
Nonrestorative Management of Dental Caries






Abstract
1. Introduction
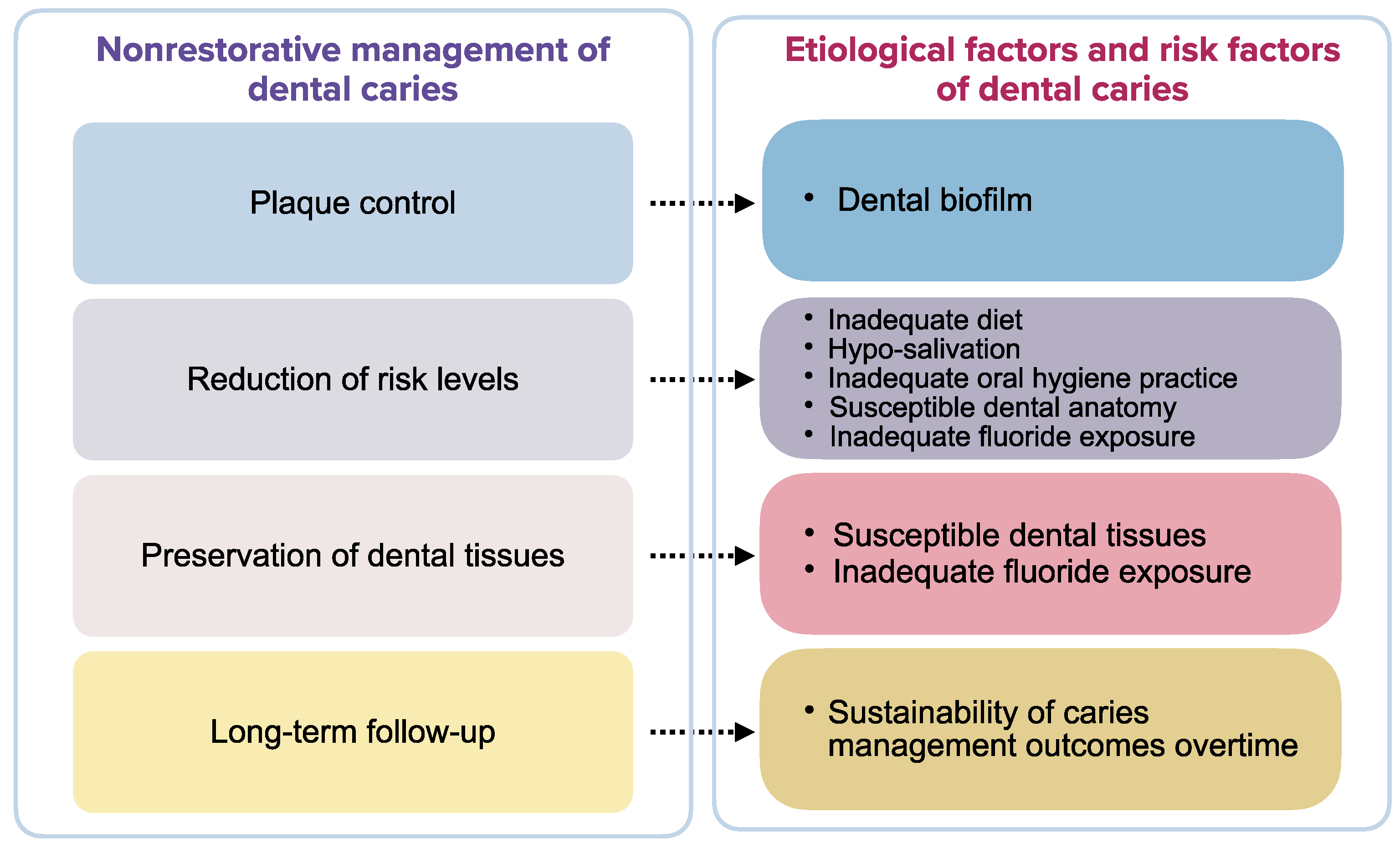
2. The Nonrestorative Management of Dental Caries
2.1. Control of Dental Plaque
2.2. Reduction of Caries Risk
2.3. Preservation of Dental Hard Tissue
2.4. Long-Term Maintenance
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.L.; Marcenes, W. Global Burden of Untreated Caries: A Systematic Review and Metaregression. J. Dent. Res. 2015, 94, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral Diseases: A Global Public Health Challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- López, R.; Smith, P.C.; Göstemeyer, G.; Schwendicke, F. Ageing, Dental Caries and Periodontal Diseases. J. Clin. Periodontol. 2017, 44, S145–S152. [Google Scholar] [CrossRef]
- AlQobaly, L.; Sabbah, W. The Association between Periodontal Disease and Root/Coronal Caries. Int. J. Dent. Hyg. 2020, 18, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Hamdan, A.M.; Maxfield, B.J.; Tüfekçi, E.; Shroff, B.; Lindauer, S.J. Preventing and Treating White-Spot Lesions Associated with Orthodontic Treatment. J. Am. Dent. Assoc. 2012, 143, 777–783. [Google Scholar] [CrossRef] [PubMed]
- Tufekci, E.; Dixon, J.S.; Gunsolley, J.C.; Lindauer, S.J. Prevalence of White Spot Lesions during Orthodontic Treatment with Fixed Appliances. Angle Orthod. 2011, 81, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Richter, A.E.; Arruda, A.O.; Peters, M.C.; Sohn, W. Incidence of Caries Lesions among Patients Treated with Comprehensive Orthodontics. Am. J. Orthod. Dentofac. 2011, 139, 657–664. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Infectious Diseases. Available online: http://www.emro.who.int/health-topics/infectious-diseases/index.html (accessed on 23 June 2021).
- Osborne, J.W.; Summitt, J.B. Extension for Prevention: Is It Relevant Today? Am. J. Dent. 1998, 11, 189–196. [Google Scholar] [PubMed]
