Myofunctional Trainer versus Twin Block in Developing Class II Division I Malocclusion: A Randomized Comparative Clinical Trial


Abstract
1. Introduction
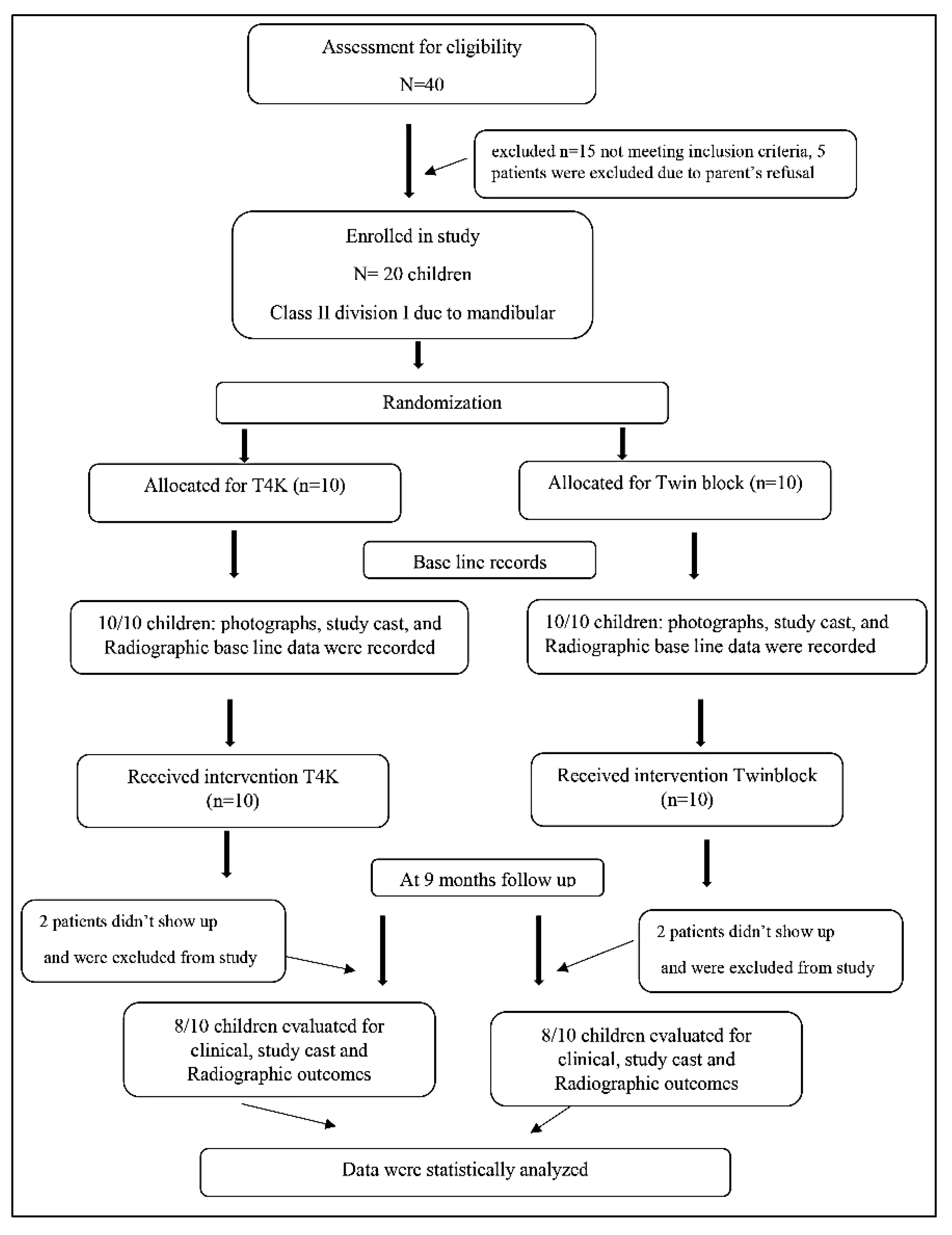
2. Materials and Methods
3. Results
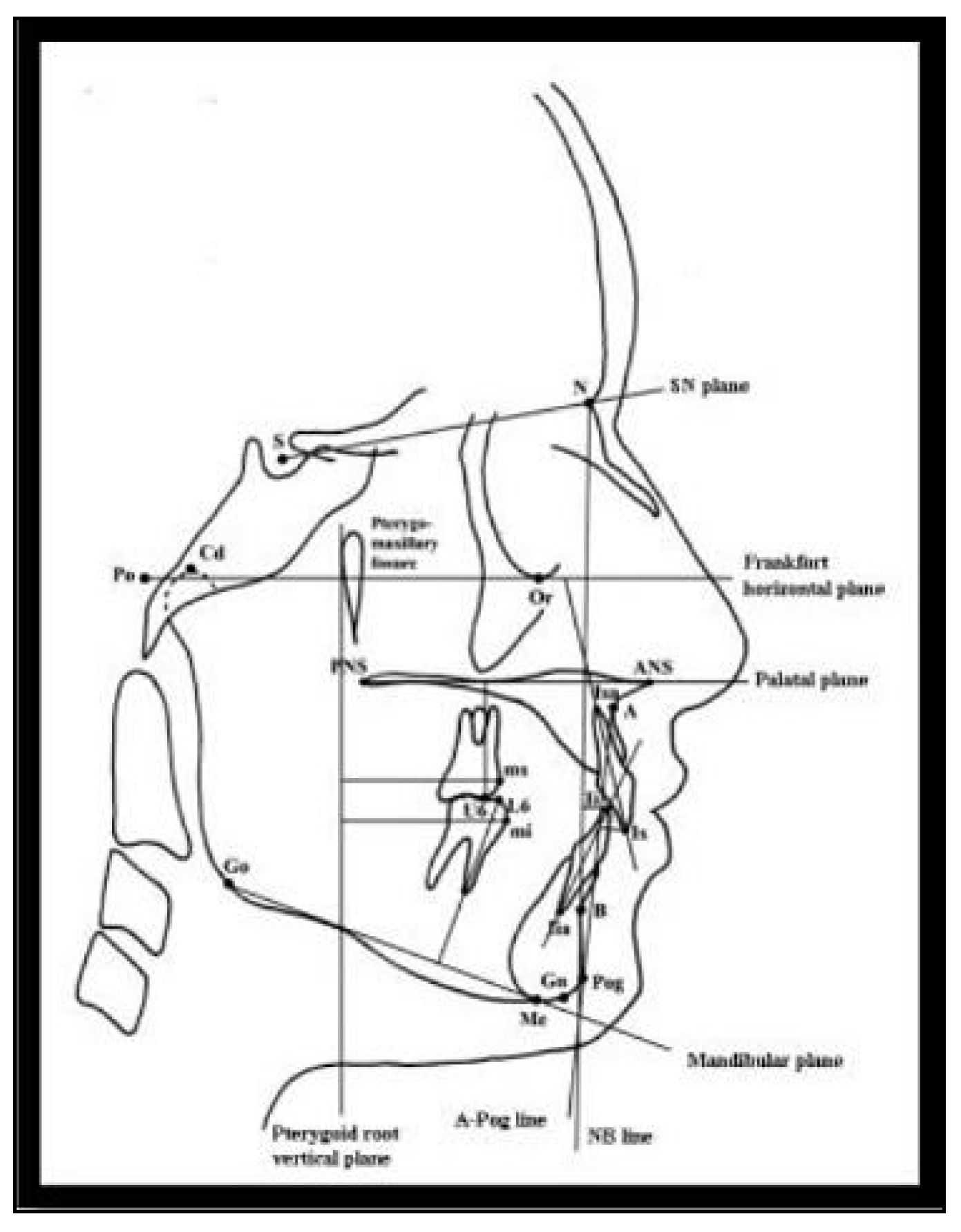
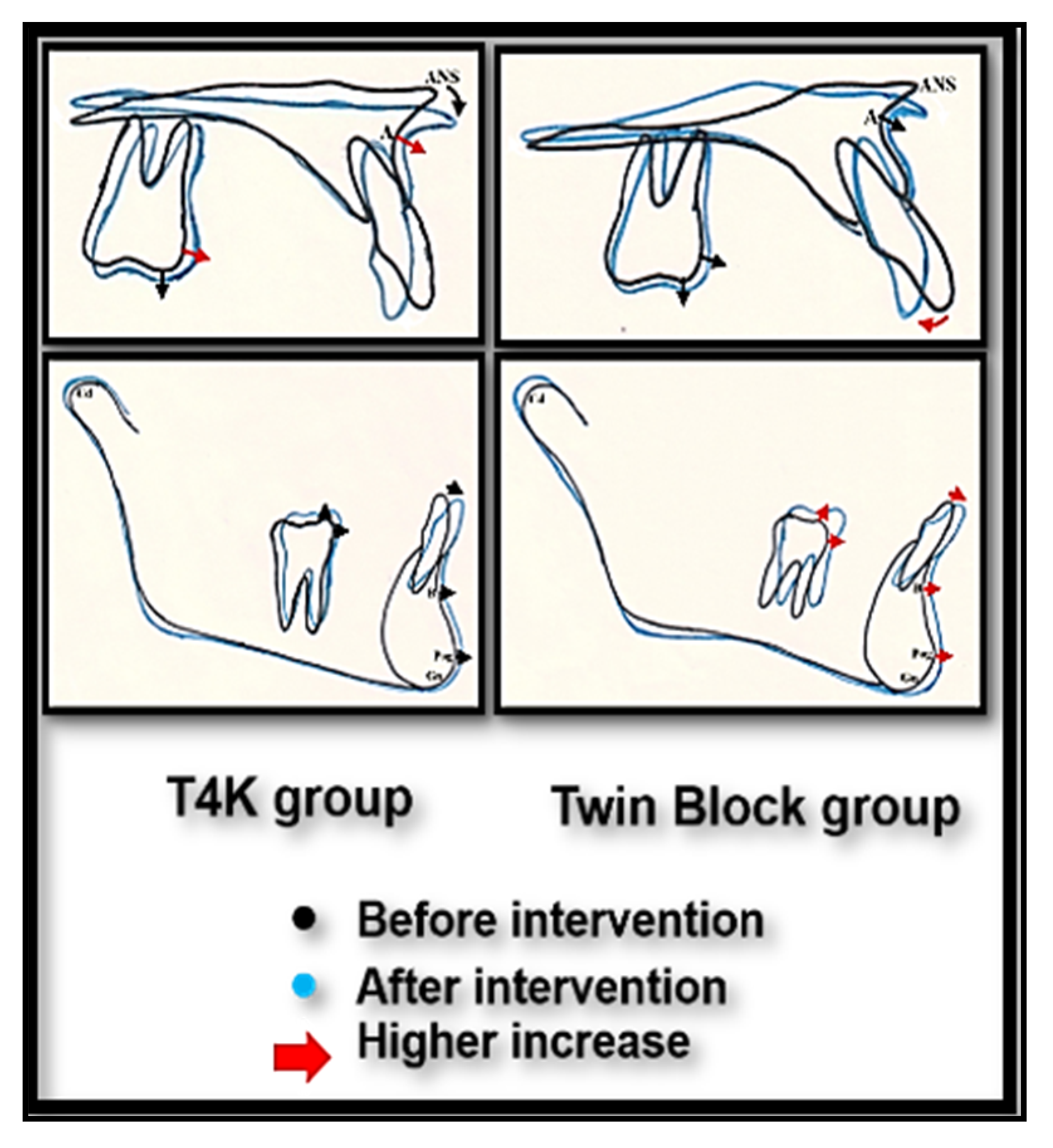
3.1. Cephalometric Dentoalveolar Changes after Appliance Therapy
3.2. Study Cast Changes after Appliance Therapy
4. Discussion
5. Conclusions
6. Recommendations
Author Contributions
Funding
Conflicts of Interest
References
- Moyers, R.E.; Riolo, M.L.; Guire, K.E.; Wainright, R.L.; Bookstein, F.L. Differential diagnosis of Class II malocclusions: Part 1. Facial types associated with Class II malocclusions. Am. J. Orthod. 1980, 78, 477–494. [Google Scholar] [CrossRef]
