
Biochemical and Hematological Markers in Workers with Chronical Exposure to Lead and Cadmium in Colombia

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Blood Pressure, Hematological and Biochemical Estimations
2.4. Chemicals and Reagents
2.5. Instrumental Analysis
2.6. Quality Control and Quality Assurance
2.7. Statistical Analysis
3. Results
3.1. Population Characteristics
3.2. Laboratory and Anthropometric Parameters
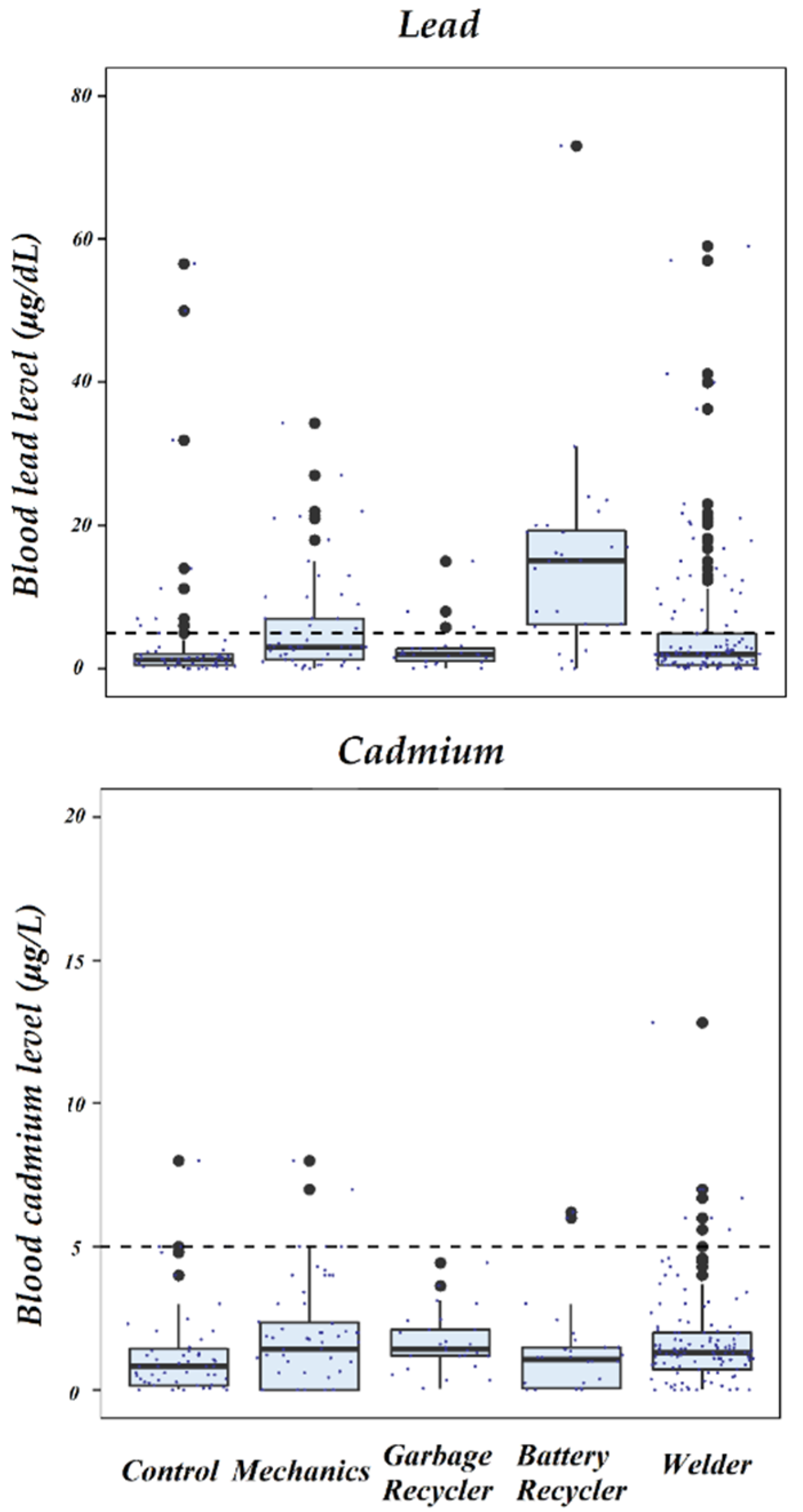
3.3. Occupational Exposure to Pb and Cd
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ledda, C.; Cannizzaro, E.; Lovreglio, P.; Vitale, E.; Stufano, A.; Montana, A.; Li Volti, G.; Rapisarda, V. Exposure to Toxic Heavy Metals Can Influence Homocysteine Metabolism? Antioxidants 2019, 9, 30. [Google Scholar] [CrossRef]
- Wu, C.Y.; Wong, C.S.; Chung, C.J.; Wu, M.Y.; Huang, Y.L.; Ao, P.L.; Lin, Y.F.; Lin, Y.C.; Shiue, H.S.; Su, C.T.; et al. The association between plasma selenium and chronic kidney disease related to lead, cadmium and arsenic exposure in a Taiwanese population. J. Hazard. Mater. 2019, 375, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Bonberg, N.; Pesch, B.; Ulrich, N.; Moebus, S.; Eisele, L.; Marr, A.; Arendt, M.; Jöckel, K.H.; Brüning, T.; Weiss, T. The distribution of blood concentrations of lead (Pb), cadmium (Cd), chromium (Cr) and manganese (Mn) in residents of the German Ruhr area and its potential association with occupational exposure in metal industry and/or other risk factors. Int. J. Hyg. Environ. Health 2017, 220, 998–1005. [Google Scholar] [CrossRef] [PubMed]
- Lanphear, B.P.; Rauch, S.; Auinger, P.; Allen, R.W.; Hornung, R.W. Low-level lead exposure and mortality in US adults: A population-based cohort study. Lancet Public Health 2018, 3, e177–e184. [Google Scholar] [CrossRef]
- Shiek, S.S.; Mani, M.S.; Kabekkodu, S.P.; Dsouza, H.S. Health repercussions of environmental exposure to lead: Methylation perspective. Toxicology 2021, 461, 152927. [Google Scholar] [CrossRef] [PubMed]
