
Indications and Complications of Subperiosteal Implants: Literature Review and Case Series

 ,
,  ,
, 
 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Review
2.2. Inclusion Criteria
- Human clinical studies, including clinical trials, cohort studies, case-control studies, case series, case reports, review articles, letters, editorials, expert opinions, and systematic reviews.
- Studies evaluating survival rates, osseointegration, or complications of subperiosteal implants.
- Studies comparing subperiosteal implants with conventional implants or alternative treatment modalities.
- English-language publications to ensure accessibility and consistency in interpretation.
- No time restrictions to include both historical and modern studies, allowing for a comprehensive perspective on subperiosteal implants’ evolution and clinical outcomes.
2.3. Exclusion Criteria
- Animal or in vitro studies that lack direct clinical implications.
- Studies focusing solely on technical or laboratory procedures without reporting clinical outcomes.
2.4. Search Strategies and Information Sources
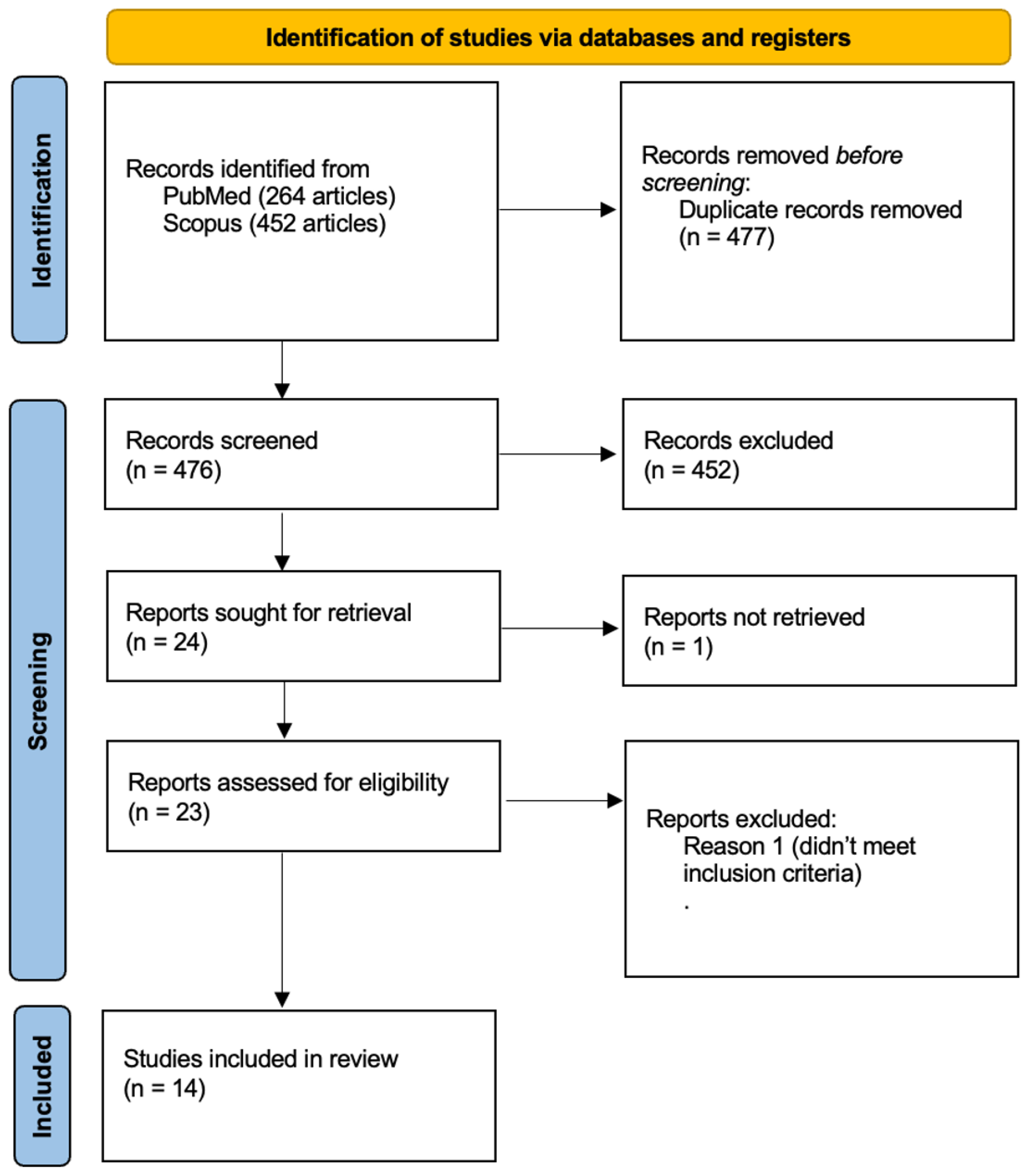
2.5. Article Selection
- Primary Search Results:
- 2.
- Duplicate Removal:
- 3.
- Title and Abstract Screening:
- 4.
- Full-Text Evaluation:
2.6. Data Extraction Process
- Study Characteristics: Author(s), year of publication, study title, journal name, and DOI/link to ensure accurate identification and citation of the sources.
- Study Design and Population: Study design, sample size, and study location/country to assess the methodological quality and generalizability of findings.
- Follow-up and Patient Characteristics: Follow-up period, patient demographics, jaw treated (maxilla, mandible, or both), and bone condition to analyze treatment outcomes in different clinical scenarios.
- Implant Characteristics: Type of implant material and fixation method to compare variations in design and placement techniques.
- Outcome Measures: Reported survival rates and success criteria used in each study to evaluate implant longevity and clinical performance.
- Complications and Prosthetic Considerations: Documented complications, prosthetic type, and patient satisfaction levels to assess functional and patient-reported outcomes.
- Key Findings and Study Limitations: Major conclusions, clinical implications, and limitations noted by the authors to contextualize study results.
2.7. Case Series
2.8. Patient Selection and Preoperative Assessment
- Severe mandibular or maxillary bone atrophy.
- Contraindication to bone grafting or patient refusal of grafting procedures.
- Need for fixed implant-supported rehabilitation.
- Good general health and absence of uncontrolled systemic conditions.
- Presence of active oral infections or untreated periodontal disease.
- Uncontrolled systemic conditions (e.g., diabetes, cardiovascular disease, immunosuppressive disorders) or history of head and neck radiation therapy.
- Severe parafunctional habits (e.g., bruxism) that could compromise implant stability.
- Pregnancy or breastfeeding at the time of treatment.