- Isola, G.; Anastasi, G.P.; Matarese, G.; Williams, R.C.; Cutroneo, G.; Bracco, P.; Piancino, M.G. Functional and molecular outcomes of the human masticatory muscles. Oral Dis. 2018, 24, 1428–1441. [Google Scholar] [CrossRef] [PubMed]
- Isola, G.; Perillo, L.; Migliorati, M.; Matarese, M.; Dalessandri, D.; Grassia, V.; Alibrandi, A.; Matarese, G. The impact of temporomandibular joint arthritis on functional disability and global health in patients with juvenile idiopathic arthritis. Eur. J. Orthod. 2019, 41, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Ivorra-Carbonell, L.; Montiel-Company, J.M.; Almerich-Silla, J.M.; Paredes-Gallardo, V.; Bellot-Arcís, C. Impact of functional mandibular advancement appliances on the temporomandibular joint—A systematic review. Med. Oral Patol. Oral Cir. Bucal. 2016, 21, e565–e572. [Google Scholar] [CrossRef] [PubMed]
- Jena, A.K.; Duggal, R.; Parkash, H. Skeletal and dentoalveolar effects of Twin-block and bionator appliances in the treatment of Class II malocclusion: A comparative study. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 594–602. [Google Scholar] [CrossRef] [PubMed]
- Clark, W.J. Twin Block Functional Therapy; Mosby-Wolfe: London, UK, 1995; pp. 13–28. [Google Scholar]
- Dyer, F.M.V.; McKeown, H.F.; Sandler, P.J. The modified Twin Block appliance in the treatment of Class II division 2 malocclusions. J. Orthod. 2001, 28, 271–280. [Google Scholar] [CrossRef]
- Saikoski, L.Z.; Cançado, R.H.; Valarelli, F.P.; de Freitas, K.M.S. Dentoskeletal effects of Class II malocclusion treatment with the Twin Block appliance in a Brazilian sample: A prospective study. Dental Press J. Orthod. 2014, 19, 36–45. [Google Scholar] [CrossRef][Green Version]
- Joseph, A.; Adyanthaya, A.K.D. Treatment of Class II Malocclusion using Twin Block Appliance. Int. J. Oral Health Med. Res. 2015, 2, 44–47. [Google Scholar]
- Parkin, N.A.; McKeown, H.F.; Sandler, P.J. Comparison of 2 modifications of the Twin-block appliance in matched Class II samples. Am. J. Orthod. Dentofac. Orthop. 2001, 119, 572–577. [Google Scholar] [CrossRef]
- Khafagy, A. A Clinical Evaluation of Twin Block Functional Applaince. Master’s Thesis, Alexandria University, Alexandria, Egypt, 2001. [Google Scholar]
- Co.T4K MR. The Trainer for kidsTM Pre Orthodontic TrainerTM. Procedures Manual. 2003. Available online: http://www.myoresearch.com/cms/download.php?9b8ad8cd7477cb33821fcdd6e7204e1c (accessed on 18 June 2008).