- Koszewicz, M.; Markowska, K.; Waliszewska-Prosol, M.; Poreba, R.; Gac, P.; Szymanska-Chabowska, A.; Mazur, G.; Wieczorek, M.; Ejma, M.; Slotwinski, K.; et al. The impact of chronic co-exposure to different heavy metals on small fibers of peripheral nerves. A study of metal industry workers. J. Occup. Med. Toxicol. 2021, 16, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Fernández, C.; Villar, L. A taxinomy of Colombia’s inflormal labor market. Coyunt. Económica Investig. Económica Soc. 2016, 39, 15–50. Available online: https://www.repository.fedesarrollo.org.co/handle/11445/3304 (accessed on 27 July 2022).
- Gasparini, L.; Tornarolli, L. Labor Informality in Latin America and the Caribbean: Patterns and Trends from Household Survey Microdata. Desarrollo y Sociedad. 2009, 63, 13–80. Available online: http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S0120-35842009000100002&lng=en&tlng=en (accessed on 2 July 2022). [CrossRef]
- World Bank Group-International Development, Poverty, & Sustainability. Available online: https://www.worldbank.org/en/home (accessed on 2 July 2022).
- Wani, A.L.; Usmani, J.A. Occupational stress among workers having exposure to lead. Clin. Epidemiol. Glob. Health 2016, 4, 163–170. [Google Scholar] [CrossRef]
- Bumoko, G.M.M.; Sadiki, N.H.; Rwatambuga, A.; Kayembe, K.P.; Okitundu, D.L.; Mumba Ngoyi, D.; Muyembe, J.J.T.; Banea, J.P.; Boivin, M.J.; Tshala-Katumbay, D. Lower serum levels of selenium, copper, and zinc are related to neuromotor impairments in children with konzo. J. Neurol. Sci. 2015, 349, 149–153. [Google Scholar] [CrossRef]
- Ni, W.; Huang, Y.; Wang, X.; Zhang, J.; Wu, K. Associations of neonatal lead, cadmium, chromium and nickel co-exposure with DNA oxidative damage in an electronic waste recycling town. Sci. Total Environ. 2014, 472, 354–362. [Google Scholar] [CrossRef]
- Agency for Toxics Substances and Disease Registry. Lead (Pb) Toxicity: What Are U.S. Standards for Lead Levels? |Environmental Medicine|ATSDR. Available online: https://www.atsdr.cdc.gov/csem/leadtoxicity/safety_standards.html (accessed on 15 February 2022).
