
Toxic Metal Content in Deciduous Teeth: A Systematic Review

 , , , , ,
, , , , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Focused Question
2.2. Protocol
2.3. Eligibility Criteria
- Studies conducted on deciduous teeth;
- Measurement of toxic metal concentrations;
- In vitro studies;
- Studies in English;
- Full-text articles.
- Studies focusing or permanent teeth or bones;
- Studies which did not examine the concentration of toxic metals;
- Non-English papers;
- Systematic review papers;
- Review articles;
- Not full-text accessible;
- Duplicated publications.
2.4. Information Sources, Search Strategy, and Study Selection
2.5. Data Collection Process and Data Items
2.6. Risk of Bias and Quality Assessment
2.7. Quality Assessment
- Is it clear in the study what is the “cause” and what is the “effect”?
- Were the participants included in any similar comparisons?
- Were the participants included in any comparisons receiving similar treatment/care, other than the exposure or intervention of interest? Was there a control group?
- Were there multiple measurements of the outcome both before and after the intervention/exposure?
- Was a follow up completed, and if not, were differences between groups in terms of their follow up adequately described and analyzed? Were the outcomes of participants included in any comparisons measured in the same way?
- Were the outcomes measured in a reliable way?
- Was an appropriate statistical analysis used?
3. Results
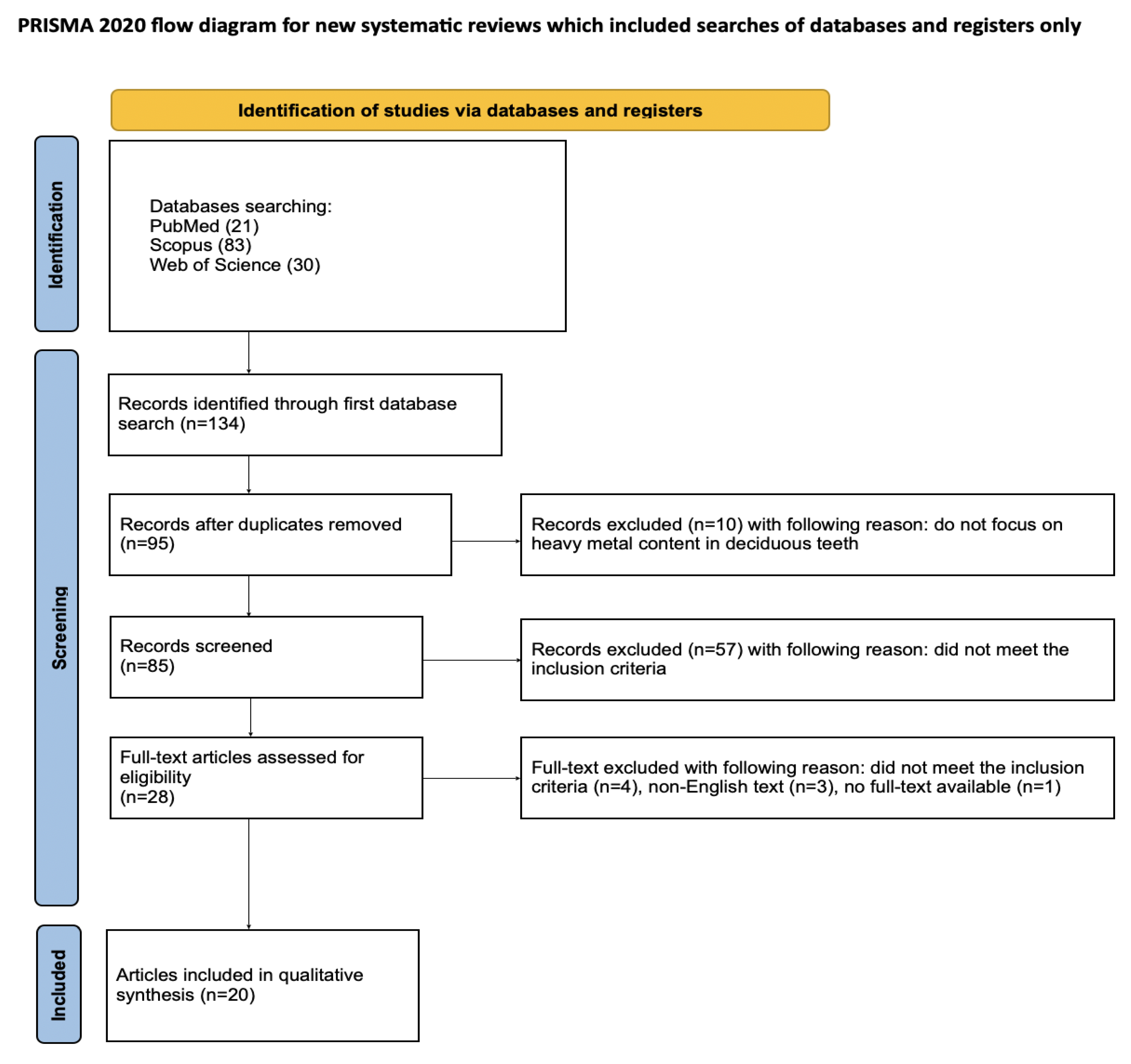
3.1. Study Selection
3.2. General Characteristics of the Included Studies
3.3. Main Study Outcomes
3.3.1. Differences by Tooth Type and Presence of Caries
3.3.2. Environmental Exposure: Industrial, Mining, and Conflict Zones
3.3.3. Socioeconomic and Behavioral Factors
3.3.4. Prenatal and Postnatal Exposure Patterns
3.3.5. Age and Dentition Differences
3.3.6. Associations with Neurodevelopmental Disorders
3.4. Quality Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gil, F.; Hernández, A.F. Toxicological Importance of Human Biomonitoring of Metallic and Metalloid Elements in Different Biological Samples. Food Chem. Toxicol. 2015, 80, 287–297. [Google Scholar] [CrossRef]
- Seow, W.K. Dental Enamel Defects in the Primary Dentition: Prevalence and Etiology. In Planning and Care for Children and Adolescents with Dental Enamel Defects: Etiology, Research and Contemporary Management; Drummond, B.K., Kilpatrick, N., Eds.; Springer: Berlin/Heidelberg, Germany, 2015; pp. 1–14. ISBN 978-3-662-44800-7. [Google Scholar]
- Sunderland, E.P.; Smith, C.J.; Sunderland, R. A Histological Study of the Chronology of Initial Mineralization in the Human Deciduous Dentition. Arch. Oral. Biol. 1987, 32, 167–174. [Google Scholar] [CrossRef]
- Bauer, J.A.; Punshon, T.; Barr, M.N.; Jackson, B.P.; Weisskopf, M.G.; Bidlack, F.B.; Coker, M.O.; Peacock, J.L.; Karagas, M.R. Deciduous Teeth from the New Hampshire Birth Cohort Study: Early Life Environmental and Dietary Predictors of Dentin Elements. Environ. Res. 2024, 256, 119170. [Google Scholar] [CrossRef] [PubMed]
- Friedman, A.; Bauer, J.A.; Austin, C.; Downs, T.J.; Tripodis, Y.; Heiger-Bernays, W.; White, R.F.; Arora, M.; Claus Henn, B. Multiple Metals in Children’s Deciduous Teeth: Results from a Community-Initiated Pilot Study. J. Expo. Sci. Environ. Epidemiol. 2022, 32, 408–417. [Google Scholar] [CrossRef] [PubMed]
- Gerbi, L.; Austin, C.; Pedretti, N.F.; McRae, N.; Amarasiriwardena, C.J.; Mercado-García, A.; Torres-Olascoaga, L.A.; Tellez-Rojo, M.M.; Wright, R.O.; Arora, M.; et al. Biomarkers of Maternal Lead Exposure during Pregnancy Using Micro-Spatial Child Deciduous Dentine Measurements. Environ. Int. 2022, 169, 107529. [Google Scholar] [CrossRef] [PubMed]
- Gunier, R.B.; Mora, A.M.; Smith, D.; Arora, M.; Austin, C.; Eskenazi, B.; Bradman, A. Biomarkers of Manganese Exposure in Pregnant Women and Children Living in an Agricultural Community in California. Environ. Sci. Technol. 2014, 48, 14695–14702. [Google Scholar] [CrossRef]
- Rojas-Torres, J.; Quijón, M.E.G.; Henríquez-Vidal, A.; Devia-Rubio, L.; Martínez-Duran, L. Permanent and Decidua Dentition as Chronological Biomarkers of Heavy Metal Contamination: A Review of the Forensic Literature. J. Trace Elem. Med. Biol. 2024, 84, 127435. [Google Scholar] [CrossRef]
- Dantham, P.; Nuvvula, S.; Ismail, A.F.; Akkilagunta, S.; Mallineni, S.K. Association between Passive Smoking and Dental Caries Status in Children: A Cross-Sectional Analytical Study. Dent. Med. Probl. 2024, 61, 209–216. [Google Scholar] [CrossRef]
- Rayad, S.; Klimas, S.; Janeczek, M.; Małyszek, A.; Bort, M.; Małysa, A.; Dominiak, M.; Dobrzyński, M. Studies on the Content of Toxic Metals in Teeth: A Narrative Review of Literature. Dent. Med. Probl. 2024, 61, 943–961. [Google Scholar] [CrossRef]
- Jarka, J.; Angerman, A. The Sequence of Replacement of Deciduous Teeth by Permanent Teeth in the Lateral Maxillary Segments and Its Clinical Significance. Authors’ Own Observation. Forum Ortod. 2021, 17, 93–105. [Google Scholar] [CrossRef]
- Punshon, T.; Bauer, J.A.; Karagas, M.R.; Coker, M.O.; Weisskopf, M.G.; Mangano, J.J.; Bidlack, F.B.; Barr, M.N.; Jackson, B.P. Quantified Retrospective Biomonitoring of Fetal and Infant Elemental Exposure Using LA-ICP-MS Analysis of Deciduous Dentin in Three Contrasting Human Cohorts. J. Expo. Sci. Environ. Epidemiol. 2024, 34, 1000–1011. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Chen, S.-Z.; Li, Y.-Y.; Xue, R.-Y.; Duan, X.; Lin, X.-Y.; Chen, S.; Zhou, D.; Li, H.-B. Gut Dysbiosis Exacerbates Intestinal Absorption of Cadmium and Arsenic from Cocontaminated Rice in Mice Due to Impaired Intestinal Barrier Functions. Environ. Sci. Technol. 2025, 59, 3459–3471. [Google Scholar] [CrossRef]
- Zhu, Q.; Chen, B.; Zhang, F.; Zhang, B.; Guo, Y.; Pang, M.; Huang, L.; Wang, T. Toxic and Essential Metals: Metabolic Interactions with the Gut Microbiota and Health Implications. Front. Nutr. 2024, 11, 1448388. [Google Scholar] [CrossRef] [PubMed]
- Bressler, J.P.; Olivi, L.; Cheong, J.H.; Kim, Y.; Maerten, A.; Bannon, D. Metal Transporters in Intestine and Brain: Their Involvement in Metal-Associated Neurotoxicities. Hum. Exp. Toxicol. 2007, 26, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Bzikowska-Jura, A.; Wesołowska, A.; Sobieraj, P.; Nawrocka, A.; Filipek, A.; Durkalec, M.; Katryńska, D.; Jedziniak, P. Essential and Non-Essential Element Concentrations in Human Milk Samples and the Assessment of Infants’ Exposure. Sci. Rep. 2024, 14, 8140. [Google Scholar] [CrossRef]