- Pitts, N.B.; Zero, D. White Paper on Dental Caries Prevention and Management; FDI World Dental Federation: Geneva, Switzerland, 2016; pp. 3–9. [Google Scholar]
- Sunnegårdh-Grönberg, K.; van Dijken, J.W.V.; Funegård, U.; Lindberg, A.; Nilsson, M. Selection of Dental Materials and Longevity of Replaced Restorations in Public Dental Health Clinics in Northern Sweden. J. Dent. 2009, 37, 673–678. [Google Scholar] [CrossRef]
- Moraschini, V.; Fai, C.K.; Alto, R.M.; Santos, G.O. Amalgam and Resin Composite Longevity of Posterior Restorations: A Systematic Review and Meta-Analysis. J. Dent. 2015, 43, 1043–1050. [Google Scholar] [CrossRef]
- Opdam, N.J.M.; van de Sande, F.H.; Bronkhorst, E.; Cenci, M.S.; Bottenberg, P.; Pallesen, U.; Gaengler, P.; Lindberg, A.; Huysmans, M.C.D.N.J.M.; Dijken, J.W. Longevity of Posterior Composite Restorations. J. Dent. Res. 2014, 93, 943–949. [Google Scholar] [CrossRef]
- Frencken, J.E.; Peters, M.C.; Manton, D.J.; Leal, S.C.; Gordan, V.V.; Eden, E. Minimal Intervention Dentistry for Managing Dental Caries—A Review: Report of a FDI Task Group. Int. Dent. J. 2012, 62, 223–243. [Google Scholar] [CrossRef] [PubMed]
- Marsh, P.D. Are Dental Diseases Examples of Ecological Catastrophes? Microbiology 2003, 149, 279–294. [Google Scholar] [CrossRef] [PubMed]
- Marsh, P.D.; Head, D.A.; Devine, D.A. Ecological Approaches to Oral Biofilms: Control without Killing. Caries Res. 2015, 49, 46–54. [Google Scholar] [CrossRef]
- Machiulskiene, V.; Campus, G.; Carvalho, J.C.; Dige, I.; Ekstrand, K.R.; Jablonski-Momeni, A.; Maltz, M.; Manton, D.J.; Martignon, S.; Martinez-Mier, E.A.; et al. Terminology of Dental Caries and Dental Caries Management: Consensus Report of a Workshop Organized by ORCA and Cariology Research Group of IADR. Caries Res. 2020, 54, 7–14. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Noncommunicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 23 June 2021).