- Sanders, T.; Liu, Y.; Buchner, V.; Tchounwou, P.B. Neurotoxic effects and biomarkers of lead exposure: A review. Rev. Environ. Health 2009, 24, 15–45. [Google Scholar] [CrossRef]
- Flora, G.; Gupta, D.; Tiwari, A.; Tech, M. Toxicity of lead: A review with recent updates. Interdiscip. Toxicol. 2012, 5, 47–58. [Google Scholar] [CrossRef]
- Mansouri, M.T.; Muñoz-Fambuena, I.; Cauli, O. Cognitive impairment associated with chronic lead exposure in adults. Neurol. Psychiatry Brain Res. 2018, 30, 5–8. [Google Scholar] [CrossRef]
- Weuve, J.; Korrick, S.A.; Weisskopf, M.A.; Ryan, L.M.; Schwartz, J.; Nie, H.; Grodstein, F.; Hu, H.; Hu, H. Cumulative Exposure to Lead in Relation to Cognitive Function in Older Women. Environ. Health Perspect. 2009, 117, 574–580. [Google Scholar] [CrossRef]
- Boskabady, M.; Marefati, N.; Farkhondeh, T.; Shakeri, F.; Farshbaf, A.; Boskabady, M.H. The effect of environmental lead exposure on human health and the contribution of inflammatory mechanisms, a review. Environ. Int. 2018, 120, 404–420. [Google Scholar] [CrossRef]
- Tanr, E.; Karaer, A.; Celik, O.; Celik, E.; Otlu, B.; Yilmaz, E.; Ozgul, O. Role of endometrial concentrations of heavy metals (cadmium, lead, mercury and arsenic) in the aetiology of unexplained infertility. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 179, 187–190. [Google Scholar] [CrossRef]
- Kumar, S. Occupational and environmental exposure to lead and reproductive health impairment: An overview. Indian J. Occup. Environ. Med. 2018, 22, 128–137. [Google Scholar] [CrossRef]
- Dicker, D.; Nguyen, G.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; et al. Global, regional, and national age-sex-specific mortality and life expectancy, 1950–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1684–1735. [Google Scholar] [CrossRef]
- Odongo, O.A.; Moturi, W.N.; Obonyo, M.A. Influence of task-based airborne lead exposures on blood lead levels: A case study of informal automobile repair artisans in Nakuru town, Kenya. Environ. Geochem. Health 2019, 42, 1893–1903. [Google Scholar] [CrossRef]
- Matović, V.; Buha, A.; Ðukić-Ćosić, D.; Bulat, Z. Insight into the oxidative stress induced by lead and/or cadmium in blood, liver and kidneys. Food Chem. Toxicol. 2015, 78, 130–140. [Google Scholar] [CrossRef] [PubMed]
- Genchi, G.; Sinicropi, M.S.; Lauria, G.; Carocci, A.; Catalano, A. The Effects of Cadmium Toxicity. Int. J. Environ. Res. Public Health 2020, 17, 3782. [Google Scholar] [CrossRef] [PubMed]
- Rahimzadeh, M.R.; Rahimzadeh, M.R.; Kazemi, S.; Moghadamnia, A.A. Cadmium toxicity and treatment: An update. Casp. J. Intern. Med. 2017, 8, 135–145. [Google Scholar]
- Javorac, D.; Antonijević, B.; Anđelković, M.; Repić, A.; Bulat, P.; Djordjevic, A.B.; Baralić, K.; Đukić-Ćosić, D.; Antonić, T.; Bulat, Z. Oxidative stress, metallomics and blood toxicity after subacute low-level lead exposure in Wistar rats: Benchmark dose analyses. Environ. Pollut. 2021, 291, 118103. [Google Scholar] [CrossRef]
- Chen, C.; Li, Q.; Nie, X.; Han, B.; Chen, Y.; Xia, F.; Zhai, H.; Wang, N.; Lu, Y. Association of lead exposure with cardiovascular risk factors and diseases in Chinese adults. Environ. Sci. Pollut. Res. 2017, 24, 22275–22283. [Google Scholar] [CrossRef]
- Ahmad, I.; Khan, B.; Khan, S.; Khan, M.T.; Schwab, A.P. Assessment of lead exposure among automobile technicians in Khyber Pakhtunkhwa, Pakistan. Sci. Total Environ. 2018, 633, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Parsons, P.J. Frances, M.V. Trace Elements in Whole Blood Event #3; New York State Department of Health: Albany, NY, USA, 30 November 2012; pp. 2–4.