- Furman, J.; Ćwieląg-Drabek, M. The Content of Metallic Trace Elements in Rice-Containing Products Used in the Diet of Infants and Young Children—Health Risks for Consumers. Food Chem. Toxicol. 2025, 197, 115310. [Google Scholar] [CrossRef]
- Małyszek, A.; Kiryk, S.; Kensy, J.; Kotela, A.; Michalak, M.; Kiryk, J.; Janeczek, M.; Matys, J.; Dobrzyński, M. Identification of Factors Influencing Fluoride Content in Tea Infusions: A Systematic Review. Appl. Sci. 2025, 15, 5974. [Google Scholar] [CrossRef]
- Tchounwou, P.B.; Yedjou, C.G.; Patlolla, A.K.; Sutton, D.J. Heavy Metals Toxicity and the Environment. In Molecular, Clinical and Environmental Toxicology; Springer: Basel, Switzerland, 2012; Volume 101, pp. 133–164. [Google Scholar] [CrossRef]
- Jaishankar, M.; Tseten, T.; Anbalagan, N.; Mathew, B.B.; Beeregowda, K.N. Toxicity, Mechanism and Health Effects of Some Heavy Metals. Interdiscip. Toxicol. 2014, 7, 60–72. [Google Scholar] [CrossRef]
- Kim, H.S.; Kim, Y.J.; Seo, Y.R. An Overview of Carcinogenic Heavy Metal: Molecular Toxicity Mechanism and Prevention. J. Cancer Prev. 2015, 20, 232–240. [Google Scholar] [CrossRef]
- Angon, P.B.; Islam, M.S.; Kc, S.; Das, A.; Anjum, N.; Poudel, A.; Suchi, S.A. Sources, Effects and Present Perspectives of Heavy Metals Contamination: Soil, Plants and Human Food Chain. Heliyon 2024, 10, e28357. [Google Scholar] [CrossRef]
- Wiatrak, B.; Rayad, S.; Gębarowski, T.; Hadzik, J.; Styczyńska, M.; Gedrange, T.; Dobrzyński, M.; Barg, E.; Dominiak, M. Comparative Analysis of Heavy Metal Content in Impacted Third Molars from Industrial and Non-Industrial Areas and Its Effect on the Isolation, Culture, and Proliferation of Dental Stem Cells (DSCs). J. Clin. Med. 2024, 13, 5465. [Google Scholar] [CrossRef]
- Chen, Q.Y.; DesMarais, T.; Costa, M. Metals and Mechanisms of Carcinogenesis. Annu. Rev. Pharmacol. Toxicol. 2019, 59, 537–554. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Gu, Y.; Zhou, Q.; Mao, G.; Zou, B.; Zhao, J. Combined Toxicity of Heavy Metal Mixtures in Liver Cells. J. Appl. Toxicol. 2016, 36, 1163–1172. [Google Scholar] [CrossRef] [PubMed]
- Chunhabundit, R. Cadmium Exposure and Potential Health Risk from Foods in Contaminated Area, Thailand. Toxicol. Res. 2016, 32, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Järup, L. Hazards of Heavy Metal Contamination. Br. Med. Bull. 2003, 68, 167–182. [Google Scholar] [CrossRef]
- Bryła, E.; Dobrzyński, M.; Konkol, D.; Kuropka, P.; Styczyńska, M.; Korczyński, M. Toxic Metals Content in Impacted Third Molars and Adjacent Bone Tissue in Different Groups of Patients. Materials 2021, 14, 793. [Google Scholar] [CrossRef]
- Rayad, S.; Dobrzyński, M.; Kuźniarski, A.; Styczyńska, M.; Diakowska, D.; Gedrange, T.; Klimas, S.; Gębarowski, T.; Dominiak, M. Mercury Content in Impacted Wisdom Teeth from Patients of the Legnica–Głogów Copper Area—An In Vitro Pilot Study. J. Xenobiot. 2023, 13, 463–478. [Google Scholar] [CrossRef]
- Rayad, S.; Dobrzyński, M.; Kuźniarski, A.; Styczyńska, M.; Diakowska, D.; Gedrange, T.; Klimas, S.; Gębarowski, T.; Dominiak, M. An In-Vitro Evaluation of Toxic Metals Concentration in the Third Molars from Residents of the Legnica-Głogów Copper Area and Risk Factors Determining the Accumulation of Those Metals: A Pilot Study. Appl. Sci. 2023, 13, 2904. [Google Scholar] [CrossRef]
- Piszko, P.J.; Piszko, A.; Kiryk, J.; Lubojański, A.; Dobrzyński, W.; Wiglusz, R.J.; Matys, J.; Dobrzyński, M. The Influence of Fluoride Gels on the Physicochemical Properties of Tooth Tissues and Dental Materials—A Systematic Review. Gels 2024, 10, 98. [Google Scholar] [CrossRef]
- Rygas, J.; Matys, J.; Wawrzyńska, M.; Szymonowicz, M.; Dobrzyński, M. The Use of Graphene Oxide in Orthodontics—A Systematic Review. J. Funct. Biomater. 2023, 14, 500. [Google Scholar] [CrossRef]
- Sztyler, K.; Wiglusz, R.J.; Dobrzynski, M. Review on Preformed Crowns in Pediatric Dentistry—The Composition and Application. Materials 2022, 15, 2081. [Google Scholar] [CrossRef] [PubMed]
- Coradduzza, D.; Congiargiu, A.; Azara, E.; Mammani, I.M.A.; De Miglio, M.R.; Zinellu, A.; Carru, C.; Medici, S. Heavy Metals in Biological Samples of Cancer Patients: A Systematic Literature Review. Biometals 2024, 37, 803–817. [Google Scholar] [CrossRef] [PubMed]
- Witkowska, D.; Słowik, J.; Chilicka, K. Heavy Metals and Human Health: Possible Exposure Pathways and the Competition for Protein Binding Sites. Molecules 2021, 26, 6060. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Adams, J.B.; Romdalvik, J.; Ramanujam, V.M.S.; Legator, M.S. Mercury, Lead, and Zinc in Baby Teeth of Children with Autism Versus Controls. J. Toxicol. Environ. Health Part A 2007, 70, 1046–1051. [Google Scholar] [CrossRef]
- Tvinnereim, H.M.; Eide, R.; Riise, T. Heavy Metals in Human Primary Teeth: Some Factors Influencing the Metal Concentrations. Sci. Total Environ. 2000, 255, 21–27. [Google Scholar] [CrossRef]
- Nazemisalman, B.; Bayat, N.; Darvish, S.; Nahavandi, S.; Mohseni, M.; Luchian, I. Polarography Can Successfully Quantify Heavy Metals in Dentistry. Medicina 2022, 58, 448. [Google Scholar] [CrossRef]
- Tacail, T.; Kovačiková, L.; Brůžek, J.; Balter, V. Spatial Distribution of Trace Element Ca-Normalized Ratios in Primary and Permanent Human Tooth Enamel. Sci. Total Environ. 2017, 603–604, 308–318. [Google Scholar] [CrossRef]
- Nedelescu, M.; Baconi, D.; Ciobanu, A.-M.; Manda, G. Heavy Metal Levels in Teeth and Hair Samples of Children Living in an Industrial Area. J. Environ. Prot. Ecol. 2015, 16, 926–932. [Google Scholar]
- Amr, M.A. Trace Elements in Egyptian Teeth. Int. J. Phys. Sci. 2011, 6, 6241–6245. [Google Scholar] [CrossRef]
