
Red Meat Consumption and Cancer Risk: A Systematic Analysis of Global Data

Abstract
:1. Introduction
2. Methods
2.1. Data Source and Selection
2.1.1. Association between Meat Consumption and Cancer Incidence
2.1.2. Effect of Regional Conditions and Customs
2.1.3. Lag of Influence from RMC on CRC Incidence
2.2. Statistical Analysis
2.2.1. Association between RMC and Cancer Incidence
2.2.2. Effect of Regional Conditions and Customs
2.2.3. Lag of Influence from RMC on CRC Incidence
2.2.4. Association between Poultry Meat Consumption or SFC and Cancer Incidence
3. Results and Discussion
3.1. RMC and Cancer Incidence
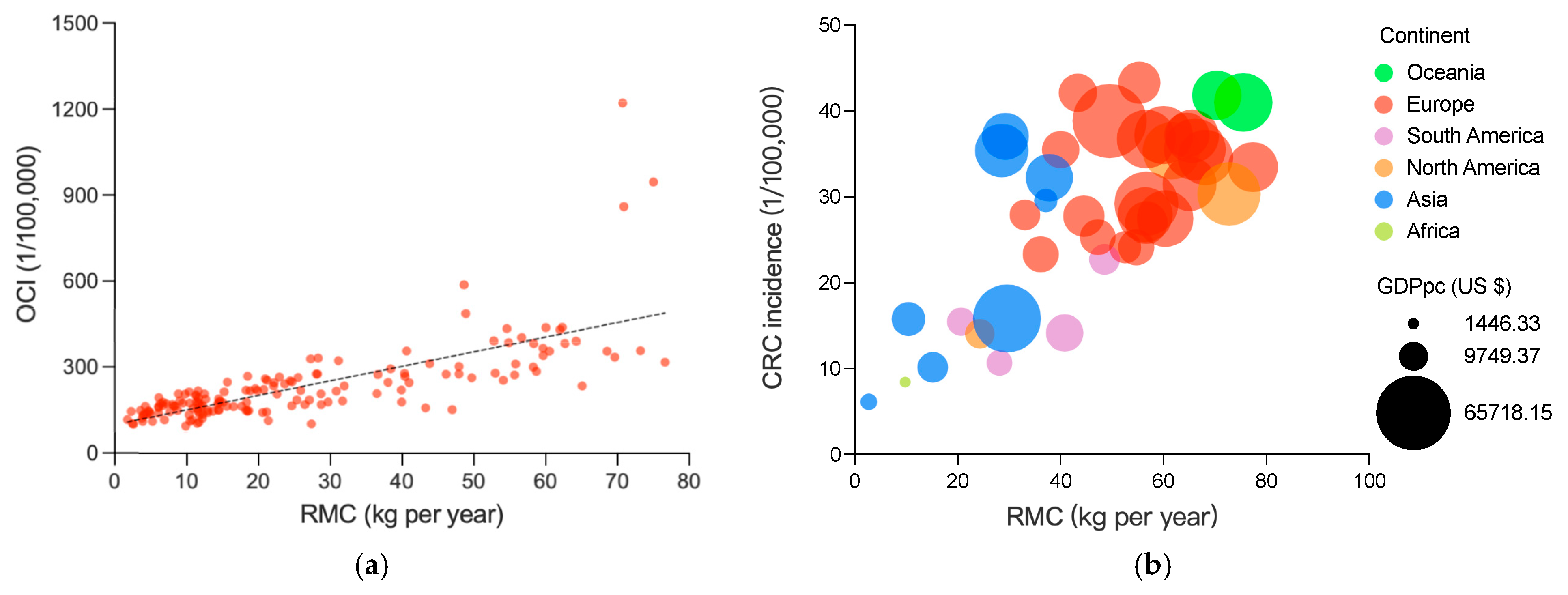
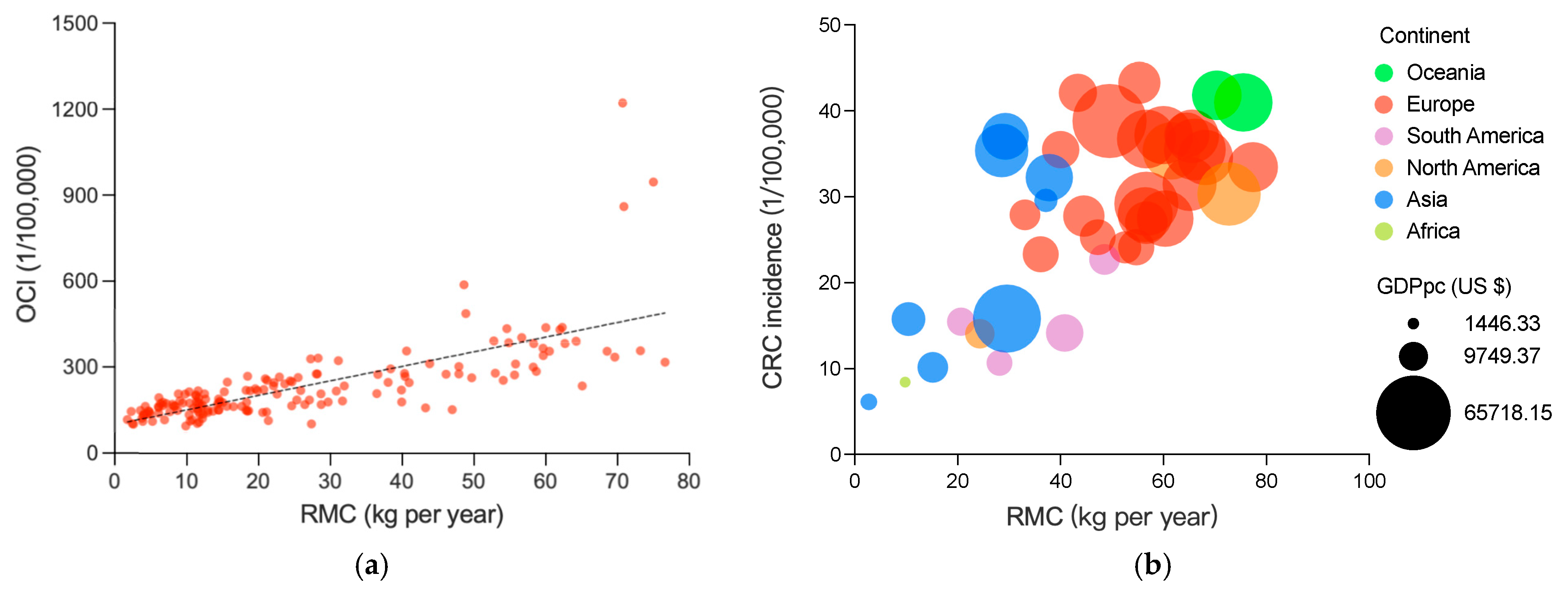
3.1.1. Association between RMC and OCI
3.1.2. Association between RMC and CRC Incidence
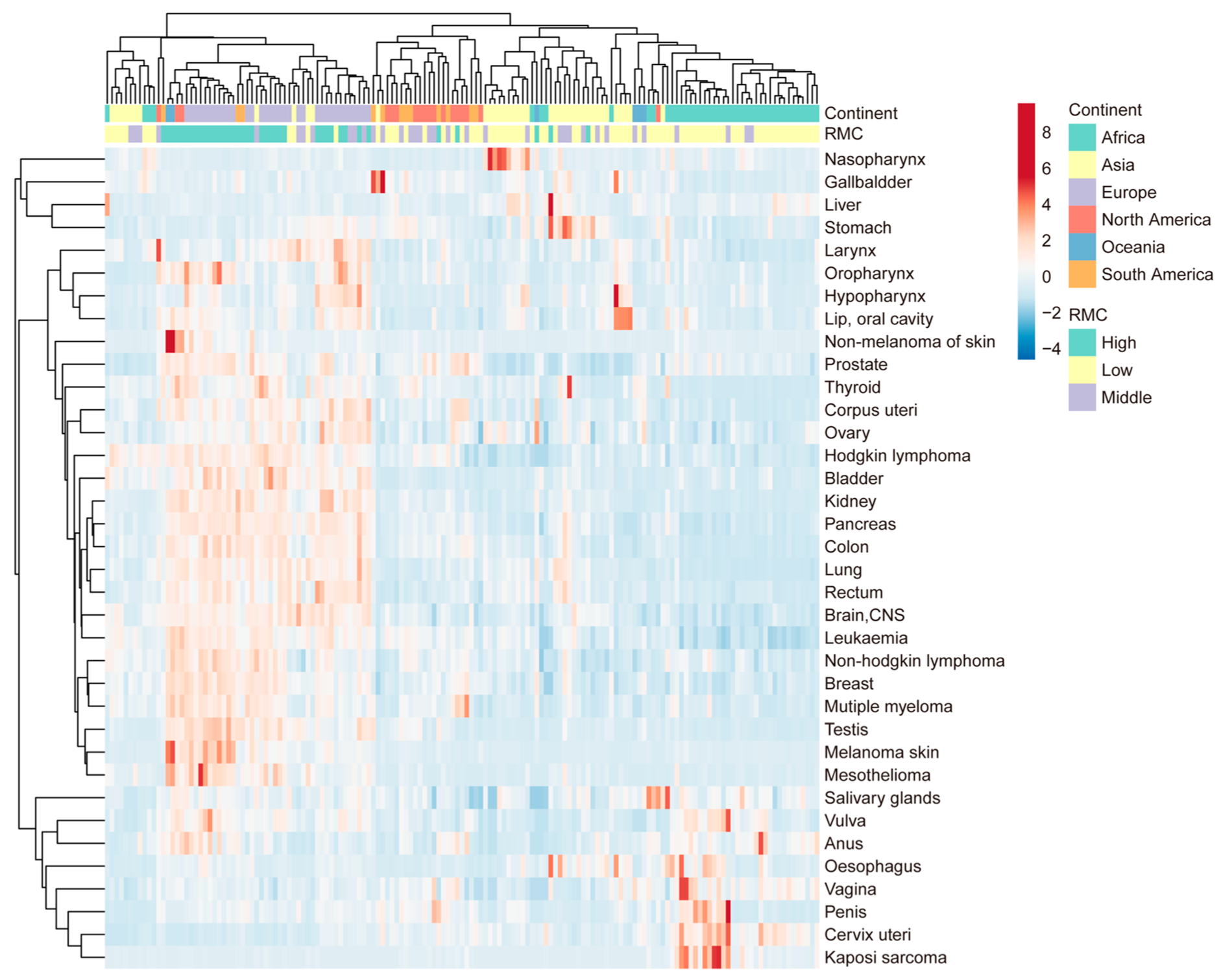
3.1.3. Association between RMC and Other Specific Cancer Incidences
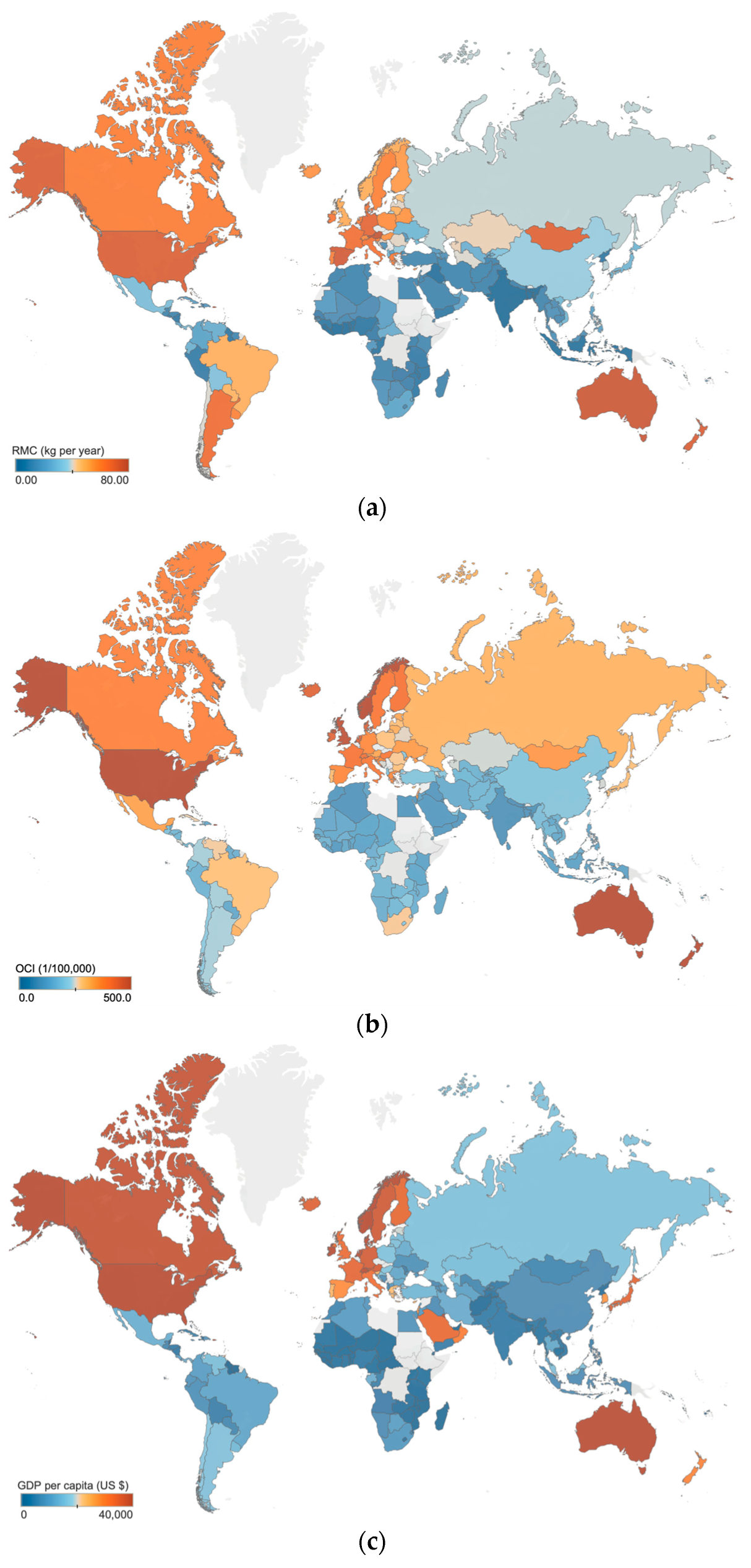
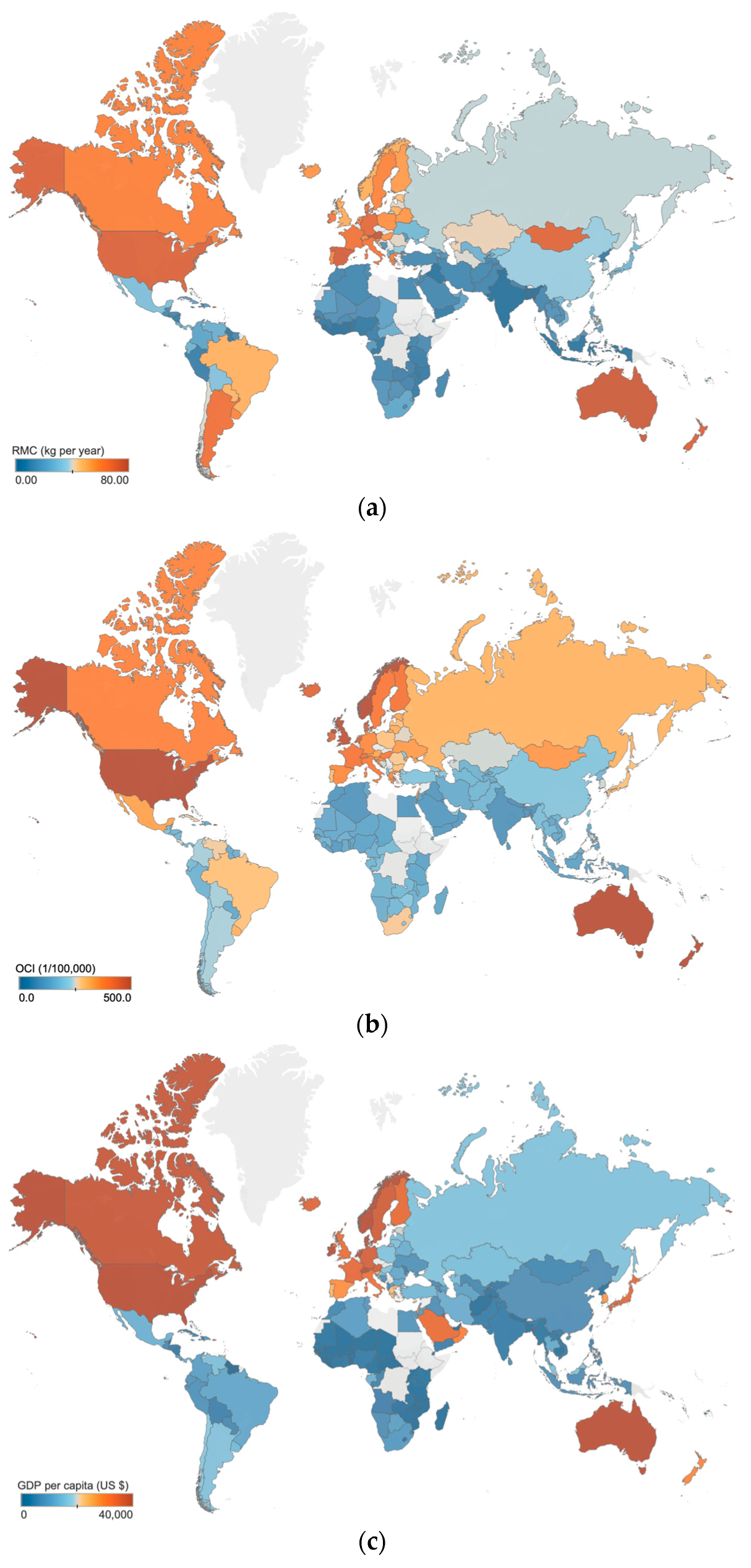
3.2. Effect of Regional Conditions and Customs
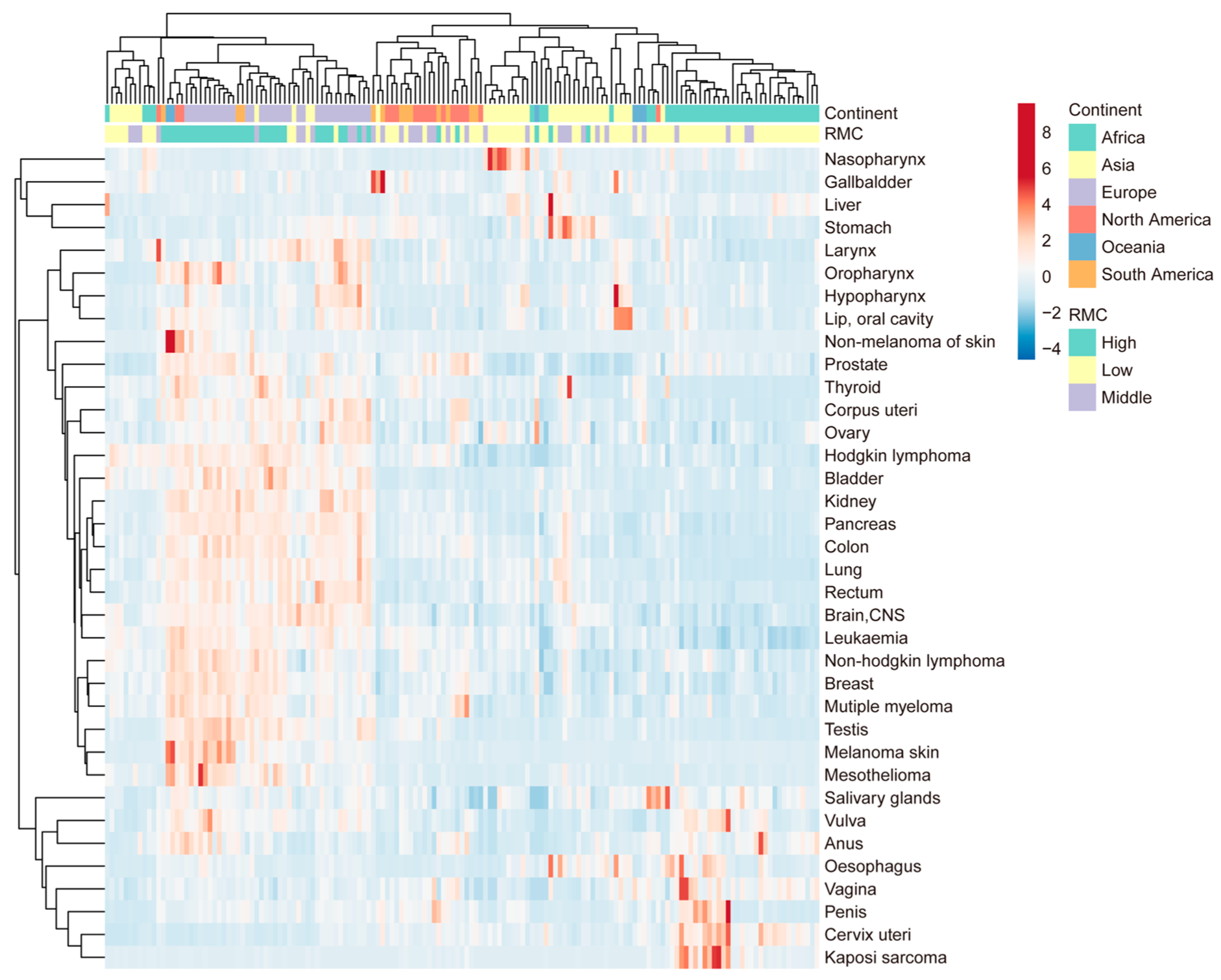
3.2.1. Cluster Analysis of Countries and Regions
3.2.2. Distribution and Partial Correlation Analysis of GDP per Capita
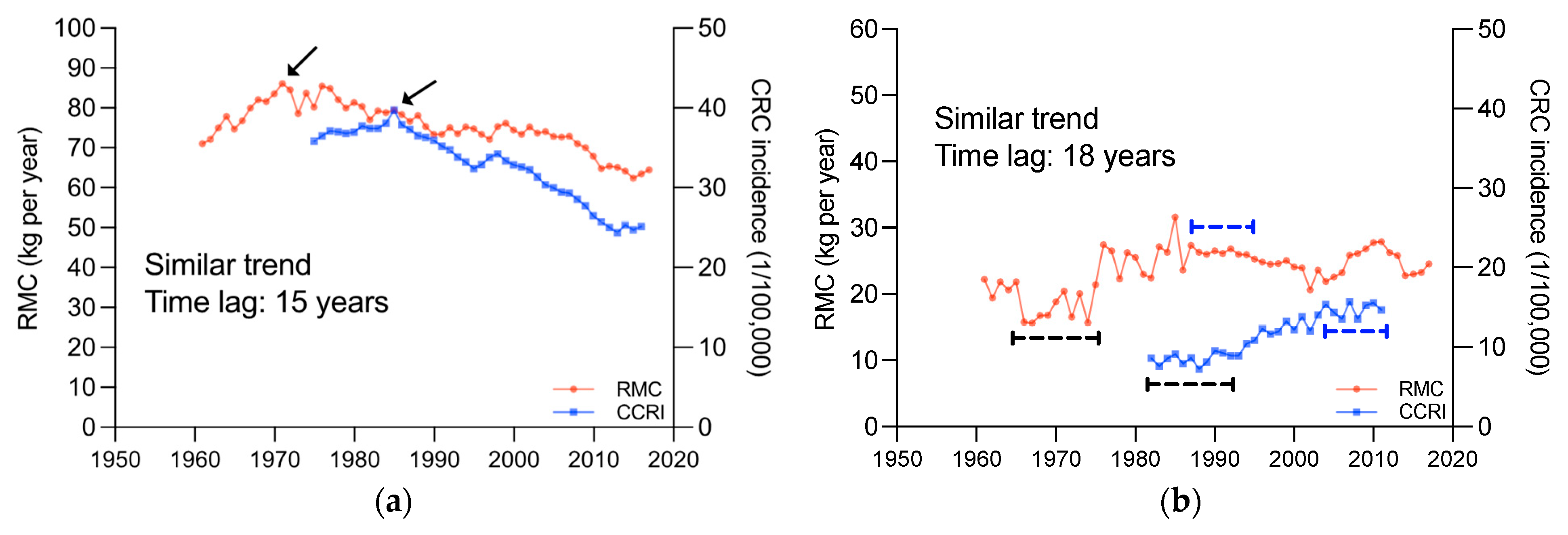
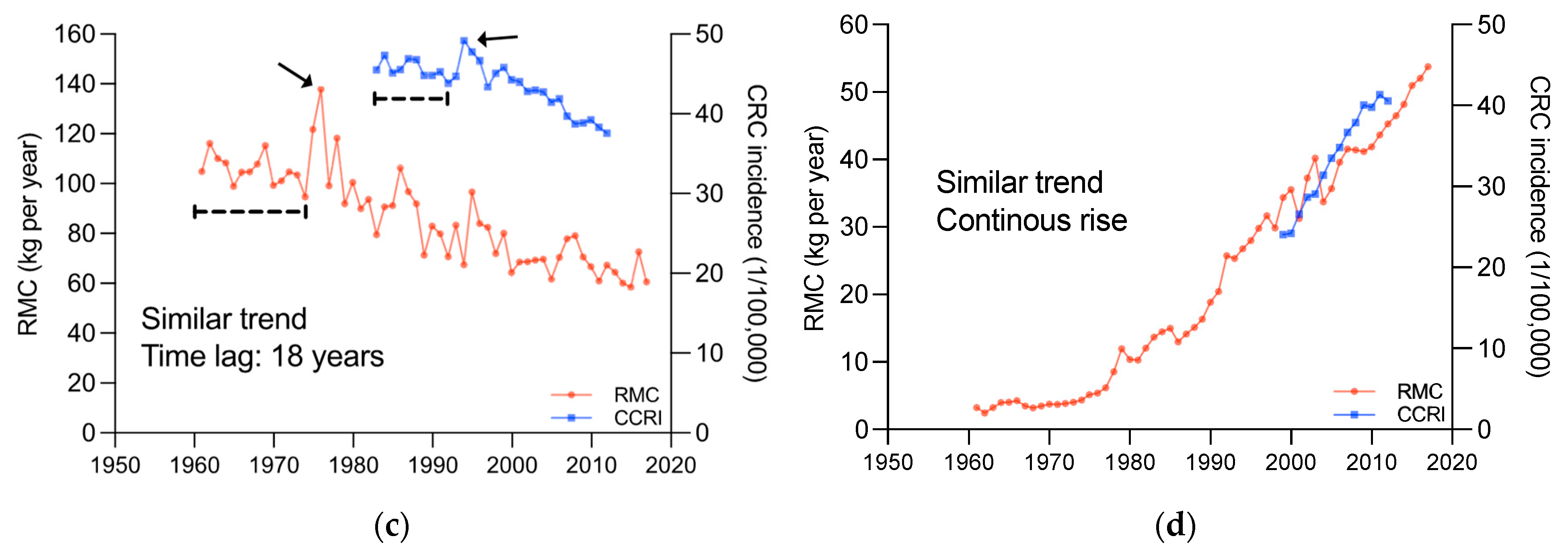
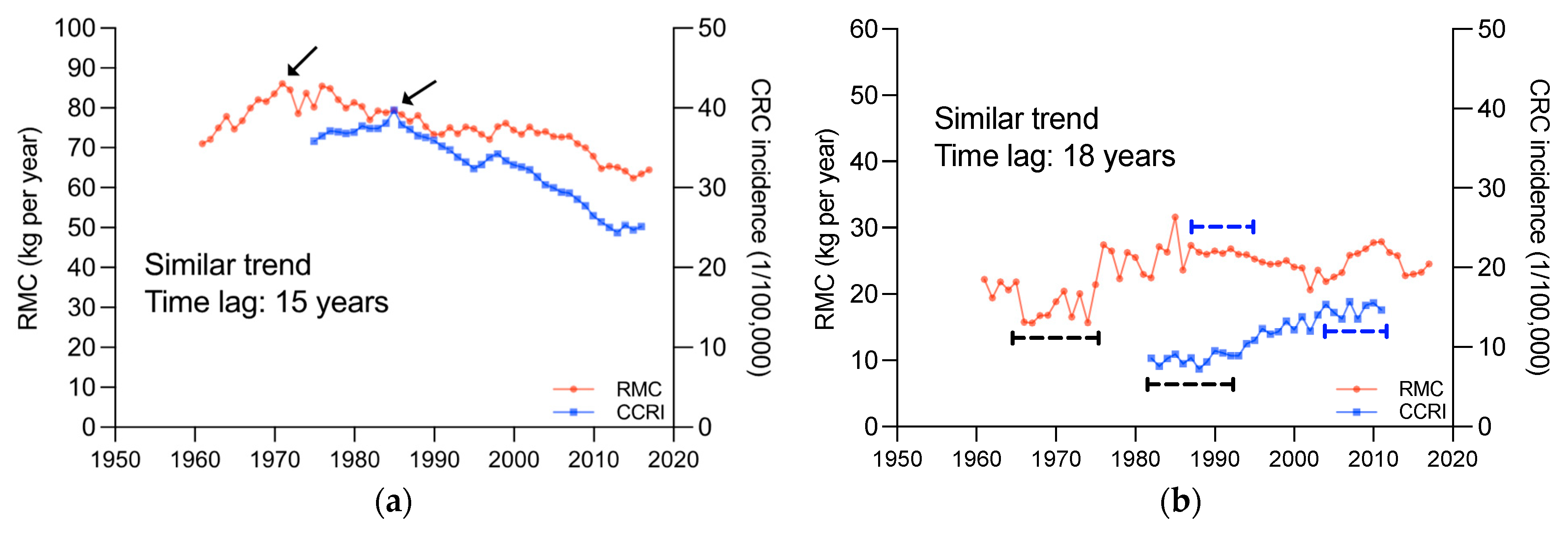
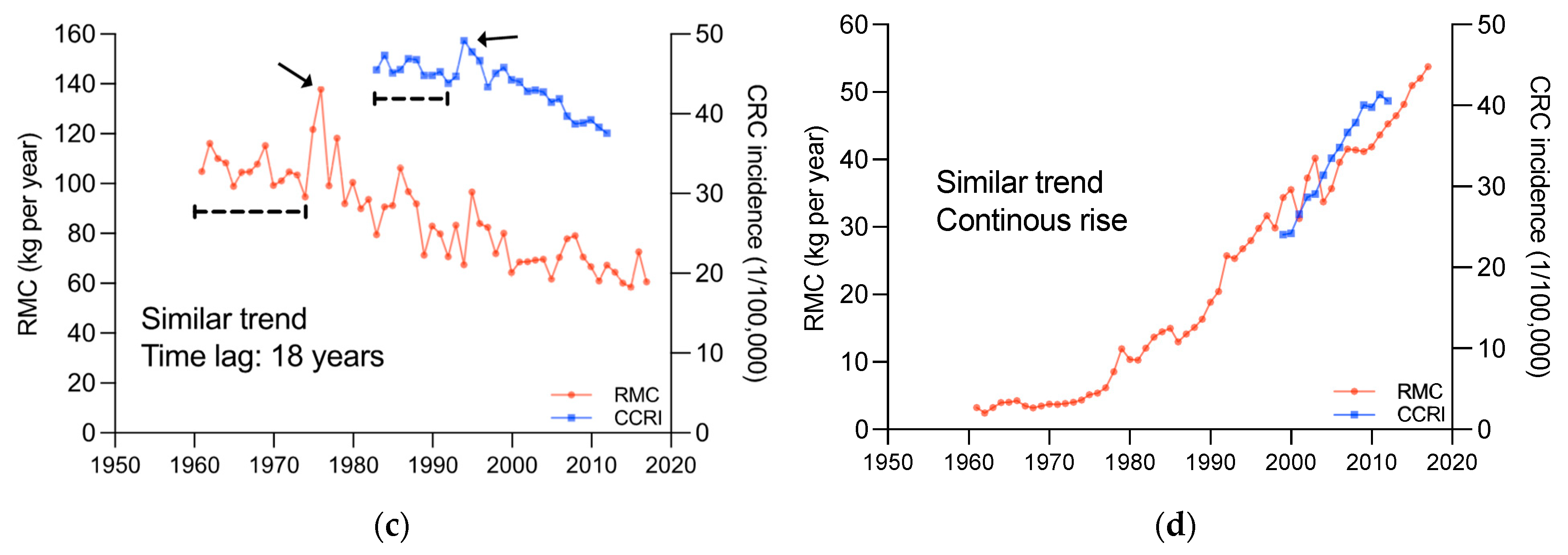
3.3. Lag of RMC’s Influence on CRC Incidence
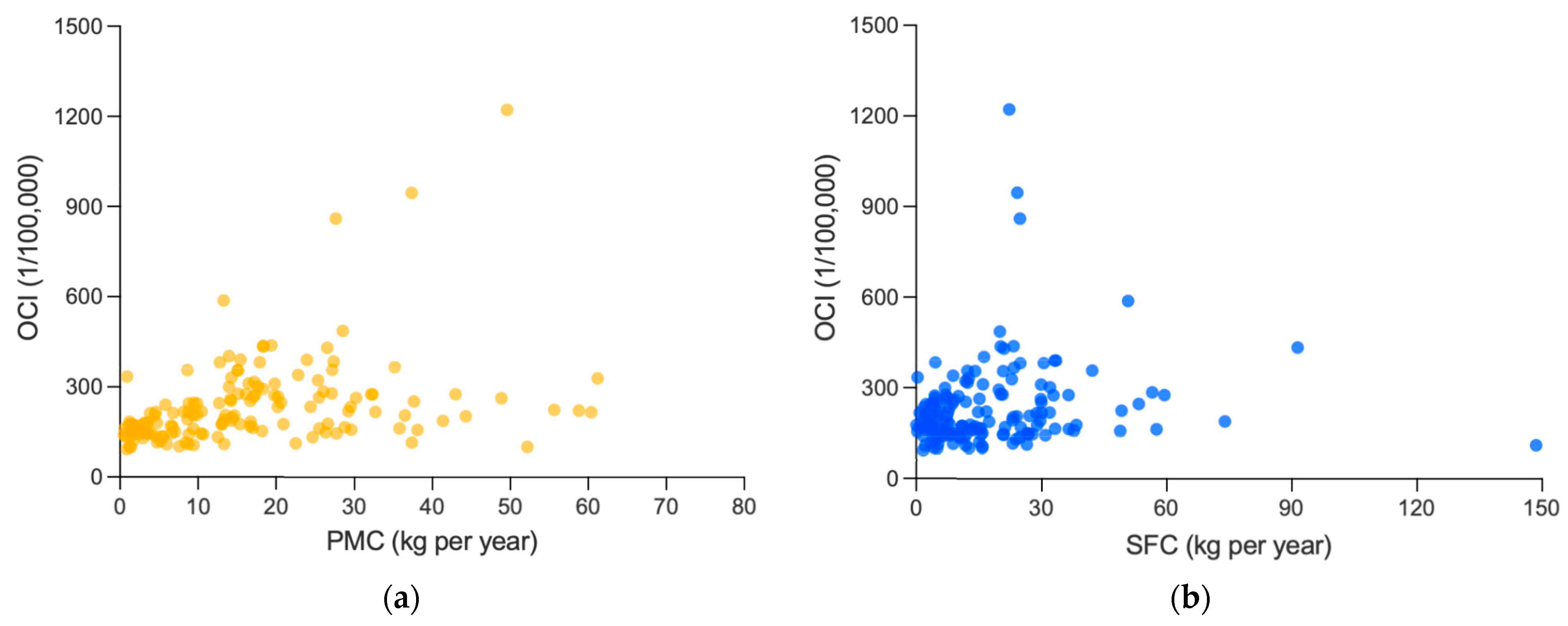
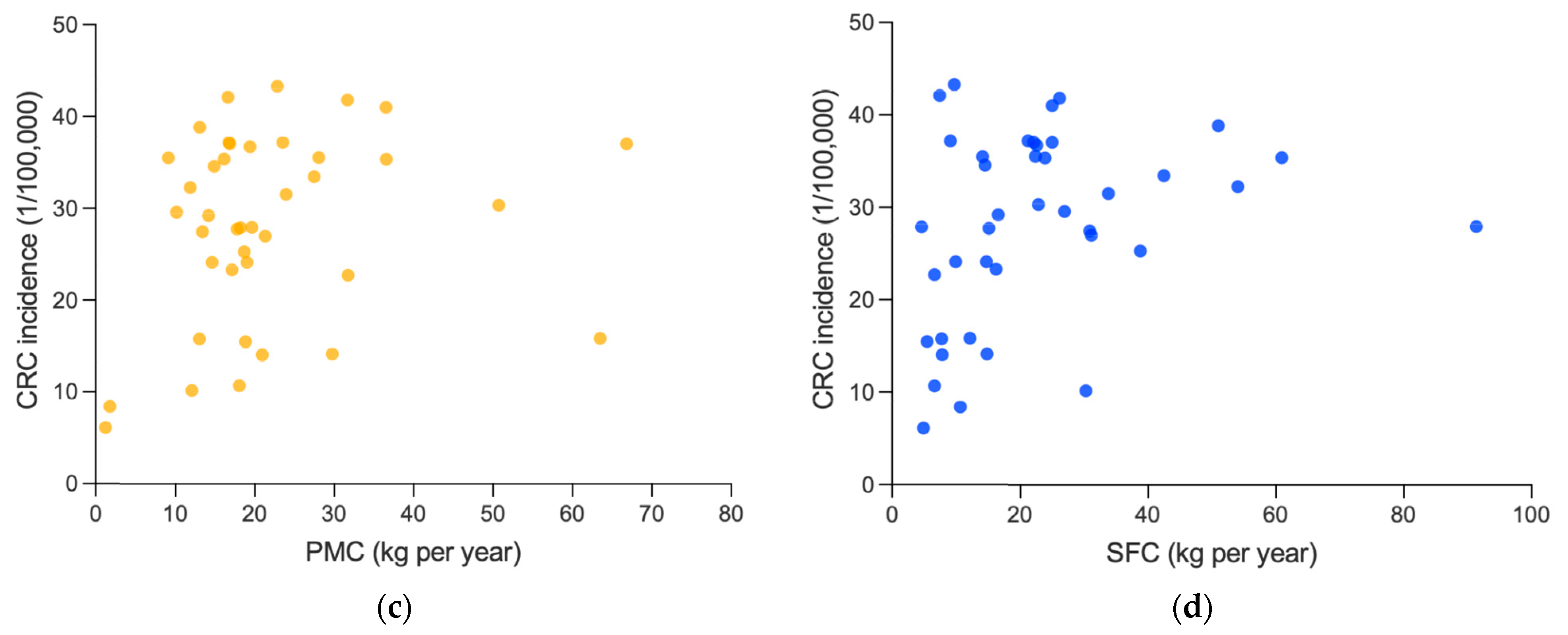
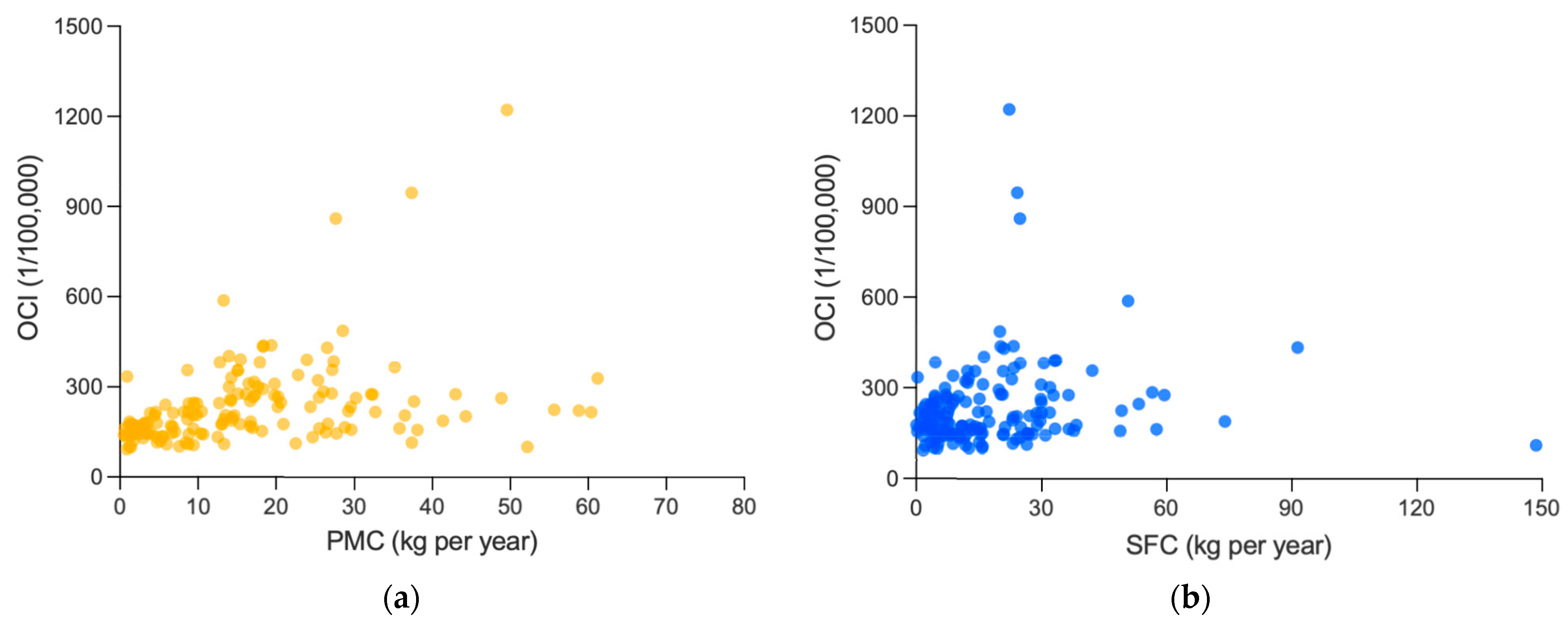
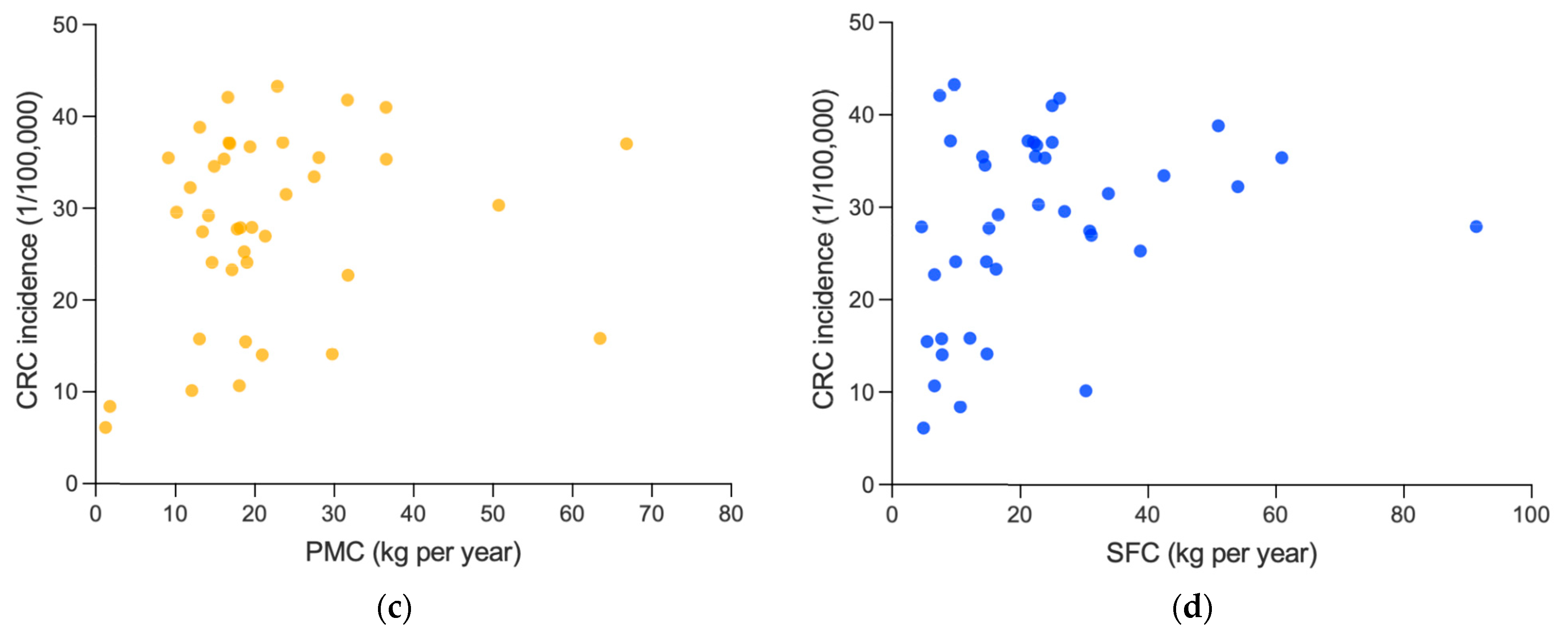
3.4. Association between PMC or SFC and Cancer Incidence
3.5. Analysis of Causality between RMC and Cancer Risk
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| RMC | Red Meat Consumption |
| PMC | Poultry Meat Consumption |
| SFC | Seafood and Fish Consumption |
| OCI | Overall Cancer Incidence |
| CRC | Colorectal Cancer |
| GDP | Gross Domestic Product |
| IARC | International Agency for Research on Cancer |
References
- Godfray, H.C.J.; Aveyard, P.; Garnett, T.; Hall, J.W.; Key, T.J.; Lorimer, J.; Pierrehumbert, R.T.; Scarborough, P.; Springmann, M.; Jebb, S.A. Meat consumption, health, and the environment. Science 2018, 361, eaam5324. [Google Scholar] [CrossRef]