- Sengupta, P. Pallav Sengupta Environmental and occupational exposure of metals and their role in male reproductive functions. Drug Chem. Toxicol. 2013, 36, 353–368. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Chraiti, M.N.; Pittet, D.; Mclaws, M.L. Blood collection guidelines for inpatients and outpatients, home-based care and long-term care facilities. J. Hosp. Infect. 2020, 104, 600–602. [Google Scholar] [CrossRef]
- SCYMED National Cholesterol Education Program. NCEP ATP-III Cholesterol Guidelines--Cholesterol 2.0. Available online: http://www.scymed.com/en/smnxdj/edzr/edzr9610.htm (accessed on 26 April 2022).
- WHO. WHO Guidelines on Drawing Blood: Best Practices in Phlebotomy; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef]
- Palmer, C.D.; Lewis, M.E.; Geraghty, C.M.; Barbosa, F.; Parsons, P.J. Determination of lead, cadmium and mercury in blood for assessment of environmental exposure: A comparison between inductively coupled plasma–mass spectrometry and atomic absorption spectrometry. Spectrochim. Acta Part B At. Spectrosc. 2006, 61, 980–990. [Google Scholar] [CrossRef]
- Ren, T.; Zhao, L.J.; Sun, B.S.; Zhong, R.G. Determination of lead, cadmium, copper, and nickel in the tonghui river of Beijing, China, by cloud point extraction-high resolution continuum source graphite furnace atomic absorption spectrometry. J. Environ. Qual. 2013, 42, 1752–1762. [Google Scholar] [CrossRef]
- Lormphongs, S.; Miyashita, K.; Morioka, I.; Chaikittiporn, C.; Miyai, N.; Yamamoto, H. Lead Exposure and Blood Lead Level of Workers in a Battery Manufacturing Plant in Thailand. Ind. Health 2003, 41, 348–353. [Google Scholar] [CrossRef] [Green Version]
- Nouioui, M.A.; Araoud, M.; Milliand, M.L.; Bessueille-Barbier, F.; Amira, D.; Ayouni-Derouiche, L.; Hedhili, A. Biomonitoring chronic lead exposure among battery manufacturing workers in Tunisia. Environ. Sci. Pollut. Res. 2019, 26, 7980–7993. [Google Scholar] [CrossRef]
- Ahmad, S.A.; Khan, M.H.; Khandker, S.; Sarwar, A.F.M.; Yasmin, N.; Faruquee, M.H.; Yasmin, R.; Babu, B.V.; Stein, Z.A. Blood Lead Levels and Health Problems of Lead Acid Battery Workers in Bangladesh. Sci. World J. 2014, 1–7. [Google Scholar] [CrossRef]
- Irawati, Y.; Kusnoputranto, H.; Achmadi, U.F.; Safrudin, A.; Sitorus, A.; Risandi, R.; Wangsamuda, S.; Asih, P.B.S.; Syafruddin, D. Blood lead levels and lead toxicity in children aged 1–5 years of Cinangka Village, Bogor Regency. PLoS ONE 2022, 17, e0264209. [Google Scholar] [CrossRef]
- Chwalba, A.; Maksym, B.; Dobrakowski, M.; Kasperczyk, S.; Pawlas, N.; Birkner, E.; Kasperczyk, A. The effect of occupational chronic lead exposure on the complete blood count and the levels of selected hematopoietic cytokines. Toxicol. Appl. Pharmacol. 2018, 355, 174–179. [Google Scholar] [CrossRef]