- Gomes, V.E.; De Sousa, M.D.L.R.; Barbosa Jr Jr, F.; Krug, F.J.; Saraiva, M.D.C.P.; Cury, J.A.; Gerlach, R.F. In Vivo Studies on Lead Content of Deciduous Teeth Superficial Enamel of Preschool Children. Sci. Total Environ. 2004, 320, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, M.M.; Ly, A.R.; Goldberg, W.A.; Clarke-Stewart, K.A.; Dudgeon, J.V.; Mull, C.G.; Chan, T.J.; Kent, E.E.; Mason, A.Z.; Ericson, J.E. Heavy Metal in Children’s Tooth Enamel: Related to Autism and Disruptive Behaviors? J. Autism Dev. Disord. 2012, 42, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Rosa, M.J.; Gennings, C.; Curtin, P.; Alcala, C.S.; Lamadrid-Figueroa, H.; Tamayo-Ortiz, M.; Mercado-Garcia, A.; Torres-Olascoaga, L.; Téllez-Rojo, M.M.; Wright, R.O.; et al. Associations between Prenatal Metal and Metalloid Mixtures in Teeth and Reductions in Childhood Lung Function. Sci. Total Environ. 2024, 938, 173352. [Google Scholar] [CrossRef] [PubMed]
- Yalçın, S.S.; Çak, T.; Yalçın, S. Lower Strontium in Two Different Body Matrices in Neurodevelopmental Disorders: A Preliminary Report. J. Trace Elem. Med. Biol. 2020, 62, 126553. [Google Scholar] [CrossRef]
- Savabieasfahani, M.; Ali, S.S.; Bacho, R.; Savabi, O.; Alsabbak, M. Prenatal Metal Exposure in the Middle East: Imprint of War in Deciduous Teeth of Children. Environ. Monit. Assess. 2016, 188, 505. [Google Scholar] [CrossRef]
- Fischer, A.; Wiechuła, D.; Przybyła-Misztela, C. Changes of Concentrations of Elements in Deciduous Teeth with Age. Biol. Trace Elem. Res. 2013, 154, 427–432. [Google Scholar] [CrossRef]
- Bayo, J.; Moreno-Grau, S.; Martinez, M.J.; Moreno, J.; Angosto, J.M.; Pérez, J.J.G.; Marcos, L.G.; Moreno-Clavel, J. Environmental and Physiological Factors Affecting Lead and Cadmium Levels in Deciduous Teeth. Arch. Environ. Contam. Toxicol. 2001, 41, 247–254. [Google Scholar] [CrossRef]
- Bayo, J.; Moreno-Grau, S.; Martínez-García, M.J.; Moreno, J.M.; Angosto, J.M.; Guillén-Pérez, J.J.; García-Marcos, L.; Moreno-Clavel, J. Contributions of Risk Factors to High Lead and Cadmium Levels in Deciduous Teeth; WIT Press: Cardiff, UK, 2001; pp. 3–12. [Google Scholar]
- Dincă, M.; Daciana, P.; Ionita, D. About Oral Health of Romanian Children from Various Polluted Area Due to Heavy Metals. UPB Sci. Bull. Ser. B Chem. Mater. Sci. 2012, 74, 171–182. [Google Scholar]
- Motevasselian, F.; Abdi, K.; Ghodarati, H.; Shamshiri, A.R.; Lippert, F.; Hessari, H. The Role of Lead and Cadmium in Deciduous Teeth and Saliva on Dental Caries in Children Residing in Tehran, Iran. J. Trace Elem. Med. Biol. 2023, 79, 127209. [Google Scholar] [CrossRef]
- Johnston, J.E.; Franklin, M.; Roh, H.; Austin, C.; Arora, M. Lead and Arsenic in Shed Deciduous Teeth of Children Living Near a Lead-Acid Battery Smelter. Environ. Sci. Technol. 2019, 53, 6000–6006. [Google Scholar] [CrossRef]
- Friedman, A.; Schildroth, S.; Bauer, J.A.; Coull, B.A.; Smith, D.R.; Placidi, D.; Cagna, G.; Krengel, M.H.; Tripodis, Y.; White, R.F.; et al. Early-Life Manganese Exposure during Multiple Developmental Periods and Adolescent Verbal Learning and Memory. Neurotoxicol. Teratol. 2023, 100, 107307. [Google Scholar] [CrossRef] [PubMed]
- Sitarik, A.R.; Arora, M.; Austin, C.; Bielak, L.F.; Eggers, S.; Johnson, C.C.; Lynch, S.V.; Kyun Park, S.; Hank Wu, K.-H.; Yong, G.J.M.; et al. Fetal and Early Postnatal Lead Exposure Measured in Teeth Associates with Infant Gut Microbiota. Environ. Int. 2020, 144, 106062. [Google Scholar] [CrossRef] [PubMed]
- Ericson, J.E. Enamel Lead Biomarker for Prenatal Exposure Assessment. Environ. Res. 2001, 87, 136–140. [Google Scholar] [CrossRef] [PubMed]
- Hostynek, J.J. Factors Determining Percutaneous Metal Absorption. Food Chem. Toxicol. 2003, 41, 327–345. [Google Scholar] [CrossRef]
- Larese Filon, F.; Maina, G.; Adami, G.; Venier, M.; Coceani, N.; Bussani, R.; Massiccio, M.; Barbieri, P.; Spinelli, P. In Vitro Percutaneous Absorption of Cobalt. Int. Arch. Occup. Environ. Health 2004, 77, 85–89. [Google Scholar] [CrossRef]
- Conley, T.E.; Beaudin, S.A.; Lasley, S.M.; Fornal, C.A.; Hartman, J.; Uribe, W.; Khan, T.; Strupp, B.J.; Smith, D.R. Early Postnatal Manganese Exposure Causes Arousal Dysregulation and Lasting Hypofunctioning of the Prefrontal Cortex Catecholaminergic Systems. J. Neurochem. 2020, 153, 631–649. [Google Scholar] [CrossRef]
- Bałasz, M.; Szkilnik, R.; Brus, R.; Malinowska-Borowska, J.; Kasperczyk, S.; Nowak, D.; Kostrzewa, R.M.; Nowak, P. Perinatal Manganese Exposure and Hydroxyl Radical Formation in Rat Brain. Neurotox. Res. 2015, 27, 1–14. [Google Scholar] [CrossRef]
- Balachandran, R.C.; Mukhopadhyay, S.; McBride, D.; Veevers, J.; Harrison, F.E.; Aschner, M.; Haynes, E.N.; Bowman, A.B. Brain Manganese and the Balance between Essential Roles and Neurotoxicity. J. Biol. Chem. 2020, 295, 6312–6329. [Google Scholar] [CrossRef]
- Fatima, G.; Raza, A.M.; Dhole, P. Heavy Metal Exposure and Its Health Implications: A Comprehensive Review. Ind. J. Clin. Biochem. 2025, 1–29. [Google Scholar] [CrossRef]
- Gundacker, C.; Hengstschläger, M. The Role of the Placenta in Fetal Exposure to Heavy Metals. Wien. Med. Wochenschr. 2012, 162, 201–206. [Google Scholar] [CrossRef]
- Grandjean, P.; Landrigan, P. Developmental Neurotoxicity of Industrial Chemicals. Lancet 2006, 368, 2167–2178. [Google Scholar] [CrossRef] [PubMed]
- Nyanza, E.C.; Mhana, R.J.; Asori, M.; Thomas, D.S.K.; Kisoka, A.P. Effects of Prenatal Lead, Mercury, Cadmium, and Arsenic Exposure on Children’s Neurodevelopment in an Artisanal Small-Scale Gold Mining Area in Northwestern Tanzania Using a Multi-Chemical Exposure Model. PLoS Glob. Public Health 2025, 5, e0004577. [Google Scholar] [CrossRef] [PubMed]
- Rice, D.; Barone, S. Critical Periods of Vulnerability for the Developing Nervous System: Evidence from Humans and Animal Models. Environ. Health Perspect. 2000, 108, 511–533. [Google Scholar] [CrossRef] [PubMed]
- Szymański, M. Molecular Mechanisms of Lead Toxicity. BioTechnologia 2015, 95, 137–149. [Google Scholar] [CrossRef]
- Virgolini, M.B.; Aschner, M. Molecular Mechanisms of Lead Neurotoxicity. In Advances in Neurotoxicology; Elsevier: Amsterdam, The Netherlands, 2021; Volume 5, pp. 159–213. ISBN 978-0-12-823775-5. [Google Scholar]
- Gonzalez-Villalva, A.; Marcela, R.-L.; Nelly, L.-V.; Patricia, B.-N.; Guadalupe, M.-R.; Brenda, C.-T.; Maria Eugenia, C.-V.; Martha, U.-C.; Isabel, G.-P.; Fortoul, T.I. Lead Systemic Toxicity: A Persistent Problem for Health. Toxicology 2025, 515, 154163. [Google Scholar] [CrossRef]
- Copland, I.; Post, M. Lung Development and Fetal Lung Growth. Paediatr. Respir. Rev. 2004, 5, S259–S264. [Google Scholar] [CrossRef]
