
Quality and Reliability of Halitosis Videos on YouTube as a Source of Information

 , and
, and 
Abstract
:1. Introduction
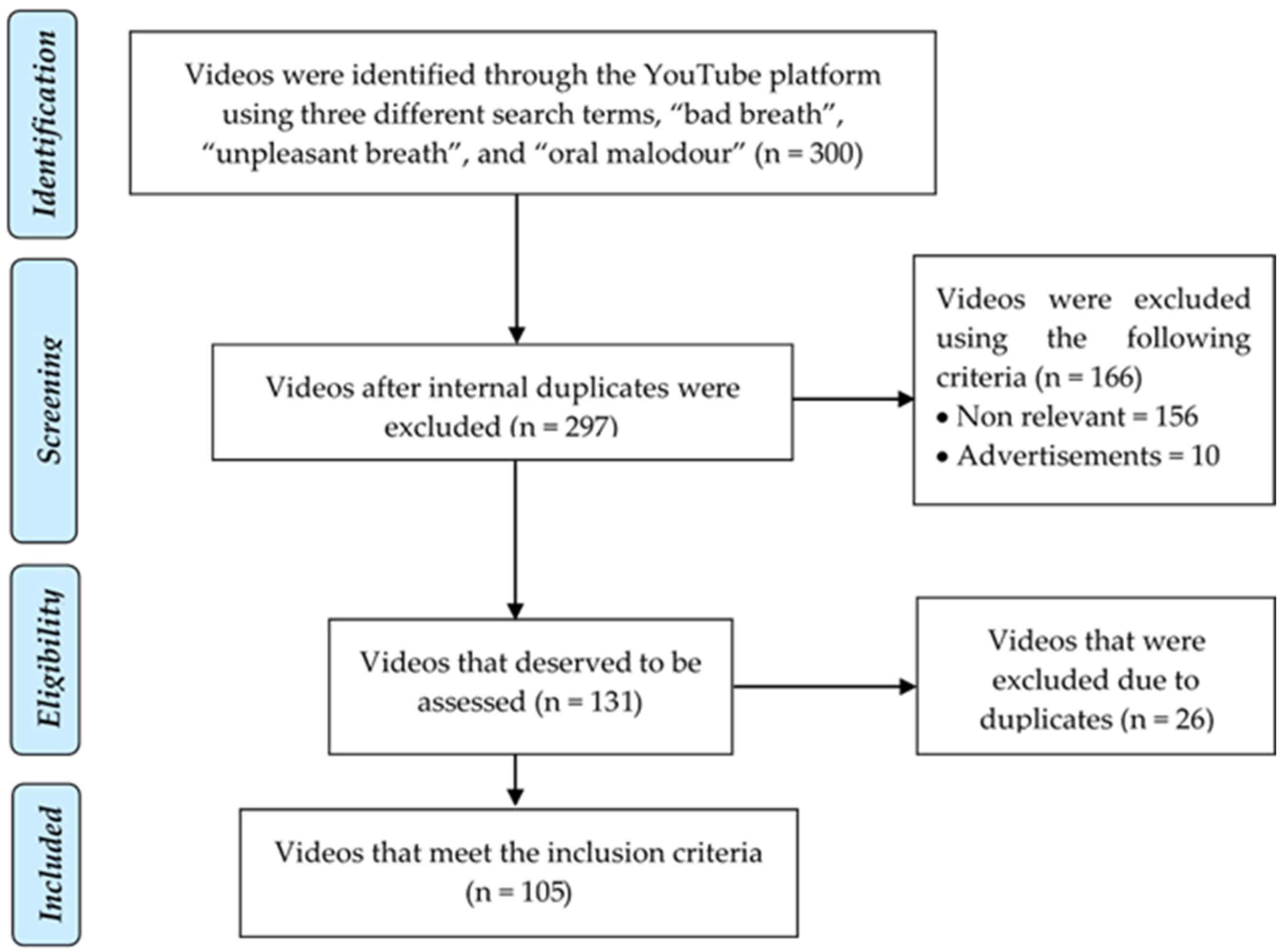
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rani, H.; Ueno, M.; Zaistu, T.; Kawaguchi, Y. Oral malodour among adolescents and its association with health behaviour and oral health status. Int. J. Dent. Hyg. 2016, 14, 135–141. [Google Scholar] [CrossRef]
- Wu, J.; Cannon, R.D.; Ji, P.; Farella, M.; Mei, L. Halitosis: Prevalence, risk factors, sources, measurement, and treatment—A review of the literature. Aust. Dent. J. 2020, 65, 4–11. [Google Scholar] [CrossRef]
- Akaji, E.A.; Folaranmi, N.; Ashiwaju, O. Halitosis: A review of the literature on its prevalence, impact and control. Oral Health Prev. Dent. 2014, 12, 297–304. [Google Scholar]
- Du, M.; Li, L.; Jiang, H.; Zheng, Y.; Zhang, J. Prevalence and relevant factors of halitosis in Chinese subjects: A clinical research. BMC Oral Health. 2019, 19, 45. [Google Scholar] [CrossRef]
- Silva, M.F.; Leite, F.; Ferreira, L.B.; Pola, N.M.; Scannapieco, F.A.; Demarco, F.F.; Nascimento, G.G. Estimated prevalence of halitosis: A systematic review and meta-regression analysis. Clin. Oral Investig. 2018, 22, 47–55. [Google Scholar] [CrossRef]
- Mubayrik, A.B.; Al Hamdan, R.; Al Hadlaq, E.M.; AlBagieh, H.; Al Ahmed, D.; Jaddoh, H.; Demyati, M.; Abu Shryei, R. Self-perception, knowledge, and awareness of halitosis among female university students. Clin. Cosmet. Investig. Dent. 2017, 9, 45–52. [Google Scholar] [CrossRef] [Green Version]
- Tuong, W.; Larsen, E.R.; Armstrong, A.W. Videos to influence: A systematic review of effectiveness of video-based education in modifying health behaviors. J. Behav. Med. 2014, 37, 218–233. [Google Scholar] [CrossRef]
- Uzunoğlu, E.; Kip, S.M. Brand communication through digital influencers: Leveraging blogger engagement. Int. J. Inform. Manag. 2014, 34, 592–602. [Google Scholar] [CrossRef]
- Tan, S.S.; Goonawardene, N. Internet health information seeking and the patient-physician relationship: A systematic review. J. Med. Internet Res. 2017, 19, e9. [Google Scholar] [CrossRef]
- Zhou, L.; Zhang, D.; Yang, C.C.; Wang, Y. Harnessing social media for health information management. Electron. Commer. Res. Appl. 2018, 27, 139–151. [Google Scholar] [CrossRef]