- Selwitz, R.H.; Ismail, A.I.; Pitts, N.B. Dental Caries. Lancet 2007, 369, 51–59. [Google Scholar] [CrossRef]
- Featherstone, J.D.B.; Chaffee, B.W. The Evidence for Caries Management by Risk Assessment (CAMBRA®). Adv. Dent. Res. 2018, 29, 9–14. [Google Scholar] [CrossRef]
- Kwan, S.Y.L.; Petersen, P.E.; Pine, C.M.; Borutta, A. Health-Promoting Schools: An Opportunity for Oral Health Promotion. Bull. World Health Organ. 2005, 83, 677–685. [Google Scholar]
- Stein, C.; Santos, N.M.L.; Hilgert, J.B.; Hugo, F.N. Effectiveness of Oral Health Education on Oral Hygiene and Dental Caries in Schoolchildren: Systematic Review and Meta-analysis. Community Dent. Oral Epidemiol. 2018, 46, 30–37. [Google Scholar] [CrossRef]
- Wu, L.; Gao, X.; Lo, E.C.M.; Ho, S.M.Y.; McGrath, C.; Wong, M.C.M. Motivational Interviewing to Promote Oral Health in Adolescents. J. Adolescent Health 2017, 61, 378–384. [Google Scholar] [CrossRef]
- Werner, H.; Hakeberg, M.; Dahlström, L.; Eriksson, M.; Sjögren, P.; Strandell, A.; Svanberg, T.; Svensson, L.; Boman, U.W. Psychological Interventions for Poor Oral Health. J. Dent. Res. 2016, 95, 506–514. [Google Scholar] [CrossRef]
- Pine, C.M.; Adair, P.M.; Burnside, G.; Brennan, L.; Sutton, L.; Edwards, R.T.; Ezeofor, V.; Albadri, S.; Curnow, M.M.; Deery, C.; et al. Dental RECUR Randomized Trial to Prevent Caries Recurrence in Children. J. Dent. Res. 2020, 99, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Colvara, B.C.; Faustino-Silva, D.D.; Meyer, E.; Hugo, F.N.; Celeste, R.K.; Hilgert, J.B. Motivational Interviewing for Preventing Early Childhood Caries: A Systematic Review and Meta-analysis. Community Dent. Oral Epidemiol. 2021, 49, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Poklepovic, T.; Worthington, H.V.; Johnson, T.M.; Sambunjak, D.; Imai, P.; Clarkson, J.E.; Tugwell, P. Interdental Brushing for the Prevention and Control of Periodontal Diseases and Dental Caries in Adults. Cochrane Database Syst. Rev. 2013, 12, 1–8. [Google Scholar] [CrossRef]
- American Dental Association. Toothbrushes. Available online: https://www.ada.org/en/member-center/oral-health-topics/toothbrushes (accessed on 4 September 2021).
