
Associations of Insecticide Exposure with Childhood Asthma and Wheezing: A Population-Based Cross-Sectional Study in Sanya, China

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Site and Population
2.2. Outcomes
- (i)
- Ever asthma: Has your child ever been diagnosed with asthma by a doctor?
- (ii)
- Ever wheezing: Has your child ever experienced wheezing, whistling, or dyspnea?
- (iii)
- Current wheezing: Has your child had wheezing, whistling, or dyspnea symptoms in the past 12 months?
2.3. Main Exposure
- (i)
- Exposure or not: Have you used insecticide in the past 12 months? Yes or no;
- (ii)
- If yes, where have you used insecticide? Outdoor, indoor, or for pets;
- (iii)
- If yes, what frequency do you use insecticides? Only once, once per half year, once per quarter, once per month, or once per week.
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Basic Characteristics
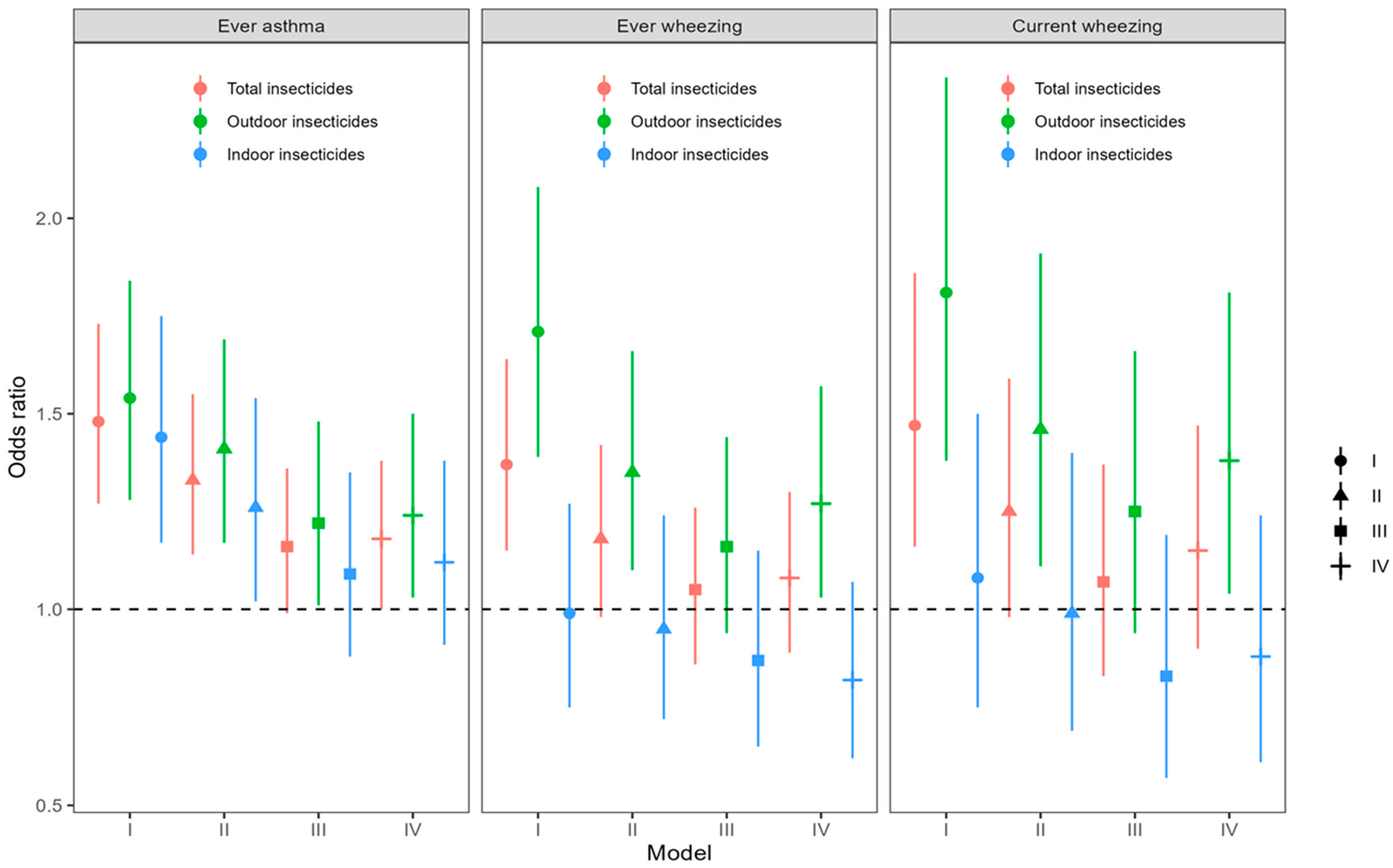
3.2. Association of Insecticide Exposure with Asthma/Wheezing in Children
