


Prenatal Metal Exposures and Associations with Kidney Injury Biomarkers in Children
 , , ,
, , ,  ,
,  , , , ,
, , , ,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
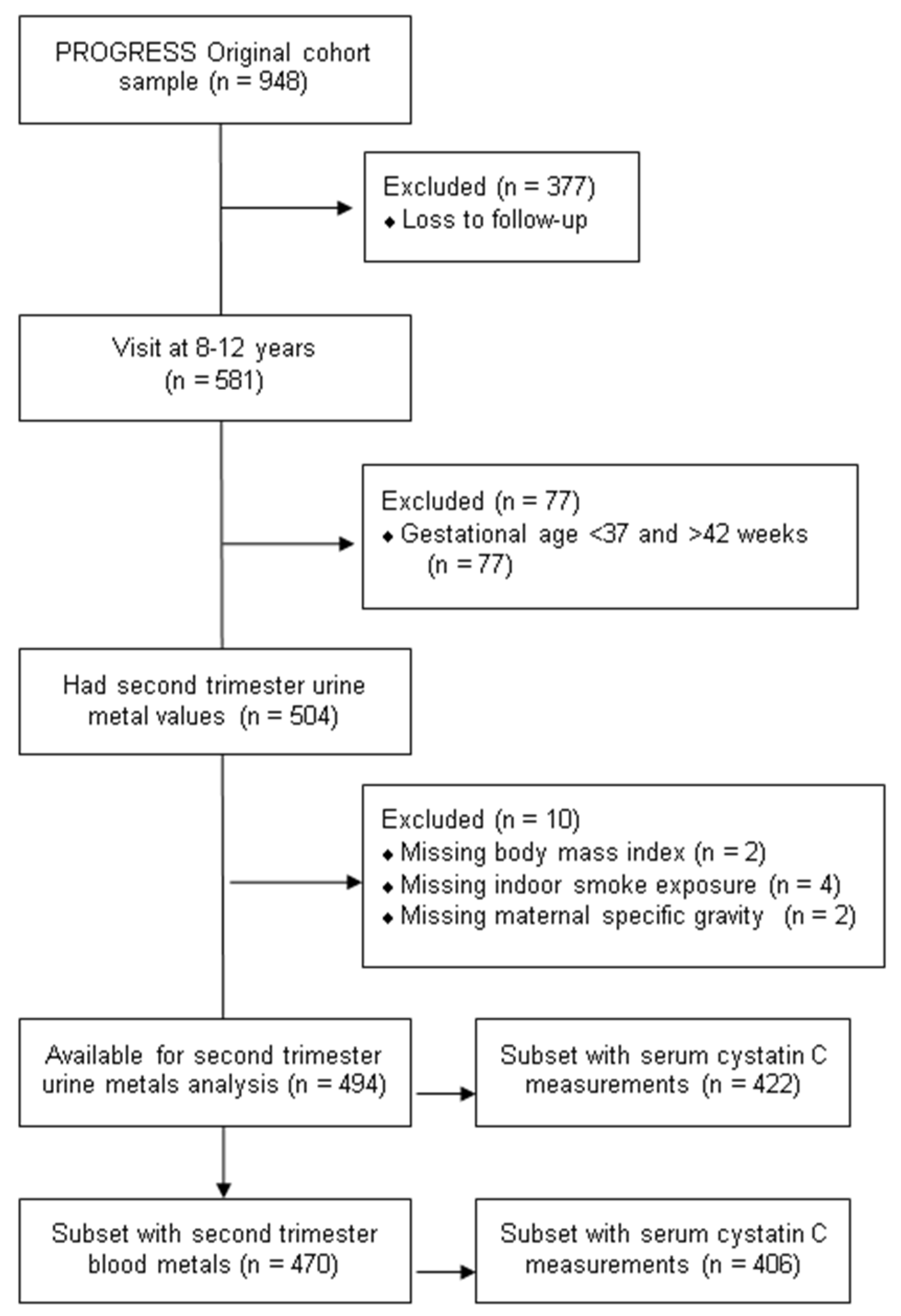
2.1. Study Population
2.2. Second Trimester Metals Assessment
2.3. Child Urinary Protein Biomarkers and Urine Creatinine
2.4. Serum Cystatin C and eGFR
2.5. Covariates
2.6. Statistical Analyses
3. Results
3.1. Characteristics of the Study Population
3.2. Pairwise Associations of Individual Metals with Individual Kidney Injury Biomarkers
3.3. Associations of Individual Metals with Multi-Protein Mixture
3.4. Associations of Individual Kidney Injury Biomarkers with Metal Mixture Index
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Selevan, S.G.; Kimmel, C.A.; Mendola, P. Identifying critical windows of exposure for children’s health. Environ. Health Perspect. 2000, 108 (Suppl. S3), 451–455. [Google Scholar] [CrossRef] [PubMed]
- Gundacker, C.; Hengstschläger, M. The role of the placenta in fetal exposure to heavy metals. Wien. Med. Wochenschr. 2012, 162, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Caserta, D.; Graziano, A.; Lo Monte, G.; Bordi, G.; Moscarini, M. Heavy metals and placental fetal-maternal barrier: A mini-review on the major concerns. Eur. Rev. Med. Pharmacol. Sci. 2013, 17, 2198–2206. [Google Scholar] [PubMed]
- Fei, D.L.; Koestler, D.C.; Li, Z.; Giambelli, C.; Sanchez-Mejias, A.; Gosse, J.A.; Marsit, C.J.; Karagas, M.R.; Robbins, D.J. Association between In Utero arsenic exposure, placental gene expression, and infant birth weight: A US birth cohort study. Environ. Health 2013, 12, 58. [Google Scholar] [CrossRef]
- Tchounwou, P.B.; Yedjou, C.G.; Patlolla, A.K.; Sutton, D.J. Heavy metal toxicity and the environment. Exp. Suppl. 2012, 101, 133–164. [Google Scholar] [CrossRef]
- Bradl, H. Heavy Metals in the Environment: Origin, Interaction and Remediation; Elsevier: Amsterdam, The Netherlands, 2005. [Google Scholar]
- Pantic, I.; Tamayo-Ortiz, M.; Rosa-Parra, A.; Bautista-Arredondo, L.; Wright, R.O.; Peterson, K.E.; Schnaas, L.; Rothenberg, S.J.; Hu, H.; Téllez-Rojo, M.M. Children’s Blood Lead Concentrations from 1988 to 2015 in Mexico City: The Contribution of Lead in Air and Traditional Lead-Glazed Ceramics. Int. J. Environ. Res. Public Health 2018, 15, 2153. [Google Scholar] [CrossRef]
- Hernandez Avila, M.; Romieu, I.; Rios, C.; Rivero, A.; Palazuelos, E. Lead-glazed ceramics as major determinants of blood lead levels in Mexican women. Environ. Health Perspect. 1991, 94, 117–120. [Google Scholar] [CrossRef]
- Zheng, T.; Zhang, J.; Sommer, K.; Bassig, B.A.; Zhang, X.; Braun, J.; Xu, S.; Boyle, P.; Zhang, B.; Shi, K.; et al. Effects of Environmental Exposures on Fetal and Childhood Growth Trajectories. Ann. Glob. Health 2016, 82, 41–99. [Google Scholar] [CrossRef]
- Farzan, S.F.; Howe, C.G.; Chen, Y.; Gilbert-Diamond, D.; Cottingham, K.L.; Jackson, B.P.; Weinstein, A.R.; Karagas, M.R. Prenatal lead exposure and elevated blood pressure in children. Environ. Int. 2018, 121, 1289–1296. [Google Scholar] [CrossRef]
- McRae, N.; Gennings, C.; Rivera Rivera, N.; Tamayo-Ortiz, M.; Pantic, I.; Amarasiriwardena, C.; Schnaas, L.; Wright, R.; Tellez-Rojo, M.M.; Wright, R.O.; et al. Association between prenatal metal exposure and adverse respiratory symptoms in childhood. Environ. Res. 2022, 205, 112448. [Google Scholar] [CrossRef]