- Usumez, S.; Uysal, T.; Sari, Z.; Basciftci, F.A.; Karaman, A.I.; Guray, E. The effects of early preorthodontic trainer treatment on class II, division 1 patients. Angle Orthod 2004, 74, 605–609. [Google Scholar]
- Das, U.M.; Reddy, D. Treatment effects produced by preorthodontic trainer appliance in patients with class II division I malocclusion. J. Indian Soc. Pedod Prev. Dent. 2010, 28, 30. [Google Scholar] [CrossRef] [PubMed]
- Da Rosa, G.N.; Del Fabro, J.P.; Tomazoni, F.; Tuchtenhagen, S.; Alves, L.S.; Ardenghi, T.M. Association of malocclusion, happiness, and oral health–related quality of life (OHRQoL) in schoolchildren. J. Public Health Dentistry 2016, 76, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Jimmy, R.; Pinkham, J. The Dynamics of change. In Pediatric Dentistry: Infancy Through Adolescence, 4th ed.; Pinkham, J., Casamassimo, P.S., Fields, H.W., McTigue, D.J., Nowak, A., Eds.; Elsevier Saunders: St. Louis, MI, USA, 2005; pp. 464–470. [Google Scholar]
- Schulz, K.F.; Altman, D.G. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomized trials. Int. J. Surg. 2011, 9, 672–677. [Google Scholar] [CrossRef] [PubMed]
- M S. Random Allocation Software. 2004. p. 1–6. Available online: https://bmcmedresmethodol.biomedcentral.com/articles/10.1186/1471-2288-4-26 (accessed on 10 March 2008).
- Power/Sample Size Calculator. Available online: https://www.stat.ubc.ca/~rollin/stats/ssize/n2.html. (accessed on 10 March 2008).
- Kayapınar, U. Measuring essay assessment: Intra-rater and inter-rater reliability. Eurasian J. Educ. Res. 2014, 16, 113–136. [Google Scholar] [CrossRef]
- Rosner, B. Hypothesis Testing: Categorical Data-Estimation of Sample Size and Power for Comparing Two Binomial Proportions. In Fundamentals of Biostatistics, 6th ed.; Cengage Learning: Boston, MA, USA, 2010. [Google Scholar]
- Mohammed, H.; Čirgić, E.; Rizk, M.Z.; Vandevska-Radunovic, V. Effectiveness of prefabricated myofunctional appliances in the treatment of Class II division 1 malocclusion: A systematic review. Eur. J. Orthod. 2020, 42, 125–134. [Google Scholar] [CrossRef]
- Ferreira, F.G. Novel Approaches for Class II Malocclusion Treatment using Myofunctional Orthodontics Therapy: A Systematic Review. Int. J. Dent. Oral. Sci. 2017, 4, 503–507. [Google Scholar]
- Sidlauskas, A. Clinical effectiveness of the Twin block appliance in the treatment of Class II Division 1 malocclusion. Stomatologija 2005, 7, 7–10. [Google Scholar]
- Uysal, T.; Yagci, A.; Kara, S.; Okkesim, S. Influence of Pre-Orthodontic Trainer treatment on the perioral and masticatory muscles in patients with Class II division 1 malocclusion. Eur. J. Orthod. 2012, 34, 96–101. [Google Scholar] [CrossRef]