- Chen, X.; Zhu, G.; Wang, Z.; Zhou, H.; He, P.; Liu, Y.; Jin, T. The association between lead and cadmium co-exposure and renal dysfunction. Ecotoxicol. Environ. Saf. 2019, 173, 429–435. [Google Scholar] [CrossRef]
- Dobrakowski, M.; Boroń, M.; Czuba, Z.P.; Birkner, E.; Chwalba, A.; Hudziec, E.; Kasperczyk, S. Blood morphology and the levels of selected cytokines related to hematopoiesis in occupational short-term exposure to lead. Toxicol. Appl. Pharmacol. 2016, 305, 111–117. [Google Scholar] [CrossRef]
- Barman, T.; Kalahasthi, R.; Rajmohan, H.R. Effects of lead exposure on the status of platelet indices in workers involved in a lead-acid battery manufacturing plant. J. Expo. Sci. Environ. Epidemiol. 2014, 24, 629–633. [Google Scholar] [CrossRef]
- Zeng, Z.; Huo, X.; Zhang, Y.; Xiao, Z.; Zhang, Y.; Xu, X. Lead exposure is associated with risk of impaired coagulation in preschool children from an e-waste recycling area. Environ. Sci. Pollut. Res. 2018, 25, 20670–20679. [Google Scholar] [CrossRef]
- Richter, P.; Faroon, O.; Pappas, R.S. Cadmium and cadmium/zinc ratios and tobacco-related morbidities. Int. J. Environ. Res. Public Health 2017, 14, 1154. [Google Scholar] [CrossRef] [PubMed]
- Djedjibegovic, J.; Marjanovic, A.; Tahirovic, D.; Caklovica, K.; Turalic, A.; Lugusic, A.; Omeragic, E.; Sober, M.; Caklovica, F. Heavy metals in commercial fish and seafood products and risk assessment in adult population in Bosnia and Herzegovina. Sci. Rep. 2020, 10, 1–8. [Google Scholar] [CrossRef]
- Çatav, Ş.S.; Genç, T.O.; Oktay, M.K.; Küçükakyüz, K. Cadmium Toxicity in Wheat: Impacts on Element Contents, Antioxidant Enzyme Activities, Oxidative Stress, and Genotoxicity. Bull Environ Contam Toxicol. 2020, 104, 71–77. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Parameter | Control (n = 59) | Mechanic (n = 59) | Garbage Recycler (n = 26) | Battery Recycler (n = 28) | Welder (n = 121) | p-Value |
|---|---|---|---|---|---|---|
| Age, years, median(range) | 43.0 (20.0–77.0) | 40.0 (20.0–68.0) | 48.0 (21.0–63.0) | 39.5 (18.0–63.0) | 47.0 (20.0–68.0) | 0.006 * |
| Experience, years, median(range) | 11.0 (1.00–63.0) | 12.0 (0.58–59.0) | 20.0 (3.00–50.0) | 7.50 (1.00–32.0) | 16.0 (2.00–49.0) | <0.001 * |
| Economic status, % | <0.001 * | |||||
| Very poor | 64.4 | 64.4 | 100 | 64.3 | 59.5 | |
| Poor | 18.6 | 30.5 | 0 | 28.6 | 33.1 | |
| Middle-class | 15.3 | 5.1 | 0 | 7.1 | 6.6 | |
| Upper middle-class | 1.7 | 0 (0) | 0 | 0 | 1 (0.8) | |
| Education, % | <0.001 * | |||||
| Elementary | 6.8 | 52.5 | 88.5 | 71.4 | 9.92 | |
| High School | 22 | 33.9 | 11.5 | 17.9 | 45.5 | |
| Technical | 69.5 | 13.6 | 0 | 10.7 | 44.6 | |
