Abstract
The aim of this study was to assess awareness and knowledge of undergraduate dental students of common caries-related preventive considerations and to highlight these factors in a concise manner to act as a guide for dental practitioners. A sample of 118 undergraduate students at a local government dental school was included. An interactive survey that contains questions related to common preventive strategies against dental caries was presented to the students. The survey contained 22 questions concerning dietary and therapeutic strategies. Students casted their votes using their mobile cellphones. The correct answer for each question was shown to the students, and further discussion was held. Data was collected, and the statistical analysis was conducted using one-sample z- and chi-squared tests at 0.05 significance level. The students answered the questions related to oral hygiene practices, xylitol, and the common knowledge regarding fluoride. The questions related to the use of chlorhexidine, dietary factors, and fluoride formulations were answered mostly incorrectly. The students seemed to grasp details of important concepts of flossing, brushing, reducing frequency of sugar exposure, and the use of fluoride products. Still, more emphasis should be given to increase students’ awareness of dietary guidelines for caries prevention, since adequate knowledge of these modalities is paramount for graduating dentists.
1. Introduction
Dental caries remains to be one of the most common diseases affecting humans [1,2]. This disease can be defined as “a biofilm-mediated, diet modulated, multifactorial, non-communicable, dynamic disease resulting in net mineral loss of dental hard tissues” [3]. According to the definition, dental caries is greatly modulated by dietary patterns of the individual among other factors. The caries process can be reversed in its early stages without the need for operative procedures [4]. Still, the use of preventive strategies is considered more beneficial and more cost-effective to deal with this disease’s signs and symptoms, since the techniques focusing on surgical intervention rarely change the oral conditions that caused the disease [5,6].
There has been a recent shift in managing dental caries with more focus on prevention and conservative and minimal intervention strategies in the hope of maintaining tooth structure [7]. The reason for this shift is the proven ineffectiveness of current surgical approaches when managing dental caries [1]. Dentists are encouraged to adopt methods for early detection and diagnosis of caries lesions and manage the situation using individualized treatment modalities based on the patient’s caries risk with the focus on behavioral changes and enhancing local protective factors [8].
Undergraduate operative curricula should focus more on presenting the concepts of dental caries dynamics and clinical diagnosis. This should be complemented with highlighting the factors associated with the onset of the disease, as well as the conditions necessary for its prevention and/or reversal. The discussion of these factors should be held at early stages of the dental curriculum, and the focus should be laid on attempting to assess the student’s knowledge frequently to ensure their understating and alignment with practice during clinical sessions. This knowledge and focused clinical practices are very important to a dentist in order to reduce the dental caries incidence, improve the caries risk status of patients, and manage the existing disease at early stages.
A quick search in the PubMed database for “Cariology Education” or “Dental Caries Education” brings a vast number of reports that discuss implementation of cariology and new concepts for teaching dental caries in undergraduate dental curricula worldwide. These approaches include lecture-based modules [9,10], competency-based cariology management programs [11], and curricula developed by regional dental organizations [12,13,14]. It is worth noting that the majority of the mentioned reports emphasized the shift towards prevention, early diagnosis, and conservative approaches of management (e.g., remineralization) when teaching dental caries [10,14,15,16,17,18,19,20,21]. Further, caries risk assessment is among the most important concepts included in these approaches; it is affected by multiple factors, including dietary aspects, oral hygiene practices, bacterial factors, and fluoride exposure [5,22]. A common model for determining caries risk based on these factors is the Caries Management by Risk Assessment (CAMBRA) [5,23]. These concepts must be included in cariology instruction, and students must be assessed for their understanding of the beforementioned concepts to ensure application of preventive and conservative approaches. Hence, the aim of the current study was to assess the knowledge and awareness of undergraduate dental students of common caries-preventive and therapeutic principles. As a secondary objective, common practices in caries prevention and management in light of the CAMBRA model were stated to act as a concise guide for graduating dentists, as well as for public health professionals and dieticians.