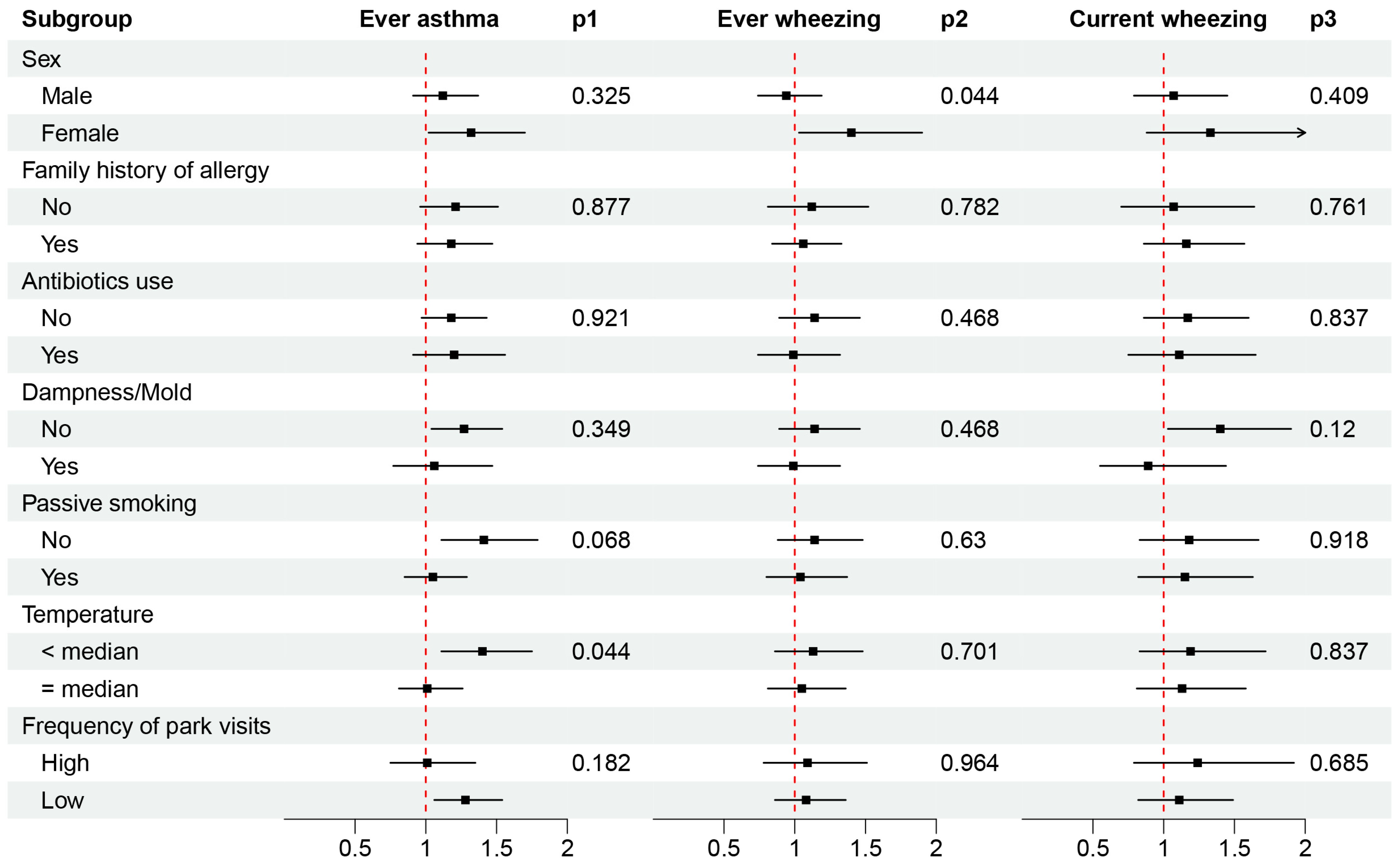
3.3. Effect Modification
4. Discussion
4.1. Key Findings
4.2. Comparison with Other Studies
4.3. Potential Mechanisms
4.4. Strengths and Limitations
4.5. Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2019 Chronic Respiratory Diseases Collaborators (GBD2019CRDC). Global burden of chronic respiratory diseases and risk factors, 1990–2019: An update from the Global Burden of Disease Study 2019. EClinicalMedicine 2023, 5, 101936. [Google Scholar] [CrossRef]
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the global burden of disease study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef] [PubMed]
- Global Asthma Network (GAN). The Global Asthma Report 2022. 2022. Available online: http://globalasthmareport.org/resources/Global_Asthma_Report_2022.pdf (accessed on 9 June 2023).
- Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and Prevention, 2023. 2023. Available online: https://ginasthma.org/wp-content/uploads/2023/05/GINA-2023-Full-Report-2023-WMS.pdf (accessed on 9 June 2023).
