
Efficiency of Inventory in Thai Hospitals: Comparing Traditional and Vendor-Managed Inventory Systems


Abstract
1. Introduction
1.1. Supply Chain Coordination in Healthcare
1.2. Benefits and Models of VMI
- Vendor-Replenished Inventory (VRI);
- Vendor-Managed Inventory Services (VMIS);
- Third Party-Replenished Inventory (3RI);
- Third Party-Managed Inventory Services (3MIS);
- Inventory Management Technical Assistance (IMTA).
- Strict Quality Control Measures: Enforcing strict quality-control standards through well-defined contractual agreements that specify quality expectations.
- Supplier Audits and Performance Reviews: Regularly auditing and reviewing supplier performance to ensure compliance with quality standards.
- Collaborative Relationships: Establishing a collaborative relationship with suppliers, like the strategies in trade credit models. This ensures that both parties prioritize quality in addition to cost efficiency. This approach is supported by the findings of Zavanella and Zanoni [21], which discussed the success of integrating VMI with consignment agreements to benefit both buyers and vendors through maintaining high-quality standards while managing costs effectively.
1.3. Application of VMI in Hospitals
2. Materials and Methods
2.1. Study Design
- Simulation Modeling Approach
2.2. Data Collection and Preparation
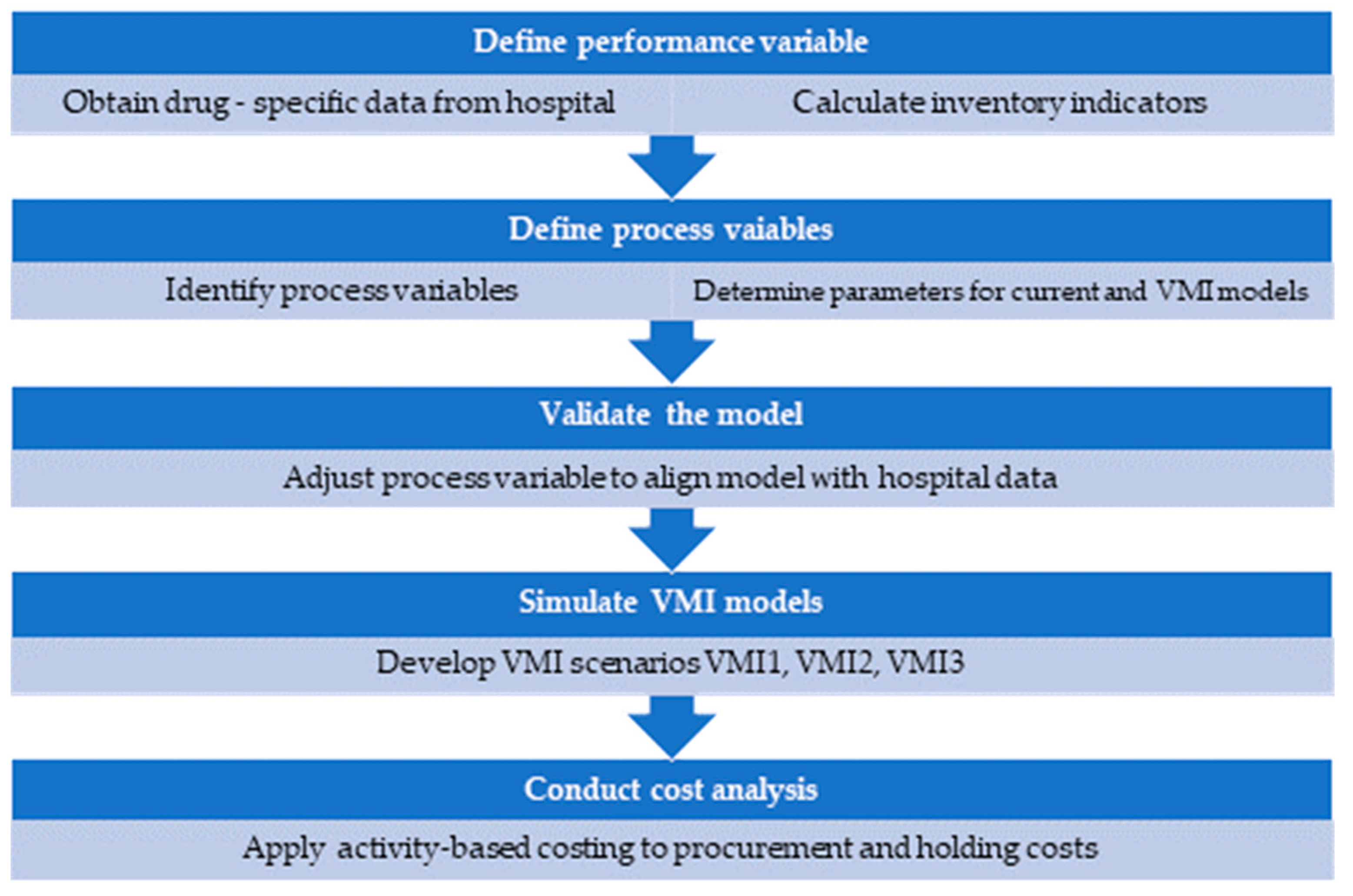
2.3. Model Development and Validation
- Performance Variables
- Process Variables
Scenarios of VMI Model Development
- VMI1 Model: This model aimed to enhance efficiency for items with lower turnover rates by targeting items with below-average ITR, adjusting purchase volumes to achieve an average ITR while maintaining annual medicine procurement values consistent with the current model.