2. Materials and Methods
This study was approved by the research ethics committee, Faculty of Dentistry, King Abdulaziz University, institutional review board (IRB protocol #157-11-19 / December 08, 2019), and all the participants voluntarily agreed to participate in the study. One hundred and eighteen fifth-year undergraduate dental students (61 males and 57 females) were enrolled into this study. These students were exposed to the concepts of dental caries dynamics, diagnosis, risk assessment, and conservative management in the previous academic year. The survey setting was a regular lecture hall that contained a digital projector and wireless internet connection; the survey was conducted separately for male and female students one day apart due to cultural restrictions within the country of the study. The survey consisted of 22 multiple choice questions dealing with common concepts of caries-preventive and conservative management that were presented one at a time using the projector (Table 1). The students were asked to join the online survey session by scanning a QR code provided on the screen using the DirectPoll online tool (http://directpoll.com/; Netcetera, Zurich, Switzerland). The stem of each question was read aloud by the presenter, and a pause was provided to allow students to cast their votes for the answer individually using their cellphones. After the majority of the students would have voted, the percentages for each option would be shown on the projector’s screen, and the correct answer was highlighted. This was supplemented by discussing the rationale behind each answer and the common misconceptions regarding that particular item. The process was repeated for each item, and the students provided their feedback at the end of the session.

Table 1.
The questions included in the survey with the correct answer in brackets (actual survey questions were not dichotomous), as well as statistical comparisons for each question of the survey showing proportions of correct vs. incorrect answers and proportions of female (n = 57) vs. male (n = 61) students with correct answers (total n = 118).
The data from both sessions were stored in the cloud on the polling service’s servers. The data were analyzed in light of five themes: caries risk, oral hygiene practices, dietary factors, fluorides, and bacterial factors. The statistical testing was done using a one-sample z-test for comparing a proportion with a fixed number to determine the significance of proportion of the students with the correct answer. Also, a chi-squared test was done to determine the proportion of the students with the correct answer in the male and female groups. All the tests were done using SPSS ver. 17 (SPSS Inc., Chicago, Illinois, USA) at 0.05 significance level.
3. Results
Table 1 shows statistical comparisons for each question. Overall, the students correctly answered the questions related to oral hygiene practices, including brushing and flossing. These questions showed more female students answering correctly, except for the recommended duration of brushing, which was not significantly different between male and female students.
Regarding the use of chlorhexidine, the students provided correct answers to all the three questions, even though more correct answers were given by female students. A similar trend was observed when the students were asked about the dietary control with low proportions of students answering correctly the majority of questions. This group of questions was presented to depict their understanding of the common dietary parameters affecting the caries process (Table 2). However, a very high percentage of students recognized xylitol as the most anticariogenic sugar substitute and frequency as the main consideration for sugar consumption in relation to dental caries.
Table 2.
Dietary parameters that can affect the caries risk status.
The students were asked four questions concerning fluorides; two questions were answered correctly by the majority of students; however, the students did not provide a lot of correct answers to the questions related to the fluoride concentration in oral hygiene products.
Overall, the female students provided more correct answers compared to the male students to the majority of questions. This can be clearly seen in Table 1 that shows more female students providing correct answers as compared to the males. This is very clear in the question related to the disease indicators of the caries management by risk assessment (CAMBRA) model (Figure 1). Table 3 states the recommendations based on this model for managing patients. Still, incorrect answers to question 16 that tested their knowledge regarding cariogenicity of breast and cow milk were predominantly provided by female students.
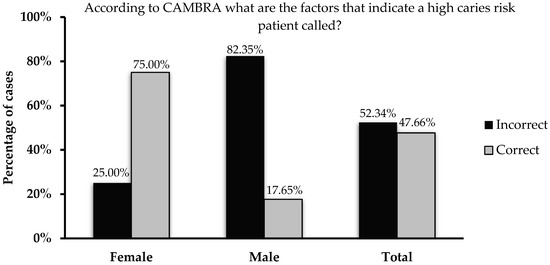
Figure 1.
Percentages of female, male, and total students who answered the question regarding the CAMBRA protocol.
Table 3.
Caries risk assessment and management guidelines based on the CAMBRA risk levels (adapted from Jenson et al., 2007).