- Yaacob, M.; Worthington, H.V.; Deacon, S.A.; Deery, C.; Walmsley, A.D.; Robinson, P.G.; Glenny, A. Powered versus Manual Toothbrushing for Oral Health. Cochrane Database Syst. Rev. 2014, 6, 1–60. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Tadakamadla, J.; Johnson, N.W. Effect of Toothbrushing Frequency on Incidence and Increment of Dental Caries. J. Dent. Res. 2016, 95, 1230–1236. [Google Scholar] [CrossRef]
- Worthington, H.V.; MacDonald, L.; Pericic, T.P.; Sambunjak, D.; Johnson, T.M.; Imai, P.; Clarkson, J.E. Home Use of Interdental Cleaning Devices, in Addition to Toothbrushing, for Preventing and Controlling Periodontal Diseases and Dental Caries. Cochrane Database Syst. Rev. 2019, 4, 1–162. [Google Scholar] [CrossRef]
- Gilbert, P.; Moore, L.E. Cationic Antiseptics: Diversity of Action under a Common Epithet. J. Appl. Microbiol. 2005, 99, 703–715. [Google Scholar] [CrossRef]
- Walsh, T.; Oliveira-Neto, J.M.; Moore, D. Chlorhexidine Treatment for the Prevention of Dental Caries in Children and Adolescents. Cochrane Database Syst. Rev. 2015, 4, 1–12. [Google Scholar] [CrossRef]
- Brookes, Z.L.S.; Bescos, R.; Belfield, L.A.; Ali, K.; Roberts, A. Current Uses of Chlorhexidine for Management of Oral Disease: A Narrative Review. J. Dent. 2020, 103, 103497. [Google Scholar] [CrossRef]
- Slayton, R.L.; Urquhart, O.; Araujo, M.W.B.; Fontana, M.; Guzmán-Armstrong, S.; Nascimento, M.M.; Nový, B.B.; Tinanoff, N.; Weyant, R.J.; Wolff, M.S.; et al. Evidence-Based Clinical Practice Guideline on Nonrestorative Treatments for Carious Lesions A Report from the American Dental Association. J. Am. Dent. Assoc. 2018, 149, 837–849. [Google Scholar] [CrossRef]
- Kanagalingam, J.; Feliciano, R.; Hah, J.H.; Labib, H.; Le, T.A.; Lin, J.C. Practical Use of Povidone-iodine Antiseptic in the Maintenance of Oral Health and in the Prevention and Treatment of Common Oropharyngeal Infections. Int. J. Clin Pract. 2015, 69, 1247–1256. [Google Scholar] [CrossRef]
- Milgrom, P.; Tut, O.; Rothen, M.; Mancl, L.; Gallen, M.; Tanzer, J.M. Addition of Povidone-Iodine to Fluoride Varnish for Dental Caries: A Randomized Clinical Trial. JDR Clin. Transl. Res. 2021, 6, 195–204. [Google Scholar] [CrossRef]
- Milgrom, P.; Zero, D.T.; Tanzer, J.M. An Examination of the Advances in Science and Technology of Prevention of Tooth Decay in Young Children since the Surgeon General’s Report on Oral Health. Acad. Pediatr. 2009, 9, 404–409. [Google Scholar] [CrossRef][Green Version]
- Gao, S.S.; Zhao, I.S.; Duffin, S.; Duangthip, D.; Lo, E.C.M.; Chu, C.H. Revitalising Silver Nitrate for Caries Management. Int. J. Environ. Res. Public Health 2018, 15, 80. [Google Scholar] [CrossRef]
- Yu, O.Y.; Zhao, I.S.; Mei, M.L.; Lo, E.C.M.; Chu, C.H. Effect of Silver Nitrate and Sodium Fluoride with Tri-Calcium Phosphate on Streptococcus Mutans and Demineralised Dentine. Int. J. Mol Sci. 2018, 19, 1288. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.S.; Chen, K.J.; Duangthip, D.; Wong, M.C.M.; Lo, E.C.M.; Chu, C.H. Arresting Early Childhood Caries Using Silver and Fluoride Products—A Randomised Trial. J. Dent. 2020, 103, 103–110. [Google Scholar] [CrossRef]
- Riley, P.; Moore, D.; Ahmed, F.; Sharif, M.O.; Worthington, H.V. Xylitol-containing Products for Preventing Dental Caries in Children and Adults. Cochrane Database Syst Rev. 2015, 3, 1–52. [Google Scholar] [CrossRef] [PubMed]