- Babich, R.; Ulrich, J.C.; Ekanayake, E.; Massarsky, A.; De Silva, P.; Manage, P.M.; Jackson, B.P.; Ferguson, P.L.; Di Giulio, R.T.; Drummond, I.A.; et al. Kidney developmental effects of metal-herbicide mixtures: Implications for chronic kidney disease of unknown etiology. Environ. Int. 2020, 144, 106019. [Google Scholar] [CrossRef] [PubMed]
- Bolignano, D.; Lacquaniti, A.; Coppolino, G.; Donato, V.; Campo, S.; Fazio, M.R.; Nicocia, G.; Buemi, M. Neutrophil gelatinase-associated lipocalin (NGAL) and progression of chronic kidney disease. Clin. J. Am. Soc. Nephrol. 2009, 4, 337–344. [Google Scholar] [CrossRef]
- Lopez-Giacoman, S.; Madero, M. Biomarkers in chronic kidney disease, from kidney function to kidney damage. World J. Nephrol. 2015, 4, 57–73. [Google Scholar] [CrossRef] [PubMed]
- Lentini, P.; Zanoli, L.; Granata, A.; Signorelli, S.S.; Castellino, P.; Dell’Aquila, R. Kidney and heavy metals—The role of environmental exposure (Review). Mol. Med. Rep. 2017, 15, 3413–3419. [Google Scholar] [CrossRef] [PubMed]
- Coca, S.G.; Singanamala, S.; Parikh, C.R. Chronic kidney disease after acute kidney injury: A systematic review and meta-analysis. Kidney Int. 2012, 81, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Masaebi, F.; Azizmohammad Looha, M.; Wang, Z.; Zarean, E.; Nasiri, M.; Kazerouni, F.; Gharishvandi, F.; Zayeri, F. Evaluation of Neutrophil Gelatinase-Associated Lipocalin and Cystatin C in Early Diagnosis of Chronic Kidney Disease in the Absence of the Gold Standard. Galen Med. J. 2020, 9, e1698. [Google Scholar] [CrossRef]
- Øvrehus, M.A.; Zürbig, P.; Vikse, B.E.; Hallan, S.I. Urinary proteomics in chronic kidney disease: Diagnosis and risk of progression beyond albuminuria. Clin. Proteom. 2015, 12, 21. [Google Scholar] [CrossRef][Green Version]
- Fernando, B.; Alli-Shaik, A.; Hemage, R.K.D.; Badurdeen, Z.; Hettiarachchi, T.W.; Abeysundara, H.T.K.; Abeysekara, T.D.J.; Wazil, A.; Rathnayake, S.; Gunaratne, J.; et al. Pilot Study of Renal Urinary Biomarkers for Diagnosis of CKD of Uncertain Etiology. Kidney Int. Rep. 2019, 4, 1401–1411. [Google Scholar] [CrossRef]
- Weidemann, D.K.; Weaver, V.M.; Fadrowski, J.J. Toxic environmental exposures and kidney health in children. Pediatr. Nephrol. 2016, 31, 2043–2054. [Google Scholar] [CrossRef]
- Cárdenas-González, M.; Osorio-Yáñez, C.; Gaspar-Ramírez, O.; Pavković, M.; Ochoa-Martínez, A.; López-Ventura, D.; Medeiros, M.; Barbier, O.C.; Pérez-Maldonado, I.N.; Sabbisetti, V.S.; et al. Environmental exposure to arsenic and chromium in children is associated with kidney injury molecule-1. Environ. Res. 2016, 150, 653–662. [Google Scholar] [CrossRef]
- Zheng, L.Y.; Sanders, A.P.; Saland, J.M.; Wright, R.O.; Arora, M. Environmental exposures and pediatric kidney function and disease: A systematic review. Environ. Res. 2017, 158, 625–648. [Google Scholar] [CrossRef]
- Chadha, V.; Warady, B.A. Epidemiology of pediatric chronic kidney disease. Adv. Chronic Kidney Dis. 2005, 12, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Warady, B.A.; Chadha, V. Chronic kidney disease in children: The global perspective. Pediatr. Nephrol. 2007, 22, 1999–2009. [Google Scholar] [CrossRef] [PubMed]