| Smoking, % | 10.1 | 5.1 | 19.2 | 25 | 13.2 | 0.112 |
| Pb, µg/d, median(range) | 1.31 (≤MQL–56.6) | 3.00 (≤MQL–34.3) | 1.96 (≤MQL–15.0) | 15.1 (≤MQL–73.0) | 2.00 (≤MQL–59.0) | <0.001 * |
| High Pb, % | <0.001 * | |||||
| No | 84.7 | 62.7 | 88.5 | 17.9 | 75.2 | |
| Yes (>5 µg/dL) | 15.3 | 37.3 | 11.5 | 82.1 | 24.8 | |
| Cd, µg/L, median (range) | 0.82 (≤MQL–8.00) | 1.43 (≤MQL–8.00) | 1.44 (≤MQL–4.44) | 1.06 (≤MQL–6.20) | 1.32 (≤MQL–12.80) | <0.001 * |
| High Cd, % | 0.287 | |||||
| No | 89.8 | 91.5 | 100 | 92.9 | 93.4 | |
| Yes (>5 µg/L) | 10.2 | 8.5 | 0 | 7.1 | 6.6 |
| Normal Values | Control | Mechanic | Garbage Recycler | Battery Recycler | Welder | ||
|---|---|---|---|---|---|---|---|
| Parameter | Median (Range) | p-Value | |||||
| n = 59 | n = 59 | n = 26 | n = 28 | n = 121 | |||
| HDL, mg/dL | 40.0–60.0 | 74.0 (58.0–86.3) | 75.3 (50.0–105.0) | N/A | 74.8 (47.0–98.6) | 75.9 (52.0–91.0) | 0.631 |
| Cholesterol, mg/dL | <200 | 196 (126–284) | 194 (94.0–298) | 156 (93.2–251) | 186 (100–248) | 181 (112–299) | <0.001 ** |
| Triglycerides, mg/dL | <150 | 134 (60.4–224) | 144 (51.0–348) | 112 (44.4–245) | 141 (75.1–249) | 141 (59.0–255) | 0.030 * |
| Glucose, mg/dL | 100.0 | 79.0 (60.6–122) | 84.6 (69.5–139) | 87.3 (56.6–165) | 81.5 (68.0–132) | 89.0 (61.0–166) | <0.001 ** |
| BMI | 20.0 | 26.1 (16.7–35.0) | 25.8 (17.9–36.9) | 25.2 (22.6–29.3) | 26.4 (17.0–39.5) | 26.9 (19.0–36.4) | 0.087 |
| SBP, (mm Hg) | <120 | 130 (90–190) | 122 (90–170) | 120 (100–160) | 127 (110–190) | 118 (95–177) | <0.001 ** |
| DBP, (mm Hg) | <130 | 83 (60–110) | 78 (60–102) | 81 (60–100) | 80 (65–143) | 78.0 (55–105) | 0.010 ** |
| Abd Circ, cm | <95.0 | 103 (75.0–135) | 97.0 (73.0–136) | 110 (92.0–130) | 103 (90.0–133) | 99.0 (77.0–136) | <0.001 ** |
| Hip-waist index | 0.96–0.99 | 0.92 (0.80–1.16) | 0.92 (0.80–1.14) | 0.91 (0.88–1.03) | 0.90 (0.86–1.10) | 0.92 (0.82–1.04) | 0.427 |
| Platelets/109, cells/L | 150–450 | 214 (169–382) | 191 (152–326) | 201 (170–326) | 236 (159–391) | 197 (153–321) | 0.009 ** |
| Hemoglobin, mg/dl | 13.8–17.2 | 14.6 (11.6–17.3) | 15.0 (13.0–16.3) | 14.6 (11.6–16.3) | 14.4 (12.0–16.3) | 15.0 (10.6–17.3) | 0.038 * |
| Hematocrit,(vol% of RBC) | 40.0–54.0 | 44.0 (35.0–52.0) | 45.0 (32.0–49.0) | 44.0 (35.0–49.0) | 44.0 (38.0–50.0) | 45.0 (32.0–52.0) | 0.047 * |
| Basophils, % | 0–3 | 24.1 | 39.0 | 17.9 | 46.4 | 24.0 | 0.023 * |
| MetS, % | N/A | 14.6 | 29.6 | 31.6 | 38.9 | 22.1 | 0.171 |
| Key Parameters | Non-Missing Data | All Patients | Normal Pb Levels | Elevated Pb Levels | Effect of Abnormal Lead | p-Value |
|---|---|---|---|---|---|---|
| n | Percentege (%) | OR (95% CI) | ||||
| Basophile | 294 | 28.6 | 11.6 | 69.0 | 12.3 (6.62 to 23.7) | <0.001 |