4. Discussion
Dental caries takes a major toll on health services owing to the restorative burden required to replace the diseased tooth structure [6]. Failure to address pathological factors within the oral environment can cause a restored tooth to enter what is known as the “restorative cycle,” since the restoration will not stop the active disease [24]. This cycle means that the restored tooth is subjected to more extensive and aggressive restorative treatments that are frequently replaced by another until the tooth is considered unrestorable owing to little remaining tooth structure. It is estimated that two thirds of restorative treatments are performed on previously restored teeth [25]. Despite this, dental caries lesions can be predictably prevented if early strategies are implemented [1,6]. These include oral hygiene practices, dietary control, fluoride therapy, antimicrobials, sealants, and glass ionomer restorations.
The primary etiology of dental caries diseases is the disturbance in the balance between protective and pathological factors within the oral cavity in favor of the growth of cariogenic bacteria [26]. If these microorganisms continue to thrive by fermenting dietary carbohydrates, they produce lactic acid that can demineralize the hydroxyapatite crystals within the tooth structure. Usually, this mineral loss could be regained in the presence of fluorides and the supersaturation status of saliva. However, if these protective factors are compromised, such as in cases with reduced salivary flow, lack of fluorides, or increased exposure to fermentable carbohydrates, continuous demineralization takes place, tipping the demineralization/remineralization balance and leading to the development of caries lesions. Still, at early stages, these lesions can be remineralized if protective factors are enhanced; however, if the acidic challenges are too extreme or persist for prolonged periods of time, irreversible cavitation can take place, necessitating surgical intervention to remove the diseased tissue according to the conservative management strategies to prevent reoccurrence of the disease [5,27].
The use of fluorides is considered one of the most effective strategies to decrease dental caries incidence and to help remineralize early lesions [4,28]. Among the many forms of fluoride delivery, toothpaste is considered effective in maintaining adequate fluoride levels for caries prevention and management [29]. Knowledge of the amounts and concentrations available in common dental products is crucial in providing the patient with a proper treatment plan and to avoid complications. The students in the current investigation do not seem to be aware of the different concentrations found in common dental products. Further, they are not aware of the major disadvantage of its use, which is toxicity. Based on these findings, additional theory sessions should be considered in order to expose students to the basic mechanisms of action of fluorides to enhance mineral uptake by the tooth structure and to discuss possible side effects due to overexposure to fluorides. The principle modes of fluoride action include: 1) increasing remineralization by enhancing the uptake of calcium and phosphates, 2) decreasing demineralization by the formation of fluorohydroxyapatite crystals that are larger and more resistant to acidic challenges, and 3) inhibiting bacterial enzymes, such as enolase [30,31].
Reducing the dental biofilm (formerly known as dental plaque) can aid in reducing the magnitude of acidic challenges and their frequency. This can be achieved via a combination of physical and pharmacological strategies. Tooth brushing and flossing are recommended to patients to clean teeth surfaces in order to reduce the bacterial load and subsequent demineralization. Brushing is recommended twice daily for 2 minutes using a soft toothbrush accompanied by a fluoride-containing toothpaste [32]. Further, the abrasive potential of toothpastes is also very important to be considered, and highly abrasive formulations, such as whitening dentifrices, should be avoided in cases with incipient lesions [33,34]. Although dental flossing can reduce the amounts of biofilm interproximally, no direct correlation between flossing and reducing proximal caries lesions was established. In addition to the small role of xylitol as an agent to decrease Streptococcus mutans load, chlorhexidine is considered very effective in patients with a high caries risk with an increased S. mutans load [35,36,37]. It should be mentioned that chlorhexidine is not very effective against Lactobacilli, which are more sensitive to dietary modifications [37]. In the present investigation, more than half of the cohort recognized this.