- VMI2 Model: This model aimed to reduce holding costs and ensure timely availability of medicines through implementing more frequent replenishments to maintain a 1-month supply for each order.
- VMI3 Model: This scenario eliminated safety stock via automatically reordering once stock levels reached a minimum threshold thus minimizing stockouts and excess inventory.
2.4. Cost Analysis of Inventory Management
- The Current Model utilized group purchasing to procure 400 items annually and a special procurement method for the remaining 500 items, requiring individual processing.
- The VMI Models employed a fixed procurement cost with automated transaction, eliminating traditional procurement processes.
3. Results
3.1. Performance of Current Inventory Management System
3.2. Performance of VMI Scenarios
- Objective: Enhance efficiency for items with low ITR.
- Results: This model increased the ITR to 7.76, reducing the average inventory value by 36% from USD 1.6 million to USD 1.01 million. It demonstrated significant improvements in managing low turnover items.
- Objective: Maintain a 1-month supply with more frequent replenishments.
- Results: The ITR further increased to 12.80, reducing the average inventory value by 44% from the current model and 13% from the VMI1 model. This model balanced inventory reduction with a timely availability of medicines.
- Objective: Minimize safety stock with automatic reordering at minimum levels.
- Results: The inventory was reduced by 70% compared to the current model and by over 50% compared to the VMI1 model, maintaining an ITR of 12.80. This model demonstrated significant cost savings by minimizing safety stock.
3.3. Cost Analysis of Inventory Management
- VMI1 reduced total costs by 40% to USD 295.1 K primarily through fixed management and lower order processing costs.
- VMI2 further decreased costs by 47%, aligning with the model’s strategy of a 1-month supply and lower inventory holding.
- VMI3 achieved a 70% reduction in inventory costs and a 69% reduction in total holding and capital costs by eliminating safety stock.
3.4. Summary of Key Findings
4. Discussion
- Contributions of the Study:
- Empirical Evidence: The study provides empirical evidence of the effectiveness of VMI models in enhancing inventory turnover rates (ITR) and reducing inventory holding costs. This evidence supports the practical application of VMI in improving hospital inventory management.
- Customized Strategies: The study highlights the importance of tailored inventory management strategies, such as the elimination of safety stock, which can lead to greater operational efficiency. The study also emphasizes the need for customized VMI approaches to address specific challenges and optimize inventory practices.
- Study Limitations
- Future Research
- The detailed cost structures and categories of medicines and supplies suitable for VMI.
- The levels of information sharing and hospital readiness for VMI implementation.
- Regulations necessary to support comprehensive VMI implementation, particularly for public hospitals.
- The long-term sustainability of VMI models.
- The integration of AI and real-time optimization tools to assess their impact on reducing stockouts and waste in VMI systems.