- Oostindjer, M.; Alexander, J.; Amdam, G.V.; Andersen, G.; Bryan, N.S.; Chen, D.; Corpet, D.E.; De Smet, S.; Dragsted, L.O.; Haug, A.; et al. The role of red and processed meat in colorectal cancer development: A perspective. Meat Sci. 2014, 97, 583–596. [Google Scholar] [CrossRef]
- Gonera, A.; Svanes, E.; Bugge, A.B.; Hatlebakk, M.M.; Prexl, K.-M.; Ueland, Ø. Moving Consumers along the Innovation Adoption Curve: A New Approach to Accelerate the Shift toward a More Sustainable Diet. Sustainability 2021, 13, 4477. [Google Scholar] [CrossRef]
- McAfee, A.J.; McSorley, E.M.; Cuskelly, G.J.; Moss, B.W.; Wallace, J.M.; Bonham, M.P.; Fearon, A.M. Red meat consumption: An overview of the risks and benefits. Meat Sci. 2010, 84, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Latvala, T.; Niva, M.; Mäkelä, J.; Pouta, E.; Heikkilä, J.; Kotro, J.; Forsman-Hugg, S. Diversifying meat consumption patterns: Consumers’ self-reported past behaviour and intentions for change. Meat Sci. 2012, 92, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Bouvard, V.; Loomis, D.; Guyton, K.Z.; Grosse, Y.; Ghissassi, F.E.; Benbrahim-Tallaa, L.; Guha, N.; Mattock, H.; Straif, K. Carcinogenicity of consumption of red and processed meat. Lancet Oncol. 2015, 16, 1599–1600. [Google Scholar] [CrossRef] [PubMed]
- Stewart, C.; Piernas, C.; Cook, B.; Jebb, S.A. Trends in UK meat consumption: Analysis of data from years 1–11 (2008-09 to 2018-19) of the National Diet and Nutrition Survey rolling programme. Lancet Planet. Health 2021, 5, e699–e708. [Google Scholar] [CrossRef]
- Williams, P. Nutritional composition of red meat. Nutr. Diet. 2007, 64, S113–S119. [Google Scholar] [CrossRef]
- Zhong, V.W.; Van Horn, L.; Greenland, P.; Carnethon, M.R.; Ning, H.; Wilkins, J.T.; Lloyd-Jones, D.M.; Allen, N.B. Associations of Processed Meat, Unprocessed Red Meat, Poultry, or Fish Intake With Incident Cardiovascular Disease and All-Cause Mortality. JAMA Intern. Med. 2020, 180, 503–512. [Google Scholar] [CrossRef]
- González, N.; Marquès, M.; Nadal, M.; Domingo, J.L. Meat consumption: Which are the current global risks? A review of recent (2010–2020) evidences. Food Res. Int. 2020, 137, 109341. [Google Scholar] [CrossRef]
- Wei, X.; Zhu, C.; Ji, M.; Fan, J.; Xie, J.; Huang, Y.; Jiang, X.; Xu, J.; Yin, R.; Du, L.; et al. Diet and Risk of Incident Lung Cancer: A Large Prospective Cohort Study in UK Biobank. Am. J. Clin. Nutr. 2021, 114, 2043–2051. [Google Scholar] [CrossRef] [PubMed]