3. Results
3.1. Literature Review
3.2. Patient Demographics and Clinical Indications
3.3. Follow-Up Periods and Duration of Evaluation
3.4. Survival Rates and Success Criteria
3.5. Complications and Clinical Outcomes
3.6. Postoperative and Early Complications
3.7. Prosthetic Complications
3.8. Long-Term and Late Complications
3.9. Infection and Implant Loss
3.10. Summary of Risk Profile
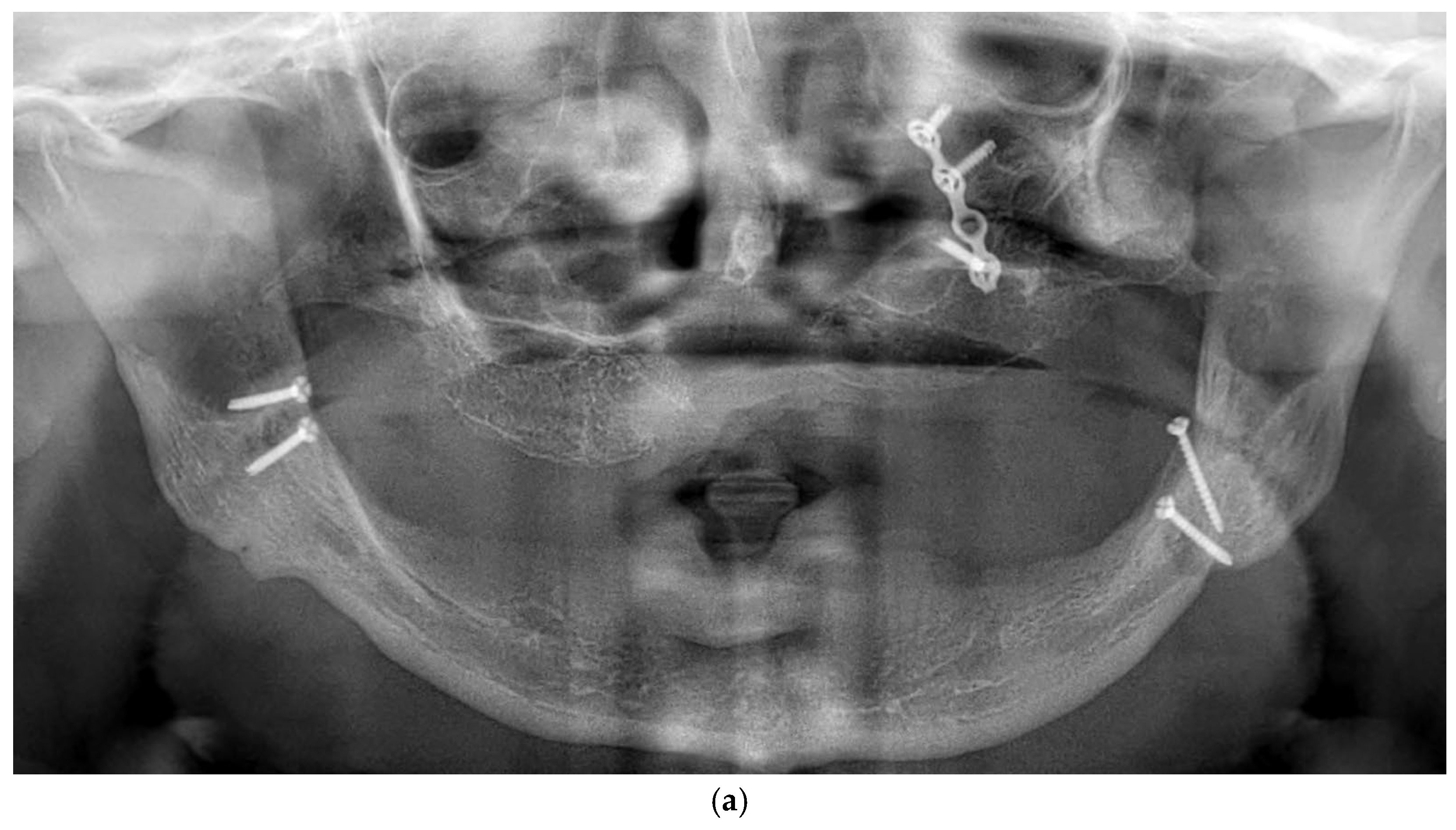
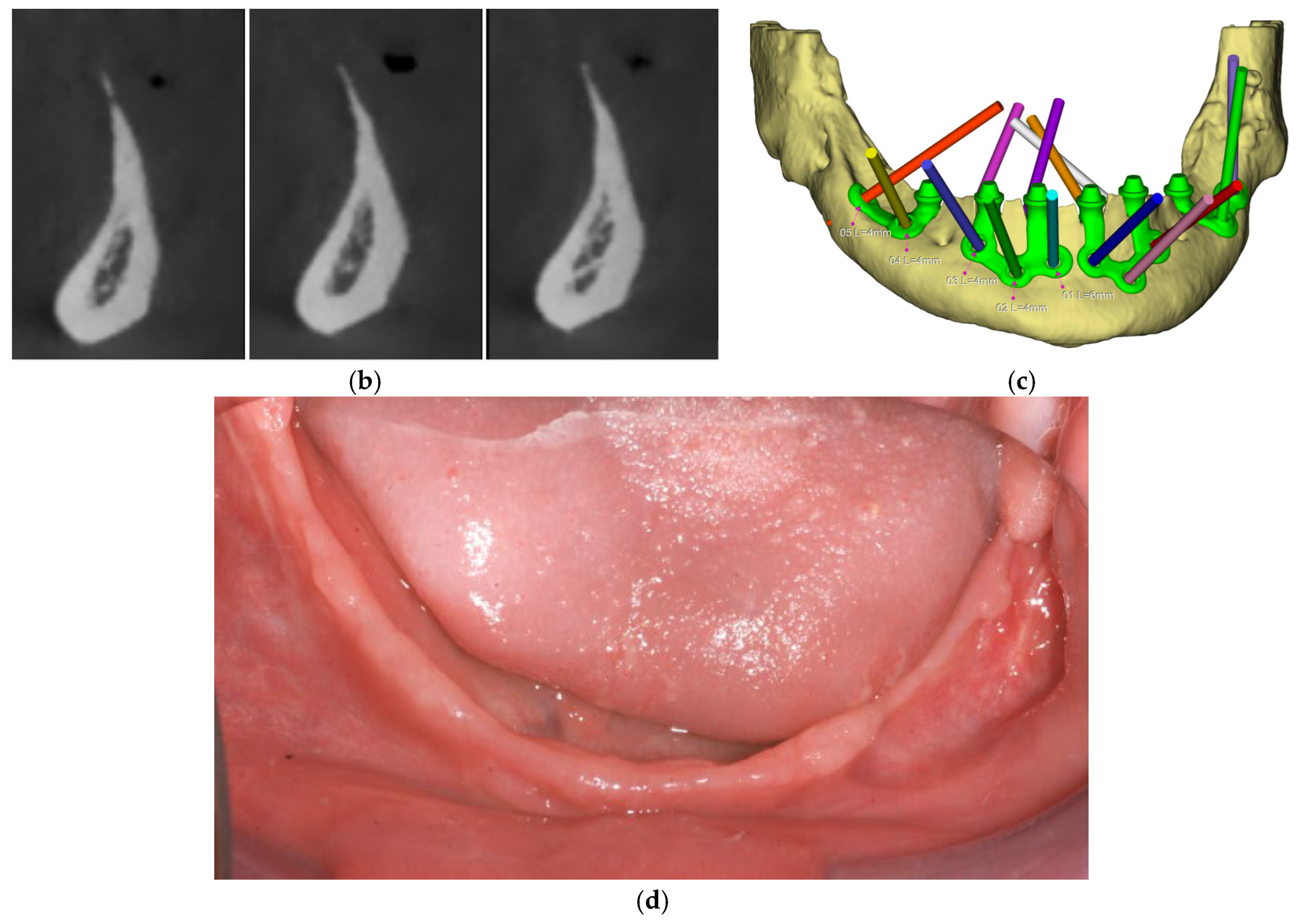
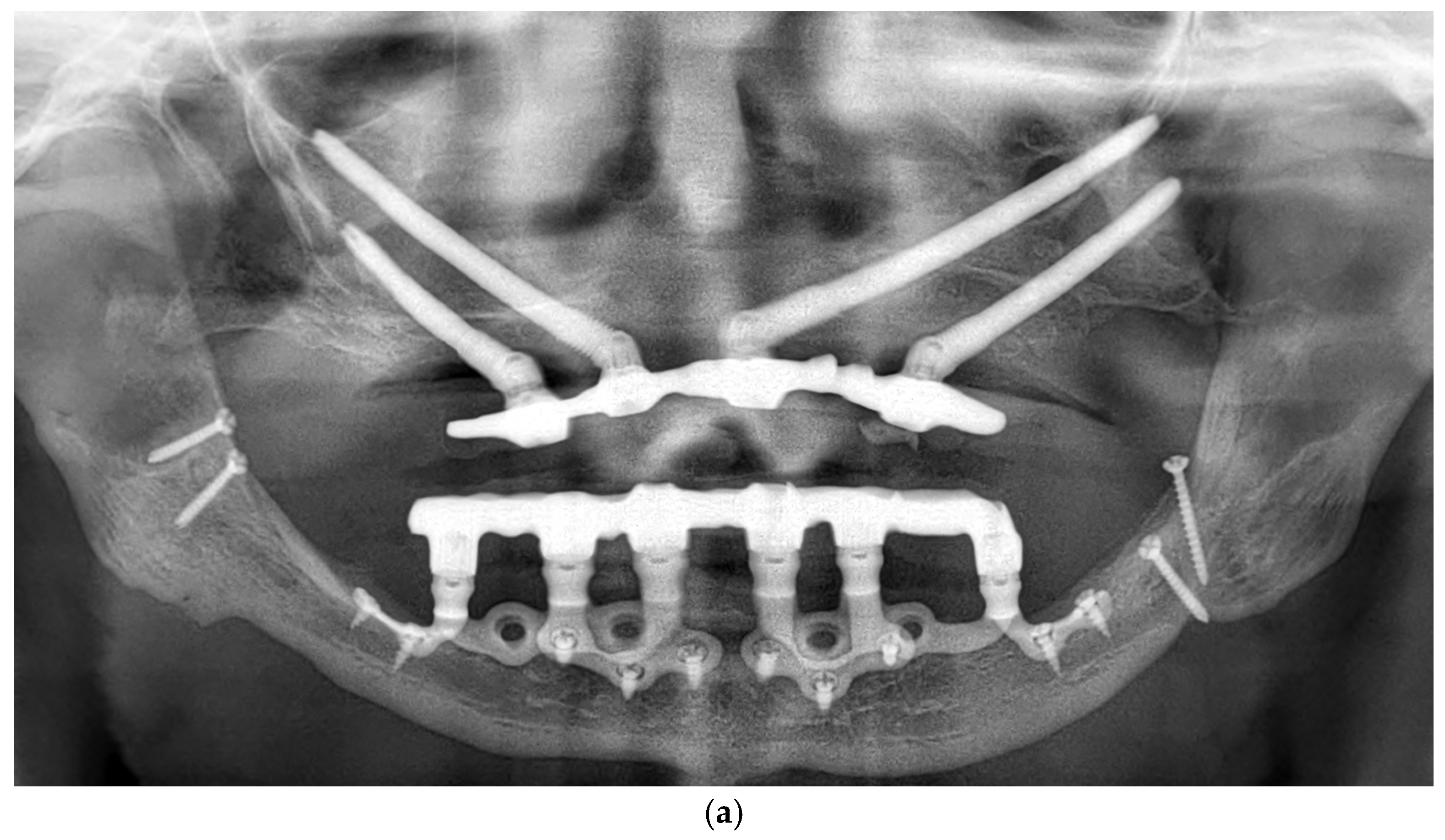
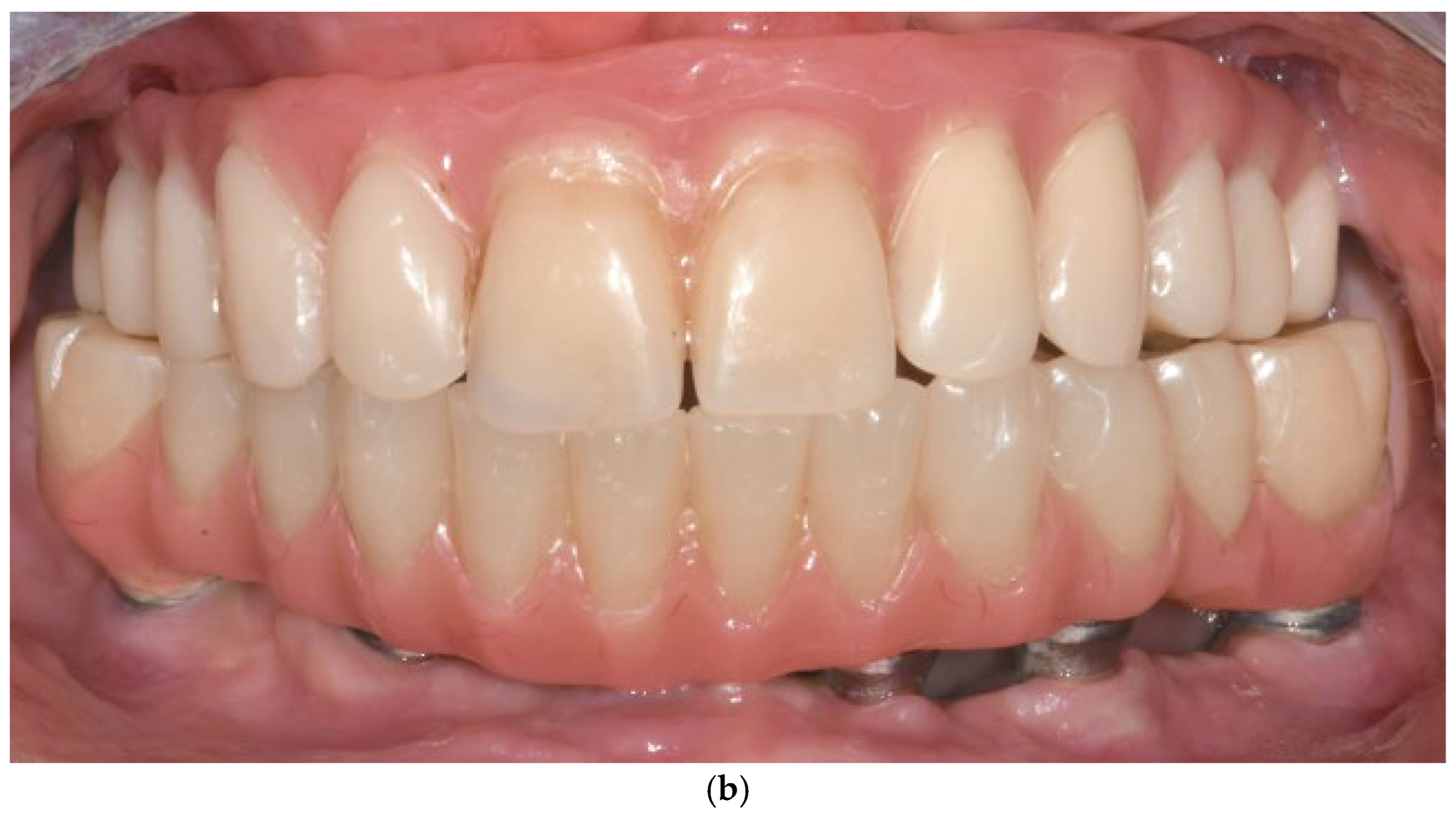
3.11. Case Series
3.11.1. Patient Demographics and Clinical Characteristics
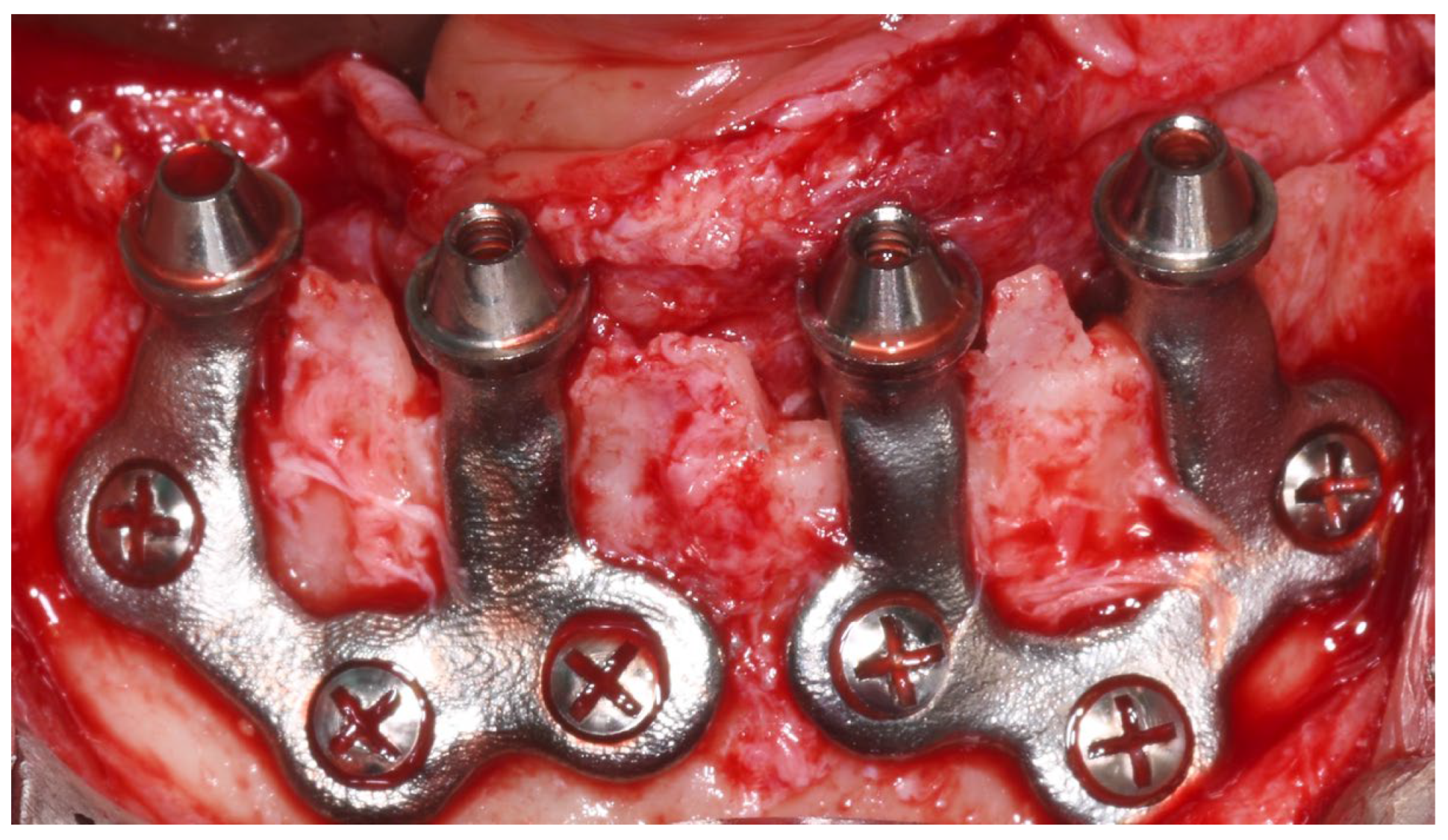
3.11.2. Surgical and Prosthetic Protocol
3.11.3. Complications and Management
- Patient 1: Developed a localized abscess in the region of tooth 13 three months postoperatively, accompanied by soft tissue dehiscence at sites 13, 15, and 17. These were managed with local irrigation and hygiene reinforcement, with full recovery.