- Madrigal, J.M.; Persky, V.; Pappalardo, A.; Argos, M. Association of Heavy Metals with Measures of Pulmonary Function in Children and Youth: Results from the National Health and Nutrition Examination Survey (NHANES). Environ. Int. 2018, 121, 871–878. [Google Scholar] [CrossRef]
- Wylie, A.C.; Murgueitio, N.; Carlson, A.L.; Fry, R.C.; Propper, C.B. The Role of the Gut Microbiome in the Associations between Lead Exposure and Child Neurodevelopment. Toxicol. Lett. 2025, 408, 95–104. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Study | Aim of the Study | Material and Methods | Results | Conclusions |
|---|---|---|---|---|
| Tvinnereim et al. [38] | To assess how tooth type, presence of roots, and caries in deciduous teeth affect the concentrations of lead (Pb), cadmium (Cd), mercury (Hg), and zinc (Zn). | 1271 deciduous teeth were analyzed (without fillings) for metal content using atomic absorption spectrometry (AAS). Sample sizes varied by element: 1271 for Pb, 554 for Hg, 1235 for Cd, and 1263 for Zn. Different AAS techniques were employed: flame technique (FAAS) for Zn, graphite furnace technique (GFAAS) for Pb and Cd, and cold vapor technique (CV-AAS) for Hg. | Carious teeth showed elevated Pb, Hg, and Zn (particularly in canines/molars). Teeth with roots contained higher Pb and Zn (especially in canines/molars). Pb was highest in incisors while Hg and Zn peaked in molars. Cd showed no significant differences between groups. Positive correlations existed between Pb and Cd/Hg/Zn, while Zn–Hg correlation appeared only in carious teeth. | The elemental composition depends on the tooth type, as well as the presence of roots and dental caries. |
| Nazemisalman et al. [39] | Evaluating Zn, Cu, Cd, and Pb concentrations in children living near lead and zinc mining areas in Zanjan, Iran. | Caries tissues were removed from 42 deciduous teeth using endodontic files. Teeth were cleaned with double-distilled water, 10% HNO3, and 30% H2O2. Elements were analyzed using polarographic system with anodic stripping voltammetry (ASV). | Toxic metal concentrations were elevated in teeth of children living near lead and zinc mines. No significant differences were found based on tooth type, jaw, or age for Pb, Cd, Cu, and Zn levels. The only significant variation was in zinc levels between males and females. | Deciduous teeth have proven to be effective biological matrices, reflecting severe environmental pollution through elevated levels of toxic metals. |
| Tacail et al. [40] | To improve trace element distribution analysis in tooth enamel for toxic metal exposure assessment and dietary reconstruction, while developing an LA-ICPMS sampling framework. | The study material consisted of 10 deciduous teeth and 12 permanent teeth. The elemental content was determined using inductively coupled plasma mass spectrometry with laser ablation (LA-ICPMS). | Deciduous teeth have lower Ca than permanent teeth with no spatial variation. Pb/Ca remains constant across enamel. Cu/Ca and Ni/Ca differentiate deciduous from permanent enamel. Permanent teeth show higher Zn/Ca (increasing at surface) and elevated Sr/Ca and Ba/Ca (decreasing outward)—gradients absent in deciduous enamel. | For reliable elemental analysis of life-history exposure, laser ablation should target the enamel–dentine junction where the most complete chemical record exists. Uniform Ca levels within teeth indicate homogeneous enamel maturation before eruption. |
| Adams et al. [37] | Assessment of mercury, lead, and zinc levels in deciduous teeth of children with autism compared with a control group. | Deciduous teeth from 15 children with autism and 10 neurotypical children were analyzed using atomic absorption spectrometry: Zn via flame AAS, Pb via graphite furnace AAS, and Hg via cold vapor AAS. | Mercury levels in teeth from children with autism were more than twice the average of the control group. Lead and zinc concentrations showed no statistically significant differences between the groups. | Children with autism showed elevated mercury exposure during prenatal and early postnatal development. Oral antibiotic use disrupts gut microbiome, potentially reducing mercury excretion and increasing absorption. |
| Ericson [56] | Assessment of Pb and Ca content in deciduous tooth enamel for use as a temporal biological matrix in evaluating prenatal and postnatal exposure. | Analysis of polished, carbon-coated longitudinal sections of enamel from deciduous mandibular central incisors from 3 children (including one with multiple lead exposure sources). Lead and calcium contents were measured using secondary-ion mass spectrometry (SIMS). | Total Pb content ranged from 1.1 to 3.7 ppm. Lead body burden (BBL) correlates with environmental lead exposure, where total lead can be estimated by multiplying 208 Pb by 1.9 (208 Pb represents 52.4% of total lead) to assess cumulative prenatal and postnatal exposure. | Lead content variation across samples indicates differences in environmental conditions or individual exposure levels. Using 208 Pb measurements provides a method for evaluating cumulative lead exposure throughout development. Multiplying 208 Pb by 1.9 converts to total lead concentration, enabling estimation of overall exposure. |
| Nedelescu [41] | Assessment of toxic metal content in primary teeth and hair of children from polluted industrialized areas. | The primary teeth and hair of 6 children aged 5–12 were examined. The samples were assessed for metal content: Pb, Zn, Cr, Mn, Cu, Cd, Ni using an inductively coupled mass spectrometer. | The content of toxic metals in the teeth of children from the studied area (Copsa Mica-Ruminia) was 60–95% higher than in children from unpolluted areas. Only the level of Pb in teeth was statistically significantly overestimated. | Toxic metals accumulate in teeth and hair. Their content in these tissues can be an indicator of pollution. |
| Sitarik [55] | To investigate the association between prenatal and postnatal lead levels and intestinal bacterial and fungal microflora in the first year of life. | Stool samples were collected from children aged 1–6 months to examine microflora. Later, they collected primary teeth from the same children after exfoliation and analyzed lead content above the neonatal line. | Higher lead levels were found in black, urban, low-birth-weight babies. Lower levels were found in babies whose mothers had contact with pets in the third trimester of pregnancy. | Higher lead levels in parts of primary teeth that formed during the second trimester of pregnancy were associated with lower abundance of Candida and Aspergillus and higher abundance of Malassezia and Saccharomyces. |