The increase in sugar consumption is linked to the increased incidence of dental caries in the literature [22]. Simple sugars can cause more dental caries owing to their faster metabolization by cariogenic bacteria [38]. Of course, different dietary habits can contribute to the dental caries process differently. Table 2 summarizes some dietary parameters and the effect on the caries process. Frequency is one of the major factors affecting the caries balance [22,39]. A more frequent exposure to fermentable carbohydrates leads to more demineralization episodes leaving the saliva struggling to neutralize these acidic challenges [40]. This factor was predominantly identified by the students. A related factor is the duration of sugar consumption; prolonged periods of sugar consumption lead to sustained lactic acid production by cariogenic bacteria causing the process of demineralization to remain for as long as the sugars are being consumed. High frequency and long duration of sugar consumption are two of the factors that will cause the plaque and salivary pH level to decrease providing a suitable acidic environment for dental caries to develop [39]. Overall, patients should be instructed to reduce the frequency and duration of fermentable carbohydrates consumption. This should be accompanied by substitution with healthy snacks and protective foods, such as nuts and cheese.
Xylitol is considered one of the bulk sweeteners or sugar alcohols [41], and by far is considered the one with the most anticariogenic potential [42] with multiple studies showing its ability to reduce the Streptococcus mutans load in plaque and saliva [43,44,45,46]. Utilizing a regimen containing a xylitol chewing gum is recommended when caries risk assessment models are considered [22,23]; for an overview, please refer to the recent review by Nassar [47]. The students seem to grasp this concept very well, and the majority of them (approximately 92%) recognized that xylitol is the only sugar substitute with an anticariogenic potential (Table 1).
The Caries Management by Risk Assessment (CAMBRA) model is one of the well-established caries risk assessment models utilized to depict a patient’s caries risk. It categorizes patients into four categories based on certain parameters. The presence of signs of the disease (also known as disease indicators, which the knowledge among the students in this cohort was less than ideal, Figure 1) establishes the patient as being at high risk of developing new caries lesions. This can be complicated by a reduced salivary flow rate below normal levels (stimulated flow rate below 1.0 mL/min.) lowering the remineralization power of the saliva and providing better conditions for an unbuffered acidic environment. This consequently places the individual in the extremely high caries risk category. If disease indicators are not present, a comparative evaluation of protective and pathological factors should be considered. The presence of more pathological factors places the patient in the moderate caries risk category; and on the contrary, more protective factors indicate a low caries risk status [22].
After determining the patient’s caries risk, the CAMBRA guidelines can provide some management and preventive regimens that can be further tailored based on the case (Table 3). The CAMBRA model recommends a combination of the strategies described above which can be tailored according to the need. Additional methods that were not discussed include calcium phosphate products, neutralizing agents, and saliva substitutes (for details, please refer to the revised CAMBRA guidelines [48]). Of course, the CAMBRA model also promotes detection of caries lesions as early as possible in order to maximize the benefits of early conservative management strategies.
5. Conclusions
It is of utmost importance to educate the new generation of dentists to be able to distinguish the criteria causing the increased risk of dental caries. This would allow the formulation of individualized prevention (and management) plans that would allow patients to keep their teeth healthy for long periods and to reduce the need of restorative procedures. Also, it would be advantageous that dieticians and other professionals working in the dietary and health-related professions become familiar with dietary patterns and caries-inducing factors in order to reduce the prevalence of the dental caries disease worldwide, since it remains a global public health issue. Based on the findings of this investigation, emphasis on the concepts of caries risk assessment, especially on dietary factors and fluoride formulations, should be considered in undergraduate dental curricula.
Speaking of limitations of the present study, undergraduate dental students require more exposure to caries preventive and management strategies. This should be complemented by frequent emphasis on the clinical application of these modalities during regular educational encounters and sessions. Restriction of dietary fermentable carbohydrates, exposure to fluoride-containing products, and early caries diagnosis should be emphasized in order to prevent dental caries and/or reduce the need of invasive restorative treatments.
Author Contributions
Conceptualization, H.N.; methodology, H.N.; formal analysis, H.N.; investigation, H.N.; resources, H.N.; data curation, H.N.; writing—review and editing, H.N.; visualization, H.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Deanship of Scientific Research (DSR), King Abdulaziz University, Jeddah, Saudi Arabia, under grant No. (DF-048-165-1441).
Acknowledgments
The author gratefully acknowledges DSR technical and financial support.