- Reddel, H.K.; Bacharier, L.B.; Bateman, E.D.; Brightling, C.E.; Brusselle, G.G.; Buhl, R.; Cruz, A.A.; Duijts, L.; Drazen, J.M.; FitzGerald, J.M.; et al. Global initiative for asthma strategy 2021: Executive summary and rationale for key changes. Eur. Respir. J. 2022, 59, 2102730. [Google Scholar] [CrossRef] [PubMed]
- Asher, M.I.; E Rutter, C.; Bissell, K.; Chiang, C.-Y.; El Sony, A.; Ellwood, E.; Ellwood, P.; García-Marcos, L.; Marks, G.B.; Morales, E.; et al. Worldwide trends in the burden of asthma symptoms in school-aged children: Global asthma network phase I cross-sectional study. Lancet 2021, 398, 1569–1580. [Google Scholar] [CrossRef] [PubMed]
- Pijnenburg, M.W.; Fleming, L. Advances in understanding and reducing the burden of severe asthma in children. Lancet Respir. Med. 2020, 8, 1032–1044. [Google Scholar] [CrossRef] [PubMed]
- von Mutius, E.; Smits, H.H. Primary prevention of asthma: From risk and protective factors to targeted strategies for prevention. Lancet 2020, 396, 854–866. [Google Scholar] [CrossRef] [PubMed]
- Yi, N.; Liu, T.; Zhou, Y.; Qi, J.; Shen, K.; Zhou, M. Disease burden of asthma among children and adolescents in China, 1990-2019. Chin. J. Epidemiol. 2023, 44, 235–242. (In Chinese) [Google Scholar] [CrossRef]
- Hu, Y.-B.; Chen, Y.-T.; Liu, S.-J.; Jiang, F.; Wu, M.-Q.; Yan, C.-H.; Tan, J.-G.; Yu, G.-J.; Hu, Y.; Yin, Y.; et al. Increasing prevalence and influencing factors of childhood asthma: A cross-sectional study in Shanghai, China. World J. Pediatr. 2021, 17, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Kelchtermans, J.; Hakonarson, H. The role of gene-ambient air pollution interactions in paediatric asthma. Eur. Respir. Rev. 2022, 31, 220094. [Google Scholar] [CrossRef] [PubMed]
- Achakulwisut, P.; Brauer, M.; Hystad, P.; Anenberg, S.C. Global, national, and urban burdens of paediatric asthma incidence attributable to ambient NO2 pollution: Estimates from global datasets. Lancet Planet. Health 2019, 3, e166–e178. [Google Scholar] [CrossRef]
- Alotaibi, R.; Bechle, M.; Marshall, J.D.; Ramani, T.; Zietsman, J.; Nieuwenhuijsen, M.J.; Khreis, H. Traffic related air pollution and the burden of childhood asthma in the contiguous united states in 2000 and 2010. Environ. Int. 2019, 127, 858–867. [Google Scholar] [CrossRef] [PubMed]
- Altman, M.C.; Kattan, M.; O'Connor, G.T.; Murphy, R.C.; Whalen, E.; LeBeau, P.; Calatroni, A.; A Gill, M.; Gruchalla, R.S.; Liu, A.H.; et al. Associations between outdoor air pollutants and non-viral asthma exacerbations and airway inflammatory responses in children and adolescents living in urban areas in the USA: A retrospective secondary analysis. Lancet Planet. Health 2023, 7, e33–e44. [Google Scholar] [CrossRef] [PubMed]
- Anenberg, S.C.; Mohegh, A.; Goldberg, D.L.; Kerr, G.H.; Brauer, M.; Burkart, K.; Hystad, P.; Larkin, A.; Wozniak, S.; Lamsal, L. Long-term trends in urban NO2 concentrations and associated paediatric asthma incidence: Estimates from global datasets. Lancet Planet. Health 2022, 6, e49–e58. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Cheng, J.; Jiang, F.; Liu, S.; Li, S.; Tan, J.; Yin, Y.; Tong, S. Season-stratified effects of meteorological factors on childhood asthma in shanghai, china. Environ. Res. 2020, 191, 110115. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Cheng, J.; Yin, Y.; Liu, S.; Tan, J.; Li, S.; Wu, M.; Yan, C.; Yu, G.; Hu, Y.; et al. Association of childhood asthma with intra-day and inter-day temperature variability in shanghai, china. Environ. Res. 2022, 204, 112350. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Xu, Z.; Jiang, F.; Li, S.; Liu, S.; Wu, M.; Yan, C.; Tan, J.; Yu, G.; Hu, Y.; et al. Relative impact of meteorological factors and air pollutants on childhood allergic diseases in shanghai, china. Sci. Total Environ. 2020, 706, 135975. [Google Scholar] [CrossRef] [PubMed]