- Patient 2: Presented with tissue dehiscence on the lingual side.
- Patient 3: Presented with tissue dehiscence around the second abutment of the upper left implant. The condition was resolved through improved oral hygiene.
4. Discussion
4.1. Patient Selection
- Patients with severe alveolar bone atrophy (Cawood and Howell Class V–VI). (Ideal for those with advanced horizontal and vertical bone loss where standard implants are contraindicated).
- Narrow alveolar crest cases unsuitable for endosseous implants. (Allows rehabilitation without vertical bone reduction. Subperiosteal implant is the only technique that allows for the rehabilitation of narrow bone crests without the loss of vertical height).
- Elderly or systemically stable patients unwilling or unable to undergo bone grafting. (Minimally invasive alternative to augmentative procedures) [50].
4.2. Digital Planning
- Fully digital workflows.
- High-resolution CBCT scan without artifacts. (Provides accurate anatomical data for implant customization).
- Use of prosthetically driven planning software. (Ensures correct abutment angulation and emergence profile).
- Collaborative workflow between surgeon, prosthodontist, and technician. (Aligns surgical feasibility with prosthetic functionality) [26].
4.3. Surgical Technique
- Full-thickness flap elevation with identification of vital structures. (Prevents nerve injury and ensures proper implant bed access).
- Minimal osteoplasty when needed for passive fit. (Improves implant adaptation to the bony surface).
- Fixation with titanium screws at preplanned anchorage points. (Provides mechanical stability without intraosseous engagement).
- Strict aseptic handling of the implant. (Reduces risk of postoperative contamination).
4.4. Implant Manufacturing and Fitting
- High-precision manufacturing and appropriate surface treatments are essential to allow a successful rehabilitation.
- The implant must achieve a passive sitting and fixation, avoiding biomechanical stress on both the structure and fixation screws, as well as the aseptic implant handling [51].
4.5. Prosthetic Design
- Immediate loading with provisional prosthesis (24–72 h post-op). (Supports soft tissue healing and functional rehabilitation).
- Final prosthesis placement after 4 months. (Ensures tissue maturation and long-term durability).
- Passive fit and absence of considerable cantilevers. (Prevents biomechanical overload and prosthetic complications) [52].
4.6. Postoperative Protocols and Long-Term Monitoring
- Scheduled evaluations at 1, 3, and 6 months post-surgery, then annually. (Allows early detection of complications and implant integration monitoring).
- Annual prosthesis removal and peri-implant hygiene assessment. (Enables thorough decontamination and inspection of framework integrity).
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Avila-Ortiz, G.; Chambrone, L.; Vignoletti, F. Effect of alveolar ridge preservation interventions following tooth extraction: A systematic review and meta-analysis. J. Clin. Periodontol. 2019, 46 (Suppl. 21), 195–223, Erratum in J. Clin. Periodontol. 2020, 47, 129. [Google Scholar] [CrossRef] [PubMed]
- Alotaibi, F.F.; Rocchietta, I.; Buti, J.; D’Aiuto, F. Comparative evidence of different surgical techniques for the management of vertical alveolar ridge defects in terms of complications and efficacy: A systematic review and network meta-analysis. J. Clin. Periodontol. 2023, 50, 1487–1519. [Google Scholar] [CrossRef] [PubMed]
- Korn, P.; Gellrich, N.C.; Spalthoff, S.; Jehn, P.; Eckstein, F.; Lentge, F.; Zeller, A.N.; Rahlf, B. Managing the severely atrophic maxilla: Farewell to zygomatic implants and extensive augmentations? J. Stomatol. Oral Maxillofac. Surg. 2022, 123, 562–565. [Google Scholar] [CrossRef] [PubMed]
- Chiapasco, M.; Casentini, P. Horizontal bone-augmentation procedures in implant dentistry: Prosthetically guided regeneration. Periodontology 2000 2018, 77, 213–240. [Google Scholar] [CrossRef] [PubMed]
- Chiapasco, M.; Casentini, P.; Zaniboni, M. Bone augmentation procedures in implant dentistry. Int. J. Oral Maxillofac. Implant. 2009, 24, 237. [Google Scholar]
- Corbella, S.; Taschieri, S.; Del Fabbro, M. Long-term outcomes for the treatment of atrophic posterior maxilla: A systematic review of literature. Clin. Implant. Dent. Relat. Res. 2015, 17, 120–132. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Barausse, C.; Balercia, A.; Pistilli, R.; Ippolito, D.R.; Felice, P. Conventional drills vs piezoelectric surgery preparation for placement of four immediately loaded zygomatic oncology implants in edentulous maxillae: Results from 1-year split-mouth randomised controlled trial. Eur. J. Oral Implantol. 2017, 10, 147–158. [Google Scholar] [PubMed]
- Felice, P.; Pistilli, R.; Piattelli, M.; Soardi, E.; Pellegrino, G.; Corvino, V.; Esposito, M. 1-stage versus 2-stage lateral maxillary sinus lift procedures: 4-month post-loading results of a multicenter randomised controlled trial. Eur. J. Oral Implantol. 2013, 6, 153–165. [Google Scholar] [PubMed]
- Esposito, M.; Barausse, C.; Pistilli, R.; Checchi, V.; Diazzi, M.; Gatto, M.R.; Felice, P. Posterior jaws rehabilitated with partial prostheses supported by 4.0 x 4.0 mm or by longer implants: Four-month post-loading data from a randomised controlled trial. Eur. J. Oral Implantol. 2015, 8, 221–230. [Google Scholar] [PubMed]