- Loveren, C. van Sugar Alcohols: What Is the Evidence for Caries-Preventive and Caries-Therapeutic Effects? Caries Res. 2004, 38, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Dowd, F.J. Saliva and Dental Caries. Dent. Clin. N. Am. 1999, 43, 579–597. [Google Scholar]
- Janket, S.J.; Benwait, J.; Isaac, P.; Ackerson, L.K.; Meurman, J.H. Oral and Systemic Effects of Xylitol Consumption. Caries Res. 2019, 53, 491–501. [Google Scholar] [CrossRef]
- Huang, X.; Exterkate, R.A.M.; Cate, J.M. ten Factors Associated with Alkali Production from Arginine in Dental Biofilms. J. Dent. Res. 2012, 91, 1130–1134. [Google Scholar] [CrossRef]
- Bijle, M.N.; Ekambaram, M.; Yiu, C.K.Y. A Scoping Review on Arginine in Caries Prevention. J. Évid. Based Dent. Pract. 2020, 20, 101–118. [Google Scholar] [CrossRef]
- Wolff, M.S.; Schenkel, A.B. The Anticaries Efficacy of a 1.5% Arginine and Fluoride Toothpaste. Adv. Dent. Res. 2018, 29, 93–97. [Google Scholar] [CrossRef]
- Cicciù, M.; Fiorillo, L.; Cervino, G. Chitosan Use in Dentistry: A Systematic Review of Recent Clinical Studies. Mar. Drugs. 2019, 17, 417. [Google Scholar] [CrossRef] [PubMed]
- Gruner, D.; Paris, S.; Schwendicke, F. Probiotics for Managing Caries and Periodontitis: Systematic Review and Meta-Analysis. J. Dent. 2016, 48, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Afennich, F.; Slot, D.; Hossainian, N.; Weijden, G.V. The Effect of Hexetidine Mouthwash on the Prevention of Plaque and Gingival Inflammation: A Systematic Review. Int. J. Dent. Hyg. 2011, 9, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Featherstone, J.D.B. The Caries Balance: Contributing Factors and Early Detection. J. Calif. Dent. Assoc. 2003, 31, 129–133. [Google Scholar]
- Featherstone, J.D.B. The Caries Balance: The Basis for Caries Management by Risk Assessment. Oral Health Prev. Dent. 2004, 2 Suppl 1, 259–264. [Google Scholar]
- Young, D.A.; Featherstone, J.D.B. Caries Management by Risk Assessment. Community Dent. Oral Epidemiol. 2013, 41, e53–e63. [Google Scholar] [CrossRef]
- Ismail, A.I.; Pitts, N.B.; Tellez, M. The International Caries Classification and Management System (ICCMSTM) An Example of a Caries Management Pathway. BMC Oral Health 2015, 15, 1–13. [Google Scholar] [CrossRef]
- Bratthall, D.; Petersson, G.H. Cariogram—A Multifactorial Risk Assessment Model for a Multifactorial Disease. Community Dent. Oral Epidemiol. 2005, 33, 256–264. [Google Scholar] [CrossRef]
- American Academy of Pediatric Dentistry. Caries-Risk Assessment and Management for Infants, Children, and Adolescents. Pediatr. Dent. 2020, 40, 220–224. [Google Scholar]
- Pitts, N.B.; Ismail, A.I.; Martignon, S.; Ekstrand, K.; Douglas, G.V.; Longbottom, C.; Deery, C.; Ellwood, R.; Gomez, J.; Kolker, J.; et al. ICCMSTM Guide for Practitioners and Educators. ICCMSTM Caries Manag. 2014, 1–84. [Google Scholar]
- World Health Organization. Guideline: Sugars Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2015; ISBN 9241549025. [Google Scholar]