Conflicts of Interest
The author declares no conflict of interest.
References
- Fontana, M.; Young, D.A.; Wolff, M.S.; Pitts, N.B.; Longbottom, C. Defining dental caries for 2010 and beyond. Dent. Clin. N. Am. 2010, 54, 423–440. [Google Scholar] [CrossRef]
- Mouradian, W.E.; Wehr, E.; Crall, J.J. Disparities in children’s oral health and access to dental care. JAMA 2000, 284, 2625–2631. [Google Scholar] [CrossRef]
- Pitts, N.B.; Zero, D.T.; Marsh, P.D.; Ekstrand, K.; Weintraub, J.A.; Ramos-Gomez, F.; Tagami, J.; Twetman, S.; Tsakos, G.; Ismail, A. Dental caries. Nat. Rev. Dis. Primers 2017, 3, 17030. [Google Scholar] [CrossRef]
- Ten Cate, J.M.; Mundorff-Shrestha, S.A. Working Group Report 1: Laboratory models for caries (in vitro and animal models). Adv. Dent. Res. 1995, 9, 332–334. [Google Scholar] [CrossRef]
- Young, D.A.; Featherstone, J.D.; Roth, J.R. Curing the silent epidemic: Caries management in the 21st century and beyond. J. Calif. Dent. Assoc. 2007, 35, 681–685. [Google Scholar]
- Marsh, P.D. Microbiology of dental plaque biofilms and their role in oral health and caries. Dent. Clin. N. Am. 2010, 54, 441–454. [Google Scholar] [CrossRef]
- Tyas, M.J.; Anusavice, K.J.; Frencken, J.E.; Mount, G.J. Minimal intervention dentistry--a review. FDI Commission Project 1-97. Int. Dent. J. 2000, 50, 1–12. [Google Scholar] [CrossRef]
- Pitts, N. Introduction, how the detection, assessment, diagnosis and monitoring of caries integrate with personalized caries management. Monogr. Oral Sci. 2009, 21, 1–14. [Google Scholar]
- Martignon, S.; Gomez, J.; Tellez, M.; Ruiz, J.A.; Marin, L.M.; Rangel, M.C. Current cariology education in dental schools in Spanish-speaking Latin American countries. J. Dent. Educ. 2013, 77, 1330–1337. [Google Scholar]
- Tikhonova, S.; Girard, F.; Fontana, M. Cariology Education in Canadian Dental Schools: Where Are We? Where Do We Need to Go? J. Dent. Educ. 2018, 82, 39–46. [Google Scholar] [CrossRef]
- Fontana, M.; Zero, D. Bridging the gap in caries management between research and practice through education: The Indiana University experience. J. Dent. Educ. 2007, 71, 579–591. [Google Scholar] [PubMed]
- Schulte, A.G.; Pitts, N.B.; Huysmans, M.C.; Splieth, C.; Buchalla, W. European Core Curriculum in Cariology for undergraduate dental students. Eur. J. Dent. Educ. 2011, 15 (Suppl. 1), 9–17. [Google Scholar] [CrossRef]
- Splieth, C.H.; Innes, N.; Sohnel, A. Evidence-based cariology in clinical and public health practice as part of the European Core Curriculum in Cariology. Eur. J. Dent. Educ. 2011, 15 (Suppl. 1), 45–51. [Google Scholar] [CrossRef] [PubMed]
- Fontana, M.; Guzman-Armstrong, S.; Schenkel, A.B.; Allen, K.L.; Featherstone, J.; Goolsby, S.; Kanjirath, P.; Kolker, J.; Martignon, S.; Pitts, N.; et al. Development of a Core Curriculum Framework in Cariology for U.S. Dental Schools. J. Dent. Educ. 2016, 80, 705–720. [Google Scholar] [PubMed]
- Ferreira-Nobilo Nde, P.; Rosario de Sousa Mda, L.; Cury, J.A. Cariology in curriculum of Brazilian dental schools. Braz. Dent. J. 2014, 25, 265–270. [Google Scholar] [CrossRef]
- Chaffee, B.W.; Featherstone, J.D. Long-term adoption of caries management by risk assessment among dental students in a university clinic. J. Dent. Educ. 2015, 79, 539–547. [Google Scholar]