- Toth, L.R.; McNamara, J.A. Treatment effects produced by the twin-block appliance and the FR-2 appliance of Fränkel compared with an untreated Class II sample. Am. J. Orthod. Dentofac. Orthop. 1999, 116, 597–609. [Google Scholar] [CrossRef]
- Cirgić, E.; Kjellberg, H.; Hansen, K. Treatment of large overjet in Angle Class II: Division 1 malocclusion with Andresen activators versus prefabricated functional appliances- A multicenter, randomized, controlled trial. Eur. J. Orthod. 2016, 38, 516–524. [Google Scholar] [CrossRef]
- Sanjay, N.; Rajesh, R.; Sreedevi, D.; Patil, R. Correction of Deep Bite with a Functional Trainer. World J. Dent. 2011, 2, 360–362. [Google Scholar] [CrossRef]
- Dinkova, M. Vertical control of overbite in mixed dentition by Trainer System. J. IMAB 2014, 20, 648–654. [Google Scholar] [CrossRef][Green Version]
- Idris, G.; Hajeer, M.Y.; Al-Jundi, A. Soft- and hard-tissue changes following treatment of Class II division 1 malocclusion with Activator versus Trainer: A randomized controlled trial. Eur. J. Orthod. 2019, 41, 21–28. [Google Scholar] [CrossRef]
- Koretsi, V.; Zymperdikas, V.F.; Papageorgiou, S.N.; Papadopoulos, M.A. Treatment effects of removable functional appliances in patients with Class II malocclusion: A systematic review and meta-analysis. Eur. J. Orthod. 2015, 37, 418–434. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measurements | Before Intervention Mean ± SD | t-Test p Value | |
|---|---|---|---|
| Group I (N = 8) | Group II (N = 8) | ||
| Cephalometric Angular Measurements | |||
| Upper incisor to Frankfort Horizontal plane (U1-FHP) (°) | 119.81 ± 4.52 | 121.13 ± 4.22 | 0.60 0.56 |
| Lower incisor to mandibular plane (L1-MP) (°) | 95.50 ± 1.67 | 95.44 ± 3.41 | 0.05 0.96 |
| Cephalometric Linear Measurements | |||
| Maxillary incisor to APog line (Is-APog) (mm) | 10.38 ± 2.26 | 11.13 ± 1.55 | 0.77 0.45 |
| Mandibular incisor to NB line (Ii-NB) (mm) | 5.19 ± 0.96 | 6.63 ± 1.58 | 2.20 0.06 |
| Maxillary molar to palatal plane (U6-PL.P) (mm) | 20.50 ± 1.77 | 19.25 ± 2.42 | 1.18 0.26 |
| Mandibular molar to mandibular plane (L6-MP) (mm) | 28.69 ± 1.53 | 27.44 ± 3.11 | 1.02 0.33 |
| Mandibular molar to PtV line (mi-PtV) (mm) | 22.13 ± 4.90 | 24.44 ± 4.99 | 0.94 0.37 |
| Maxillary molar to PtV line (ms-PtV) (mm) | 25.13 ± 3.93 | 27.06 ± 5.26 | 0.83 0.42 |
| Study Cast Measurements | |||
| Overjet (mm) | 7.88 ± 1.66 | 7.94 ± 1.82 | 0.07 0.94 |
| Overbite (%) | 46.47 ± 23.54 | 61.39 ± 17.66 | 1.43 0.17 |
| Upper Arch perimeter (UAP) (mm) | 88.06 ± 4.44 | 83.00 ± 5.20 | 2.09 0.06 |
| Lower Arch perimeter (LAP) (mm) | 72.63 ± 2.94 | 72.56 ± 6.96 | 0.02 0.98 |
