


The Success of Endodontic Treatments Performed by Dental Residents in Advanced Education in General Dentistry Program: A 10-Year Retrospective Study

 ,
,  , ,
, , 
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
- Had permanent, fully developed teeth.
- Underwent initial NSRCT by AEGD residents at EIOH within the specified date range.
- Had complete radiographic documentation: pre-treatment periapical (PA) X-ray, PA X-ray at the completion of RCT, and a bitewing (if restored with a crown).
- Had a documented recall examination (EXAM05) in axiUm.
- Completed a minimum of 12 months of follow-up from the date of the final restoration to the documented recall visit.
- They had immature teeth at the time of treatment.
- Their follow-up duration was less than 12 months.
- Required radiographic documentation was incomplete or missing.
2.3. Resident Calibration and Data Quality
2.4. Data Collection and Variables
- Technique used: Hand filing, rotary instruments, or both.
- Tooth classification: Anterior, premolar, or molar; maxillary or mandibular.
- Radiographic data: Quality of obturation, presence of pre- and post-operative radiolucency.
- Pain scores: Using the Visual Analog Scale (VAS).
- Type of final restoration: Amalgam, composite, or crown.
- Timing of final restoration: Number of days between RCT completion and restoration placement.
- Patient-reported satisfaction: Esthetics, function, occlusion, overall experience (0–10 Likert scale).
2.5. Outcome Assessment
- Clinical: Absence of pain, swelling, sinus tract, and sensitivity to percussion or palpation.
- Radiographic: Absence or reduction in periapical radiolucency.
- Functional: Retention of the treated tooth without complications for ≥12 months after restoration.
2.6. Criteria for Evaluation
3. Statistical Analysis
Sample Size
4. Results
4.1. Characteristics of the Cohort
4.2. Treatment Protocol Used in AEGD Clinic
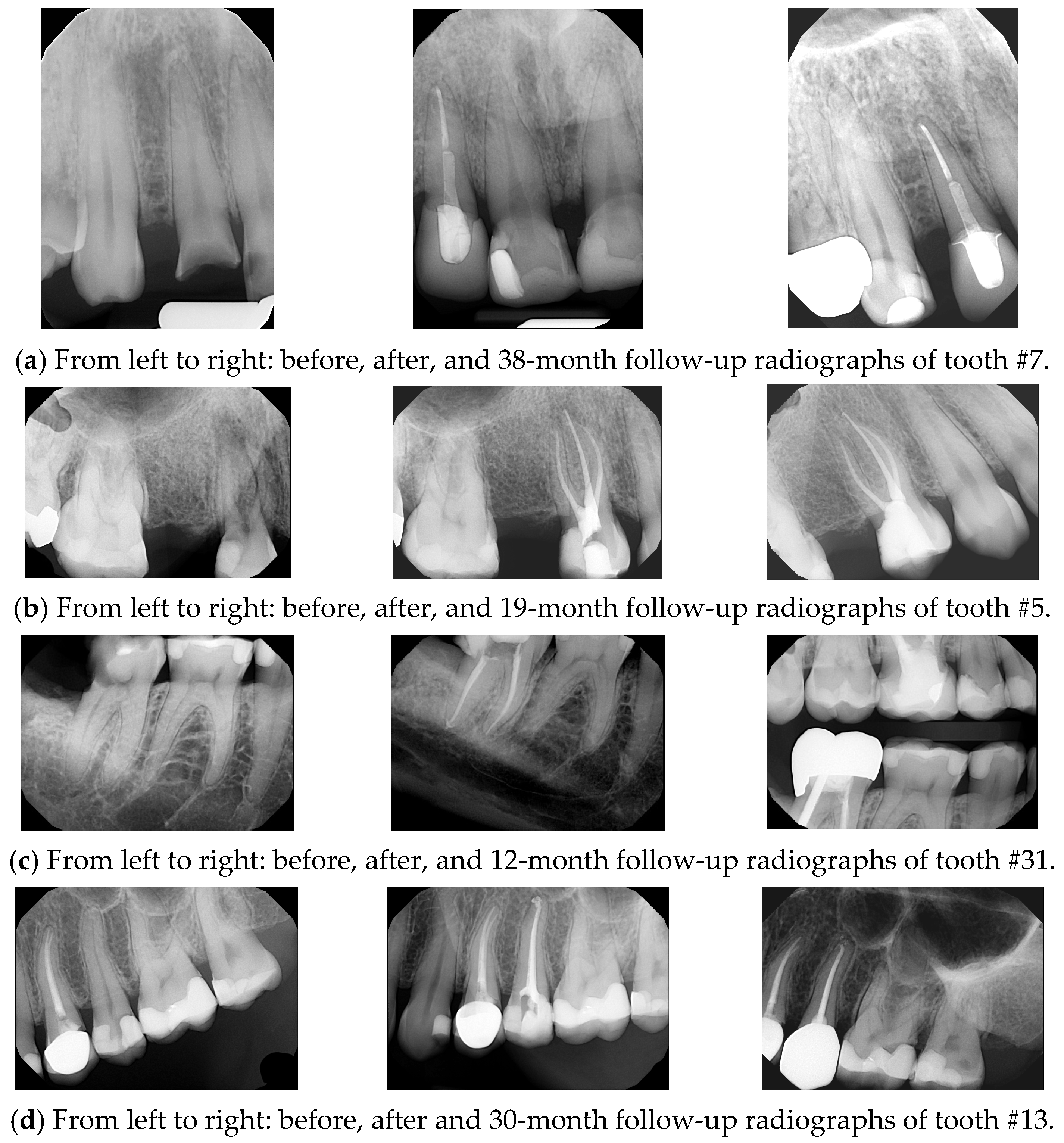
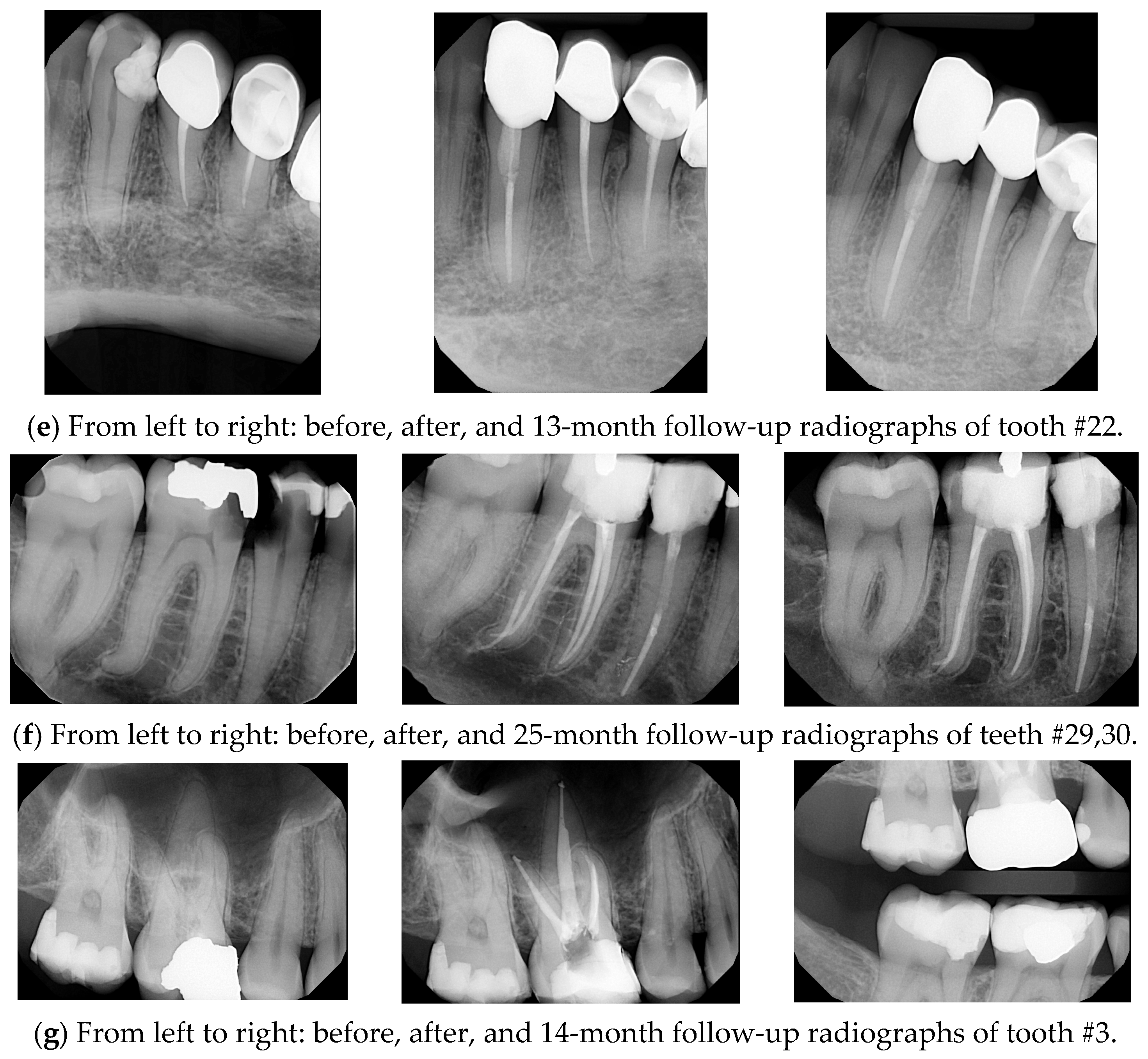
4.3. Treatment Outcomes and Success Rate
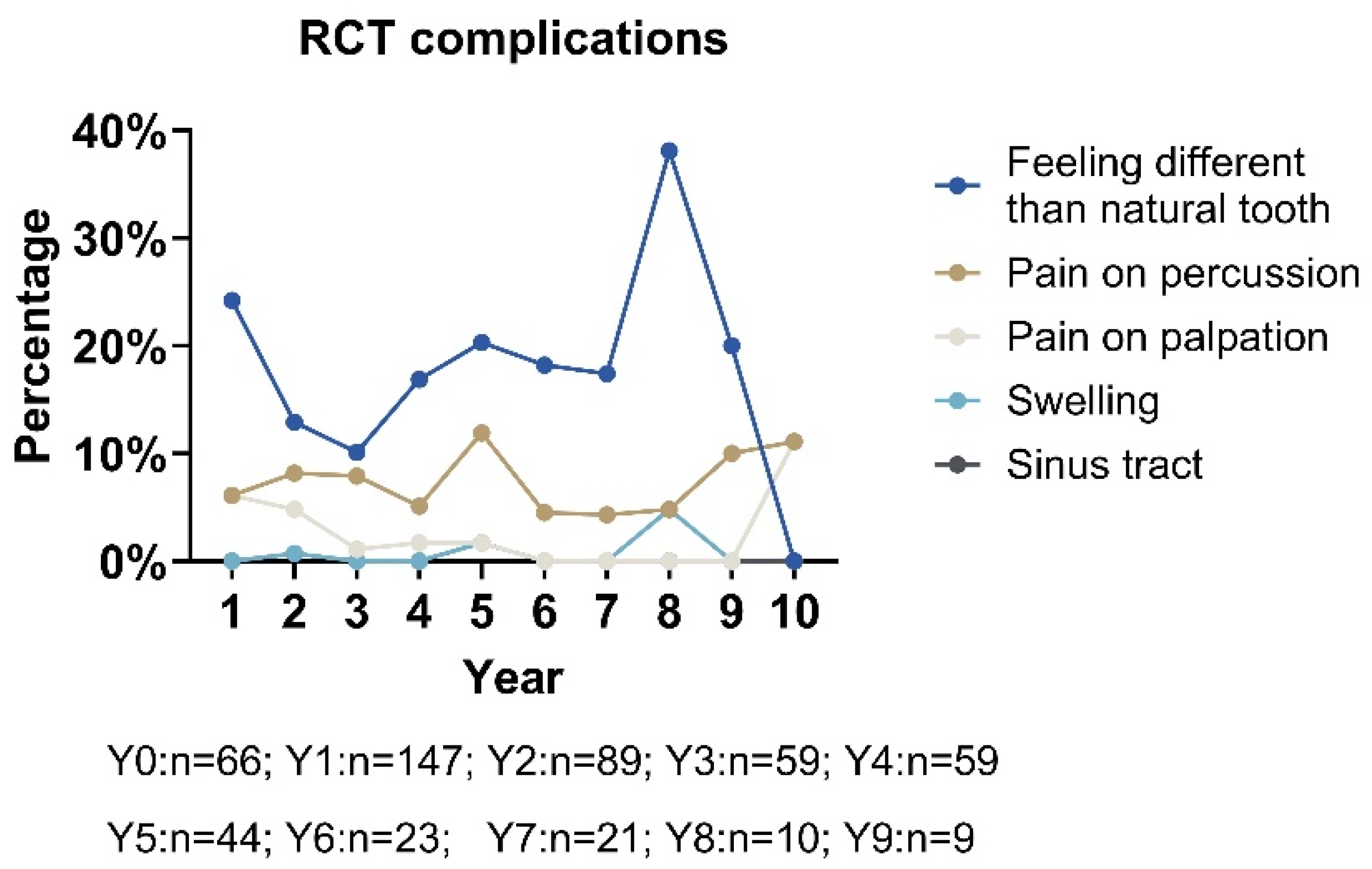
4.4. Complications of RCT
4.5. Impact of Restoration Type and Integrity on Treatment Success and Patient
4.6. Predictive Factors Related to RCT Outcomes
Predictive Factors for RCT Outcomes When the Tooth Is Present
4.7. Predictive Factors for Pain on Percussion
4.8. Predictive Factors for Patient Satisfaction with Esthetics
4.9. Predictive Factors for Patient Satisfaction with Function
4.10. Predictive Factors for Patient Satisfaction with Occlusion
5. Discussions
5.1. Comparisons of RCT Success Rate to Published Studies
5.2. Comparisons of RCT Complications to Published Studies
5.3. The Impact of Pre-Existing Conditions, Periodontal Health, and Restoration Integrity on Patient Satisfaction with RCT Outcomes
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mordohai, N.; Reshad, M.; Jivraj, S.; Chee, W. Factors that affect individual tooth prognosis and choices in contemporary treatment planning. Br. Dent. J. 2007, 202, 63–72. [Google Scholar] [CrossRef] [PubMed]
- American Association of Endodontists. Guide to Clinical Endodontics [Internet], 5th ed.; American Association of Endodontists: Chicago, IL, USA, 2013; Available online: https://www.aae.org/specialty/clinical-resources/guide-clinical-endodontics/ (accessed on 27 June 2025).