- Khreis, H.; Cirach, M.; Mueller, N.; de Hoogh, K.; Hoek, G.; Nieuwenhuijsen, M.J.; Rojas-Rueda, D. Outdoor air pollution and the burden of childhood asthma across Europe. Eur. Respir. J. 2019, 54, 1802194. [Google Scholar] [CrossRef] [PubMed]
- Lavigne, E.; Talarico, R.; van Donkelaar, A.; Martin, R.; Stieb, D.M.; Crighton, E.; Weichenthal, S.; Smith-Doiron, M.; Burnett, R.T.; Chen, H. Fine particulate matter concentration and composition and the incidence of childhood asthma. Environ. Int. 2021, 152, 106486. [Google Scholar] [CrossRef]
- Lu, C.; Zhang, Y.; Li, B.; Zhao, Z.; Huang, C.; Zhang, X.; Qian, H.; Wang, J.; Liu, W.; Sun, Y.; et al. Interaction effect of prenatal and postnatal exposure to ambient air pollution and temperature on childhood asthma. Environ. Int. 2022, 167, 107456. [Google Scholar] [CrossRef]
- Olsson, D.; Forsberg, B.; Braback, L.; Geels, C.; Brandt, J.; Christensen, J.H.; Frohn, L.M.; Oudin, A. Early childhood exposure to ambient air pollution is associated with increased risk of paediatric asthma: An administrative cohort study from stockholm, sweden. Environ. Int. 2021, 155, 106667. [Google Scholar] [CrossRef]
- To, T.; Zhu, J.; Stieb, D.; Gray, N.; Fong, I.; Pinault, L.; Jerrett, M.; Robichaud, A.; Menard, R.; van Donkelaar, A.; et al. Early life exposure to air pollution and incidence of childhood asthma, allergic rhinitis and eczema. Eur. Respir. J. 2020, 55, 1900913. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Zhang, Y.; Wei, J.; Zhao, Z.; Norback, D.; Zhang, X.; Lu, C.; Yu, W.; Wang, T.; Zheng, X.; et al. Associations of early-life exposure to submicron particulate matter with childhood asthma and wheeze in china. JAMA Netw. Open 2022, 5, e2236003. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Yin, Z.; Zhou, P.; Zhang, L.; Zhao, Z.; Norback, D.; Zhang, X.; Lu, C.; Yu, W.; Wang, T.; et al. Early-life exposure to PM2.5 constituents and childhood asthma and wheezing: Findings from China, Children, Homes, Health study. Environ. Int. 2022, 165, 107297. [Google Scholar] [CrossRef] [PubMed]
- Maritano, S.; Moirano, G.; Popovic, M.; D'Errico, A.; Rusconi, F.; Maule, M.; Richiardi, L. Maternal pesticides exposure in pregnancy and the risk of wheezing in infancy: A prospective cohort study. Environ. Int. 2022, 163, 107229. [Google Scholar] [CrossRef] [PubMed]
- Mora, A.M.; Hoppin, J.A.; Córdoba, L.; Cano, J.C.; Soto-Martínez, M.; Eskenazi, B.; Lindh, C.H.; Joode, B.v.W.d. Prenatal pesticide exposure and respiratory health outcomes in the first year of life: Results from the infants’ Environmental Health (ISA) study. Int. J. Hyg. Environ. Health 2020, 225, 113474. [Google Scholar] [CrossRef] [PubMed]
- Raanan, R.; Harley, K.G.; Balmes, J.R.; Bradman, A.; Lipsett, M.; Eskenazi, B. Early-life exposure to organophosphate pesticides and pediatric respiratory symptoms in the CHAMACOS cohort. Environ. Health Perspect. 2015, 123, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Weselak, M.; Arbuckle, T.E.; Wigle, D.T.; Krewski, D. In utero pesticide exposure and childhood morbidity. Environ. Res. 2007, 103, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Xiao, S.; Ngo, A.L.; Mendola, P.; Bates, M.N.; Barcellos, A.L.; Ferrara, A.; Zhu, Y. Household mold pesticide use childhood asthma: A nationwide study in the, U.S. Int. J. Hyg. Environ. Health 2021, 233, 113694. [Google Scholar] [CrossRef]