- Soderland, P.; Lovekar, S.; Weiner, D.E.; Brooks, D.R.; Kaufman, J.S. Chronic kidney disease associated with environmental toxins and exposures. Adv. Chronic Kidney Dis. 2010, 17, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Kataria, A.; Trasande, L.; Trachtman, H. The effects of environmental chemicals on renal function. Nat. Rev. Nephrol. 2015, 11, 610–625. [Google Scholar] [CrossRef] [PubMed]
- Levin-Schwartz, Y.; Politis, M.D.; Gennings, C.; Tamayo-Ortiz, M.; Flores, D.; Amarasiriwardena, C.; Pantic, I.; Tolentino, M.C.; Estrada-Gutierrez, G.; Lamadrid-Figueroa, H.; et al. Nephrotoxic Metal Mixtures and Preadolescent Kidney Function. Children 2021, 8, 673. [Google Scholar] [CrossRef] [PubMed]
- Elmonem, M.A.; Berlingerio, S.P.; Van den Heuvel, L.P.; De Witte, P.A.; Lowe, M.; Levtchenko, E.N. Genetic Renal Diseases: The Emerging Role of Zebrafish Models. Cells 2018, 7, 130. [Google Scholar] [CrossRef] [PubMed]
- Gurusinghe, S.; Tambay, A.; Sethna, C.B. Developmental Origins and Nephron Endowment in Hypertension. Front. Pediatr. 2017, 5. [Google Scholar] [CrossRef]
- Ryan, D.; Sutherland, M.R.; Flores, T.J.; Kent, A.L.; Dahlstrom, J.E.; Puelles, V.G.; Bertram, J.F.; McMahon, A.P.; Little, M.H.; Moore, L.; et al. Development of the Human Fetal Kidney from Mid to Late Gestation in Male and Female Infants. eBioMedicine 2018, 27, 275–283. [Google Scholar] [CrossRef]
- Luyckx, V.A.; Brenner, B.M. Clinical consequences of developmental programming of low nephron number. Anat. Rec. 2020, 303, 2613–2631. [Google Scholar] [CrossRef]
- Sanders, A.P.; Gennings, C.; Tamayo-Ortiz, M.; Mistry, S.; Pantic, I.; Martinez, M.; Estrada-Gutierrez, G.; Espejel-Nuñez, A.; Olascoaga, L.T.; Wright, R.O.; et al. Prenatal and early childhood critical windows for the association of nephrotoxic metal and metalloid mixtures with kidney function. Environ. Int. 2022, 166, 107361. [Google Scholar] [CrossRef]
- Rosa, M.J.; Hair, G.M.; Just, A.C.; Kloog, I.; Svensson, K.; Pizano-Zárate, M.L.; Pantic, I.; Schnaas, L.; Tamayo-Ortiz, M.; Baccarelli, A.A.; et al. Identifying critical windows of prenatal particulate matter (PM2.5) exposure and early childhood blood pressure. Environ. Res. 2020, 182, 109073. [Google Scholar] [CrossRef] [PubMed]
- Sanders, A.P.; Svensson, K.; Gennings, C.; Burris, H.H.; Oken, E.; Amarasiriwardena, C.; Basnet, P.; Pizano-Zarate, M.L.; Schnaas, L.; Tamayo-Ortiz, M.; et al. Prenatal lead exposure modifies the effect of shorter gestation on increased blood pressure in children. Environ. Int. 2018, 120, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Renzetti, S.; Just, A.C.; Burris, H.H.; Oken, E.; Amarasiriwardena, C.; Svensson, K.; Mercado-García, A.; Cantoral, A.; Schnaas, L.; Baccarelli, A.A.; et al. The association of lead exposure during pregnancy and childhood anthropometry in the Mexican PROGRESS cohort. Environ. Res. 2017, 152, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Saylor, C.; Tamayo-Ortiz, M.; Pantic, I.; Amarasiriwardena, C.; McRae, N.; Estrada-Gutierrez, G.; Parra-Hernandez, S.; Tolentino, M.C.; Baccarelli, A.A.; Fadrowski, J.J.; et al. Prenatal blood lead levels and reduced preadolescent glomerular filtration rate: Modification by body mass index. Environ. Int. 2021, 154, 106414. [Google Scholar] [CrossRef] [PubMed]