- Moynihan, P.J.; Kelly, S.A.M. Effect on Caries of Restricting Sugars Intake. J. Dent. Res. 2013, 93, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Moynihan, P.; Makino, Y.; Petersen, P.E.; Ogawa, H. Implications of WHO Guideline on Sugars for Dental Health Professionals. Community Dent. Oral Epidemiol. 2018, 46, 1–7. [Google Scholar] [CrossRef]
- Ahovuo-Saloranta, A.; Forss, H.; Walsh, T.; Nordblad, A.; Mäkelä, M.; Worthington, H.V. Pit and Fissure Sealants for Preventing Dental Decay in Permanent Teeth. Cochrane Database Syst. Rev. 2017, 7, 1–143. [Google Scholar] [CrossRef]
- Fontana, M.; Platt, J.A.; Eckert, G.J.; Gonzalez-Cabezas, C.; Yoder, K.; Zero, D.T.; Ando, M.; Soto-Rojas, A.E.; Peters, M.C. Monitoring of Sound and Carious Surfaces under Sealants over 44 Months. J. Dent. Res. 2014, 93, 1070–1075. [Google Scholar] [CrossRef]
- Fontana, M.; Innes, N. Sealing Carious Tissue Using Resin and Glass-Ionomer Cements. Monogr. Oral Sci. 2018, 27, 103–112. [Google Scholar] [CrossRef]
- Kühnisch, J.; Bedir, A.; Lo, Y.-F.; Kessler, A.; Lang, T.; Mansmann, U.; Heinrich-Weltzien, R.; Hickel, R. Meta-Analysis of the Longevity of Commonly Used Pit and Fissure Sealant Materials. Dent. Mater. 2020, 36, e158–e168. [Google Scholar] [CrossRef]
- Urquhart, O.; Tampi, M.P.; Pilcher, L.; Slayton, R.L.; Araujo, M.W.B.; Fontana, M.; Guzmán-Armstrong, S.; Nascimento, M.M.; Nový, B.B.; Tinanoff, N.; et al. Nonrestorative Treatments for Caries: Systematic Review and Network Meta-Analysis. J. Dent. Res. 2019, 98, 14–26. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, A.; Splieth, C.; Breschi, L.; Fontana, M.; Paris, S.; Burrow, M.; Crombie, F.; Page, L.F.; Gatón-Hernández, P.; Giacaman, R.A.; et al. When to Intervene in the Caries Process? A Delphi Consensus Statement. Br. Dent. J. 2020, 229, 474–482. [Google Scholar] [CrossRef] [PubMed]
- Schwendicke, F.; Frencken, J.E.; Bjørndal, L.; Maltz, M.; Manton, D.J.; Ricketts, D.; Landuyt, K.V.; Banerjee, A.; Campus, G.; Doméjean, S.; et al. Managing Carious Lesions: Consensus Recommendations on Carious Tissue Removal. Adv. Dent. Res. 2016, 28, 58–67. [Google Scholar] [CrossRef]
- Schwendicke, F.; Splieth, C.; Breschi, L.; Banerjee, A.; Fontana, M.; Paris, S.; Burrow, M.F.; Crombie, F.; Page, L.F.; Gatón-Hernández, P.; et al. When to Intervene in the Caries Process? An Expert Delphi Consensus Statement. Clin. Oral Investig. 2019, 23, 3691–3703. [Google Scholar] [CrossRef]
- Chu, C.H.; Mei, M.L.; Lo, E.C.M. Use of Fluorides in Dental Caries Management. Gen. Dent. 2010, 58, 37–43. [Google Scholar]
- Marinho, V.C.C.; Chong, L.Y.; Worthington, H.V.; Walsh, T. Fluoride Mouthrinses for Preventing Dental Caries in Children and Adolescents. Cochrane Database Syst. Rev. 2016, 7, 1–117. [Google Scholar] [CrossRef]
- Marinho, V.C.; Higgins, J.P.; Sheiham, A.; Logan, S. Fluoride Toothpastes for Preventing Dental Caries in Children and Adolescents. Cochrane Database Syst. Rev. 2003, 2, 1–93. [Google Scholar] [CrossRef]
- Marinho, V.C.C.; Worthington, H.V.; Walsh, T.; Chong, L.Y. Fluoride Gels for Preventing Dental Caries in Children and Adolescents. Cochrane Database Syst. Rev. 2015, 13, 1–96. [Google Scholar] [CrossRef]
- Marinho, V.C.C.; Worthington, H.V.; Walsh, T.; Clarkson, J.E. Fluoride Varnishes for Preventing Dental Caries in Children and Adolescents. Cochrane Database Syst. Rev. 2013, 40, 1–78. [Google Scholar] [CrossRef] [PubMed]