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Monton, C.; Charoenchai, L.; Suksaeree, J. Purchasing and Inventory Management by Pharmacist of a Private Hospital in Northeast of Thailand. Int. J. Pharm. Pharm. Sci. 2014, 6, 401–405. [Google Scholar]
- Khalil, V.; Foo, S. A Lean Approach for Improving Medicines Management in Australia’s First Cardiac Hospital Inventory System. Int. J. Health Plann Manag. 2024, 39, 1642–1651. [Google Scholar] [CrossRef] [PubMed]
- Krichanchai, S.; MacCarthy, B.L. The Adoption of Vendor Managed Inventory for Hospital Pharmaceutical Supply. Int. J. Logist. Manag. 2017, 28, 755–780. [Google Scholar] [CrossRef]
- van den Bogaert, J.; van Jaarsveld, W. Vendor-Managed Inventory in Practice: Understanding and Mitigating the Impact of Supplier Heterogeneity. Int. J. Prod. Res. 2022, 60, 6087–6103. [Google Scholar] [CrossRef]
- Sharma, N.; Singhi, R. Performance Evaluation of Vendor Managed Inventory Variables in Hospitals Using ANOVA Technique. Int. J. Supply Chain Inventory Manag. 2018, 3, 66. [Google Scholar] [CrossRef]
- Sumrit, D. Understanding Critical Success Factors of Vendor-Managed Inventory in Healthcare Sector: A Case Study in Thailand. Int. J. Healthc. Manag. 2021, 14, 629–640. [Google Scholar] [CrossRef]
- Kritchanchai, D. A Framework for Healthcare Supply Chain Improvement in Thailand. Oper. Supply Chain Manag. Int. J. 2014, 5, 103–113. [Google Scholar] [CrossRef]
- Kanyakam, S.; Pimpa, W.; Kamlai, K. Inventory Management in Medical Stores of Secondary Care Unit Service Level Hospitals in Northeast of Thailand. Eng. Access 2018, 4, 17–23. [Google Scholar] [CrossRef]
- World Health Organization Health Products Policy and Standards. Available online: https://www.who.int/teams/health-product-policy-and-standards/medicines-selection-ip-and-affordability/medicines-policy/medicines-supply (accessed on 27 June 2024).
- Williams, B.D.; Tokar, T. A Review of Inventory Management Research in Major Logistics Journals: Themes and Future Directions. Int. J. Logist. Manag. 2008, 19, 212–232. [Google Scholar] [CrossRef]
- Panigrahi, R.R.; Shrivastava, A.K.; Kapur, P.K. Impact of Inventory Management Practices on the Operational Performances of SMEs: Review and Future Research Directions. Int. J. Syst. Assur. Eng. Manag. 2024, 15, 1934–1955. [Google Scholar] [CrossRef]
- Arshinder; Kanda, A.; Deshmukh, S.G. Supply Chain Coordination: Perspectives, Empirical Studies and Research Directions. Int. J. Prod. Econ. 2008, 115, 316–335. [Google Scholar] [CrossRef]
- Li, X.; Wang, Q. Coordination Mechanisms of Supply Chain Systems. Eur. J. Oper. Res. 2007, 179, 1–16. [Google Scholar] [CrossRef]
- Achabal, D.D.; McIntyre, S.H.; Smith, S.A.; Kalyanam, K. A Decision Support System for Vendor Managed Inventory. J. Retail. 2000, 76, 430–454. [Google Scholar] [CrossRef]
- Zhao, R. A Review on Theoretical Development of Vendor-Managed Inventory in Supply Chain. Am. J. Ind. Bus. Manag. 2019, 9, 999–1010. [Google Scholar] [CrossRef]
- Kong, H.; Feng, D.; Fan, W.; Li, Q. Design and Implementation of Pharmaceutical Logistics and Supply Chain Management System for Hospital. In Proceedings of the 2015 International Conference on Advances in Mechanical Engineering and Industrial Informatics, Zhengzhou, China, 11–12 April 2015; Atlantis Press: Paris, France, 2015. [Google Scholar]
- Watson, N.; Serumaga, B.; McCord, J. Selecting and Implementing Vendor Managed Inventory Systems for Public Health Supply Chains; International Association of Public Health Logisticians: Arlington, VA, USA, 2012. [Google Scholar]
- Chen, B.; Xie, W.; Huang, F.; He, J. Quality Competition and Coordination in a VMI Supply Chain with Two Risk-Averse Manufacturers. J. Ind. Manag. Optim. 2021, 17, 2903. [Google Scholar] [CrossRef]