- Kupsco, A.; Kioumourtzoglou, M.-A.; Just, A.C.; Amarasiriwardena, C.; Estrada-Gutierrez, G.; Cantoral, A.; Sanders, A.P.; Braun, J.M.; Svensson, K.; Brennan, K.J.M.; et al. Prenatal Metal Concentrations and Childhood Cardiometabolic Risk Using Bayesian Kernel Machine Regression to Assess Mixture and Interaction Effects. Epidemiology 2019, 30, 263–273. [Google Scholar] [CrossRef]
- Gunasekara, T.; De Silva, P.; Herath, C.; Siribaddana, S.; Siribaddana, N.; Jayasumana, C.; Jayasinghe, S.; Cardenas-Gonzalez, M.; Jayasundara, N. The Utility of Novel Renal Biomarkers in Assessment of Chronic Kidney Disease of Unknown Etiology (CKDu): A Review. Int. J. Environ. Res. Public Health 2020, 17, 9522. [Google Scholar] [CrossRef]
- Murray, P.T.; Mehta, R.L.; Shaw, A.; Ronco, C.; Endre, Z.; Kellum, J.A.; Chawla, L.S.; Cruz, D.; Ince, C.; Okusa, M.D. Potential use of biomarkers in acute kidney injury: Report and summary of recommendations from the 10th Acute Dialysis Quality Initiative consensus conference. Kidney Int. 2014, 85, 513–521. [Google Scholar] [CrossRef]
- Ng, D.K.; Schwartz, G.J.; Schneider, M.F.; Furth, S.L.; Warady, B.A. Combination of pediatric and adult formulas yield valid glomerular filtration rate estimates in young adults with a history of pediatric chronic kidney disease. Kidney Int. 2018, 94, 170–177. [Google Scholar] [CrossRef]
- WHO Multicentre Growth Reference Study Group. WHO Child Growth Standards based on length/height, weight and age. Acta Paediatr. Suppl. 2006, 450, 76–85. [Google Scholar] [CrossRef]
- Carrasco, A.V. The AMAI System of Classifying Households by Socio-Economic Level: ESOMAR; Health & Environmental Research Online (HERO): Durham, NC, USA, 2002. [Google Scholar]
- Tanner, E.M.; Bornehag, C.-G.; Gennings, C. Repeated holdout validation for weighted quantile sum regression. MethodsX 2019, 6, 2855–2860. [Google Scholar] [CrossRef] [PubMed]
- Wettersten, N.; Katz, R.; Shlipak, M.G.; Scherzer, R.; Waikar, S.S.; Ix, J.H.; Estrella, M.M. Urinary Biomarkers and Kidney Outcomes: Impact of Indexing Versus Adjusting for Urinary Creatinine. Kidney Med. 2021, 3, 546–554.e1. [Google Scholar] [CrossRef]
- Kuiper, J.R.; O’Brien, K.M.; Ferguson, K.K.; Buckley, J.P. Urinary specific gravity measures in the U.S. population: Implications for the adjustment of non-persistent chemical urinary biomarker data. Environ. Int. 2021, 156, 106656. [Google Scholar] [CrossRef] [PubMed]
- Levin, A.; Stevens, P.E.; Bilous, R.W.; Coresh, J.; De Francisco, A.L.M.; De Jong, P.E.; Griffith, K.E.; Hemmelgarn, B.R.; Iseki, K.; Lamb, E.J.; et al. Kidney disease: Improving global outcomes (KDIGO) CKD work group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar]
- Howe, C.G.; Margetaki, K.; Vafeiadi, M.; Roumeliotaki, T.; Karachaliou, M.; Kogevinas, M.; McConnell, R.; Eckel, S.P.; Conti, D.V.; Kippler, M.; et al. Prenatal metal mixtures and child blood pressure in the Rhea mother-child cohort in Greece. Environ. Health 2021, 20, 1. [Google Scholar] [CrossRef]
- De Silva, P.; Gunasekara, T.; Gunarathna, S.D.; Sandamini, P.; Pinipa, R.A.I.; Ekanayake, E.; Thakshila, W.; Jayasinghe, S.S.; Chandana, E.P.S.; Jayasundara, N. Urinary Biomarkers of Renal Injury KIM-1 and NGAL: Reference Intervals for Healthy Pediatric Population in Sri Lanka. Children 2021, 8, 684. [Google Scholar] [CrossRef]