- Inoue-Choi, M.; Sinha, R.; Gierach, G.L.; Ward, M.H. Red and processed meat, nitrite, and heme iron intakes and postmenopausal breast cancer risk in the NIH-AARP Diet and Health Study. Int. J. Cancer 2016, 138, 1609–1618. [Google Scholar] [CrossRef]
- Lo, J.J.; Park, Y.M.; Sinha, R.; Sandler, D.P. Association between meat consumption and risk of breast cancer: Findings from the Sister Study. Int. J. Cancer 2020, 146, 2156–2165. [Google Scholar] [CrossRef]
- Bradbury, K.E.; Murphy, N.; Key, T.J. Diet and colorectal cancer in UK Biobank: A prospective study. Int. J. Epidemiol. 2020, 49, 246–258. [Google Scholar] [CrossRef]
- Vieira, A.R.; Abar, L.; Chan, D.S.M.; Vingeliene, S.; Polemiti, E.; Stevens, C.; Greenwood, D.; Norat, T. Foods and beverages and colorectal cancer risk: A systematic review and meta-analysis of cohort studies, an update of the evidence of the WCRF-AICR Continuous Update Project. Ann. Oncol. 2017, 28, 1788–1802. [Google Scholar] [CrossRef] [PubMed]
- Jiang, G.; Li, B.; Liao, X.; Zhong, C. Poultry and fish intake and risk of esophageal cancer: A meta-analysis of observational studies. Asia Pac. J. Clin. Oncol. 2016, 12, e82–e91. [Google Scholar] [CrossRef]
- Wang, F.; Chandler, P.D.; Zeleznik, O.A.; Wu, K.; Wu, Y.; Yin, K.; Song, R.; Avila-Pacheco, J.; Clish, C.B.; Meyerhardt, J.A.; et al. Plasma Metabolite Profiles of Red Meat, Poultry, and Fish Consumption, and Their Associations with Colorectal Cancer Risk. Nutrients 2022, 14, 978. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Su, H.; Wang, B.L.; Zhou, Y.Y.; Guo, L.L. Fish consumption and lung cancer risk: Systematic review and meta-analysis. Nutr. Cancer 2014, 66, 539–549. [Google Scholar] [CrossRef]
- Pham, N.M.; Mizoue, T.; Tanaka, K.; Tsuji, I.; Tamakoshi, A.; Matsuo, K.; Wakai, K.; Nagata, C.; Inoue, M.; Tsugane, S.; et al. Fish consumption and colorectal cancer risk: An evaluation based on a systematic review of epidemiologic evidence among the Japanese population. Jpn. J. Clin. Oncol. 2013, 43, 935–941. [Google Scholar] [CrossRef]