| Measurements | Before Intervention Mean ± SD | After Intervention Mean ± SD | Paired t-Test p Value | Difference Mean ± SD |
|---|---|---|---|---|
| Cephalometric Angular Measurements | ||||
| Upper incisor to Frankfort Horizontal plane (U1-FHP) (°) | 119.81 ± 4.52 | 115.81 ± 5.47 | 3.80 0.01 * | −4.00 ± 2.98 |
| Lower incisor to mandibular plane (L1-MP) (°) | 95.50 ± 1.67 | 97.44 ± 1.70 | 4.33 0.003 * | 1.94 ± 1.27 |
| Cephalometric Linear Measurements | ||||
| Maxillary incisor to APog line (Is-APog) (mm) | 10.38 ± 2.26 | 8.38 ± 2.63 | 5.47 0.001 * | −2.00 ± 1.04 |
| Mandibular incisor to NB line (Ii-NB) (mm) | 5.19 ± 0.96 | 6.25 ± 1.39 | 4.43 0.003 * | 1.06 ± 0.68 |
| Maxillary molar to palatal plane (U6-PL.P) (mm) | 20.50 ± 1.77 | 20.88 ± 1.79 | 2.39 0.05 * | 0.38 ± 0.44 |
| Mandibular molar to mandibular plane (L6-MP) (mm) | 28.69 ± 1.53 | 29.19 ± 1.36 | 3.74 0.01 * | 0.50 ± 0.38 |
| Mandibular molar to PtV line (mi-PtV) (mm) | 22.13 ± 4.90 | 23.88 ± 4.49 | 6.55 <0.0001 * | 1.75 ± 0.76 |
| Maxillary molar to PtV line (ms-PtV) (mm) | 25.13 ± 3.93 | 26.19 ± 3.89 | 4.43 0.003 * | 1.06 ± 0.68 |
| Study Cast Measurements | ||||
| Overjet (mm) | 7.88 ± 1.66 | 5.38 ± 2.17 | 7.07 <0.0001 * | −2.50 ± 1.00 |
| Overbite % | 46.47 ± 23.54 | 51.12 ± 21.64 | 1.72 0.13 | 4.65 ± 7.65 |
| Upper Arch perimeter (UAP) (mm) | 88.06 ± 4.44 | 88.94 ± 4.84 | 1.67 0.14 | 0.88 ± 1.48 |
| Lower Arch perimeter (LAP) (mm) | 72.63 ± 2.94 | 73.81 ± 2.83 | 3.49 0.01 * | 1.19 ± 0.96 |
| Measurements | Before Intervention Mean ± SD | After Intervention Mean ± SD | Paired t-Test p Value | Difference Mean ± SD |
|---|---|---|---|---|
| Cephalometric Angular Measurements | ||||
| Upper incisor to Frankfort Horizontal plane (U1-FHP) (°) | 121.13 ± 4.22 | 113.38 ± 3.89 | 5.54 0.001 * | −7.75 ± 3.96 |
| Lower incisor to mandibular plane (L1-MP) (°) | 95.44 ± 3.41 | 97.63 ± 4.30 | 5.19 0.001 * | 2.19 ± 1.19 |
| Cephalometric Linear Measurements | ||||
| Maxillary incisor to APog line (Is-APog) (mm) | 11.13 ± 1.55 | 8.13 ±1.27 | 14.20 <0.0001 * | −3.00 ± 0.60 |
| Mandibular incisor to NB line (Ii-NB) (mm) | 6.63 ± 1.58 | 7.81 ± 1.62 | 7.33 <0.0001 * | 1.19 ± 0.46 |
| Maxillary molar to palatal plane (U6-PL.P) (mm) | 19.25 ± 2.42 | 19.63 ± 2.75 | 2.39 0.05 * | 0.38 ± 0.44 |
| Mandibular molar to mandibular plane (L6-MP) (mm) | 27.44 ± 3.11 | 29.56 ± 3.27 | 6.30 <0.0001 * | 2.13 ± 0.95 |
| Mandibular molar to PtV line (mi-PtV) (mm) | 24.44 ± 4.99 | 26.44 ± 5.21 | 9.47 <0.0001 * | 2.00 ± 0.60 |
| Maxillary molar to PtV line (ms-PtV) (mm) | 27.06 ± 5.26 | 27.19 ± 5.62 | 0.40 0.70 | 0.13 ± 0.88 |
| Study Cast Measurements | ||||
| Overjet (mm) | 7.94 ± 1.82 | 4.19 ± 1.39 | 9.63 <0.0001 * | −3.75 ± 1.10 |