| Amr [42] | Comparison of the concentrations of toxic and essential elements in primary and permanent teeth collected in the city of Al-Kanayat, Egypt. | Primary teeth from 64 children were ground and their elemental content was analyzed using inductively coupled plasma mass spectrometry. The amounts obtained were compared with those in permanent teeth. | The mean concentrations of Na, Mg, Al, Fe, Ni, Cu, Sr, Cd, Ba, Pb and U were higher in permanent teeth, whereas concentrations of Mn, Co, As, Se, Mo and Bi were higher in primary teeth. | The concentration of toxic elements is higher in permanent teeth than in primary teeth. |
| Gomes [43] | To assess lead content in primary teeth surface enamel of preschool children and compare results based on their different living environments. | Enamel biopsies were taken from primary teeth of 329 children (some from industrial areas) and lead content was measured using graphite furnace atomic absorption spectrometry. | Lead levels in children’s tooth enamel showed 68.6% of children from non-industrial areas and 56.1% from industrial areas had 100–200 μg/g, while 44.2% from non-industrial areas and 28.8% from industrial areas had <100 μg/g. | Lead concentrations in enamel biopsies taken from children living in industrial areas were significantly higher than in biopsies from children living far from industry. |
| Abdullah [44] | To measure lead, mercury and manganese concentrations in primary teeth enamel of children with autism spectrum disorder and disruptive behavior, comparing results with normally developing children. | The content of elements in the enamel from the prenatal and postnatal periods was determined separately using laser ablation inductively coupled plasma mass spectrometry. | Children with autism spectrum disorder had lower levels of manganese in their postnatal enamel than healthy children and this is the only significant difference in the compared groups. | There is no association between exposure to toxic metals in very early life and the etiology of autism spectrum disorders and disruptive behavior. |
| Rosa [45] | To investigate the relationship between elevated concentrations of toxic metals in primary teeth and a deterioration in lung function in childhood. | The content of As, Cd, Co, Cu, Mn, Ni and Pb in the dentin of primary teeth was examined by laser ablation inductively coupled plasma mass spectrometry in children with a medical history of pulmonary dysfunction and compared with the results of healthy children. | An association was found between increased levels of cadmium and manganese in the period 12 to 14 weeks before birth with impaired lung function at 8–14 years of age. | Prenatal exposure to metals is associated with impaired lung function in childhood. |
| Yalcin [46] | Comparison of the content of Ca, Mg, Zn, Cd, Hg, Pb, Cu, Cr, Fe, Mn, Mo, P, Sr in the dentin of primary teeth of children with autism spectrum disorder and ADHD with the results obtained in normally developing children. | The content of elements in the dentine of primary teeth in children with ASD or ADHD confirmed by a psychiatrist and in healthy children was examined. Inductively coupled plasma mass spectrometry was used for this purpose. | Sick children had a significantly lower Sr level and Sr/Ca ratio. | Children with ASD and ADHD have significantly lower Sr levels in the dentin of primary teeth. |
| Friedman [54] | To investigate the association between early Mn exposure and adolescent neurodevelopment. | Primary teeth dentin manganese content was measured using inductively coupled plasma mass spectrometry with laser ablation. Analysis distinguished three formation periods: prenatal, early postnatal (to ~1 year), and early childhood. | The average manganese content was higher in the prenatal period than in the postnatal period. | Associations were found between intrusion errors and prenatal Mn levels, and between short- and long-delay recall and childhood Mn levels, particularly in males. |
| Savabieasfahani [47] | To investigate the relationship between increased military activity and increased metal content in primary teeth. | Primary teeth were collected from children from Iraq and Iran. The content of Li, Mg, Ca, Cr, Mn, Zn, Sr, Ba, Pb, Th and U was measured using laser ablation-inductively coupled plasma-mass spectrometry. | Pb was present in all dental tissues, with the highest levels in children with congenital defects. Higher amounts of Zn were found in dentin than in enamel. U and Th were not present in any samples. | Children were exposed to comparable amounts of Pb and other neurotoxic metals, often prenatally. |
| Fischer [48] | Analysis of Ca, Mn, Fe, Mg, Cu, K, Cr, Pb and Cd concentrations in hard tissues of primary teeth. | The primary teeth were collected from healthy children who had lived their entire lives in Silesia. The content of elements was examined using the atomic absorption spectroscopy. | The teeth contained the most Ca, K, Mg, and the least Cd, Mn, Cu, and Cr. | The concentration of metals in the tissues of primary teeth decreases with age. |
| Bayo et al. [49] | To assess the levels of lead and cadmium in shed deciduous teeth of children from Cartagena, Spain. | All 371 deciduous teeth were labeled, refrigerated in paper bags, then analyzed for lead and cadmium using microwave acid digestion and differential pulse anodic stripping voltammetry. | Higher lead and cadmium in children’s deciduous teeth were found in socially disadvantaged families and polluted areas. Lead increased with upper jaw teeth and thumb-sucking/nail-biting. Cadmium increased in non-carious teeth and without school fluoride. Both metals concentrated more in incisors than molars and decreased with tooth weight. No sex differences observed. | Children in Cartagena showed low lead and cadmium in deciduous teeth, affected by environmental and physiological factors, with tooth type being the primary determinant. |