- Nindrea, R.D.; Aryandono, T.; Lazuardi, L.; Dwiprahasto, I. Protective Effect of Omega-3 Fatty Acids in Fish Consumption Against Breast Cancer in Asian Patients: A Meta-Analysis. Asian Pac. J. Cancer Prev. 2019, 20, 327–332. [Google Scholar] [CrossRef] [PubMed]
- McClain, K.M.; Bradshaw, P.T.; Khankari, N.K.; Gammon, M.D.; Olshan, A.F. Fish/shellfish intake and the risk of head and neck cancer. Eur. J. Cancer Prev. 2019, 28, 102–108. [Google Scholar] [CrossRef]
- Alexander, D.D.; Cushing, C.A. Red meat and colorectal cancer: A critical summary of prospective epidemiologic studies. Obes. Rev. 2011, 12, e472–e493. [Google Scholar] [CrossRef]
- Wilunda, C.; Yamaji, T.; Iwasaki, M.; Inoue, M.; Tsugane, S.; Sawada, N. Meat consumption and gastric cancer risk: The Japan Public Health Center-based Prospective Study. Am. J. Clin. Nutr. 2022, 115, 652–661. [Google Scholar] [CrossRef]
- Han, M.A.; Zeraatkar, D.; Guyatt, G.H.; Vernooij, R.W.M.; El Dib, R.; Zhang, Y.; Algarni, A.; Leung, G.; Storman, D.; Valli, C.; et al. Reduction of Red and Processed Meat Intake and Cancer Mortality and Incidence: A Systematic Review and Meta-analysis of Cohort Studies. Ann. Intern. Med. 2019, 171, 711–720. [Google Scholar] [CrossRef]
- Wu, K.; Liu, L.; Shu, T.; Li, A.; Xia, D.; Sun, X. The relationship between processed meat, red meat, and risk of types of cancer: A Mendelian randomization study. Front. Nutr. 2022, 9, 942155. [Google Scholar] [CrossRef]
- Shim, J.S.; Oh, K.; Kim, H.C. Dietary assessment methods in epidemiologic studies. Epidemiol. Health 2014, 36, e2014009. [Google Scholar] [CrossRef]
- Farvid, M.S.; Sidahmed, E.; Spence, N.D.; Mante Angua, K.; Rosner, B.A.; Barnett, J.B. Consumption of red meat and processed meat and cancer incidence: A systematic review and meta-analysis of prospective studies. Eur. J. Epidemiol. 2021, 36, 937–951. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.R.; Kim, K.; Lee, S.A.; Kwon, S.O.; Lee, J.K.; Keum, N.; Park, S.M. Effect of Red, Processed, and White Meat Consumption on the Risk of Gastric Cancer: An Overall and Dose–Response Meta-Analysis. Nutrients 2019, 11, 826. [Google Scholar] [CrossRef] [PubMed]
- Taunk, P.; Hecht, E.; Stolzenberg-Solomon, R. Are meat and heme iron intake associated with pancreatic cancer? Results from the NIH-AARP diet and health cohort. Int. J. Cancer 2016, 138, 2172–2189. [Google Scholar] [CrossRef]