- Burry, J.C.; Stover, S.; Eichmiller, F.; Bhagavatula, P. Outcomes of Primary Endodontic Therapy Provided by Endodontic Specialists Compared with Other Providers. J. Endod. 2016, 42, 702–705. [Google Scholar] [CrossRef] [PubMed]
- Saunders, W.P.; Saunders, E.M.; Sadiq, J.; Cruickshank, E. Technical standard of root canal treatment in an adult Scottish sub-population. Br. Dent. J. 1997, 182, 382–386. [Google Scholar] [CrossRef]
- Benenati, F.W.; Khajotia, S.S. A radiographic recall evaluation of 894 endodontic cases treated in a dental school setting. J. Endod. 2002, 28, 391–395. [Google Scholar] [CrossRef]
- Alley, B.S.; Kitchens, G.G.; Alley, L.W.; Eleazer, P.D. A comparison of survival of teeth following endodontic treatment performed by general dentists or by specialists. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2004, 98, 115–118. [Google Scholar] [CrossRef]
- Friedman, S.; Abitbol, S.; Lawrence, H.P. Treatment outcome in endodontics: The Toronto Study. Phase 1: Initial treatment. J. Endod. 2003, 29, 787–793. [Google Scholar] [CrossRef] [PubMed]
- de Chevigny, C.; Dao, T.T.; Basrani, B.R.; Marquis, V.; Farzaneh, M.; Abitbol, S.; Friedman, S. Treatment outcome in endodontics: The Toronto study—Phase 4: Initial treatment. J. Endod. 2008, 34, 258–263. [Google Scholar] [CrossRef]
- Burns, L.E.; Kim, J.; Wu, Y.; Alzwaideh, R.; McGowan, R.; Sigurdsson, A. Outcomes of primary root canal therapy: An updated systematic review of longitudinal clinical studies published between 2003 and 2020. Int. Endod. J. 2022, 55, 714–731. [Google Scholar] [CrossRef]
- Lazarski, M.P.; Walker, W.A.; Flores, C.M., 3rd; Schindler, W.G.; Hargreaves, K.M. Epidemiological evaluation of the outcomes of nonsurgical root canal treatment in a large cohort of insured dental patients. J. Endod. 2001, 27, 791–796. [Google Scholar] [CrossRef]
- Friedman, S.; Mor, C. The success of endodontic therapy—Healing and functionality. J. Calif. Dent. Assoc. 2004, 32, 493–503. [Google Scholar] [CrossRef]
- Touboul, V.; Germa, A.; Lasfargues, J.J.; Bonte, E. Outcome of endodontic treatments made by postgraduate students in the dental clinic of bretonneau hospital. Int. J. Dent. 2014, 2014, 684979. [Google Scholar] [CrossRef] [PubMed]
- Ng, Y.L.; Mann, V.; Gulabivala, K. A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: Part 1: Periapical health. Int. Endod. J. 2011, 44, 583–609. [Google Scholar] [CrossRef] [PubMed]
- Orstavik, D.; Kerekes, K.; Eriksen, H.M. The periapical index: A scoring system for radiographic assessment of apical periodontitis. Dent. Traumatol. 1986, 2, 20–34. [Google Scholar] [CrossRef] [PubMed]
- Baker, B.W. Systematic Review of the Published Literature on Success and Failure Rates of Nonsurgical Endodontic Treatment. Master’s Thesis, Marquette University, Milwaukee, WI, USA, 2013. Available online: https://epublications.marquette.edu/cgi/viewcontent.cgi?article=1181&context=theses_open (accessed on 27 June 2025).
- Firth, D. Bias reduction of maximum likelihood estimates. Biometrika 1993, 80, 27–38. [Google Scholar] [CrossRef]
- Dutner, J.M.; Sidow, S.J.; Cervero, R.M.; Soh, M. Endodontic competence of the new general dentist as conceptualized by predoctoral educators: A qualitative exploration. J. Dent. Oral Epidemiol. 2024, 4, 109. [Google Scholar]
- Tronstad, L.; Asbjørnsen, K.; Døving, L.; Pedersen, I.; Eriksen, H.M. Influence of coronal restorations on the periapical health of endodontically treated teeth. Dent. Traumatol. 2000, 16, 218–221. [Google Scholar] [CrossRef]
- Mehta, D.; Coleman, A.; Lessani, M. Success and failure of endodontic treatment: Predictability, complications, challenges and maintenance. Br. Dent. J. 2025, 238, 527–535. [Google Scholar] [CrossRef]