| Bayo et al. [50] | To present the lead and cadmium levels measured in deciduous teeth of children from Cartagena, Spain, and examine their relationships with various variables. | A total of 834 shed, deciduous teeth were collected from children and subjected to analytical determination of lead and cadmium. | Lead distribution was log-normal while cadmium was not. No sex differences found. Metal levels decreased from incisors to molars and with age. Key environmental factors: fluoride use, residential zone, home age, and family socioeconomic status (latter two affecting lead). | Cartagena residents have low lead and cadmium levels, with lead influenced by tooth type, jaw, home age, and residential zone, while cadmium was affected only by zone of residence. |
| Dinca et al. [25] | To examine the impact of toxic metals on primary teeth and the influence of different drinks on the teeth dissolution and demineralization. | A total of 93 primary teeth from areas with varying pollution levels were analyzed for toxic metals using ICP-MS and tested for dissolution in sugary and sugar-free drinks. Teeth were weighed before and after immersion, with surfaces examined using AFM and SEM. | Teeth from industrial areas had higher toxic metal content, especially zinc. Carious teeth showed higher metal levels and greater material loss in sugary drinks, which caused more demineralization and surface roughness, particularly in carious teeth. | Teeth from polluted areas show higher toxic metal levels, more material loss in sugary drinks, and greater demineralization. |
| Motevaseliana et al. [52] | Association between lead (Pb) and cadmium (Cd) levels in primary teeth and saliva and dental caries in children living in Tehran, Iran. | Primary teeth from 211 Tehran children (6–11 years) were cleaned, stimulated saliva collected via paraffin chewing, pH measured with test strips, and Pb/Cd levels in teeth and saliva determined using atomic absorption spectrophotometry. | Mean concentrations in teeth: Pb 213.26 ppb, Cd 23.75 ppb; in saliva: Pb 11.83 ppb, Cd 3.18 ppb. Posterior teeth had higher Pb (235.20 ppb) than anterior teeth (107.87 ppb, p = 0.006). No age or gender differences in metal concentrations. | Despite finding no association between Pb or Cd levels and dental caries, there were high Pb and Cd concentrations in many children’s samples. |
| Johnston et al. [53] | To investigate historical lead (Pb) exposure near a lead-acid battery recycling facility in Vernon, California by analyzing deciduous teeth as a biological matrix reflecting toxic metal exposure. | Fifty deciduous teeth from 43 Latinx children were collected to measure pre/postnatal Pb exposure and analyzed in relation to soil lead data. Pb and As concentrations were determined using LA-ICP-MS. | Mean prenatal lead (208 Pb:43Ca ratio): 4.104 × 10−4 (SD 4.123 × 10−4); postnatal: 4.109 × 10−4 (SD 3.369 × 10−4); high correlation between periods (r = 0.87). Of 50 teeth, 20 showed prenatal arsenic and 17 postnatal arsenic. Females had higher lead levels and stronger soil-to-tooth lead associations than males. Children with detectable arsenic averaged 2.5 × 10−4 (95% CI 0.20, 4.80) higher prenatal lead levels. | Environmental lead contamination creates a cycle of exposure affecting both mothers and their developing children. Association between soil lead levels and prenatal tooth lead concentrations was found. |
| Study | Study Location | Sample Type, N (Number of Samples) | Determination Method | Metals Analyzed | Levels of Concentration | Environmental Factors |
|---|---|---|---|---|---|---|
| Tvinnereim et al. [38] | 19 counties of Norway, both urban and rural areas. | 1271 deciduous teeth without fillings. Pb was determined in 1271 samples (139 incisors, including 21 with caries, 452 canines, including 45 with caries, and 680 molars, including 290 with caries), Hg in 554 (16 incisors, including 3 with caries, 152 canines, including 18 with caries, and 386 molars, including 174 with caries), Cd in 1235 (140 incisors, including 21 with caries, 442 canines, including 44 with caries, and 660 molars, including 281 with caries), and Zn in 1263 (140 incisors, including 21 with caries, 451 canines, including 45 with caries, and 238 molars, including 119 with caries). | Zn—the flame technique (FAAS), Pb and Cd—the graphite furnace technique (GFAAS), Hg—the cold vapor technique (CV-AAS). | Zn, Pb, Cd, Hg | Overall mean elemental content in deciduous teeth: 1.37 µg/g of Pb, 0.267 µg/g of Hg, 0.113 µg/g of Cd, 157 µg/g of Zn. Incisors: 1.45 µg/g of Pb, 0.06 µg/g of Hg, 0.04 µg/g of Cd, 141 µg/g of Zn. Canines: 1.17 µg/g of Pb, 0.06 µg/g of Hg, 0.04 µg/g of Cd, 134 µg/g of Zn. Molars: 1.11 µg/g of Pb, 1.10 µg/g of Hg, 0.005 µg/g of Cd, 149 µg/g of Zn. Carious: 1.36 µg/g of Pb, 0.13 µg/g of Hg, 0.05 µg/g of Cd, 169 µg/g of Zn. Non-carious: 1.10 µg/g of Pb, 0.07 µg/g of Hg, 0.04 µg/g of Cd, 133 µg/g of Zn. Carious incisors: 1.59 µg/g of Pb, 0.117 µg/g of Hg, 0.048 µg/g of Cd, 140 µg/g of Zn. Non-carious incisors: 1.42 µg/g of Pb, 0.056 µg/g of Hg, 0.043 µg/g of Cd, 141 µg/g of Zn. Carious canines: 1.41 µg/g of Pb, 0.099 µg/g of Hg, 0.039 µg/g of Cd, 136 µg/g of Zn. Non-carious canines: 1.15 µg/g of Pb, 0.060 µg/g of Hg, 0.039 µg/g of Cd, 133 µg/g of Zn. Carious molars: 1.34 µg/g of Pb, 0.136 µg/g of Hg, 0.047 µg/g of Cd, 177 µg/g of Zn. Non-carious molars: 0.97 µg/g of Pb, 0.079 µg/g of Hg, 0.044 µg/g of Cd, 131 µg/g of Zn. Roots: 1.31 µg/g of Pb, 0.09 µg/g of Hg, 0.05 µg/g of Cd, 153 µg/g of Zn. No roots: 1.00 µg/g of Pb, 0.09 µg/g of Hg, 0.04 µg/g of Cd, 129 µg/g of Zn. | Presence of caries. |
| Nazemisalman et al. [39] | Zanjan, Iran. | Forty-two deciduous teeth, divided into tooth type (incisors, molars), location (upper, lower.) | Polarographic system based on anodic stripping voltammetry (ASV). | Zn, Cd, Pb, Cu. | Overall mean elemental content: 7.66 µg/g of Pb, 5.33 µg/g of Cu, 0.0879 µg/g of Cd, 245 µg/g of Zn. Female: 8.20 µg/g of Pb, 5.91 µg/g of Cu, 0.08 µg/g of Cd, 293.16 µg/g of Zn. Male: 6.91 µg/g of Pb, 4.56 µg/g of Cu, 0.09 µg/g of Cd, 181.37 µg/g of Zn. From a donor in the age range of 1–5 years: 6.33 µg/g of Pb, 4.90 µg/g of Cu, 0.08 µg/g of Cd, 224.48 µg/g of Zn. from a donor in the age range of 5–10 years: 8.88 µg/g of Pb, 5.73 µg/g of Cu, 0.09 µg/g of Cd, 264.13 µg/g of Zn. Incisors: 8.98 µg/g of Pb, 5.02 µg/g of Cu, 0.09 µg/g of Cd, 311.32 µg/g of Zn. Molars: 7.20 µg/g of Pb, 5.44 µg/g of Cu, 0.08 µg/g of Cd, 221.80 µg/g of Zn. Upper teeth: 6.79 µg/g of Pb, 3.88 µg/g of Cu, 0.06 µg/g of Cd, 107.09 µg/g of Zn. Lower teeth: 8.02 µg/g of Pb, 5.91 µg/g of Cu, 0.10 µg/g of Cd, 214.93 µg/g of Zn. | Urban environment far from factories; high socio-economic status. |