- Ahadzadeh, A.S.; Sharif, S.P.; Ong, F.S.; Khong, K.W. Integrating health belief model and technology acceptance model: An investigation of health-related internet use. J. Med. Internet Res. 2015, 17, e45. [Google Scholar] [CrossRef]
- Maharani, D.A.; El Tantawi, M.; Yoseph, M.G.; Rahardjo, A. The use of internet platforms for oral health information and associated factors among adolescents from Jakarta: A cross sectional study. BMC Oral Health 2021, 21, 22. [Google Scholar] [CrossRef]
- Hassona, Y.; Taimeh, D.; Marahleh, A.; Scully, C. YouTube as a source of information on mouth (oral) cancer. Oral Dis. 2016, 22, 202–208. [Google Scholar] [CrossRef]
- Khan, M.L. Social media engagement: What motivates user participation and consumption on YouTube? Comp. Hum. Behav. 2017, 66, 36–47. [Google Scholar] [CrossRef]
- Madathil, K.C.; Rivera-Rodriguez, A.J.; Greenstein, J.S.; Gramopadhye, A.K. Healthcare information on YouTube: A systematic review. Health Inform. J. 2015, 21, 173–194. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Rössler, B.; Lahner, D.; Schebesta, K.; Chiari, A.; Plöchl, W. Medical information on the intermet: Quality assessment of lumbar puncture and neuroaxial block techniques on YouTube. Clin. Neurol. Neurosurg. 2012, 114, 655–658. [Google Scholar] [CrossRef]
- Kovalski, L.; Cardoso, F.B.; D’Avila, O.P.; Corrêa, A.; Martins, M.; Martins, M.D.; Carrard, V.C. Is the YouTube™ an useful source of information on oral leukoplakia? Oral Dis. 2019, 25, 1897–1905. [Google Scholar] [CrossRef]
- Fortuna, G.; Schiavo, J.H.; Aria, M.; Mignogna, M.D.; Klasser, G.D. The usefulness of YouTube™ videos as a source of information on burning mouth syndrome. J. Oral Rehabil. 2019, 46, 657–665. [Google Scholar] [CrossRef]
- Singh, A.G.; Singh, S.; Singh, P.P. YouTube for information on rheumatoid arthritis—A wakeup call? J. Rheumatol. 2012, 39, 899–903. [Google Scholar] [CrossRef]
- Delli, K.; Livas, C.; Vissink, A.; Spijkervet, F.K. Is YouTube useful as a source of information for Sjögren’s syndrome? Oral Dis. 2016, 22, 196–201. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Zhang, S.; Xiao, Q.; Cao, Y.; Li, B. YouTube™ as a source of information for Candida auris infection: A systematic review. BMC Public Health. 2020, 20, 832. [Google Scholar] [CrossRef]
- Li, M.; Yan, S.; Yang, D.; Li, B.; Cui, W. YouTube™ as a source of information on food poisoning. BMC Public Health 2019, 19, 952. [Google Scholar] [CrossRef]