- Creugers, N.H.; Mentink, A.G.; Käyser, A.F. An analysis of durability data on post and core restorations. J. Dent. 1993, 21, 281–284. [Google Scholar] [CrossRef]
- Setzer, F.C.; Shah, S.B.; Kohli, M.R.; Karabucak, B.; Kim, S. Outcome of endodontic surgery: A meta-analysis of the literature—Part 1: Comparison of traditional root-end surgery and endodontic microsurgery. J. Endod. 2010, 36, 1757–1765. [Google Scholar] [CrossRef]
- Mannocci, F.; Bertelli, E.; Sherriff, M.; Watson, T.F.; Ford, T.R. Three-year clinical comparison of survival of endodontically treated teeth restored with either full cast coverage or with direct composite restoration. J. Prosthet. Dent. 2002, 88, 297–301. [Google Scholar] [CrossRef]
- Jakovljevic, A.; Nikolic, N.; Jacimovic, J.; Pavlovic, O.; Milicic, B.; Beljic-Ivanovic, K.; Miletic, M.; Andric, M.; Milasin, J. Prevalence of Apical Periodontitis and Conventional Nonsurgical Root Canal Treatment in General Adult Population: An Updated Systematic Review and Meta-analysis of Cross-sectional Studies Published between 2012 and 2020. J. Endod. 2020, 46, 1371–1386.e8. [Google Scholar] [CrossRef] [PubMed]
- Sadaf, D.; Ahmad, M.Z. Factors associated with postoperative pain in endodontic therapy. Int. J. Biomed. Sci. 2014, 10, 243–247. [Google Scholar] [CrossRef]
- Klasser, G.D.; Kugelmann, A.M.; Villines, D.; Johnson, B.R. The prevalence of persistent pain after nonsurgical root canal treatment. Quintessence Int. 2011, 42, 259–269. [Google Scholar]
- López-López, J.A.; Davies, S.R.; Caldwell, D.M.; Churchill, R.; Peters, T.J.; Tallon, D.; Dawson, S.; Wu, Q.; Li, J.; Taylor, A.; et al. The process and delivery of CBT for depression in adults: A systematic review and network meta-analysis. Psychol. Med. 2019, 49, 1937–1947. [Google Scholar] [CrossRef] [PubMed]
- Torabinejad, M.; Higa, R.K.; McKendry, D.J.; Pitt Ford, T.R. Dye leakage of four root end filling materials: Effects of blood contamination. J. Endod. 1994, 20, 159–163. [Google Scholar] [CrossRef]
- Saunders, W.P.; Saunders, E.M. Coronal leakage as a cause of failure in root-canal therapy: A review. Dent. Traumatol. 1994, 10, 105–108. [Google Scholar] [CrossRef]
- Sequeira-Byron, P.; Fedorowicz, Z.; Carter, B.; Nasser, M.; Alrowaili, E.F. Single crowns versus conventional fillings for the restoration of root-filled teeth. Cochrane Database Syst. Rev. 2015, 2015, Cd009109. [Google Scholar] [CrossRef] [PubMed]
- Morgano, S.M. Restoration of pulpless teeth: Application of traditional principles in present and future contexts. J. Prosthet. Dent. 1996, 75, 375–380. [Google Scholar] [CrossRef]
- Gillen, B.M.; Looney, S.W.; Gu, L.S.; Loushine, B.A.; Weller, R.N.; Loushine, R.J.; Pashley, D.H.; Tay, F.R. Impact of the quality of coronal restoration versus the quality of root canal fillings on success of root canal treatment: A systematic review and meta-analysis. J. Endod. 2011, 37, 895–902. [Google Scholar] [CrossRef]
- Siqueira, J.F.; Rôças, I.N. Diversity of Endodontic Microbiota Revisited. J. Dent. Res. 2009, 88, 969–981. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Characteristic | Number (%) |
|---|---|
| Gender | |
| Female | 354 (63.78%) |
| Male | 201 (36.22%) |
| Race | |
| White | 256 (46.13%) |
| African American | 139 (25.05%) |
| Unknown | 111 (20%) |
| Asian | 42 (7.57%) |
| Multiracial | 5 (0.90%) |
| Native American | 1 (0.18%) |
| Native Hawaiian and Other Pacific Islander | 1 (0.18%) |
| Ethnicity | |
| Not Hispanic | 435 (78.38%) |
| Hispanic | 66 (11.89%) |
| Unknown | 54 (9.73%) |
| Medical Condition | |