- Asher, M.; Keil, U.; Anderson, H.; Beasley, R.; Crane, J.; Martinez, F.; Mitchell, E.; Pearce, N.; Sibbald, B.; Stewart, A.; et al. International Study of Asthma and Allergies in Childhood (ISAAC): Rationale and methods. Eur. Respir. J. 1995, 8, 483–491. [Google Scholar] [CrossRef]
- Bornehag, C.G.; Sundell, J.; Sigsgaard, T. Dampness in buildings and health (DBH): Report from an ongoing epidemiological investigation on the association between indoor environmental factors and health effects among children in Sweden. Indoor Air 2004, 14, 59–66. [Google Scholar] [CrossRef]
- Hu, Y.; Liu, W.; Huang, C.; Zou, Z.J.; Zhao, Z.H.; Shen, L.; Sundell, J. Home dampness, childhood asthma, hay fever, and airway symptoms in Shanghai, China: Associations, dose-response relationships, and lifestyle’s influences. Indoor Air 2014, 24, 450–463. [Google Scholar] [CrossRef] [PubMed]
- Textor, J.; van der Zander, B.; Gilthorpe, M.S.; Liskiewicz, M.; Ellison, G.T. Robust causal inference using directed acyclic graphs: The R package ‘dagitty’. Int. J. Epidemiol. 2016, 45, 1887–1894. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.G.; Bland, J.M. Interaction revisited: The difference between two estimates. BMJ 2003, 326, 219. [Google Scholar] [CrossRef]
- Chen, Y.; Zhu, J.; Lyu, J.; Xia, Y.; Ying, Y.; Hu, Y.; Qu, J.; Tong, S.; Li, S. Association of maternal prepregnancy weight and gestational weight gain with children’s allergic diseases. JAMA Netw. Open 2020, 3, e2015643. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Chen, Y.; Liu, S.; Jiang, F.; Wu, M.; Yan, C.; Tan, J.; Yu, G.; Hu, Y.; Yin, Y.; et al. Breastfeeding duration modified the effects of neonatal and familial risk factors on childhood asthma and allergy: A population-based study. Respir. Res. 2021, 22, 41. [Google Scholar] [CrossRef]
- Gascon, M.; Vrijheid, M.; Martínez, D.; Ballester, F.; Basterrechea, M.; Blarduni, E.; Esplugues, A.; Vizcaino, E.; Grimalt, J.O.; Morales, E.; et al. Pre-natal exposure to dichlorodiphenyldichloroethylene and infant lower respiratory tract infections and wheeze. Eur. Respir. J. 2012, 39, 1188–1196. [Google Scholar] [CrossRef]
- Sunyer, J.; Torrent, M.; Muñoz-Ortiz, L.; Ribas-Fitó, N.; Carrizo, D.; Grimalt, J.; Antó, J.M.; Cullinan, P. Prenatal dichlorodiphenyldichloroethylene (DDE) and asthma in children. Environ. Health Perspect. 2005, 113, 1787–1790. [Google Scholar] [CrossRef]
- Perla, M.E.; Rue, T.; Cheadle, A.; Krieger, J.; Karr, C.J. Biomarkers of Insecticide Exposure and Asthma in Children: A National Health and Nutrition Examination Survey (NHANES) 1999–2008 Analysis. Arch. Environ. Occup. Health 2015, 70, 309–322. [Google Scholar] [CrossRef]
- Islam, J.Y.; Hoppin, J.; Mora, A.M.; E Soto-Martinez, M.; Gamboa, L.C.; Castañeda, J.E.P.; Reich, B.; Lindh, C.; Joode, B.v.W.d. Respiratory and allergic outcomes among 5-year-old children exposed to pesticides. Thorax 2023, 78, 41–49. [Google Scholar] [CrossRef]
- Levin, M.E.; Botha, M.; Basera, W.; Facey-Thomas, H.E.; Gaunt, B.; Gray, C.L.; Kiragu, W.; Ramjith, J.; Watkins, A.; Genuneit, J. Environmental factors associated with allergy in urban and rural children from the South African Food Allergy (SAFFA) cohort. J. Allergy Clin. Immunol. 2020, 145, 415–426. [Google Scholar] [CrossRef]