- Cucchi, A.; Vignudelli, E.; Fiorino, A.; Pellegrino, G.; Corinaldesi, G. Vertical ridge augmentation (VRA) with Ti-reinforced d-PTFE membranes or Ti meshes and collagen membranes: 1-year results of a randomized clinical trial. Clin. Oral Implant. Res. 2021, 32, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Pellegrino, G.; Lizio, G.; Corinaldesi, G.; Marchetti, C. Titanium Mesh Technique in Rehabilitation of Totally Edentulous Atrophic Maxillae: A Retrospective Case Series. J. Periodontol. 2016, 87, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Chrcanovic, B.R.; Pedrosa, A.R.; Custódio, A.L.N. Zygomatic implants: Critical review of surgical techniques. Oral Maxillofac. Surg. 2013, 17, 1–9. [Google Scholar] [CrossRef] [PubMed]
- De Bruyn, H.; Raes, S.; Östman, P.O.; Cosyn, J. Immediate loading in edentulous jaws: Literature review with clinical guidelines. Periodontology 2000 2014, 66, 153–187. [Google Scholar] [CrossRef] [PubMed]
- Keleş, H.G.; Karaca, Ç. Stress distribution among standard, zygomatic and subperiosteal implants in the atrophic maxilla: 3-D FEA. Int. J. Oral Maxillofac. Implant. 2023, 38, 347–356. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E.; Alkhraisat, M.H. Clinical performance of short implants supporting single crowns: Cement vs screw retention. Int. J. Oral Maxillofac. Implant. 2019, 34, 969–976. [Google Scholar] [CrossRef] [PubMed]
- Fernández, H.; Gómez-Delgado, A.; Trujillo-Saldarriaga, S.; Varón-Cardona, D.; Castro-Núñez, J. Zygomatic implants for the management of the severely atrophied maxilla: A retrospective analysis of 244 implants. J. Oral Maxillofac. Surg. 2014, 72, 887–891. [Google Scholar] [CrossRef] [PubMed]
- Stacchi, C.; Andolsek, F.; Berton, F.; Perinetti, G.; Navarra, C.O.; Di Lenarda, R. Intraoperative Complications During Sinus Floor Elevation with Lateral Approach: A Systematic Review. Int. J. Oral Maxillofac. Implant. 2017, 32, e107–e118. [Google Scholar] [CrossRef] [PubMed]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Survival and Complications of Zygomatic Implants: An Updated Systematic Review. J. Oral Maxillofac. Surg. 2016, 74, 1949–1964. [Google Scholar] [CrossRef] [PubMed]
- Fontana, F.; Maschera, E.; Rocchietta, I.; Simion, M. Classification of complications in guided bone regeneration with non-resorbable membrane. Int. J. Periodontics Restor. Dent. 2011, 31, 265–273. [Google Scholar]
- Molina, A.; Sanz-Sánchez, I.; Sanz-Martín, I.; Ortiz-Vigón, A.; Sanz, M. Complications in sinus lifting: Classification and management. Periodontology 2000 2022, 88, 103–115. [Google Scholar] [CrossRef] [PubMed]
- Urban, I.A.; Montero, E.; Monje, A.; Sanz-Sánchez, I. Effectiveness of vertical ridge augmentation interventions: A systematic review and meta-analysis. J. Clin. Periodontol. 2019, 46 (Suppl. 21), 319–339. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E.; Alkhraisat, M.H. 15-year follow-up of short dental implants placed in the partially edentulous patient: Mandible Vs. maxilla. Ann. Anat. 2019, 222, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Vetromilla, B.M.; Mazzetti, T.; Pereira-Cenci, T. Short versus standard implants associated with sinus floor elevation: An umbrella review of meta-analyses of multiple outcomes. J. Prosthet. Dent. 2021, 126, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Stefanelli, L.V.; Franchina, A.; Pranno, A.; Pellegrino, G.; Ferri, A.; Pranno, N.; Di Carlo, S.; De Angelis, F. Use of Intraoral Scanners for Full Dental Arches: Could Different Strategies or Overlapping Software Affect Accuracy? Int. J. Environ. Res. Public Health 2021, 18, 9946. [Google Scholar] [CrossRef] [PubMed]
- De Moor, E.; Huys, S.E.F.; van Lenthe, G.H.; Mommaerts, M.Y.; Vander Sloten, J. Finite-element evaluation of a patient-specific AMSJI. Int. J. Oral Maxillofac. Surg. 2022, 51, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Pellegrino, G.; Karaban, M.; Scalchi, V.; Urbani, M.; Giudice, A.; Barausse, C.; Felice, P. Finite Element Analysis of Functionally Loaded Subperiosteal Implants Evaluated on a Realistic Model Reproducing Severe Atrophic Jaws. Methods Protoc. 2025, 8, 8. [Google Scholar] [CrossRef] [PubMed]
- Cipollina, A.; Ceddia, M.; Di Pietro, N.; Inchingolo, F.; Tumedei, M.; Romasco, T.; Piattelli, A.; Specchiulli, A.; Trentadue, B. Finite Element Analysis (FEA) of a Premaxillary Device: A New Type of Subperiosteal Implant to Treat Severe Atrophy of the Maxilla. Biomimetics 2023, 8, 336. [Google Scholar] [CrossRef] [PubMed]
- Kundakcioglu, A.; Ayhan, M. Subperiosteal implant thickness: Mechanical strength and bone stress by finite element analysis. Int. J. Med. Sci. 2024, 21, 1672–1680. [Google Scholar] [CrossRef] [PubMed]
- Buser, D.; Sennerby, L.; De Bruyn, H. Modern implant dentistry based on osseointegration: 50 years of progress, current trends and open questions. Periodontol. 2000 2017, 73, 7–21. [Google Scholar] [CrossRef] [PubMed]
- Mommaerts, M.Y. Evolutionary steps in the design and biofunctionalization of the additively manufactured sub-periosteal jaw implant ‘AMSJI’ for the maxilla. Int. J. Oral Maxillofac. Surg. 2019, 48, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.J.; Hansen, P.A. 18-year retrospective review of subperiosteal implants in severely atrophied edentulous mandibles. J. Prosthet. Dent. 2004, 92, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Vatteroni, E.; Covani, U.; Menchini Fabris, G.B. The New Generation of Subperiosteal Implants for Patient-Specific Treatment of Atrophic Dental Arches: Literature Review and Two Case Reports. Int. J. Periodontics Restor. Dent. 2023, 43, 735–741. [Google Scholar] [CrossRef] [PubMed]