| Alcoholism | 171 (30.8%) |
| High blood pressure | 145 (26.1%) |
| Diabetes | 93 (16.8%) |
| Asthma | 80 (14.4%) |
| Arthritis | 77 (13.9%) |
| Psychiatric care | 77 (13.9%) |
| Anemia | 34 (6.1%) |
| Has/had cancer or tumor | 23 (4.1%) |
| Artificial joint or valve | 17 (3.1%) |
| Heart murmur / Heart valve | 19 (3.4%) |
| Kidney disease | 15 (2.7%) |
| Angina or heart disease | 14 (2.5%) |
| Hepatitis | 11 (2.0%) |
| Epilepsy | 9 (1.6%) |
| Herpes | 7 (1.3%) |
| TB | 4 (0.7%) |
| Pacemaker | 3 (0.5%) |
| AIDS/HIV | 3 (0.5%) |
| Allergies | |
| No known allergy | 356 (64.1%) |
| Penicillin allergy | 72 (13.0%) |
| Allergies or hives | 58 (10.5%) |
| Codeine allergy | 31 (5.6%) |
| Latex allergy | 31 (5.6%) |
| Sulfa allergy | 29 (5.2%) |
| Hay fever or sinus trouble | 27 (4.9%) |
| Aspirin allergy | 15 (2.7%) |
| Barbiturate or sedative allergy | 3 (0.5%) |
| Local anesthetic allergy | 1 (0.2%) |
| Smoking | |
| Smoke or use chewing tobacco | 98 (17.7%) |
| Complications | Premolar (Mandible) n = 77 | Premolar (Maxilla) n = 142 | Molar (Mandible) n = 54 | Molar (Maxilla) n = 40 | Anterior (Mandible) n = 41 | Anterior (Maxilla) n = 177 |
|---|---|---|---|---|---|---|
| Pain on Percussion | 2 (2.6%) | 13 (9.2%) | 6 (11.1%) | 3 (7.5%) | 3 (7.3%) | 13 (7.3%) |
| Pain on Palpation | 0 (0.0%) | 4 (2.8%) | 3 (5.6%) | 3 (7.5%) | 1 (2.4%) | 5 (2.8%) |
| Swelling | 0 (0.0%) | 0 (0.0%) | 1 (1.9%) | 0 (0.0%) | 1 (2.4%) | 1 (0.6%) |
| Sinus Tract | 0 (0.0%) | 0 (0.0%) | 2 (3.7%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| Location | Classification | Level 0 | Level 1 | Level 2 | Level 3 | Level 4 | Level 5 | Level 6 | Level 7 | Level 8 | Level 9 | Level 10 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Premolar | Mandible (67) | 100% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% |
| Maxilla (113) | 94.7% | 0% | 0% | 2.65% | 0.88% | 1.77% | 0% | 0% | 0% | 0% | 0% | |
| Molar | Mandible (35) | 91.4% | 0% | 0% | 2.86% | 2.86% | 2.86% | 0% | 0% | 0% | 0% | 0% |
| Maxilla (32) | 93.75% | 0% | 0% | 0% | 3.13% | 0% | 0% | 0% | 0% | 0% | 3.13% | |
| Anterior | Mandible (37) | 91.89% | 0% | 2.7% | 0% | 0% | 2.7% | 2.7% | 0% | 0% | 0% | 0% |
| Maxilla (146) | 97.95% | 0% | 0% | 0.68% | 0.68% | 0% | 0.68% | 0% | 0% | 0% | 0% |
| Covariate | Est. | Std. Error | 95% PL CI | -Value | Sig. | |
|---|---|---|---|---|---|---|
| (Intercept) | 1.9608 | 2.0937 | (−4.1336, 8.8225) | 0.4853 | 0.48600 | |
| Age | −0.0034 | 0.0214 | (−0.0599, 0.0521) | 0.0162 | 0.89870 | |
| Male (Y/N) | 0.6294 | 0.6906 | (−1.0586, 3.4043) | 0.5089 | 0.47560 | |
| Non-white (Y/N) | 0.8360 | 0.7384 | (−1.006, 3.1707) | 0.7962 | 0.37220 | |
| Hispanic (Y/N) | −1.0509 | 0.9592 | (−4.2243, 1.7484) | 0.6281 | 0.42800 | |
| No conditions (Y/N) | 0.3567 | 0.8379 | (−2.3237, 2.8713) | 0.1057 | 0.74510 | |
| Smoke/use chewing tobacco (Y/N) | −1.5247 | 0.8164 | (−5.8464, 0.6966) | 1.8092 | 0.17860 | |
| Location is maxilla (Y/N) | −0.2932 | 0.7556 | (−2.3902, 1.6981) | 0.0893 | 0.76500 | |
| Classification is molar (Y/N) | 0.3022 | 0.9378 | (−1.9945, 2.8381) | 0.0695 | 0.79210 | |
| Classification is anterior (Y/N) | −0.1265 | 0.6705 | (−1.7774, 1.4741) | 0.0252 | 0.87380 | |
| Num. of appts. to complete RCT | 0.0516 | 0.2397 | (−0.5757, 0.9136) | 0.0279 | 0.86720 | |
| Pre-existing radiolucency (Y/N) | −2.7398 | 1.0058 | (−8.3087, −0.3886) | 5.5972 | 0.01799 | * |
| Periodontal status of the tooth | −0.3360 | 0.3331 | (−1.4609, 0.547) | 0.5584 | 0.45490 | |
| Type of restoration | 0.3086 | 0.4836 | (−0.8302, 1.507) | 0.2978 | 0.58530 | |
| Restoration is intact (Y/N) | 3.4463 | 0.8232 | (1.5963, 7.895) | 17.6380 | 0.00003 | *** |