- Patrick, D.M.; Sbihi, H.; Dai, D.L.Y.; Al Mamun, A.; Rasali, D.; Rose, C.; Marra, F.; Boutin, R.C.T.; Petersen, C.; Stiemsma, L.T.; et al. Decreasing antibiotic use, the gut microbiota, and asthma incidence in children: Evidence from population-based and prospective cohort studies. Lancet Respir. Med. 2020, 8, 1094–1105. [Google Scholar] [CrossRef] [PubMed]
- Slob, E.M.; Brew, B.K.; Vijverberg, S.J.; Kats, C.J.; Longo, C.; Pijnenburg, M.W.; van Beijsterveldt, T.C.; Dolan, C.V.; Bartels, M.; Magnusson, P.; et al. Early-life antibiotic use and risk of asthma and eczema: Results of a discordant twin study. Eur. Respir. J. 2020, 55, 1902021. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Wang, T.; Liu, J.; Li, C. A comparative study on sub-health of traditional Chinese medicine between the middle-aged and elderly migratory bird population in Sanya and the middle-aged and elderly population in northern China. China Pract. Med. 2022, 17, 149–151. [Google Scholar] [CrossRef]
- Hu, Y.; Chen, Y.; Liu, S.; Tan, J.; Yu, G.; Yan, C.; Yin, Y.; Li, S.; Tong, S. Residential greenspace and childhood asthma: An intra-city study. Sci. Total Environ. 2023, 857, 159792. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Chen, Y.; Liu, S.; Tan, J.; Yu, G.; Yan, C.; Yin, Y.; Li, S.; Tong, S. Higher greenspace exposure is associated with a decreased risk of childhood asthma in Shanghai—A megacity in China. Ecotoxicol. Environ. Saf. 2023, 256, 114868. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H.; Kabir, E.; Jahan, S.A. Exposure to pesticides and the associated human health effects. Sci. Total Environ. 2017, 575, 525–535. [Google Scholar] [CrossRef]
- Duramad, P.; Harley, K.; Lipsett, M.; Bradman, A.; Eskenazi, B.; Holland, N.T.; Tager, I.B. Early environmental exposures and intracellular Th1/Th2 cytokine profiles in 24-month-old children living in an agricultural area. Environ. Health Perspect. 2006, 114, 1916–1922. [Google Scholar] [CrossRef] [PubMed]
- Hoppin, J.A.; Umbach, D.M.; London, S.J.; Henneberger, P.K.; Kullman, G.J.; Coble, J.; Alavanja, M.C.R.; Freeman, L.E.B.; Sandler, D.P. Pesticide use and adult-onset asthma among male farmers in the Agricultural Health Study. Eur. Respir. J. 2009, 34, 1296–1303. [Google Scholar] [CrossRef]
- Helali, I.; Ferchichi, S.; Maaouia, A.; Aouni, M.; Harizi, H. Modulation of macrophage functionality induced in vitro by chlorpyrifos and carbendazim pesticides. J. Immunotoxicol. 2016, 13, 745–750. [Google Scholar] [CrossRef]
- Xu, R.-F.; Mei, H.; Chen, L.; Tang, B.; Lu, Q.-Y.; Cai, F.-S.; Yan, X.; Zheng, J.; Shen, X.-T.; Yu, Y.-J. Development and validation of an HPLC-MS/MS method for the simultaneous analysis of volatile organic compound metabolites, hydroxylated polycyclic aromatic hydrocarbons, and 8-hydroxy-2′-deoxyguanosine in human urine. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2023, 1229, 123885. [Google Scholar] [CrossRef]
- Benka-Coker, W.; Hoskovec, L.; Severson, R.; Balmes, J.; Wilson, A.; Magzamen, S. The joint effect of ambient air pollution and agricultural pesticide exposures on lung function among children with asthma. Environ. Res. 2020, 190, 109903. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Characteristics | Overall, N = 9754 | Ever Asthma | p-Value 1 | Ever Wheezing | p-Value 1 | Current Wheezing | p-Value 1 | |||
|---|---|---|---|---|---|---|---|---|---|---|
| No, N = 9028 | Yes, N = 726 | No, N = 9234 | Yes, N = 520 | No, N = 9471 | Yes, N = 283 | |||||
| Child age, years, median (IQR) | 6.7 (2.9) | 6.7 (2.9) | 6.7 (3.0) | 0.600 | 6.7 (2.9) | 7.1 (2.7) | <0.001 | 6.7 (2.9) | 6.6 (3.0) | 0.700 |