- McWilliam, S.J.; Antoine, D.J.; Sabbisetti, V.; Pearce, R.E.; Jorgensen, A.L.; Lin, Y.; Leeder, J.S.; Bonventre, J.V.; Smyth, R.L.; Pirmohamed, M. Reference intervals for urinary renal injury biomarkers KIM-1 and NGAL in healthy children. Biomark. Med. 2014, 8, 1189–1197. [Google Scholar] [CrossRef]
- Zheng, L.; Kuo, C.C.; Fadrowski, J.; Agnew, J.; Weaver, V.M.; Navas-Acien, A. Arsenic and Chronic Kidney Disease: A Systematic Review. Curr. Environ. Health Rep. 2014, 1, 192–207. [Google Scholar] [CrossRef]
- Satarug, S.; Gobe, G.C.; Vesey, D.A.; Phelps, K.R. Cadmium and Lead Exposure, Nephrotoxicity, and Mortality. Toxics 2020, 8, 86. [Google Scholar] [CrossRef]
- Huang, M.; Choi, S.J.; Kim, D.W.; Kim, N.Y.; Park, C.H.; Yu, S.D.; Kim, D.S.; Park, K.S.; Song, J.S.; Kim, H.; et al. Risk assessment of low-level cadmium and arsenic on the kidney. J. Toxicol. Environ. Health A 2009, 72, 1493–1498. [Google Scholar] [CrossRef]
- Penders, J.; Delanghe, J.R. Alpha 1-microglobulin: Clinical laboratory aspects and applications. Clin. Chim. Acta 2004, 346, 107–118. [Google Scholar] [CrossRef]
- Bernard, A. Renal dysfunction induced by cadmium: Biomarkers of critical effects. Biometals 2004, 17, 519–523. [Google Scholar] [CrossRef]
- Butler-Dawson, J.; James, K.A.; Krisher, L.; Jaramillo, D.; Dally, M.; Neumann, N.; Pilloni, D.; Cruz, A.; Asensio, C.; Johnson, R.J.; et al. Environmental metal exposures and kidney function of Guatemalan sugarcane workers. J. Expo. Sci. Environ. Epidemiol. 2022, 32, 461–471. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Li, M.; Han, T.-x.; Chen, J.-w.; Ye, L.-x.; Wang, Q.; Zhou, Y.-k. Benchmark Dose Estimation for Cadmium-Induced Renal Tubular Damage among Environmental Cadmium-Exposed Women Aged 35–54 Years in Two Counties of China. PLoS ONE 2014, 9, e115794. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, Z.A.; Smith, L.M. Biological indicators of cadmium exposure and toxicity. Exp. Suppl. 1986, 50, 124–130. [Google Scholar] [CrossRef]
- Catania, J.M.; Chen, G.; Parrish, A.R. Role of matrix metalloproteinases in renal pathophysiologies. Am. J. Physiol. Ren. Physiol. 2007, 292, F905–F911. [Google Scholar] [CrossRef]
- Genovese, F.; Manresa, A.A.; Leeming, D.J.; Karsdal, M.A.; Boor, P. The extracellular matrix in the kidney: A source of novel non-invasive biomarkers of kidney fibrosis? Fibrogenes. Tissue Repair. 2014, 7, 4. [Google Scholar] [CrossRef]
- Sanders, A.P.; Mazzella, M.J.; Malin, A.J.; Hair, G.M.; Busgang, S.A.; Saland, J.M.; Curtin, P. Combined exposure to lead, cadmium, mercury, and arsenic and kidney health in adolescents age 12-19 in NHANES 2009-2014. Environ. Int. 2019, 131, 104993. [Google Scholar] [CrossRef]
- Luo, J.; Hendryx, M. Metal mixtures and kidney function: An application of machine learning to NHANES data. Environ. Res. 2020, 191, 110126. [Google Scholar] [CrossRef]
- Eichler, T.; Ma, Q.; Kelly, C.; Mishra, J.; Parikh, S.; Ransom, R.F.; Devarajan, P.; Smoyer, W.E. Single and combination toxic metal exposures induce apoptosis in cultured murine podocytes exclusively via the extrinsic caspase 8 pathway. Toxicol. Sci. 2006, 90, 392–399. [Google Scholar] [CrossRef]