| Metal post (Y/N) | −4.2963 | 1.5272 | (−13.3039, −0.7049) | 6.3619 | 0.01166 | * |
| Fiber post (Y/N) | −1.4415 | 1.5255 | (−7.172, 4.2949) | 0.3640 | 0.54630 | |
| Post in straight root (Y/N) | 4.2421 | 1.5293 | (0.4856, 13.8117) | 5.3571 | 0.02064 | * |
| Post in curved root (Y/N) | 2.0990 | 1.4224 | (−1.648, 8.005) | 1.1253 | 0.28880 | |
| Radiographic eval. | −0.0153 | 0.3327 | (−0.8575, 1.0244) | 0.0012 | 0.97240 |
| Covariate | Est. | Std. Error | 95% PL CI | -Value | Sig. | |
|---|---|---|---|---|---|---|
| (Intercept) | −0.2105 | 1.2035 | (−2.7956, 2.3414) | 0.0261 | 0.87150 | |
| Age | −0.0104 | 0.0130 | (−0.0386, 0.0173) | 0.5480 | 0.45920 | |
| Male (Y/N) | 0.1046 | 0.4309 | (−0.8418, 1.0126) | 0.0496 | 0.82380 | |
| Non-white (Y/N) | −0.5281 | 0.4188 | (−1.4473, 0.35) | 1.3789 | 0.24030 | |
| Hispanic (Y/N) | −0.7689 | 0.7863 | (−3.0065, 0.7129) | 0.8954 | 0.34400 | |
| No conditions (Y/N) | −0.4554 | 0.5018 | (−1.6218, 0.559) | 0.7316 | 0.39240 | |
| Smoke/use chewing tobacco (Y/N) | 0.4330 | 0.4487 | (−0.548, 1.3528) | 0.7880 | 0.37470 | |
| Location is maxilla (Y/N) | 0.0061 | 0.4480 | (−0.9383, 0.9901) | 0.0002 | 0.99000 | |
| Classification is molar (Y/N) | −0.3027 | 0.5678 | (−1.5787, 0.8711) | 0.2458 | 0.62010 | |
| Classification is anterior (Y/N) | −0.2056 | 0.4546 | (−1.1837, 0.7596) | 0.1754 | 0.67540 | |
| Num. of appts. to complete RCT | 0.2063 | 0.1508 | (−0.1388, 0.518) | 1.4651 | 0.22610 | |
| Pre-existing radiolucency (Y/N) | 0.1172 | 0.3926 | (−0.7277, 0.9643) | 0.0752 | 0.78390 | |
| Periodontal status of tooth | 0.5550 | 0.1684 | (0.2045, 0.9057) | 9.2942 | 0.00230 | ** |
| Type of restoration | −0.7659 | 0.3139 | (−1.4267, −0.1024) | 5.0869 | 0.02411 | * |
| Restoration is intact (Y/N) | −0.4171 | 0.4534 | (−1.3524, 0.5843) | 0.7037 | 0.40150 | |
| Metal post (Y/N) | 0.5391 | 0.6372 | (−0.8875, 1.8587) | 0.5954 | 0.44030 | |
| Fiber post (Y/N) | 0.4256 | 0.5658 | (−0.8079, 1.6544) | 0.4711 | 0.49250 | |
| Post in straight root (Y/N) | −0.8536 | 0.5024 | (−1.9465, 0.1965) | 2.5382 | 0.11110 | |
| Post in curved root (Y/N) | −0.6488 | 0.7831 | (−2.5202, 0.9103) | 0.6194 | 0.43130 | |
| Radiographic Eval. | −0.2347 | 0.2133 | (−0.7425, 0.1974) | 1.0660 | 0.30190 |
| Covariate | Est. | Std. Error | 95% CI | Stat. | -Value | Sig. |
|---|---|---|---|---|---|---|
| Age | 0.0057 | 0.0080 | (0.0214, −0.01) | 0.7172497 | 0.47320 | |
| Male (Y/N) | 0.0714 | 0.2477 | (0.5569, −0.4141) | 0.2882467 | 0.77320 | |
| Non-white (Y/N) | 0.3396 | 0.2260 | (0.7826, −0.1034) | 1.5028592 | 0.13290 | |
| Hispanic (Y/N) | −0.0395 | 0.3015 | (0.5514, −0.6304) | −0.1309459 | 0.89580 | |
| Asthma (Y/N) | −0.2985 | 0.3171 | (0.323, −0.92) | −0.9414325 | 0.34650 | |
| No conditions (Y/N) | −0.0996 | 0.2755 | (0.4404, −0.6396) | −0.3614109 | 0.71780 | |
| Smoke/use chewing tobacco (Y/N) | 0.0235 | 0.2909 | (0.5937, −0.5467) | 0.0808452 | 0.93560 | |
| Location is maxilla (Y/N) | −0.0041 | 0.2420 | (0.4702, −0.4784) | −0.0168121 | 0.98660 | |
| Classification is molar (Y/N) | −0.1355 | 0.3123 | (0.4766, −0.7476) | −0.4336780 | 0.66450 | |
| Classification is anterior (Y/N) | −0.2297 | 0.2389 | (0.2385, −0.6979) | −0.9614684 | 0.33630 | |
| Restoration is intact (Y/N) | 3.0872 | 0.3357 | (3.7452, 2.4292) | 9.1957321 | 0.00000 | *** |
| Radiographic Eval. | 0.0426 | 0.1075 | (0.2533, −0.1681) | 0.3966283 | 0.69160 | |
| Intercept | Est. | Std. Error | 95% CI | stat. | -value | Sig. |
| 01 | −0.9333 | 0.6156 | (0.2733, −2.1399) | −1.5161329 | 0.12950 | |
| 12 | −0.7680 | 0.6108 | (0.4292, −1.9652) | −1.2574571 | 0.20860 | |
| 23 | −0.6914 | 0.6087 | (0.5017, −1.8845) | −1.1358350 | 0.25600 | |