- Smolińska, K.; Paluszkiewicz, P. Risk of colorectal cancer in relation to frequency and total amount of red meat consumption. Systematic review and meta-analysis. Arch. Med. Sci. 2010, 6, 605–610. [Google Scholar] [CrossRef] [PubMed]
- Lescinsky, H.; Afshin, A.; Ashbaugh, C.; Bisignano, C.; Brauer, M.; Ferrara, G.; Hay, S.I.; He, J.; Iannucci, V.; Marczak, L.B.; et al. Health effects associated with consumption of unprocessed red meat: A Burden of Proof study. Nat. Med. 2022, 28, 2075–2082. [Google Scholar] [CrossRef] [PubMed]
- Zheng, P.; Afshin, A.; Biryukov, S.; Bisignano, C.; Brauer, M.; Bryazka, D.; Burkart, K.; Cercy, K.M.; Cornaby, L.; Dai, X.; et al. The Burden of Proof studies: Assessing the evidence of risk. Nat. Med. 2022, 28, 2038–2044. [Google Scholar] [CrossRef] [PubMed]
- Stanaway, J.D.; Afshin, A.; Ashbaugh, C.; Bisignano, C.; Brauer, M.; Ferrara, G.; Garcia, V.; Haile, D.; Hay, S.I.; He, J.; et al. Health effects associated with vegetable consumption: A Burden of Proof study. Nat. Med. 2022, 28, 2066–2074. [Google Scholar] [CrossRef] [PubMed]
- Dai, X.; Gil, G.F.; Reitsma, M.B.; Ahmad, N.S.; Anderson, J.A.; Bisignano, C.; Carr, S.; Feldman, R.; Hay, S.I.; He, J.; et al. Health effects associated with smoking: A Burden of Proof study. Nat. Med. 2022, 28, 2045–2055. [Google Scholar] [CrossRef]
- Razo, C.; Welgan, C.A.; Johnson, C.O.; McLaughlin, S.A.; Iannucci, V.; Rodgers, A.; Wang, N.; LeGrand, K.E.; Sorensen, R.J.D.; He, J.; et al. Effects of elevated systolic blood pressure on ischemic heart disease: A Burden of Proof study. Nat. Med. 2022, 28, 2056–2065. [Google Scholar] [CrossRef]
- Tong, T.Y.N.; Papier, K.; Key, T.J. Meat, vegetables and health—Interpreting the evidence. Nat. Med. 2022, 28, 2001–2002. [Google Scholar] [CrossRef]
- Mutanen, M.; Pajari, A.M.; Oikarinen, S.I. Beef induces and rye bran prevents the formation of intestinal polyps in Apc(Min) mice: Relation to beta-catenin and PKC isozymes. Carcinogenesis 2000, 21, 1167–1173. [Google Scholar] [CrossRef]
- Parnaud, G.; Peiffer, G.; Taché, S.; Corpet, D.E. Effect of meat (beef, chicken, and bacon) on rat colon carcinogenesis. Nutr. Cancer. 1998, 32, 165–173. [Google Scholar] [CrossRef]