- Van den Borre, C.; Rinaldi, M.; De Neef, B.; Loomans, N.A.J.; Nout, E.; Van Doorne, L.; Naert, I.; Politis, C.; Schouten, H.; Klomp, G.; et al. Outcomes for AMSJI in the maxilla: Multicentre 1-year follow-up. Int. J. Oral Maxillofac. Surg. 2022, 51, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Herce-López, J.; Pingarrón, M.D.C.; Tofé-Povedano, Á.; García-Arana, L.; Espino-Segura-Illa, M.; Sieira-Gil, R.; Rodado-Alonso, C.; Sánchez-Torres, A.; Figueiredo, R. Customized Subperiosteal Implants for the Rehabilitation of Atrophic Jaws: A Consensus Report and Literature Review. Biomimetics 2024, 9, 61. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cerea, M.; Dolcini, G.A. Custom-made direct metal laser sintering titanium sub-periosteal implants: A retrospective clinical study on 70 patients. BioMed Res. Int. 2018, 2018, 5420391. [Google Scholar] [CrossRef] [PubMed]
- Mangano, C.; Bianchi, A.; Mangano, F.G.; Dana, J.; Colombo, M.; Solop, I.; Admakin, O. Custom-made 3D printed subperiosteal titanium implants for the prosthetic restoration of the atrophic posterior mandible of elderly patients: A case series. 3D Print. Med. 2020, 6, 1. [Google Scholar] [CrossRef] [PubMed]
- Strappa, E.M.; Memè, L.; Cerea, M.; Roy, M.; Bambini, F. Custom-made additively manufactured subperiosteal implant. Minerva Dent. Oral Sci. 2022, 71, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Nemtoi, A.; Covrig, V.; Nemtoi, A.; Stoica, G.; Vatavu, R.; Haba, D.; Zetu, I. Custom-Made Direct Metal Laser Sintering Titanium Subperiosteal Implants in Oral and Maxillofacial Surgery for Severe Bone-Deficient Patients-A Pilot Study. Diagnostics 2022, 12, 2531. [Google Scholar] [CrossRef] [PubMed]
- Marconcini, S.; Giammarinaro, E.; Covani, U. The rehabilitation of the atrophic posterior maxilla with a custom-made subperiosteal implant in a patient with a history of medications related to osteonecrosis of the jaws: One-year case report. Oral Maxillofac. Surg. Cases 2023, 9, 100292. [Google Scholar] [CrossRef]
- Onică, N.; Budală, D.G.; Baciu, E.R.; Onică, C.A.; Gelețu, G.L.; Murariu, A.; Balan, M.; Pertea, M.; Stelea, C. Long-Term Clinical Outcomes of 3D-Printed Subperiosteal Titanium Implants: A 6-Year Follow-Up. J. Pers. Med. 2024, 14, 541. [Google Scholar] [CrossRef] [PubMed]
- Ayhan, M.; Yey Özkeskin, S.Z. Rehabilitation of Severely Atrophic Maxilla with Le Fort I Advancement Surgery and Subperiosteal Implant in a Patient With Ectodermal Dysplasia. J. Craniofacial Surg. 2024, 35, e484–e486. [Google Scholar] [CrossRef] [PubMed]
- Gellrich, N.C.; Korn, P.; Jehn, P.; Neuhaus, M.; Lentge, F.; Rahlf, B. Exceptional Cases Demand Exceptional Personalized Solutions: The Next Level in Dental Rehabilitation. J. Pers. Med. 2024, 14, 294. [Google Scholar] [CrossRef] [PubMed]
- Ayhan, M.; Ozturk Muhtar, M.; Kundakcioglu, A.; Kucukcakir, O.; Cansiz, E. Evaluation of Clinical Success of the 3D-Printed Custom-Made Subperiosteal Implants. J. Craniofacial Surg. 2024, 35, 1146–1151. [Google Scholar] [CrossRef] [PubMed]
- Vaira, L.A.; Biglio, A.; Favro, A.; Salzano, G.; Abbate, V.; Lechien, J.R.; De Riu, G. Implant-prosthetic rehabilitation of the atrophic posterior mandible with additively manufactured custom-made subperiosteal implants: A cohort study. Int. J. Oral Maxillofac. Surg. 2024, 53, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E.; Eguia, A.; Staudigl, C.; Alkhraisat, M.H. Clinical performance of additively manufactured subperiosteal implants: A systematic review. Int. J. Implant. Dent. 2024, 10, 4. [Google Scholar] [CrossRef] [PubMed]
- El-Sawy, M.A.; Hegazy, S.A. Subperiosteal implants constructed with digital technology: A systematic review. Oral Maxillofac. Surg. 2024, 28, 1063–1075. [Google Scholar] [CrossRef] [PubMed]
- Zielinski, R.; Okulski, J.; Piechaczek, M.; Łoś, J.; Sowiński, J.; Sadowska-Sowińska, M.; Kołkowska, A.; Simka, W.; Kozakiewicz, M. Five-Year Comparative Study of Zygomatic and Subperiosteal Implants: Clinical Outcomes, Complications, and Treatment Strategies for Severe Maxillary Atrophy. J. Clin. Med. 2025, 14, 661. [Google Scholar] [CrossRef] [PubMed]
- Santiago, P.H.; Tavares, M.G.; Grillo, R. Personalized Rehabilitation of Atrophic Customized Subperiosteal Implants. J. Craniofacal Surg. 2025, 36, e20–e22. [Google Scholar] [CrossRef] [PubMed]
- Cawood, J.I.; Howell, R.A. A classification of the edentulous jaws. Int. J. Oral Maxillofac. Surg. 1988, 17, 232–236. [Google Scholar] [CrossRef] [PubMed]
- Vatteroni, E.; Toti, P.; Covani, U.; Crespi, R.; Cosola, S.; Menchini-Fabris, G.B. A Retrospective Radiological and Clinical Survey of Full-Arch Immediate Fixed Prostheses Supported by Custom-Made Three- Dimensional Printed Subperiosteal Titanium Implants in Patients with Severe Atrophic Jaws: Implant Success Code. Int. J. Oral Maxillofac. Implant. 2025, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Vaira, L.A.; Biglio, A.; Salzano, G.; Lechien, J.R.; De Riu, G. Additively manufactured custom-made subperiosteal implant rehabilitation for severely atrophic maxillary molar area: A technical note. J. Stomatol. Oral Maxillofac. Surg. 2024, 125 (Suppl. 1), 101917. [Google Scholar] [CrossRef] [PubMed]
- Felice, P.; Bertacci, A.; Bonifazi, L.; Karaban, M.; Canullo, L.; Pistilli, R.; Sammartino, P.; Gasparro, R.; Barausse, C. A Proposed Protocol for Ordinary and Extraordinary Hygienic Maintenance in Different Implant Prosthetic Scenarios. Appl. Sci. 2021, 11, 2957. [Google Scholar] [CrossRef]