| Smoking | 276 | 13.4 | 14.6 | 10.7 | 0.81 (0.34 to 1.78) | 0.499 |
| Median (range) | β (95% CI) | |||||
| BMI | 291 | 26.4 (15.4–39.5) | 26.3 (15.4–36.9) | 26.8 (17.5–39.5) | 0.19 (−0.91 to 1.30) | 0.314 |
| HDL, mg/dL | 219 | 75.7 (47.0–105.0) | 75.7 (50.0–105.0) | 76.0 (47.0–98.6) | 1.61 (−8.42 to 11.64) | 0.857 * |
| Cholesterol, mg/dL | 294 | 185 (93–299) | 187 (93–284) | 178 (100–299) | 3.86 (−0.80 to 8.52) | 0.294 |
| SBP, mm Hg | 272 | 122 (90–190) | 120 (90–190) | 125 (95–190) | 1.93 (−1.06 to 4.92) | 0.160 |
| DBP, mm Hg | 272 | 80 (55–143) | 80 (60–110) | 80 (55–143) | −6.61 (−23.16 to 9.94) | 0.710 * |
| Platelets/109, cells/L | 181 | 201 (152–391) | 210 (155–382) | 193 (152–391) | −2.55 (−6.74 to 1.63) | 0.012 |
| Glucose, mg/dL | 306 | 86 (57–166) | 86 (61–166) | 86 (57–140) | −0.41 (−1.45 to 0.62) | 0.367 |
| Hematocrit, (vol% of RBC) | 188 | 44.0 (32.0–52.0) | 44.0 (32.0–52.0) | 44.0 (32.0–50.0) | 0.19 (−0.91 to 1.30) | 0.884 |
| Job Types | Cd | Pb | ||
|---|---|---|---|---|
| Crude OR (95% CI) | Adjusted OR (95% CI) | Crude OR (95% CI) | Adjusted OR (95% CI) | |
| Control workers | Reference | Reference | Reference | Reference |
| Mechanic | 0.82 (0.22 to 2.87) | 0.71 (0.12 to 4.83) | 3.30 (1.40 to 8.34) | 3.20 (1.13 to 9.74) |
| Garbage recycler | N.E. | N.E. | 0.45 (0.10 to 1.63) | 0.55 (0.10 to 2.57) |
| Battery recycler | 0.68 (0.10 to 3.19) | 0.75 (0.07 to 7.03) | 25.56 (8.29 to 93.85) | 29.55 (7.17 to 145.64) |
| Welder | 0.63 (0.21 to 1.98) | 0.61 (0.13 to 3.43) | 1.83 (0.83 to 4.37) | 1.42 (0.59 to 3.73) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vergara-Murillo, F.; Martinez-Yanez, K.; Fortich-Revollo, A.; Paternina-Caicedo, A.; Johnson-Restrepo, B. Biochemical and Hematological Markers in Workers with Chronical Exposure to Lead and Cadmium in Colombia. Toxics 2022, 10, 524. https://doi.org/10.3390/toxics10090524
Vergara-Murillo F, Martinez-Yanez K, Fortich-Revollo A, Paternina-Caicedo A, Johnson-Restrepo B. Biochemical and Hematological Markers in Workers with Chronical Exposure to Lead and Cadmium in Colombia. Toxics. 2022; 10(9):524. https://doi.org/10.3390/toxics10090524
Chicago/Turabian StyleVergara-Murillo, Fredy, Katiana Martinez-Yanez, Alvaro Fortich-Revollo, Angel Paternina-Caicedo, and Boris Johnson-Restrepo. 2022. "Biochemical and Hematological Markers in Workers with Chronical Exposure to Lead and Cadmium in Colombia" Toxics 10, no. 9: 524. https://doi.org/10.3390/toxics10090524
APA StyleVergara-Murillo, F., Martinez-Yanez, K., Fortich-Revollo, A., Paternina-Caicedo, A., & Johnson-Restrepo, B. (2022). Biochemical and Hematological Markers in Workers with Chronical Exposure to Lead and Cadmium in Colombia. Toxics, 10(9), 524. https://doi.org/10.3390/toxics10090524