- Kirkwood, B.R.; Sterne, J.A.C. Essential Medical Statistics, 2nd ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2003. [Google Scholar]
- Ajumobi, A.B.; Malakouti, M.; Bullen, A.; Ahaneku, H.; Lunsford, T.N. YouTube™ as a source of instructional videos on bowel preparation: A content analysis. J. Cancer Educ. 2015, 31, 755–759. [Google Scholar] [CrossRef]
- ElKarmi, R.; Hassona, Y.; Taimeh, D.; Scully, C. YouTube as a source for parents’ education on early childhood caries. Int. J. Paediatr. Dent. 2017, 27, 437–443. [Google Scholar] [CrossRef]
- Nason, K.; Donnelly, A.; Duncan, H.F. YouTube as a patient-information source for root canal treatment. Int. Endod. J. 2016, 49, 1194–1200. [Google Scholar] [CrossRef] [PubMed]
- Jo, J.H.; Kim, E.J.; Kim, J.R.; Kim, M.J.; Chung, J.W.; Park, J.W. Quality and readability of internet-based information on halitosis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 215–222. [Google Scholar] [CrossRef]
- Mueller, S.; Hongler, V.; Jungo, P.; Cajacob, L.; Schwegler, S.; Steveling, E.H.; Manjaly Thomas, Z.R.; Fuchs, O.; Navarini, A.; Scherer, K.; et al. Fiction, falsehoods, and few facts: Cross-sectional study on the content-related quality of atopic eczema-related videos on YouTube. J. Med. Internet Res. 2020, 22, e15599. [Google Scholar] [CrossRef] [Green Version]
- Gokcen, H.B.; Gumussuyu, G. A quality analysis of disc herniation videos on YouTube. World Neurosurg. 2019, 124, e799–e804. [Google Scholar] [CrossRef]
- Brame, C.J. Effective educational videos: Principles and guidelines for maximizing student learning from video content. CBE Life Sci. Educ. 2016, 15, es6. [Google Scholar] [CrossRef] [Green Version]
- Scully, C.; Greenman, J. Halitosis (breath odor). Periodontology 2000 2008, 48, 66–75. [Google Scholar] [CrossRef]

{kind=link}
| Variables | Median (Min–Max) |
|---|---|
| Likes | 21 (1–5255) |
| Dislikes | 0 (0–488) |
| Views | 686 (12–596,755) |
| Duration (mins) | 04:53 (00:51–13:19) |
| Timespan since the video was uploaded (days) | 182 (7–344) |
| Interaction Index | 2.3 (0.1–1596.8) |
| Viewing Rate | 450.7 (5.9–375,317.6) |
| GQS Score | 2 (1–5) |
| Comprehensiveness Score | 4 (1–11) |
| DISCERN Score | 1 (1–5) |
| Global Quality Scale Score | |||
|---|---|---|---|
| Item Scored | n (%) | ||