- Barbier, O.; Jacquillet, G.; Tauc, M.; Cougnon, M.; Poujeol, P. Effect of Heavy Metals on, and Handling by, the Kidney. Nephron Physiol. 2005, 99, p105–p110. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.-N.; Tain, Y.-L. Adverse Impact of Environmental Chemicals on Developmental Origins of Kidney Disease and Hypertension. Front. Endocrinol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Sabolić, I. Common Mechanisms in Nephropathy Induced by Toxic Metals. Nephron Physiol. 2006, 104, p107–p114. [Google Scholar] [CrossRef]
- Daenen, K.; Andries, A.; Mekahli, D.; Van Schepdael, A.; Jouret, F.; Bammens, B. Oxidative stress in chronic kidney disease. Pediatr. Nephrol. 2019, 34, 975–991. [Google Scholar] [CrossRef]
- Li, J.; Ma, L.; Yu, H.; Yao, Y.; Xu, Z.; Lin, W.; Wang, L.; Wang, X.; Yang, H. MicroRNAs as Potential Biomarkers for the Diagnosis of Chronic Kidney Disease: A Systematic Review and Meta-Analysis. Front. Med. 2021, 8, 782561. [Google Scholar] [CrossRef]
- Bidin, M.Z.; Shah, A.M.; Stanslas, J.; Seong, C.L.T. Blood and urine biomarkers in chronic kidney disease: An update. Clin. Chim. Acta 2019, 495, 239–250. [Google Scholar] [CrossRef]
- Davis, M.A.; Gilbert-Diamond, D.; Karagas, M.R.; Li, Z.; Moore, J.H.; Williams, S.M.; Frost, H.R. A Dietary-Wide Association Study (DWAS) of Environmental Metal Exposure in US Children and Adults. PLoS ONE 2014, 9, e104768. [Google Scholar] [CrossRef] [PubMed]
- Day, P.L.; Nelson, E.J.; Bluhm, A.M.; Wood-Wentz, C.M.; Jannetto, P.J. Discovery of an arsenic and mercury co-elevation in the Midwest United States using reference laboratory data. Environ. Pollut. 2019, 254, 113049. [Google Scholar] [CrossRef]
- Grandjean, P.; Budtz-Jørgensen, E. An ignored risk factor in toxicology: The total imprecision of exposure assessment. Pure Appl. Chem. 2010, 82, 383–391. [Google Scholar] [CrossRef]
- Weaver, V.M.; Kotchmar, D.J.; Fadrowski, J.J.; Silbergeld, E.K. Challenges for environmental epidemiology research: Are biomarker concentrations altered by kidney function or urine concentration adjustment? J. Expo. Sci. Environ. Epidemiol. 2016, 26, 1–8. [Google Scholar] [CrossRef]
- Carrico, C.; Gennings, C.; Wheeler, D.C.; Factor-Litvak, P. Characterization of Weighted Quantile Sum Regression for Highly Correlated Data in a Risk Analysis Setting. J. Agric. Biol. Environ. Stat. 2015, 20, 100–120. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| N (%) | |
|---|---|
| Child Sex | |
| Male | 252 (51.01) |
| Female | 242 (48.99) |
| Socioeconomic Status during Pregnancy | |
| Lower | 265 (53.64) |
| Medium | 184 (37.25) |
| Higher | 45 (9.11) |
| Child Body Mass Index | |
| Normal | 272 (55.06) |
| Overweight | 118 (23.89) |
| Obese | 104 (21.05) |
| Indoor Tobacco Smoke Exposure during Pregnancy | |
| No | 344 (69.64) |
| Yes | 150 (30.36) |
| Mean (Range) | |
| Age at urine collection (years) | 9.66 (8.08–12.07) |
| Child Body Mass Index z-score | 0.86 (−3.00–3.98) |
| Kidney function measures | |
| eGFR (mL/min/1.73 m2) (n = 422) | 99.50 (46.76–201.33) |
| Serum Cystatin C (mg/L) | 0.73 (0.32–1.56) |
| Median (25th–75th Percentile) | |
| Second Trimester Urine Metal Concentrations † | |
| Arsenic (µg/L) | 13.72 (9.07–22.48) |
| Cadmium (µg/L) | 0.22 (0.14–0.37) |
| Lead (µg/L) | 3.42 (2.08–6.66) |
| Mercury (µg/L) | 1.12 (0.67–2.14) |
| Second Trimester Blood Metal Concentrations (n = 470) | |
| Arsenic (µg/dL) | 0.07 (0.06–0.09) |
| Cadmium (µg/dL) | 0.02 (0.02–0.03) |