- Pierre, F.; Freeman, A.; Taché, S.; Van der Meer, R.; Corpet, D.E. Beef meat and blood sausage promote the formation of azoxymethane-induced mucin-depleted foci and aberrant crypt foci in rat colons. J. Nutr. 2004, 134, 2711–2716. [Google Scholar] [CrossRef] [PubMed]
- Rombouts, C.; Van Meulebroek, L.; De Spiegeleer, M.; Goethals, S.; Van Hecke, T.; De Smet, S.; De Vos, W.H.; Vanhaecke, L. Untargeted Metabolomics Reveals Elevated L-Carnitine Metabolism in Pig and Rat Colon Tissue Following Red Versus White Meat Intake. Mol. Nutr. Food Res. 2021, 65, e2000463. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Belton, B.; Edwards, P.; Henriksson, P.J.G.; Little, D.C.; Newton, R.; Troell, M. Aquaculture will continue to depend more on land than sea. Nature 2022, 603, E2–E4. [Google Scholar] [CrossRef] [PubMed]
- Costello, C.; Cao, L.; Gelcich, S.; Cisneros-Mata, M.; Free, C.M.; Froehlich, H.E.; Golden, C.D.; Ishimura, G.; Maier, J.; Macadam-Somer, I.; et al. The future of food from the sea. Nature 2020, 588, 95–100. [Google Scholar] [CrossRef]
- Geyik, Ö.; Hadjikakou, M.; Bryan, B.A. Climate-friendly and nutrition-sensitive interventions can close the global dietary nutrient gap while reducing GHG emissions. Nat. Food 2023, 4, 61–73. [Google Scholar] [CrossRef]
- Wassénius, E.; Porkka, M.; Nyström, M.; Søgaard Jørgensen, P. A global analysis of potential self-sufficiency and diversity displays diverse supply risks. Global Food Secur. 2023, 37, 100673. [Google Scholar] [CrossRef]
- Diallo, A.; Deschasaux, M.; Latino-Martel, P.; Hercberg, S.; Galan, P.; Fassier, P.; Allès, B.; Guéraud, F.; Pierre, F.H.; Touvier, M. Red and processed meat intake and cancer risk: Results from the prospective NutriNet-Santé cohort study. Int. J. Cancer 2018, 142, 230–237. [Google Scholar] [CrossRef]
- Huang, Y.; Cao, D.; Chen, Z.; Chen, B.; Li, J.; Guo, J.; Dong, Q.; Liu, L.; Wei, Q. Red and processed meat consumption and cancer outcomes: Umbrella review. Food Chem. 2021, 356, 129697. [Google Scholar] [CrossRef]
- Seiwert, N.; Heylmann, D.; Hasselwander, S.; Fahrer, J. Mechanism of colorectal carcinogenesis triggered by heme iron from red meat. Biochim. Biophys. Acta. Rev. Cancer 2020, 1873, 188334. [Google Scholar] [CrossRef]
- Schiller, J.T.; Lowy, D.R. An Introduction to Virus Infections and Human Cancer. Recent Results Cancer Res. 2021, 217, 1–11. [Google Scholar]