| Tacail et al. [40] | No data. | Twelve permanent molars and ten deciduous teeth (4 incisors, 2 canines and 4 molars), longitudinally sectioned along the buccal–lingual axis. | Laser ablation inductively coupled plasma mass spectrometry (LA-ICP MS). | Ca, Cu, Zn, Ni, Sr, Ba, Pb. | No data. | No data. |
| Adams et al. [37] | Arizona State, USA. | Teeth obtained from 15 children on the autism spectrum and 11 neurotypical controls. | Hg—Cold vapor atomic absorption spectrophotometry (CV-AAS), Zn—flame atomic absorption spectrophotometer (flame AA), Pb—graphite furnace atomic absorption spectrophotometer (GFAAS). | Hg, Pb, Zn. | Mean of elements: Hg: Autism: 0.15 ± 0.11 μg/g Control: 0.07 ± 0.06 μg/g Pb: Autism: 0.38 ± 0.32 μg/g Control: 0.29 ± 0.14 μg/g Zn: Autism: 100 ± 20 μg/g Control: 98 ± 16 μg/g | Maternal fish consumption during pregnancy; Presence or placement of amalgam fillings in the mother during pregnancy; Presence of amalgam fillings in the child. Administration of anti-D immunoglobulin (Anti-Rho D) to the mother; Maternal use of antibiotics during pregnancy and antibiotic use in the child up to 48 months of age; Paint consumption (pica behavior). |
| Ericson [56] | Los Angeles, California, USA (urban area), Tijuana, Mexico (urban area) Sinaloa, Mexico (rural area). | Three longitudinal sections through the enamel of exfoliated primary mandibular central incisors. | Secondary-ion mass spectrometry (SIMS). | Pb, Ca. | Total Pb concentration: Los Angeles—1.1 ppm Tijuana—3.7 ppm Sinaloa—1.57 ppm Ca—no numeric data | Area of residence (urban/rural); Exposure to tableware covered with lead glaze; Consumption of lead-contaminated sweets; Presence of car batteries in the residence. |
| Nedelescu [41] | Industrial area Copsa Mica, Sibiu County, Romania. | Entire primary teeth-after physiological resorption; hair (no numbers of samples for either samples). | Inductively coupled plasma mass spectrometry (ICP-MS). | Cd, Pb, Cu, Zn, Cr, Mn, Co, Ni. | Tooth samples from polluted area (μg/g): Cd—0.018 Pb—0.77 Cu—0.74 Zn—52.70 Cr—11.73 Mn—1.99 Co—0.98 Ni—46.16 Tooth samples from unpolluted area (μg/g): Cd—0.012 Pb—0.08 Cu—0.52 Zn—61.51 Cr—8.33 Mn—0.43 Co—0.52 Ni—23.52 | Activity of smelter. |
| Sitarik [55] | Detroit, Michigan. | Enamel and dentine of primary teeth (N = 146). | Laser ablation inductively coupled plasma mass spectrometry (LA-ICP-MS). | Pb. | Suburban: 2nd trimester: 0.021 (0.026) 3rd trimester: 0.027 (0.030) Postnatal: 0.022 (0.028) 0.003 Urban: 2nd trimester: 0.028 (0.039) 3rd trimester: 0.041 (0.056) Postnatal: 0.033 (0.027) | Location of residence; Environmental tobacco smoke during pregnancy; Mother smoked during pregnancy; Prenatal indoor pets; Year house was built; Prenatal antibiotic use; Prenatal antifungal use; Season of birth. |
| Amr [42] | El-Kanayat City, Egypt. | Sixty-four primary teeth pulp. | Inductively coupled plasma mass spectrometry (ICP-MS). | Na, Mg, Al, Cr, Zn, Ag, Fe, Ni, Cu, Sr, Cd, Ba, Pb, U, Mn, Co, As, Se, Mo, Bi. | Na 5454 ± 950 ppm Mg 1755 ± 340 ppm Al 17.9 ± 12.3 ppm Cr 0.04 ± 0.01 ppm Mn 5.5 ± 2 ppm Co 0.54 ± 0.12 ppm Fe 80.1 ± 16.5 ppm Ni 1.66 ± 0.46 ppm Cu 6.4 ± 4.8 ppm Zn 133 ± 30 ppm As 0.82 ± 0.07 ppm Se 10.5 ± 1.57 ppm Sr 87 ± 11.3 ppm Mo 1.8 ± 0.29 ppm Ag 0.08 ± 0.03 ppm Cd 0.00011 ± 0.00001 ppm Ba 7.8 ± 3.2 ppm Pb 1.2 ± 0.89 ppm Bi 23 ± 2.34 ppm U 0.005 ± 0.002 ppm | No data. |
| Gomes [43] | Piracicaba, Brazil. | Enamel of primary teeth (N = 329). | Graphite furnace atomic absorption spectrometry (GFAAS). | Pb. | Non-industrial 183.1 (190.6) μg /g Industrial 275.5 (326.7) μg /g | Industrial area. |
| Abdullah [44] | No data. | Enamel of primary teeth (N = 84). | Laser ablation inductively coupled plasma mass spectrometry (LA-ICP-MS). | Pb, Hg, Mn. | Prenatal Pb ASD = 0.27 (0.27) ppm TD = 0.38 (0.59) ppm HDB = 0.33 (0.33) ppm TD = 0.32 (0.36) ppm Postnatal Pb ASD = 0.29 (0.29) ppm TD = 0.43 (0.61) ppm HDB = 1.10 (3.47) ppm TD = 0.22 (0.23) ppm Prenatal Hg ASD = 1.42 (0.61) ppm TD = 1.90 (2.79) ppm HDB = 1.27 (0.76) ppm TD = 1.82 (2.34) ppm Postnatal Hg ASD = 1.47 (0.77) ppm TD = 1.45 (0.90) ppm HDB = 1.01 (0.45) ppm TD = 1.22 (0.70) ppm Prenatal Mn ASD = 1.41 (1.10) ppm TD = 1.63 (0.95) ppm HDB = 1.62 (0.77) ppm TD = 1.58 (0.88) ppm Postnatal Mn ASD = 1.87 (2.01) ppm TD = 2.91 (2.43) ppm HDB = 2.11 (2.22) ppm TD = 1.80 (1.70) ppm | No data. |
| Rosa [45] | Mexico City, Mexico. | Dentin of primary teeth (N = 291). | Laser ablation inductively coupled plasma mass spectrometry (LA-ICP-MS). | As, Cd, Co, Cu, Mn, Ni, Pb. | Mn = 0.41 Cd = 0.30 Pb = 0.17 As = 0.09 Co = 0.02 Ni = 0.01 Cu = 0.00 | No data. |
| Yalcin [46] | Ankara, Turkey. | Dentin of primary teeth (N = 25). | Inductively coupled plasma mass spectrometry (ICP-MS). | Ca, Mg, Zn, Cd, Hg, Pb, Cu, Cr, Fe, Mn, Mo, P, Sr. | Mg, mg/g TDC = 6.1 NDD = 5.5 P, mg/g TDC = 143 NDD = 129 Ca, mg/g TDC = 251 NDD = 248 Cr, μg/g TDC = 0.06 NDD = 0.07 Mn, μg/g TDC = 1.02 NDD = 0.58 Fe, μg/g TDC = 4.05 NDD = 3.77 Cu, μg/g TDC = 0.12 NDD = 0.24 Zn, μg/g TDC = 106 NDD = 101 Sr, μg/g TDC = 95.2 NDD = 54.2 Mo, μg/g TDC = 0.02 NDD = 0.03 Cd, μg/g TDC = 0.002 NDD = 0.002 Pb, μg/g TDC = 0.57 NDD = 0.68 Hg, μg/g TDC and NDD < DL | Smoking exposure. |
| Friedman [54] | Bagnolo Mella, Valcamonica and Garda Lake, Italy. | Dentin of primary teeth (N = 280). | Laser ablation inductively coupled plasma mass spectrometry (LA-ICP-MS). | Mn. | Patients with intrusion errors: Prenatal = 0.23 Postnatal = 1.16 Childhood = 1.09 Patients with perseveration errors: Prenatal = 1.50 Postnatal = 0.92 Childhood = 1.00 | Active/historical/no history of ferroalloy production. |
| Savabieasfahani [47] | Iraq, Iran, Lebanon. | Dentin and enamel of primary teeth (N = 9). | Laser ablation inductively coupled plasma mass spectrometry (LA-ICP-MS). | Li, Mg, Ca, Cr, Mn, Zn, Sr, Ba, Pb, Th, U. | No data | War zone. |