- Daouda, F.; Aida, K.; Mbacke, L.C.; Mamadou, M. Assessment of dental caries prevention program applied to a cohort of elementary school children of Kebemer, a city in Senegal. J. Int. Soc. Prev. Community Dent. 2016, 6 (Suppl. 2), S105–S110. [Google Scholar] [CrossRef]
- Fontana, M.; Gonzalez-Cabezas, C.; de Peralta, T.; Johnsen, D.C. Dental Education Required for the Changing Health Care Environment. J. Dent. Educ. 2017, 81, eS153–eS161. [Google Scholar] [CrossRef]
- Pitts, N.B.; Mazevet, M.E.; Mayne, C. Shaping the future of dental education: Caries as a case-study. Eur. J. Dent. Educ. 2018, 22 (Suppl. 1), 30–37. [Google Scholar] [CrossRef]
- Raphael, S.L.; Foster Page, L.A.; Hopcraft, M.S.; Dennison, P.J.; Widmer, R.P.; Evans, R.W. A survey of cariology teaching in Australia and New Zealand. BMC Med. Educ. 2018, 18, 75. [Google Scholar] [CrossRef]
- Rayapudi, J.; Usha, C. Knowledge, attitude and skills of dental practitioners of Puducherry on minimally invasive dentistry concepts: A questionnaire survey. J. Conserv. Dent. 2018, 21, 257–262. [Google Scholar] [CrossRef]
- Hurlbutt, M.; Young, D.A. A best practices approach to caries management. J. Evid. Based Dent. Pr. 2014, 14, 77–86. [Google Scholar] [CrossRef]
- Featherstone, J.D. The caries balance: The basis for caries management by risk assessment. Oral Health Prev. Dent. 2004, 2 (Suppl. 1), 259–264. [Google Scholar]
- Featherstone, J.D.; White, J.M.; Hoover, C.I.; Rapozo-Hilo, M.; Weintraub, J.A.; Wilson, R.S.; Zhan, L.; Gansky, S.A. A randomized clinical trial of anticaries therapies targeted according to risk assessment (caries management by risk assessment). Caries Res. 2012, 46, 118–129. [Google Scholar] [CrossRef]
- Fontana, M.; Gonzalez-Cabezas, C. Secondary caries and restoration replacement: An unresolved problem. Compend. Contin. Educ. Dent. 2000, 21, 15–18. [Google Scholar]
- Takahashi, N.; Nyvad, B. Caries ecology revisited: Microbial dynamics and the caries process. Caries Res. 2008, 42, 409–418. [Google Scholar] [CrossRef]
- Featherstone, J.D. The science and practice of caries prevention. J. Am. Dent. Assoc. (1939) 2000, 131, 887–899. [Google Scholar] [CrossRef]
- Ogaard, B.; Rolla, G. The in vivo orthodontic banding model for vital teeth and the in situ orthodontic banding model for hard-tissue slabs. J. Dent. Res. 1992, 71, 832–835. [Google Scholar] [CrossRef]
- Ripa, L.W. A critique of topical fluoride methods (dentifrices, mouthrinses, operator-, and self-applied gels) in an era of decreased caries and increased fluorosis prevalence. J. Public Health Dent. 1991, 51, 23–41. [Google Scholar] [CrossRef]
- Wiegand, A.; Buchalla, W.; Attin, T. Review on fluoride-releasing restorative materials--fluoride release and uptake characteristics, antibacterial activity and influence on caries formation. Dent. Mater. 2007, 23, 343–362. [Google Scholar] [CrossRef]
- Pandit, S.; Kim, J.E.; Jung, K.H.; Chang, K.W.; Jeon, J.G. Effect of sodium fluoride on the virulence factors and composition of Streptococcus mutans biofilms. Arch. Oral Biol. 2011, 56, 643–649. [Google Scholar] [CrossRef]