- Araldi, R.P.; Sant’Ana, T.A.; Módolo, D.G.; de Melo, T.C.; Spadacci-Morena, D.D.; de Cassia Stocco, R.; Cerutti, J.M.; de Souza, E.B. The human papillomavirus (HPV)-related cancer biology: An overview. Biomed. Pharmacother. 2018, 106, 1537–1556. [Google Scholar] [CrossRef]
- Casas, C.P.R.; Albuquerque, R.C.R.; Loureiro, R.B.; Gollner, A.M.; Freitas, M.G.; Duque, G.; Viscondi, J.Y.K. Cervical cancer screening in low- and middle-income countries: A systematic review of economic evaluation studies. Clinics 2022, 77, 100080. [Google Scholar] [CrossRef]
- Rothman, K.J.; Greenland, S. Causation and causal inference in epidemiology. Am. J. Public Health 2005, 95 (Suppl. S1), S144–S150. [Google Scholar] [CrossRef] [PubMed]
- Ueland, Ø.; Rødbotten, R.; Varela, P. Meat consumption and consumer attitudes—A Norwegian perspective. Meat Sci. 2022, 192, 108920. [Google Scholar] [CrossRef] [PubMed]
- Font, I.F.M.; Guerrero, L. Spanish perspective on meat consumption and consumer attitudes. Meat Sci. 2022, 191, 108874. [Google Scholar] [CrossRef] [PubMed]
- Estévez-Moreno, L.X.; Miranda-de la Lama, G.C. Meat consumption and consumer attitudes in México: Can persistence lead to change? Meat Sci. 2022, 193, 108943. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cancer Type | Correlation Coefficient | p-Value |
|---|---|---|
| Skin melanoma ** | 0.771 | 0.000 |
| Multiple myeloma ** | 0.766 | 0.000 |
| Breast | 0.755 | 0.000 |
| Leukemia ** | 0.712 | 0.000 |
| Prostate | 0.682 | 0.000 |
| Colorectum | 0.625 | 0.000 |
| Testis ** | 0.608 | 0.000 |
| Hodgkin lymphoma ** | 0.562 | 0.000 |
| Non-Hodgkin lymphoma | 0.550 | 0.000 |
| Bladder | 0.525 | 0.001 |
| Kidney | 0.506 | 0.001 |
| Brain, CNS ** | 0.470 | 0.002 |
| Corpus uteri ** | 0.440 | 0.004 |
| Lung | 0.387 | 0.014 |
| Ovary ** | 0.372 | 0.018 |
| Pancreas | 0.361 | 0.022 |
| Oropharynx ** | 0.333 | 0.036 |
| Larynx | 0.147 | 0.364 |
| Oesophagus | 0.147 | 0.367 |
| Kaposi sarcoma | −0.003 | 0.985 |
| Thyroid | 0.019 | 0.908 |
| Gallbladder | −0.115 | 0.479 |
| Liver | −0.143 | 0.379 |
| Uterus | −0.216 | 0.180 |
| Stomach | −0.392 | 0.012 |
| Cervix uteri ** | −0.473 | 0.002 |
| Type | Correlation Coefficient (n = 159/40) | p-Value | Partial-Correlation Coefficient (n = 144/40) | p-Value |
|---|---|---|---|---|
| OCI/RMC | 0.798 | 0.000 | 0.463 | 0.000 |