| Lead (µg/dL) | 2.85 (1.97–4.40) |
| Urinary Kidney Injury Biomarkers at 8–12 years of age | |
| Albumin (mg/dl) | 2.39 (1.26–4.80) |
| Cystatin C (ng/mL) | 12.03 (4.94–21.62) |
| KIM-1 (ng/mL) | 0.45 (0.21–0.79) |
| NGAL (ng/mL) | 8.24 (3.38–22.91) |
| A1M (ng/mL) | 170.74 (108.53–265.76) |
| B2M (ng/mL) | 223.43 (79.05–473.11) |
| RBP4 (ng/mL) | 1418.52 (625.26–2813.50) |
| OPN (ng/mL) | 774.13 (246.53–1404.00) |
| Uromodulin (MFI) | 3943.00 (2476.73–5747.65) |
| GSTα (ng/mL) | 0.67 (0.09–4.47) |
| FABP1 (ng/mL) | 17.91 (12.98–26.47) |
| EGF (ng/mL) | 43.13 (26.08–70.14) |
| Clusterin (ng/mL) | 678.26 (341.57–1334.53) |
| Calbindin (ng/mL) | 22.29 (8.26–66.17) |
| TIMP1 (ng/mL) | 0.94 (0.63–1.49) |
| IP10 (ng/mL) | 0.004 (0.003–0.02) |
| Renin (ng/mL) | 0.08 (0.02–0.18) |
| Urine | Blood | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Arsenic | Cadmium | Mercury | Lead | Arsenic | Cadmium | Lead | ||||||||
| Beta | 95% CI | Beta | 95% CI | Beta | 95% CI | Beta | 95% CI | Beta | 95% CI | Beta | 95% CI | Beta | 95% CI | |
| Glomerular | ||||||||||||||
| eGFR (mL/min/1.73 m2) | −0.19 | −1.78–1.40 | −1.27 | 2.99–0.45 | 0.69 | −0.89–2.27 | 0.27 | −1.22–1.78 | 1.03 | −2.19–4.24 | −1.07 | −3.89–1.75 | −0.08 | −2.46–2.30 |
| Albumin (mg/dL) | 0.16 | 0.05–0.26 | 0.22 | 0.11–0.33 | 0.10 | −0.002–0.21 | 0.14 | 0.04–0.24 | −0.04 | −0.25–0.17 | 0.06 | −0.12–0.23 | 0.02 | −0.13–0.18 |
| Cystatin C (ng/mL) | 0.11 | 0.01–0.21 | 0.13 | 0.03–0.23 | 0.03 | −0.06–0.13 | 0.08 | −0.01–0.17 | −0.06 | −0.25–0.13 | 0.09 | −0.07–0.25 | 0.03 | −0.11–0.17 |
| Tubular | ||||||||||||||
| KIM-1 (ng/mL) | 0.07 | −0.01–0.16 | 0.08 | −0.01–0.17 | 0.05 | −0.04–0.13 | 0.08 | 0.01–0.16 | −0.09 | −0.26–0.08 | 0.11 | −0.03–0.25 | −0.01 | −0.13–0.12 |
| NGAL (ng/mL) | 0.16 | −0.08–0.41 | 0.16 | −0.11–0.42 | −0.03 | −0.27–0.22 | 0.18 | −0.05–0.42 | −0.02 | −0.53–0.49 | 0.18 | −0.24–0.61 | −0.07 | −0.44–0.31 |
| A1M (ng/mL) | 0.02 | −0.04–0.08 | 0.08 | 0.02–0.14 | 0.03 | −0.03–0.08 | 0.02 | −0.03–0.07 | 0.002 | −0.11–0.12 | 0.04 | −0.06–0.13 | 0.02 | −0.07–0.10 |
| B2M (ng/mL) | 0.11 | −0.01–0.23 | 0.14 | 0.01–0.28 | 0.07 | −0.05–0.20 | 0.02 | −0.10–0.14 | −0.25 | −0.50–−0.001 | 0.09 | −0.12–0.30 | −0.01 | −0.20–0.17 |
| RBP4 (ng/mL) | 0.07 | −0.04–0.17 | 0.10 | −0.01–0.22 | 0.03 | −0.08–0.14 | 0.03 | −0.07–0.14 | −0.28 | −0.49–−0.07 | 0.12 | −0.06–0.30 | −0.03 | −0.19–0.12 |
| OPN (ng/mL) | −0.01 | −0.14–0.11 | 0.01 | −0.12–0.15 | 0.02 | −0.10–0.15 | 0.05 | −0.07–0.16 | −0.12 | −0.39–0.13 | −0.12 | −0.33–0.09 | −0.03 | −0.21–0.16 |
| Uromodulin (MFI) | −0.002 | −0.08–0.08 | −0.01 | −0.10–0.08 | −0.03 | −0.11–0.06 | −0.05 | −0.13–0.03 | −0.18 | −0.34–−0.02 | 0.02 | −0.12–0.15 | −0.09 | −0.21–0.03 |
| GSTα (ng/mL) | 0.09 | −0.14–0.31 | 0.12 | −0.13–0.36 | 0.19 | −0.03–0.41 | 0.03 | −0.18–0.24 | 0.01 | −0.44–0.46 | 0.47 | 0.09–0.85 | 0.06 | −0.28–0.39 |
| Liver | ||||||||||||||
| FABP1 (ng/mL) | 0.06 | −0.003–0.13 | 0.04 | −0.03–0.11 | 0.04 | −0.02–0.11 | 0.02 | −0.04–0.08 | 0.07 | −0.06–0.20 | −0.01 | −0.12–0.10 | −0.01 | −0.10–0.09 |
| General | ||||||||||||||
| EGF (ng/mL) | 0.03 | −0.03–0.08 | 0.07 | 0.01–0.12 | 0.04 | −0.02–0.09 | 0.03 | −0.02–0.08 | −0.11 | −0.22–−0.003 | 0.02 | −0.08–0.11 | −0.02 | −0.10–0.06 |
| Clusterin (ng/mL) | 0.06 | −0.03–0.15 | 0.12 | 0.03–0.22 | 0.05 | −0.04–0.14 | 0.06 | −0.03–0.15 | −0.09 | −0.27–0.10 | 0.01 | −0.14–0.16 | 0.02 | −0.12–0.14 |