- Monje, A.; Aranda, L.; Diaz, K.T.; Alarcón, M.A.; Bagramian, R.A.; Wang, H.L.; Catena, A. Impact of maintenance therapy on prevention of peri-implant diseases: Systematic review and meta-analysis. J. Dent. Res. 2016, 95, 372–379. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author(s), Year | Study Design | Sample | Average Age | Population | Systemic Conditions | Follow-Up | Implant Type/ Implant Brand | Survival | Success Criteria | Complications |
|---|---|---|---|---|---|---|---|---|---|---|
| Cerea & Dolcini, 2018 [36] | Retrospective | 70 | 67.8 | Elderly with jaw atrophy | Excluded smokers and bruxists | 2 years | Custom-made DMLS titanium; surface not specified; (Eagle-Grid, BTK, Dueville, Vicenza); polished surface | 95.8% | Implant and restoration function | 5.7% postop symptoms; 1.4% infection; 8.9% prosthetic issues |
| Mangano et al., 2020 [37] | Case Series | 10 | 69.6 | Elderly, mandibular atrophy | N/R | 1 year | Custom 3D-printed titanium (DMLS); (Iuxta3D ®, BTK, Dueville, Vicenza, Italy); porous surface | 100% | Stable fit, no infection | 10% discomfort; 20% provisional fractures |
| Strappa et al., 2022 [38] | Case Report | 1 | 67 | 67 y/o female, maxillary atrophy | None | 2 years | DMLS titanium alloy; (Eagle-Grid, Eagle-Grid S.r.l., Bergamo, Italia) | 100% | No complications | None |
| Nemtoi et al., 2022 [39] | Pilot Study | 16 | N/R | Severe resorption | 2 diabetes; 1 cardiovascular case | Several months | DMLS titanium (CBCT-designed); (3D Medica SABETTIMED® and Bone Easy®; polished and rough surface | 93.75% | Stability, integration | 1 failure due to infection |
| Marconcini et al., 2023 [40] | Case Report | 1 | 72 | Elderly, osteoporosis | Osteoporosis | 1 year | 3D-printed titanium; (3Dfast srl, Padova (Italy); porous surface | 100% | Implant stability | None |
| Onică et al., 2024 [41] | Retrospective | 36 | 59.7 | Edentulous, severe atrophy | NR | 6 years | CAD/CAM titanium; (Sisma S.p.A., Piovene Rocchette, Italy) | ~25% | Long-term function without complications | Early exposure, mobility in 27/36 cases |
| Ayhan et al., 2024 [42] | Case Report | 1 | 18 | 18 y/o, ectodermal dysplasia | Ectodermal dysplasia | N/A | Custom DMLS titanium; polished and rough surface | N/A | Oral function restoration | None reported |
| Gellrich et al., 2024 [43] | Case Series | 4 | N/R | Severe bone loss | Not specified | Up to 68 mo | Patient-specific titanium framework; IPS Implants. Preprosthetic (KLS Martin Group, Tuttlingen, Germany); polished surface | 100% | Stability maintained | None |
| Ayhan et al., 2024 [44] | Retrospective | 31 | N/R | Severe bone loss | NR | 15 months | 3D-printed titanium; NR | 86.7% | Function, adaptation | Fit issues (23); soft tissue (12); infections (5) |
| Vaira et al., 2024 [45] | Retrospective | 17 | 61.5 | Posterior mandible atrophy | N/R | 7–53 mo | DMLS double-laser titanium; (B&B Dental, San Pietro in Casale, Italy); porous surface | 100% | Stable implants | Hypoesthesia (transient); edema |
| Anitua et al., 2024 [46] | Systematic Review | 227 | N/R | Bone atrophy | Included diabetes, cardiovascular, smoking | 21.4 mo | Various, mainly titanium; N/A | 97.8% | Functionality maintained | 25.6% exposure; 7.5% postop issues |
| El-Sawy & Hegazy, 2024 [47] | Systematic Review | 302 | N/R | Atrophic jaws incl. med. compromised | Included diabetes, hypertension, cancer | 17.2 mo | Titanium/PEEK blends in some studies; N/A | 95.3% | Functional with minor issues | 11.5% bio issues; 5.9% prosthetic problems |
| Zielinski et al., 2025 [48] | Comparative Study | 150 | N/R | Maxillary atrophy | Included smokers and immunocompromised | ≥5 years | CAD titanium; roughened surface in select designs; Mai Implant® (Integra Implants®, Lodz, Poland) | 97.1% | Clinical and prosthetic stability | 5.6% peri-implantitis |
| Santiago et al., 2025 [49] | Case Series | 3 | 62.3 | Maxillary atrophy | N/R | 6 months | Custom-designed titanium | High | Stability, patient satisfaction | None observed |
| Patient | Sex | Age | Early Complications (≤3 months) | Late Complications (>3 months) | Management |
|---|---|---|---|---|---|
| 1 | M | 68 | Abscess in zone 13 at 3 months | Mucosal dehiscence at 13, 15, 17 | Antibiotics, soft tissue monitoring |
| 2 | M | 27 | None | Mucosal dehiscence (lingually) | Improved hygiene |
| 3 | M | 55 | None | Mucosal dehiscence (upper left implant, 2nd abutment) | Improved hygiene |
| 4 | F | 69 | None | None | N/A |
| 5 | M | 54 | None | None | N/A |
| 6 | F | 60 | None | None | N/A |
| 7 | F | 63 | None | None | N/A |
| 8 | F | 76 | None | None | N/A |
| 9 | F | 64 | None | None | N/A |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pellegrino, G.; Karaban, M.; Barausse, C.; Giudice, A.; Antonelli, A.; Pistilli, R.; Felice, P. Indications and Complications of Subperiosteal Implants: Literature Review and Case Series. Dent. J. 2025, 13, 337. https://doi.org/10.3390/dj13080337
Pellegrino G, Karaban M, Barausse C, Giudice A, Antonelli A, Pistilli R, Felice P. Indications and Complications of Subperiosteal Implants: Literature Review and Case Series. Dentistry Journal. 2025; 13(8):337. https://doi.org/10.3390/dj13080337
Chicago/Turabian StylePellegrino, Gerardo, Maryia Karaban, Carlo Barausse, Amerigo Giudice, Alessandro Antonelli, Roberto Pistilli, and Pietro Felice. 2025. "Indications and Complications of Subperiosteal Implants: Literature Review and Case Series" Dentistry Journal 13, no. 8: 337. https://doi.org/10.3390/dj13080337
APA StylePellegrino, G., Karaban, M., Barausse, C., Giudice, A., Antonelli, A., Pistilli, R., & Felice, P. (2025). Indications and Complications of Subperiosteal Implants: Literature Review and Case Series. Dentistry Journal, 13(8), 337. https://doi.org/10.3390/dj13080337