tissue fibrosis of ketamine-induced cystitis in rat bladder. Sci. Rep. 2016, 6, 30881. [Google Scholar] [CrossRef] [Green Version]
- Mochizuki, T.; Sokabe, T.; Araki, I.; Fujishita, K.; Shibasaki, K.; Uchida, K.; Naruse, K.; Koizumi, S.; Takeda, M.; Tominaga, M. The TRPV4 Cation Channel Mediates Stretchevoked Ca2+ Influx and ATP Release in Primary Urothelial Cell Cultures. J. Biol. Chem. 2009, 284, 21257–21264. [Google Scholar] [CrossRef] [Green Version]
- Dmochowski, R.R. Bladder Outlet Obstruction: Etiology and Evaluation. Rev. Urol. 2005, 7, S3–S13. [Google Scholar] [PubMed]
- Metcalfe, P.D.; Wang, J.; Jiao, H.; Huang, Y.; Hori, K.; Moore, R.B.; Tredget, E.E. Bladder outlet obstruction: Progression from inflammation to fibrosis. BJU Int. 2010, 106, 1686–1694. [Google Scholar] [CrossRef]
- Bosch, R.; Abrams, P.; Averbeck, M.A.; Agró, E.F.; Gammie, A.; Marcelissen, T.; Solomon, E. Do functional changes occur in the bladder due to bladder outlet obstruction?—ICI-RS 2018. Neurourol. Urodyn. 2019, 38, S56–S65. [Google Scholar] [CrossRef]
- Fusco, F.; Creta, M.; De Nunzio, C.; Iacovelli, V.; Mangiapia, F.; Marzi, V.L.; Agrò, E.F. Progressive bladder remodeling due to bladder outlet obstruction: A systematic review of morphological and molecular evidences in humans. BMC Urol. 2018, 18, 15. [Google Scholar] [CrossRef]
- Al-Hayek, S.; Thomas, A.; Abrams, P. Natural history of detrusor contractility—minimum ten-year urodynamic follow-up in men with bladder outlet obstruction and those with detrusor. Scand. J. Urol. Nephrol. Suppl. 2004, 215, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Wang, J.; Wang, R.; Xu, Y.; Chen, F.; Tang, L.; Ren, W.; Fu, L.; Tan, B.; Huang, P.; et al. Time-dependent functional, morphological, and molecular changes in diabetic bladder dysfunction in streptozotocin-induced diabetic mice. Neurourol. Urodyn. 2019, 38, 1266–1277. [Google Scholar] [CrossRef] [Green Version]
- Daneshgari, F.; Liu, G.; Birder, L.; Hanna-Mitchell, A.T.; Chacko, S. Diabetic Bladder Dysfunction: Current Translational Knowledge. J. Urol. 2009, 182, S18–S26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mannikarottu, A.S.; Hypolite, J.A.; Zderic, S.A.; Wein, A.J.; Chacko, S.; Disanto, M.E. Regional alterations in the expression of smooth muscle myosin isoforms in response to partial bladder outlet obstruction. J. Urol. 2005, 173, 302–308. [Google Scholar] [CrossRef]
- Mirone, V.; Imbimbo, C.; Sessa, G.; Palmieri, A.; Longo, N.; Granata, A.M.; Fusco, F. Correlation between detrusor collagen content and urinary symptoms in patients with prostatic obstruction. J. Urol. 2004, 172, 1386–1389. [Google Scholar] [CrossRef]
- Averbeck, M.A.; De Lima, N.G.; Motta, G.A.; Beltrao, L.F.; Filho, N.J.A.; Rigotti, C.P.; Dos Santos, W.N.; Dos Santos, S.K.; Da Silva, L.F.; Rhoden, E.L. Collagen content in the bladder of men with LUTS undergoing open prostatectomy: A pilot study. Neurourol. Urodynamics 2018, 37, 1088–1094. [Google Scholar] [CrossRef]
- Lin, H.-C.; Lee, H.-S.; Chiueh, T.-S.; Lin, Y.-C.; Cha, T.-L.; Meng, E. Histopathological assessment of inflammation and expression of inflammatory markers in patients with ketamine-induced cystitis. Mol. Med. Rep. 2015, 11, 2421–2428. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeh, C.-H.; Chen, B.-H.; Tseng, X.-W.; Liao, C.-H.; Tsai, W.-K.; Chiang, H.-S.; Wu, Y.-N. Intravesical Instillation of Norketamine, a Ketamine Metabolite, and Induced Bladder Functional Changes in Rats. Toxics 2021, 9, 154. https://doi.org/10.3390/toxics9070154
Yeh C-H, Chen B-H, Tseng X-W, Liao C-H, Tsai W-K, Chiang H-S, Wu Y-N. Intravesical Instillation of Norketamine, a Ketamine Metabolite, and Induced Bladder Functional Changes in Rats. Toxics. 2021; 9(7):154. https://doi.org/10.3390/toxics9070154
Chicago/Turabian StyleYeh, Chung-Hsin, Bo-He Chen, Xiao-Wen Tseng, Chun-Hou Liao, Wei-Kung Tsai, Han-Sun Chiang, and Yi-No Wu. 2021. "Intravesical Instillation of Norketamine, a Ketamine Metabolite, and Induced Bladder Functional Changes in Rats" Toxics 9, no. 7: 154. https://doi.org/10.3390/toxics9070154
APA StyleYeh, C.-H., Chen, B.-H., Tseng, X.-W., Liao, C.-H., Tsai, W.-K., Chiang, H.-S., & Wu, Y.-N. (2021). Intravesical Instillation of Norketamine, a Ketamine Metabolite, and Induced Bladder Functional Changes in Rats. Toxics, 9(7), 154. https://doi.org/10.3390/toxics9070154