- Gümüş, M.; Jewkes, E.M.; Bookbinder, J.H. Impact of Consignment Inventory and Vendor-Managed Inventory for a Two-Party Supply Chain. Int. J. Prod. Econ. 2008, 113, 502–517. [Google Scholar] [CrossRef]
- Abad, P.L.; Jaggi, C.K. A Joint Approach for Setting Unit Price and the Length of the Credit Period for a Seller When End Demand Is Price Sensitive. Int. J. Prod. Econ. 2003, 83, 115–122. [Google Scholar] [CrossRef]
- Zavanella, L.; Zanoni, S. A One-Vendor Multi-Buyer Integrated Production-Inventory Model: The ‘Consignment Stock’ Case. Int. J. Prod. Econ. 2009, 118, 225–232. [Google Scholar] [CrossRef]
- Chopra, S.; Meindl, P. Supply Chain Management: Strategy, Planning, and Operation; Pearson: London, UK, 2016; ISBN 9780133800203. [Google Scholar]
- Kaplan, R.S.; Anderson, S.R. Time-Driven Activity-Based Costing. Harv. Bus. Rev. 2004, 82, 131–138, 150. [Google Scholar] [CrossRef]
- Law, A.M.; Kelton, W.D. Simulation Modeling and Analysis; Mcgraw-Hill: New York, NY, USA, 2014. [Google Scholar]
- Durlinger, P. Inventory and Holding Costs; Durlinger Consultancy: Posterholt, The Netherlands, 2015. [Google Scholar]
- Badi, I.; Bouraima, M.B.; Stević, Ž.; Oloketuyi, E.A.; Makinde, O.O. Optimizing Vendor-Managed Inventory in Multi-Tier Distribution Systems. Spectr. Oper. Res. 2024, 1, 33–43. [Google Scholar] [CrossRef]
- Joseph, J.F.; Sundarakani, B.; Hosie, P.; Nagarajan, S. Analysis of Vendor Managed Inventory Practices for Greater Supply Chain Performance. Int. J. Logist. Econ. Glob. 2010, 2, 297. [Google Scholar] [CrossRef]
- Brummelhuis, B. Coping with Variability: Improving the Inbound Process of the VMI Holland Warehouse. Master’s Thesis, University of Twente, Enschede, The Netherlands, 2016. [Google Scholar]
- Ganesan, S.; Wicaksono, H.; Fatahi Valilai, O. Enhancing Vendor Managed Inventory with the Application of Blockchain Technology. In Advances in System-Integrated Intelligence; Springer: Cham, Switzerland, 2023; Volume 546, pp. 262–275. [Google Scholar] [CrossRef]
- Viswanadham, Y.V.R.S.; Jayavel, K. A Framework for Data Privacy Preserving in Supply Chain Management Using Hybrid Meta-Heuristic Algorithm with Ethereum Blockchain Technology. Electronics 2023, 12, 1404. [Google Scholar] [CrossRef]
- Zingirian, N. Privacy-Preserving Data Publishing in Small-Sized Business Communities. In Proceedings of the 2023 International Conference on Computational Intelligence, Networks and Security (ICCINS), Mylavaram, India, 22–23 December 2023; pp. 1–6. [Google Scholar]

{kind=link}
| Performance Variable | Definition |
|---|---|
| Variables acquired from the hospital database | |
| Drug name | The name of the medicine listed in the hospital drug inventory |
| Beginning-of-year volume | The quantity of each medicine counted at the start of the fiscal year |
| End-of-year volume | The quantity of each medicine counted at the end of the fiscal year |
| Unit price | The cost of one unit of a medicine |
| Annual procurement volume | The total volume of each medicine in a year |
| Calculated inventory indicators | |
| Annual procurement value | The total value of each medicine in a year, calculated from the annual procurement volume and unit price |
| Actual average inventory volume | The average quantity of each medicine, calculated from the beginning-of-year volume and end-of-year volume |
| Actual average inventory value | The average value of each medicine, calculated by multiplying the average inventory volume by the unit price |
| Annual use rate | The total quantity at which each medicine is dispensed or used within a year, calculated using the formula (beginning-of-year volume + procurement volume − end-of-year volume) |
| Annual use value | The total value of each medicine dispensed or used within a year, calculated by multiplying the annual use rate by the unit price |