| Overbite (%) | 61.39 ± 17.66 | 45.17 ± 12.20 | 2.70 0.03 * | −16.22 ± 17.02 |
| Upper Arch perimeter (UAP) (mm) | 83.00 ± 5.20 | 81.75 ± 5.96 | 2.24 0.06 | −1.25 ± 1.58 |
| Lower Arch perimeter (LAP) (mm) | 72.56 ± 6.96 | 70.88 ± 6.99 | 6.78 <0.0001 * | −1.69 ± 0.70 |
| Measurements | After Intervention Mean ± SD | t-Test p Value | |
|---|---|---|---|
| Group I (N = 8) | Group II (N = 8) | ||
| Cephalometric Angular Measurements | |||
| Upper incisor to Frankfort Horizontal plane (U1-FHP) (°) | −4.00 ± 2.98 | −7.75 ± 3.96 | 2.14 0.05 * |
| Lower incisor to mandibular plane (L1-MP) (°) | 1.94 ± 1.27 | 2.19 ± 1.19 | 0.41 0.69 |
| Cephalometric Linear Measurements | |||
| Maxillary incisor to APog line (Is-APog) (mm) | −2.00 ± 1.04 | −3.00 ± 0.60 | 2.37 0.04 * |
| Mandibular incisor to NB line (Ii-NB) (mm) | 1.06 ± 0.68 | 1.19 ± 0.46 | 0.43 0.67 |
| Maxillary molar to palatal plane (U6-PL.P) (mm) | 0.38 ± 0.44 | 0.38 ± 0.44 | 0 1.00 |
| Mandibular molar to mandibular plane (L6-MP) (mm) | 0.50 ± 0.38 | 2.13 ± 0.95 | 4.48 0.001 * |
| Mandibular molar to PtV line (mi-PtV) (mm) | 1.75 ± 0.76 | 2.00 ± 0.60 | 0.73 0.48 |
| Maxillary molar to PtV line (ms-PtV) (mm) | 1.06 ± 0.68 | 0.13 ± 0.88 | 2.39 0.03 * |
| Study Cast Measurements | |||
| Overjet (mm) | −2.50 ± 1.00 | −3.75 ± 1.10 | 2.38 0.03 * |
| Overbite % | 4.65 ± 7.65 | −16.22 ± 17.02 | 3.16 0.007 * |
| Upper Arch perimeter (UAP) (mm) | 0.88 ± 1.48 | −1.25 ± 1.58 | 2.77 0.02 * |
| Lower Arch perimeter (LAP) (mm) | 1.19 ± 0.96 | −1.69 ± 0.70 | 6.83 <0.0001 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elhamouly, Y.; El-Housseiny, A.A.; Ismail, H.A.; El Habashy, L.M. Myofunctional Trainer versus Twin Block in Developing Class II Division I Malocclusion: A Randomized Comparative Clinical Trial. Dent. J. 2020, 8, 44. https://doi.org/10.3390/dj8020044
Elhamouly Y, El-Housseiny AA, Ismail HA, El Habashy LM. Myofunctional Trainer versus Twin Block in Developing Class II Division I Malocclusion: A Randomized Comparative Clinical Trial. Dentistry Journal. 2020; 8(2):44. https://doi.org/10.3390/dj8020044
Chicago/Turabian StyleElhamouly, Yasmine, Azza A. El-Housseiny, Hanan A. Ismail, and Laila M. El Habashy. 2020. "Myofunctional Trainer versus Twin Block in Developing Class II Division I Malocclusion: A Randomized Comparative Clinical Trial" Dentistry Journal 8, no. 2: 44. https://doi.org/10.3390/dj8020044
APA StyleElhamouly, Y., El-Housseiny, A. A., Ismail, H. A., & El Habashy, L. M. (2020). Myofunctional Trainer versus Twin Block in Developing Class II Division I Malocclusion: A Randomized Comparative Clinical Trial. Dentistry Journal, 8(2), 44. https://doi.org/10.3390/dj8020044