| Sex, n (%) | <0.001 | <0.001 | <0.001 | |||||||
| Male | 5345 (54.8) | 4893 (91.5) | 452 (8.5) | 5010 (93.7) | 335 (6.3) | 5158 (96.5) | 187 (3.5) | |||
| Female | 4409 (45.2) | 4135 (93.8) | 274 (6.2) | 4224 (95.8) | 185 (4.2) | 4313 (97.8) | 96 (2.2) | |||
| Household income per month, CNY, n (%) | 0.038 | <0.001 | 0.003 | |||||||
| <3000 | 2932 (30.1) | 2689 (91.7) | 243 (8.3) | 2817 (96.1) | 115 (3.9) | 2854 (97.3) | 78 (2.7) | |||
| 3000–5999 | 2782 (28.5) | 2578 (92.7) | 204 (7.3) | 2645 (95.1) | 137 (4.9) | 2721 (97.8) | 61 (2.2) | |||
| 6000–8999 | 1586 (16.3) | 1459 (92.0) | 127 (8.0) | 1491 (94.0) | 95 (6.0) | 1537 (96.9) | 49 (3.1) | |||
| 9000–11,999 | 1022 (10.5) | 953 (93.2) | 69 (6.8) | 945 (92.5) | 77 (7.5) | 977 (95.6) | 45 (4.4) | |||
| >12,000 | 1432 (14.7) | 1349 (94.2) | 83 (5.8) | 1336 (93.3) | 96 (6.7) | 1382 (96.5) | 50 (3.5) | |||
| Gestational week, weeks, n (%) | 0.005 | 0.002 | 0.046 | |||||||
| <37 | 549 (5.7) | 497 (90.5) | 52 (9.5) | 505 (92.0) | 44 (8.0) | 528 (96.2) | 21 (3.8) | |||
| 37–42 | 8762 (90.3) | 8136 (92.9) | 626 (7.1) | 8318 (94.9) | 444 (5.1) | 8519 (97.2) | 243 (2.8) | |||
| ≥42 | 392 (4.0) | 350 (89.3) | 42 (10.7) | 363 (92.6) | 29 (7.4) | 374 (95.4) | 18 (4.6) | |||
| Unknown | 51 | 45 | 6 | 48 | 3 | 50 | 1 | |||
| History of miscarriage, n (%) | 2283 (23.4) | 2079 (91.1) | 204 (8.9) | 0.002 | 2121 (92.9) | 162 (7.1) | <0.001 | 2188 (95.8) | 95 (4.2) | <0.001 |
| Family history of allergy, n (%) | 3079 (31.6) | 2691 (87.4) | 388 (12.6) | <0.001 | 2738 (88.9) | 341 (11.1) | <0.001 | 2890 (93.9) | 189 (6.1) | <0.001 |
| Antibiotic use during pregnancy, n (%) | 193 (2.0) | 161 (83.4) | 32 (16.6) | <0.001 | 161 (83.4) | 32 (16.6) | <0.001 | 179 (92.7) | 14 (7.3) | <0.001 |
| Antibiotic use within the first year, n (%) | 1625 (16.7) | 1367 (84.1) | 258 (15.9) | <0.001 | 1400 (86.2) | 225 (13.8) | <0.001 | 1519 (93.5) | 106 (6.5) | <0.001 |
| Passive smoking, n (%) | 4308 (44.2) | 3889 (90.3) | 419 (9.7) | <0.001 | 4056 (94.2) | 252 (5.8) | 0.043 | 4163 (96.6) | 145 (3.4) | 0.015 |
| Decoration, n (%) | 2816 (31.7) | 2596 (92.2) | 220 (7.8) | 0.038 | 2635 (93.6) | 181 (6.4) | 0.003 | 2715 (96.4) | 101 (3.6) | 0.014 |
| Unknown | 870 | 765 | 105 | 827 | 43 | 848 | 22 | |||
| Having a pet since conception, n (%) | <0.001 | <0.001 | <0.001 | |||||||
| Yes | 1172 (12.0) | 1056 (90.1) | 116 (9.9) | 1085 (92.6) | 87 (7.4) | 1117 (95.3) | 55 (4.7) | |||
| No | 8582 (88.0) | 7972 (92.9) | 610 (7.1) | 8149 (95.0) | 433 (5.0) | 8354 (97.3) | 228 (2.7) | |||
| Insecticide use, n (%) | <0.001 | <0.001 | 0.001 | |||||||
| Yes | 3702 (38.0) | 3362 (90.8) | 340 (9.2) | 3467 (93.7) | 235 (6.3) | 3569 (96.4) | 133 (3.6) | |||
| No | 6052 (62.0) | 5666 (93.6) | 386 6.4) | 5767 (95.3) | 285 (4.7) | 5902 (97.5) | 150 (2.5) | |||
| Dampness/mold, n (%) | <0.001 | <0.001 | <0.001 | |||||||
| Yes | 1447 (14.8) | 1259 (87.0) | 188 (13.0) | 1321 (91.3) | 126 (8.7) | 1372 (94.8) | 75 (5.2) | |||
| No | 7428 (76.2) | 6967 (93.8) | 461 (6.2) | 7090 (95.4) | 338 (4.6) | 7249 (97.6) | 179 (2.4) | |||
| Unknown | 879 (9.0) | 802 (91.2) | 77 (8.8) | 823 (93.6) | 56 (6.4) | 850 (96.7) | 29 (3.3) | |||
| Traffic within 50 m, n (%) | 0.013 | <0.001 | <0.001 | |||||||
| Much | 2499 (25.6) | 2281 (91.3) | 218 (8.7) | 2311 (92.5) | 188 (7.5) | 2390 (95.6) | 109 (4.4) | |||
| Not much | 4122 (42.3) | 3824 (92.8) | 298 (7.2) | 3926 (95.2) | 196 (4.8) | 4019 (97.5) | 103 (2.5) | |||
| Less | 3133 (32.1) | 2923 (93.3) | 210 (6.7) | 2997 (95.7) | 136 (4.3) | 3062 (97.7) | 71 (2.3) | |||