| Inventory turnover rate (ITR) | Annual use value/average inventory value |
| Variables | Equation | |
|---|---|---|
| Safety stock level | = | |
| Reorder point | =() | |
| Minimum stock level (min) | = | |
| Maximum stock level (MAX) | = | |
| Calculated average stock level | = | |
| Estimated procurement volume The procurement volume should be rounded up to the package | Current model | = |
| VMI model | = | |
| Hospital’s Actual Data | Current Model | VMI1 Model | VMI2 Model | VMI3 Model | |
|---|---|---|---|---|---|
| Safety stock (days) | 15.00 | 15.00 | 15.00 | 0 | |
| Lead time (days) | 5.00 | 5.00 | 5.00 | 5.00 | |
| Reorder point = stock required during lead time (days) | 20.00 | 20.00 | 20.00 | 5.00 | |
| Inventory turnover rate (ITR) | 6.52 | 6.31 | 7.76 | 12.80 | 12.80 |
| Procurement value per round (USD) | 2042 K | 2042 K | 1056 K | 635 K | 635 K |
| Procurement value per year (USD) | 8168 K | 8168 K | 8191 K | 8122 K | 8122 K |
| Minimum stock value (USD) | 795 K | 698 K | 769 K | 342 K | |
| Maximum stock value (USD) | 2496 K | 1413 K | 1062 K | 635 K | |
| Average inventory value (USD) | 1646 K | 1646 K | 1056 K | 915 K | 488 K |
| Variables | Volume | Frequency | Cost/Unit | Total (USD) |
|---|---|---|---|---|
| Current model | ||||
| Fixed cost of procurement activities | 900 | 1 | 41.18 | 57.6 K |
| Group purchasing method | 400 | 1 | 11.6 | 4.6 K |
| Special selection process | 500 | 6.31 | 4.64 | 14.6 K |
| Total procurement cost | 76.9 K | |||
| Inventory holding cost | 1 | 1 | 411.6 K | 411.6 K |
| Total inventory management cost | 488.5 K | |||
| Capital cost | 1 | 1 | 1646.2 K | 1646.2 K |
| VMI1 model | ||||
| Initial investment for the VMI system | ||||
| Fixed cost of procurement activities | 900 | 1 | 23.1 | 20.8 K |
| VMI provider selection process | 1 | 1 | 10,440 | 10.4 K |
| Special selection process | 0 | 1 | 0.00 | - |
| Total procurement cost | 31.2 K | |||
| Inventory holding cost | 1 | 1 | 263.9 K | 263.9 K |
| Total inventory management cost | 295.1 K | |||
| Capital costs | 1 | 1 | 1055.6 K | 1055.6 K |
| Variables | Current | VMI1 | VMI2 | VMI3 |
|---|---|---|---|---|
| Fixed cost of procurement activities | 57,642 | 3445 | 3445 | 3445 |
| Group purchasing method | 4640 | 0 | 0 | 0 |
| Special selection process | 14,639 | 0 | 0 | 0 |
| VMI provider selection process | 10,445 | 10,445 | 10,445 | |
| Total procurement cost (USD) | 76,921 | 31,230 | 31,230 | 31,230 |
| Holding cost | 411,562 | 263,902 | 228,798 | 122,037 |
| Total inventory management cost (% of current model) | 488,483 - | 295,132 (60%) | 260,028 (53%) | 153,267 (31%) |
| Capital cost of inventory (% of current model) | 1,646,246 - | 1,055,606 (64%) | 915,193 (56%) | 488,147 (30%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adirektawon, S.; Theeraroungchaisri, A.; Sakulbumrungsil, R.C. Efficiency of Inventory in Thai Hospitals: Comparing Traditional and Vendor-Managed Inventory Systems. Logistics 2024, 8, 89. https://doi.org/10.3390/logistics8030089
Adirektawon S, Theeraroungchaisri A, Sakulbumrungsil RC. Efficiency of Inventory in Thai Hospitals: Comparing Traditional and Vendor-Managed Inventory Systems. Logistics. 2024; 8(3):89. https://doi.org/10.3390/logistics8030089
Chicago/Turabian StyleAdirektawon, Sarunya, Anuchai Theeraroungchaisri, and Rungpetch C. Sakulbumrungsil. 2024. "Efficiency of Inventory in Thai Hospitals: Comparing Traditional and Vendor-Managed Inventory Systems" Logistics 8, no. 3: 89. https://doi.org/10.3390/logistics8030089
APA StyleAdirektawon, S., Theeraroungchaisri, A., & Sakulbumrungsil, R. C. (2024). Efficiency of Inventory in Thai Hospitals: Comparing Traditional and Vendor-Managed Inventory Systems. Logistics, 8(3), 89. https://doi.org/10.3390/logistics8030089