| The quality and flow of explanation is poor, information is inadequate; pointless information | 5 (4.8%) | ||
| The quality and flow of explanation is low, some information is available but does not include many imperative topics; slightly beneficial information | 48 (45.7%) | ||
| The quality and flow of explanation is moderate, some important information is available but others are poorly discussed; useful information | 21 (20%) | ||
| The quality and flow of explanation is generally good, most of the relevant information is available but some are not covered; helpful information | 18 (17.1%) | ||
| The quality and flow of explanation is exceptional, all relevant information is available; effective information | 13 (12.4%) | ||
| Comprehensiveness Score | |||
| Item scored | Not explained n (%) | Explained briefly n (%) | Explained in detail n (%) |
| Risk Factor | 57 (54.3%) | 22 (21%) | 26 (24.8%) |
| Epidemiology | 104 (99%) | 1 (1%) | 0 (0%) |
| Etiology | 33 (31.4%) | 40 (38.1%) | 32 (30.5%) |
| Classification | 97 (92.4%) | 4 (3.8%) | 4 (3.8%) |
| Diagnosis | 97 (92.4%) | 8 (7.6%) | 0 (0%) |
| Management | 17 (16.2%) | 62 (59%) | 26 (24.8%) |
| Prevention | 6 (5.7%) | 62 (59%) | 37 (35.2%) |
| Total video score | |||
| Video Score | N (%) | ||
| Poor (1–6) | 58 (55.2%) | ||
| Good (7–13) | 39 (37.1%) | ||
| Excellent (14–19) | 8 (7.6%) | ||
| Health Professional (n = 22) | Non-Professional (n = 68) | Education Channel (n = 10) | For-Profit Companies (n = 5) | p-Value | |
|---|---|---|---|---|---|
| Median (Min–Max) | Median (Min–Max) | Median (Min–Max) | Median (Min–Max) | ||
| Likes | 27 (6–383) | 21 (1–5255) | 16 (3–65) | 25 (13–1164) | 0.333 |
| Dislikes | 0 (0–82) | 1 (0–488) | 0 (0–18) | 0 (0–45) | 0.439 |
| Views | 583 (60–56,842) | 982 (12–596,755) | 307 (74–10,463) | 649 (70–26,922) | 0.186 |
| Interaction Index | 5.7 (0.5–21.7) | 1.9 (0.4–32.5) | 5.1 (0.1–12.6) | 1.8 (0.9–1596.8) | 0.062 |
| Viewing Rate | 434 (56.1–35,305.6) | 514.7 (5.9–375,317.6) | 339.3 (36.7–3180.2) | 220 (21.1–11,407.6) | 0.667 |
| GQS score | 5 (3–5) | 2 (1–4) | 4 (2–4) | 2 (1–3) | 0.001 * |
| Comprehensiveness score | 8 (4–11) | 3 (1–7) | 6 (2–8) | 2 (1–5) | 0.001 * |
| Video score | 13 (7–16) | 5 (2–11) | 10 (4–12) | 4 (2–8) | 0.001 * |
| DISCERN score | 4 (3–5) | 1 (1–4) | 3 (1–5) | 1 (1–3) | 0.001 * |
| Poor (n = 58) | Good (n = 39) | Excellent (n = 8) | p-Value | |
|---|---|---|---|---|