| Frequency of park visits, n (%) | 0.003 | 0.002 | 0.002 | |||||||
| ≤once/month | 2272 (25.6) | 2079 (91.5) | 193 (8.5) | 2120 (93.3) | 152 (6.7) | 2180 (96.0) | 92 (4.0) | |||
| 2–3 times/month | 2948 (33.2) | 2736 (92.8) | 212 (7.2) | 2787 (94.5) | 161 (5.5) | 2866 (97.2) | 82 (2.8) | |||
| 1–2 times/week | 2341 (26.4) | 2195 (93.8) | 146 (6.2) | 2230 (95.3) | 111 (4.7) | 2284 (97.6) | 57 (2.4) | |||
| 3–5 times/week | 938 (10.6) | 886 (94.5) | 52 (5.5) | 894 (95.3) | 44 (4.7) | 912 (97.2) | 26 (2.8) | |||
| ≥ once/day | 385 (4.3) | 367 (95.3) | 18 (4.7) | 376 (97.7) | 9 (2.3) | 381 (99.0) | 4 (1.0) | |||
| unknown | 870 | 765 | 105 | 827 | 43 | 848 | 22 | |||
| Ambient temperature, °C, median (IQR) | 26.1 (0.1) | 26.1 (0.1) | 26.1 (0.2) | 0.120 | 26.1 (0.1) | 26.1 (0.1) | >0.9 | 26.1 (0.1) | 26.1 (0.1) | >0.9 |
| Relative humidity, %, median (IQR) | 82.3(0.5) | 82.3 (0.5) | 82.3 (0.5) | 0.200 | 82.3 (0.5) | 82.2 (0.3) | 0.004 | 82.3 (0.5) | 82.3 (0.5) | 0.400 |
| Exposure Frequencies | Ever Asthma | Ever Wheezing | Current Wheezing | |||
|---|---|---|---|---|---|---|
| Crude Model | Adjusted Model | Crude Model | Adjusted Model | Crude Model | Adjusted Model | |
| No exposure (n = 6052, 70.9%) | Reference | Reference | Reference | Reference | Reference | Reference |
| Only once (n = 477, 5.6%) | 1.42 (1.00, 1.95) | 1.15 (0.81, 1.61) | 1.65 (1.13, 2.34) | 1.39 (0.94, 2.00) | 1.54 (0.91, 2.47) | 1.26 (0.73, 2.04) |
| Once/half year (n = 877, 10.3%) | 1.47 (1.14, 1.89) | 1.21 (0.93, 1.56) | 1.41 (1.04, 1.87) | 1.07 (0.78, 1.45) | 1.73 (1.18, 2.47) | 1.35 (0.91, 1.95) |
| Once/quarter (n = 428, 5.0%) | 1.47 (1.03, 2.05) | 1.24 (0.86, 1.76) | 1.53 (1.01, 2.22) | 1.19 (0.78, 1.76) | 1.43 (0.80, 2.37) | 1.11 (0.62, 1.87) |
| Once/month (n = 442, 5.2%) | 1.42 (1.00, 1.98) | 1.18 (0.82, 1.67) | 0.96 (0.58, 1.49) | 0.77 (0.46, 1.22) | 1.38 (0.77, 2.29) | 1.15 (0.63, 1.94) |
| Once/week (n = 260, 3.1%) | 2.51 (1.73, 3.56) | 1.87 (1.26, 2.70) | 1.87 (1.16, 2.88) | 1.43 (0.86, 2.27) | 2.24 (1.22, 3.79) | 1.73 (0.92, 3.00) |
| OR for trend | 1.14 (1.08, 1.20) | 1.09 (1.03, 1.15) | 1.09 (1.02, 1.16) | 1.03 (0.96, 1.10) | 1.15 (1.06, 1.24) | 1.09 (1.00, 1.18) |
| p for trend | <0.001 | 0.001 | 0.007 | 0.380 | <0.001 | 0.034 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, Y.; Yang, G.; Wang, D.; Gu, W.; Xie, D.; Huang, T.; Xue, P.; Tang, J.; Wei, H.; Li, S.; et al. Associations of Insecticide Exposure with Childhood Asthma and Wheezing: A Population-Based Cross-Sectional Study in Sanya, China. Toxics 2024, 12, 392. https://doi.org/10.3390/toxics12060392
Hu Y, Yang G, Wang D, Gu W, Xie D, Huang T, Xue P, Tang J, Wei H, Li S, et al. Associations of Insecticide Exposure with Childhood Asthma and Wheezing: A Population-Based Cross-Sectional Study in Sanya, China. Toxics. 2024; 12(6):392. https://doi.org/10.3390/toxics12060392
Chicago/Turabian StyleHu, Yabin, Guiyan Yang, Dan Wang, Wangyang Gu, Dan Xie, Tingyue Huang, Peng Xue, Jingyi Tang, Hui Wei, Shenghui Li, and et al. 2024. "Associations of Insecticide Exposure with Childhood Asthma and Wheezing: A Population-Based Cross-Sectional Study in Sanya, China" Toxics 12, no. 6: 392. https://doi.org/10.3390/toxics12060392
APA StyleHu, Y., Yang, G., Wang, D., Gu, W., Xie, D., Huang, T., Xue, P., Tang, J., Wei, H., Li, S., Tong, S., & Liu, S. (2024). Associations of Insecticide Exposure with Childhood Asthma and Wheezing: A Population-Based Cross-Sectional Study in Sanya, China. Toxics, 12(6), 392. https://doi.org/10.3390/toxics12060392