| Calbindin (ng/mL) | −0.03 | −0.20–0.14 | 0.07 | −0.11–0.25 | −0.01 | −0.18–0.16 | −0.09 | −0.25–0.06 | −0.03 | −0.38–0.31 | 0.06 | −0.24–0.35 | −0.17 | −0.42–0.08 |
| TIMP1 (ng/mL) | 0.06 | 0.01–0.12 | 0.10 | 0.04–0.16 | 0.03 | −0.03–0.08 | 0.06 | 0.005–0.11 | −0.06 | −0.18–0.05 | 0.09 | −0.01–0.18 | 0.005 | −0.08–0.09 |
| IP10 (ng/mL) | 0.13 | 0.02–0.24 | 0.09 | −0.03–0.21 | −0.05 | −0.17–0.06 | 0.02 | −0.08–0.13 | 0.08 | −0.15–0.30 | −0.12 | −0.31–0.07 | 0.02 | −0.15–0.18 |
| Renin (ng/mL) | 0.08 | −0.05–0.21 | 0.09 | −0.04–0.23 | −0.01 | −0.14–0.12 | 0.01 | −0.11–0.14 | 0.09 | −0.17–0.35 | −0.06 | −0.29–0.16 | 0.02 | −0.17–0.22 |
| n | Estimate | Standard Error | 2.50% | 97.50% | Metal Weights | ||||
|---|---|---|---|---|---|---|---|---|---|
| w1 | w2 | w3 | w4 | ||||||
| Glomerular | |||||||||
| Albumin (ng/mL) | 491 | 0.23 | 0.07 | 0.10 | 0.37 | Cd: 0.50 | As: 0.20 | Hg: 0.15 | Pb: 0.15 |
| Cystatin C (ng/mL) | 494 | 0.17 | 0.07 | 0.05 | 0.31 | As: 0.36 | Cd: 0.32 | Hg: 0.17 | Pb: 0.14 |
| Tubular | |||||||||
| KIM-1 (ng/mL) | 494 | 0.13 | 0.05 | 0.02 | 0.24 | As: 0.31 | Pb: 0.27 | Hg: 0.23 | Cd: 0.20 |
| B2M (ng/mL) | 493 | 0.18 | 0.07 | 0.05 | 0.32 | Cd: 0.47 | Hg: 0.23 | As: 0.19 | Pb: 0.11 |
| RBP4 (ng/mL) | 494 | 0.15 | 0.07 | 0.02 | 0.28 | Cd: 0.51 | Pb: 0.19 | Hg: 0.15 | As: 0.14 |
| Liver | |||||||||
| FABP1 (ng/mL) | 494 | 0.11 | 0.04 | 0.03 | 0.19 | As: 0.69 | Hg: 0.16 | Cd: 0.13 | Pb: 0.02 |
| General | |||||||||
| EGF (ng/mL) | 494 | 0.06 | 0.03 | 0.002 | 0.13 | Cd: 0.45 | Hg: 0.25 | Pb: 0.18 | As: 0.13 |
| Clusterin (ng/mL) | 494 | 0.13 | 0.05 | 0.03 | 0.22 | Cd: 0.47 | Pb: 0.22 | As: 0.17 | Hg: 0.13 |
| TIMP1 (ng/mL) | 494 | 0.13 | 0.04 | 0.05 | 0.20 | Cd: 0.44 | As: 0.30 | Hg: 0.14 | Pb: 0.12 |
| IP10 (ng/mL) | 494 | 0.15 | 0.07 | 0.02 | 0.28 | As: 0.65 | Cd: 0.21 | Pb: 0.10 | Hg: 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Politis, M.D.; Yao, M.; Gennings, C.; Tamayo-Ortiz, M.; Valvi, D.; Kim-Schulze, S.; Qi, J.; Amarasiriwardena, C.; Pantic, I.; Tolentino, M.C.; et al. Prenatal Metal Exposures and Associations with Kidney Injury Biomarkers in Children. Toxics 2022, 10, 692. https://doi.org/10.3390/toxics10110692
Politis MD, Yao M, Gennings C, Tamayo-Ortiz M, Valvi D, Kim-Schulze S, Qi J, Amarasiriwardena C, Pantic I, Tolentino MC, et al. Prenatal Metal Exposures and Associations with Kidney Injury Biomarkers in Children. Toxics. 2022; 10(11):692. https://doi.org/10.3390/toxics10110692
Chicago/Turabian StylePolitis, Maria D., Meizhen Yao, Chris Gennings, Marcela Tamayo-Ortiz, Damaskini Valvi, Seunghee Kim-Schulze, Jingjing Qi, Chitra Amarasiriwardena, Ivan Pantic, Mari Cruz Tolentino, and et al. 2022. "Prenatal Metal Exposures and Associations with Kidney Injury Biomarkers in Children" Toxics 10, no. 11: 692. https://doi.org/10.3390/toxics10110692
APA StylePolitis, M. D., Yao, M., Gennings, C., Tamayo-Ortiz, M., Valvi, D., Kim-Schulze, S., Qi, J., Amarasiriwardena, C., Pantic, I., Tolentino, M. C., Estrada-Gutierrez, G., Greenberg, J. H., Téllez-Rojo, M. M., Wright, R. O., Sanders, A. P., & Rosa, M. J. (2022). Prenatal Metal Exposures and Associations with Kidney Injury Biomarkers in Children. Toxics, 10(11), 692. https://doi.org/10.3390/toxics10110692