| Median (Min–Max) | Median (Min–Max) | Median (Min–Max) | ||
| Likes | 23 (1–5255) | 21 (2–2359) | 19 (13–103) | 0.958 |
| Dislikes | 0 (0–488) | 0 (0–82) | 0 (0–1) | 0.112 |
| Views | 1130 (12–596,755) | 493 (37–73,093) | 437 (175–1.811) | 0.144 |
| Interaction Index | 1.7 (0.4–1596.8) | 3.4 (0.1–25.1) | 7 (0.7–16.8) | 0.029 * |
| Viewing Rate | 613.3 (5.9–375,317.6) | 292.5 (20–35,305.6) | 583.5 (109.2–4100) | 0.688 |
| DISCERN score | 1 (1–2) | 3 (1–5) | 4 (3–5) | 0.001 * |
| DISCERN Score (0–1) (n = 55) | DISCERN Score (2–5) (n = 50) | p-Value | |
|---|---|---|---|
| Median (Min–Max) | Median (Min–Max) | ||
| Likes | 20 (1–5255) | 23 (3–2359) | 0.409 |
| Views | 995 (12–596,755) | 545 (37–73,093) | 0.239 |
| Interaction index | 1.7 (0.4–1596.8) | 3.7 (0.1–28.9) | 0.008 * |
| Viewing rate | 555 (5.9–375,317.6) | 352.3 (20–35,305.6) | 0.691 |
| Less than 4 min (n = 41) | More than 4 min (n = 64) | p-Value | |
|---|---|---|---|
| Median (Min–Max) | Median (Min–Max) | ||
| Views | 968 (59–392,216) | 629 (12–596,755) | 0.377 |
| Viewing rate | 671.5 (36.7–121,054.3) | 358.2 (5.9–375,317.6) | 0.434 |
| Likes | 21 (2–2819) | 21 (1–5255) | 0.480 |
| Interaction index | 1.4 (0.4–32.5) | 2.9 (0.1–1596.8) | 0.012 * |
| GQS Score | 2 (1–4) | 3 (1–5) | 0.046 * |
| Video score | 5 (3–13) | 7 (2–16) | 0.042 * |
| DISCERN score | 1 (1–4) | 2 (1–5) | 0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramadhani, A.; Zettira, Z.; Rachmawati, Y.L.; Hariyani, N.; Maharani, D.A. Quality and Reliability of Halitosis Videos on YouTube as a Source of Information. Dent. J. 2021, 9, 120. https://doi.org/10.3390/dj9100120
Ramadhani A, Zettira Z, Rachmawati YL, Hariyani N, Maharani DA. Quality and Reliability of Halitosis Videos on YouTube as a Source of Information. Dentistry Journal. 2021; 9(10):120. https://doi.org/10.3390/dj9100120
Chicago/Turabian StyleRamadhani, Atik, Zenobia Zettira, Yuanita Lely Rachmawati, Ninuk Hariyani, and Diah Ayu Maharani. 2021. "Quality and Reliability of Halitosis Videos on YouTube as a Source of Information" Dentistry Journal 9, no. 10: 120. https://doi.org/10.3390/dj9100120
APA StyleRamadhani, A., Zettira, Z., Rachmawati, Y. L., Hariyani, N., & Maharani, D. A. (2021). Quality and Reliability of Halitosis Videos on YouTube as a Source of Information. Dentistry Journal, 9(10), 120. https://doi.org/10.3390/dj9100120