- Yu, O.Y.; Zhao, I.S.; Mei, M.L.; Lo, E.C.M.; Chu, C.H. Caries-Arresting Effects of Silver Diamine Fluoride and Sodium Fluoride on Dentine Caries Lesions. J. Dent. 2018, 78, 65–71. [Google Scholar] [CrossRef]
- Yu, O.Y.; Mei, M.L.; Zhao, I.S.; Li, Q.L.; Lo, E.C.M.; Chu, C.H. Remineralisation of Enamel with Silver Diamine Fluoride and Sodium Fluoride. Dent. Mater. 2018, 34, e344–e352. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.S.; Zhang, S.; Mei, M.L.; Lo, E.C.M.; Chu, C.H. Caries Remineralisation and Arresting Effect in Children by Professionally Applied Fluoride Treatment—A Systematic Review. BMC Oral Health 2016, 16, 12–21. [Google Scholar] [CrossRef]
- Seifo, N.; Cassie, H.; Radford, J.R.; Innes, N.P.T. Silver Diamine Fluoride for Managing Carious Lesions: An Umbrella Review. BMC Oral Health 2019, 19, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, B.H.; Rajendra, A.; Veitz-Keenan, A.; Niederman, R. The Effect of Silver Diamine Fluoride in Preventing Caries in the Primary Dentition: A Systematic Review and Meta-Analysis. Caries Res. 2018, 53, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Bijle, M.N.A.; Yiu, C.K.Y.; Ekambaram, M. Calcium-Based Caries Preventive Agents: A Meta-Evaluation of Systematic Reviews and Meta-Analysis. J. Evid. Based Dent. Pract. 2018, 18, 203–217. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.J.; Gao, S.S.; Duangthip, D.; Lo, E.C.M.; Chu, C.H. Randomized Clinical Trial on Sodium Fluoride with Tricalcium Phosphate. J. Dent. Res. 2021, 100, 66–73. [Google Scholar] [CrossRef]
- Hummel, R.; Akveld, N.A.E.; Bruers, J.J.M.; van der Sanden, W.J.M.; Su, N.; Heijden, G.J.M.G. van der Caries Progression Rates Revisited: A Systematic Review. J. Dent. Res. 2019, 98, 746–754. [Google Scholar] [CrossRef]
- Fee, P.A.; Riley, P.; Worthington, H.V.; Clarkson, J.E.; Boyers, D.; Beirne, P.V. Recall Intervals for Oral Health in Primary Care Patients. Cochrane Database Syst. Rev. 2020, 10, 1–56. [Google Scholar] [CrossRef]


{kind=link}
| Topical Fluorides | No. of Studies | No. of Participants | D(M)FS- Prevented Fractions |
|---|---|---|---|
| Fluoride Toothpaste [72] | 70 | 42,300 | 24% (95%CI 21–28%) |
| Fluoride Mouthrinses [71] | 35 | 15,305 | 27% (95%CI 23–30%) |
| Fluoride Mousse | - | - | |
| Fluoride Gels [73] | 25 | 8479 | 28% (95%CI 19–36%) |
| Fluoride foam | - | - | |
| Fluoride Varnishes [74] | 13 | 6479 | 43% (95%CI 30–57%) |
| Fluoride solutions | - | - | |
| Silver Diamine Fluoride [79] | 2 | 915 | 78% (95%CI 68–87%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, O.Y.; Lam, W.Y.-H.; Wong, A.W.-Y.; Duangthip, D.; Chu, C.-H. Nonrestorative Management of Dental Caries. Dent. J. 2021, 9, 121. https://doi.org/10.3390/dj9100121
Yu OY, Lam WY-H, Wong AW-Y, Duangthip D, Chu C-H. Nonrestorative Management of Dental Caries. Dentistry Journal. 2021; 9(10):121. https://doi.org/10.3390/dj9100121
Chicago/Turabian StyleYu, Ollie Yiru, Walter Yu-Hang Lam, Amy Wai-Yee Wong, Duangporn Duangthip, and Chun-Hung Chu. 2021. "Nonrestorative Management of Dental Caries" Dentistry Journal 9, no. 10: 121. https://doi.org/10.3390/dj9100121
APA StyleYu, O. Y., Lam, W. Y.-H., Wong, A. W.-Y., Duangthip, D., & Chu, C.-H. (2021). Nonrestorative Management of Dental Caries. Dentistry Journal, 9(10), 121. https://doi.org/10.3390/dj9100121