- Van der Weijden, G.A.; Timmerman, M.F.; Nijboer, A.; Lie, M.A.; Van der Velden, U. A comparative study of electric toothbrushes for the effectiveness of plaque removal in relation to toothbrushing duration. Timerstudy. J. Clin. Periodontol. 1993, 20, 476–481. [Google Scholar] [CrossRef]
- Nassar, H.M.; Lippert, F.; Eckert, G.J.; Hara, A.T. Dentifrice fluoride and abrasivity interplay on artificial caries lesions. Caries Res. 2014, 48, 557–565. [Google Scholar] [CrossRef]
- Nassar, H.M.; Lippert, F.; Eckert, G.J.; Hara, A.T. Impact of toothbrushing frequency and toothpaste fluoride/abrasivity levels on incipient artificial caries lesion abrasion. J. Dent. 2018, 76, 89–92. [Google Scholar] [CrossRef]
- Jenson, L.; Budenz, A.W.; Featherstone, J.D.; Ramos-Gomez, F.J.; Spolsky, V.W.; Young, D.A. Clinical protocols for caries management by risk assessment. J. Calif. Dent. Assoc. 2007, 35, 714–723. [Google Scholar]
- Anderson, M. Chlorhexidine and xylitol gum in caries prevention. Spec. Care Dent. 2003, 23, 173–176. [Google Scholar] [CrossRef]
- Anderson, M.H. A review of the efficacy of chlorhexidine on dental caries and the caries infection. J. Calif. Dent. Assoc. 2003, 31, 211–214. [Google Scholar]
- Hara, A.T.; Zero, D.T. The caries environment: Saliva, pellicle, diet, and hard tissue ultrastructure. Dent. Clin. N. Am. 2010, 54, 455–467. [Google Scholar] [CrossRef]
- Alstad, T.; Holmberg, I.; Osterberg, T.; Birkhed, D. Associations between oral sugar clearance, dental caries, and related factors among 71-year-olds. Acta Odontol. Scand. 2008, 66, 358–367. [Google Scholar] [CrossRef]
- Touger-Decker, R.; van Loveren, C. Sugars and dental caries. Am. J. Clin. Nutr. 2003, 78, 881S–892S. [Google Scholar] [CrossRef]
- Ly, K.A.; Milgrom, P.; Rothen, M. Xylitol, sweeteners, and dental caries. Pediatric Dent. 2006, 28, 154–163, discussion 192-8. [Google Scholar]
- Makinen, K.K.; Bennett, C.A.; Hujoel, P.P.; Isokangas, P.J.; Isotupa, K.P.; Pape, H.R., Jr.; Makinen, P.L. Xylitol chewing gums and caries rates: A 40-month cohort study. J. Dent. Res. 1995, 74, 1904–1913. [Google Scholar] [CrossRef]
- Trahan, L. Xylitol: A review of its action on mutans streptococci and dental plaque--its clinical significance. Int. Dent. J. 1995, 45 (Suppl. 1), 77–92. [Google Scholar]
- Maguire, A.; Rugg-Gunn, A.J. Xylitol and caries prevention--is it a magic bullet? Br. Dent. J. 2003, 194, 429–436. [Google Scholar] [CrossRef]
- Ghezzi, E.M. Developing pathways for oral care in elders: Evidence-based interventions for dental caries prevention in dentate elders. Gerodontology 2014, 31 (Suppl. 1), 31–36. [Google Scholar] [CrossRef]
- Deshpande, A.; Jadad, A.R. The impact of polyol-containing chewing gums on dental caries: A systematic review of original randomized controlled trials and observational studies. J. Am. Dent. Assoc. (1939) 2008, 139, 1602–1614. [Google Scholar] [CrossRef]
- Nassar, H.M. Xylitol in Chewing Gums. J. Am. Sci. 2017, 13, 60–66. [Google Scholar]
- Featherstone, J.D.B.; Alston, P.; Chaffee, B.W.; Rechmann, P. Caries Management by Risk Assessment (CAMBRA): An Update for Use in Clinical Practice for Patients Aged 6 Through Adult. J. Calif. Dent. Assoc. 2019, 47, 16–25. [Google Scholar]
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).