| Fischer [48] | Silesia, Poland. | Primary teeth (N = 45). | Flame atomic absorption spectrometry (FAAS). | Ca, Mn, Fe, Mg, Cu, K, Cr, Pb and Cd. | Mn 4.39 μg/g Fe 51.0 μg/g Pb 13.4 μg/g Cd 0.70 μg/g Cu 4.62 μg/g Cr 8.97 μg/g K 240 μg/g Ca 20.0 μg/g Mg 2367 μg/g | No data. |
| Bayo et al. [49] | Three zones in Cartagena, Spain- nonpolluted zone, polluted zone, intermediate zone. | Three hundred and seventy-one deciduous teeth; entire incisors, canines and molars. | Differential pulse anodic stripping voltammetry (DPASV). | Pb, Cd. | Pb (~3.5 μg/g): Higher in upper jaw, non-carious teeth, thumb-sucking/nail-biting habits, disadvantaged families, polluted areas, smoking fathers, no school fluoride. Decreases from incisors to molars. Cd (~58 ng/g): Higher in non-carious teeth, polluted zones, older houses, no school fluoride. Decreases from incisors to molars. | Home antiquity, socioeconomic status, parents’ smoking habit, thumb-sucking and nail-biting habits, pollution of the residential zone, use of fluoride. |
| Bayo et al. [50] | Cartagena, Spain. | Eight hundred and thirty-four shed, deciduous teeth. | Differential pulse anodic stripping voltammetry (DPASV). | Pb and Cd. | Cd: 59.776 ± 63.68 μg/g; lower in older children, with fluoride use, in upper jaw, and in incisors. Pb: 4.17 ± 2.64 μg/g; lower in newer houses, older children, higher socioeconomic status, non-smoking fathers, school fluoride use, less-polluted areas, upper jaw, and incisors. | Home antiquity, family socio-economic status, parents’ smoking habit, thumb-sucking habit, zone of residence, use of fluoride. |
| Dinca et al. [25] | Bucharest, Romania Pătârlagele city as a less polluted city and Slatina city as more polluted. | Ninety-three deciduous teeth; carious and non-carious. | Inductively coupled plasma mass spectrometry (ICP-MS). | Cu, Pb, Cd, Cr, Zn. | Cd: Pătârlagele: Carious: 0.06 ppb Non-carious: 0.04 ppb Slatina: Carious: 0.13 ppb Non-carious: 0.08 ppb Pb: Pătârlagele: Carious: 0.05 ppb Non-carious: 0.02 ppb Slatina: Carious: 0.075 ppb Non-carious: 0.063 ppb Cr: Pătârlagele: Carious: 1.22 ppb Non-carious: 0.8 ppb Slatina: Carious: 1.27 ppb Non-carious: 1.10 ppb Cu: Pătârlagele: Carious: 0.3 ppb Non-carious: 0.08 ppb Slatina: Carious: 0.72 ppb Non-carious: 0.41 ppb Zn: Pătârlagele: Carious: 221.36 ppb Non-carious: 435.78 ppb Slatina: Carious: 199.44 ppb Non-carious: 385.60 ppb | Air pollution. |
| Motevaseliana et al. [52] | Tehran, Iran. | Anterior and posterior deciduous teeth with and without caries; N = 211. | Graphite furnace atomic absorption spectrometry (GFAAS). | Pb, Cd. | Teeth: - Pb: 213.26 ppb (95% CI: 164.29–274.84 ppb) - Cd: 23.75 ppb (95% CI: 20.86–27.05 ppb) Saliva: - Pb: 11.83 ppb (95% CI: 10.71–13.06 ppb) - Cd: 3.18 ppb (95% CI: 2.69–3.75 ppb) | - Socioeconomic status (family income, parental education, housing status); - Region of residence within Tehran (affluent vs. non-affluent areas); - Oral hygiene behaviors (tooth brushing frequency, dental visits); - Dietary habits (snacking frequency); - Passive smoking; - Salivary pH. |
| Authors | 1. Is It Clear in the Study What Is the “Cause” and What Is the “Effect”? | 2. Were the Participants Included in Any Similar Comparisons? | 3. Were the Participants Included in Any Comparisons Receiving Similar Treatment/Care, Other than the Exposure or Intervention of Interest? | 4. Was There a Control Group? | 5. Were There Multiple Measurements of the Outcome Both Pre- and Post- Intervention/ Exposure? | 6. Was Follow Up Complete and If Not, Were Differences Between Groups in Terms of Their Follow Up Adequately Described and Analyzed? | 7. Were the Outcomes of Participants Included in Any Comparisons Measured in the Same Way? | 8. Were Outcomes Measured in a Reliable Way? | 9. Was Appropriate Statistical Analysis Used? |
|---|---|---|---|---|---|---|---|---|---|
| Tvinnereim [38] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
| Nazemisalman [39] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes |
| Tacail [40] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | No |
| Adams [37] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
| Ericson [56] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | No |
| Nedelescu [41] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
| Sitarik [55] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes |
| Amr [42] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes |
| Gomes [43] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
| Abdullah [44] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes |
| Rosa [45] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes |
| Yalcin [46] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
| Friedman [54] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes |
| Savabieasfahani [47] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | No |
| Fischer [48] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes |
| Bayo [49] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes |
| Bayo [50] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes |
| Dinca [25] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
| Motevaseliana [52] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes |
| Johnston [53] | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zawiślak, I.; Kiryk, S.; Kiryk, J.; Kotela, A.; Kensy, J.; Michalak, M.; Matys, J.; Dobrzyński, M. Toxic Metal Content in Deciduous Teeth: A Systematic Review. Toxics 2025, 13, 556. https://doi.org/10.3390/toxics13070556
Zawiślak I, Kiryk S, Kiryk J, Kotela A, Kensy J, Michalak M, Matys J, Dobrzyński M. Toxic Metal Content in Deciduous Teeth: A Systematic Review. Toxics. 2025; 13(7):556. https://doi.org/10.3390/toxics13070556
Chicago/Turabian StyleZawiślak, Ireneusz, Sylwia Kiryk, Jan Kiryk, Agnieszka Kotela, Julia Kensy, Mateusz Michalak, Jacek Matys, and Maciej Dobrzyński. 2025. "Toxic Metal Content in Deciduous Teeth: A Systematic Review" Toxics 13, no. 7: 556. https://doi.org/10.3390/toxics13070556
APA StyleZawiślak, I., Kiryk, S., Kiryk, J., Kotela, A., Kensy, J., Michalak, M., Matys, J., & Dobrzyński, M. (2025). Toxic Metal Content in Deciduous Teeth: A Systematic Review. Toxics, 13(7), 556. https://doi.org/10.3390/toxics13070556