| OCI/PMC | 0.499 | 0.000 | 0.089 | 0.288 |
| OCI/SFC | 0.213 | 0.007 | −0.055 | 0.514 |
| CRC incidence/RMC | 0.625 | 0.000 | 0.592 | 0.000 |
| CRC incidence/PMC | 0.232 | 0.150 | −0.018 | 0.912 |
| CRC incidence/SFC | 0.330 | 0.038 | 0.081 | 0.625 |
| Countries and Regions | GDP per Capita (US $) | OCI (1/100,000) | RMC (kg/Year) | PMC (kg/Year) | SFC (kg/Year) |
|---|---|---|---|---|---|
| NOR | 63,400.99 | 587.52 | 48.68 | 13.30 | 50.83 |
| KWT | 52,182.33 | 100.45 | 27.39 | 52.25 | 12.69 |
| CHE | 48,385.96 | 402.52 | 56.72 | 13.98 | 16.26 |
| USA | 46,827.12 | 1221.51 | 70.77 | 49.64 | 22.37 |
| IRL | 41,997.98 | 430.41 | 62.03 | 26.58 | 21.06 |
| AUS | 40,018.90 | 945.43 | 75.07 | 37.40 | 24.31 |
| DNK | 39,982.15 | 438.24 | 62.35 | 19.42 | 23.40 |
| NLD | 39,166.50 | 437.71 | 60.06 | 18.38 | 20.28 |
| CAN | 38,243.56 | 365.55 | 59.64 | 35.24 | 23.43 |
| SWE | 36,893.81 | 382.05 | 58.34 | 12.83 | 30.59 |
| DEU | 36,474.24 | 354.93 | 68.56 | 15.13 | 14.16 |
| AUT | 36,453.57 | 316.46 | 76.62 | 17.21 | 12.34 |
| ISL | 34,852.42 | 433.72 | 54.64 | 18.35 | 91.45 |
| JPN | 34,202.50 | 275.94 | 28.22 | 16.14 | 59.50 |
| FRA | 34,012.14 | 390.28 | 64.26 | 23.94 | 33.15 |
| FIN | 33,659.75 | 390.65 | 52.82 | 15.48 | 33.59 |
| SAU | 33,268.51 | 114.91 | 10.78 | 37.43 | 8.85 |
| GBR | 33,105.29 | 486.56 | 48.93 | 28.57 | 20.11 |
| ITA | 32,559.55 | 381.81 | 62.69 | 17.93 | 24.96 |
| TWN | 30,874.74 | 274.60 | 46.16 | 32.41 | 32.90 |
| OMN | 29,910.23 | 111.72 | 21.39 | 22.54 | 26.51 |
| NZL | 28,864.18 | 860.11 | 70.95 | 27.66 | 24.95 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, H.; Qi, X. Red Meat Consumption and Cancer Risk: A Systematic Analysis of Global Data. Foods 2023, 12, 4164. https://doi.org/10.3390/foods12224164
Ma H, Qi X. Red Meat Consumption and Cancer Risk: A Systematic Analysis of Global Data. Foods. 2023; 12(22):4164. https://doi.org/10.3390/foods12224164
Chicago/Turabian StyleMa, Hongyue, and Xiangming Qi. 2023. "Red Meat Consumption and Cancer Risk: A Systematic Analysis of Global Data" Foods 12, no. 22: 4164. https://doi.org/10.3390/foods12224164
APA StyleMa, H., & Qi, X. (2023). Red Meat Consumption and Cancer Risk: A Systematic Analysis of Global Data. Foods, 12(22), 4164. https://doi.org/10.3390/foods12224164