| 34 | −0.5507 | 0.6055 | (0.6361, −1.7375) | −0.9094519 | 0.36310 | |
| 45 | −0.0809 | 0.6002 | (1.0955, −1.2573) | −0.1347940 | 0.89280 | |
| 56 | 0.5793 | 0.6021 | (1.7594, −0.6008) | 0.9620442 | 0.33600 | |
| 67 | 1.1759 | 0.6085 | (2.3686, −0.0168) | 1.9322787 | 0.05333 | |
| 78 | 1.8469 | 0.6180 | (3.0582, 0.6356) | 2.9887187 | 0.00280 | ** |
| 89 | 2.6237 | 0.6264 | (3.8514, 1.396) | 4.1882417 | 0.00003 | *** |
| 910 | 3.1192 | 0.6292 | (4.3524, 1.886) | 4.9573202 | 0.00000 | *** |
| Covariate | Est. | Std. Error | 95% CI | Stat | -Value | Sig. |
|---|---|---|---|---|---|---|
| Age | 0.0127 | 0.0098 | (−0.0065, 0.0319) | 1.2989196 | 0.19400 | |
| Male (Y/N) | 0.3717 | 0.3360 | (−0.2869, 1.0303) | 1.1062783 | 0.26860 | |
| Non-white (Y/N) | 0.4427 | 0.2955 | (−0.1365, 1.0219) | 1.4982001 | 0.13410 | |
| Hispanic (Y/N) | −0.7456 | 0.3879 | (−1.5059, 0.0147) | −1.9219718 | 0.05461 | |
| Asthma (Y/N) | −0.0133 | 0.3883 | (−0.7744, 0.7478) | −0.0343227 | 0.97260 | |
| No conditions (Y/N) | 1.3490 | 0.4201 | (0.5256, 2.1724) | 3.2114060 | 0.00132 | ** |
| Smoke/use chewing tobacco (Y/N) | 0.3131 | 0.3668 | (−0.4058, 1.032) | 0.8536207 | 0.39330 | |
| Location is maxilla (Y/N) | −0.0376 | 0.3037 | (−0.6329, 0.5577) | −0.1238733 | 0.90140 | |
| Classification is molar (Y/N) | −0.4837 | 0.3995 | (−1.2667, 0.2993) | −1.2107436 | 0.22600 | |
| Classification is anterior (Y/N) | −0.1875 | 0.3167 | (−0.8082, 0.4332) | −0.5922568 | 0.55370 | |
| Num. of appts. to complete RCT | 0.0381 | 0.1237 | (−0.2044, 0.2806) | 0.3082347 | 0.75790 | |
| Pre-existing radiolucency (Y/N) | −0.7699 | 0.2804 | (−1.3195, −0.2203) | −2.7454762 | 0.00604 | ** |
| Periodontal status of tooth | −0.9005 | 0.1498 | (−1.1941, −0.6069) | −6.0136463 | 0.00000 | *** |
| Type of restoration | 0.4214 | 0.2497 | (−0.068, 0.9108) | 1.6875502 | 0.09150 | |
| Restoration is intact (Y/N) | 3.9584 | 0.4488 | (3.0788, 4.838) | 8.8207555 | 0.00000 | *** |
| Metal post (Y/N) | −0.3082 | 0.4658 | (−1.2212, 0.6048) | −0.6617978 | 0.50810 | |
| Fiber post (Y/N) | −0.2891 | 0.3652 | (−1.0049, 0.4267) | −0.7916293 | 0.42860 | |
| Post in straight root (Y/N) | 1.0538 | 0.3936 | (0.2823, 1.8253) | 2.6776059 | 0.00741 | ** |
| Post in curved root (Y/N) | 0.8671 | 0.5773 | (−0.2644, 1.9986) | 1.5021694 | 0.13310 | |
| Radiographic eval | 0.2405 | 0.1437 | (−0.0412, 0.5222) | 1.6740322 | 0.09412 | |
| Intercept | Est. | Std. Error | 95% CI | stat. | -value | Sig. |
| 01 | 0.8366 | 0.9597 | (−1.0444, 2.7176) | 0.8716637 | 0.38340 | |
| 12 | 1.0178 | 0.9571 | (−0.8581, 2.8937) | 1.0633914 | 0.28760 | |
| 23 | 1.1031 | 0.9562 | (−0.7711, 2.9773) | 1.1535688 | 0.24870 | |
| 34 | 1.1031 | 0.9562 | (−0.7711, 2.9773) | 1.1535691 | 0.24870 | |
| 45 | 1.2674 | 0.9553 | (−0.605, 3.1398) | 1.3267701 | 0.18460 | |
| 56 | 2.0704 | 0.9612 | (0.1864, 3.9544) | 2.1541018 | 0.03123 | * |
| 67 | 2.7968 | 0.9730 | (0.8897, 4.7039) | 2.8743878 | 0.00405 | ** |
| 78 | 3.5436 | 0.9838 | (1.6154, 5.4718) | 3.6021003 | 0.00032 | *** |
| 89 | 4.4770 | 0.9978 | (2.5213, 6.4327) | 4.4867608 | 0.00001 | *** |
| 910 | 5.2657 | 1.0118 | (3.2826, 7.2488) | 5.2041119 | 0.00000 | *** |
| Covariate | Est. | Std. Error | 95% CI | Stat | -Value | Sig. |
|---|---|---|---|---|---|---|
| Age | 0.0181 | 0.0099 | (−0.0013, 0.0375) | 1.8237583 | 0.06954 | |
| Male (Y/N) | 0.1276 | 0.3325 | (−0.5241, 0.7793) | 0.3836267 | 0.70160 | |
| Non-white (Y/N) | 0.4669 | 0.3002 | (−0.1215, 1.0553) | 1.5549825 | 0.12140 | |
| Hispanic (Y/N) | −0.6464 | 0.3943 | (−1.4192, 0.1264) | −1.6392154 | 0.10260 | |
| Asthma (Y/N) | −0.0011 | 0.3885 | (−0.7626, 0.7604) | −0.0028486 | 0.99770 | |
| No conditions (Y/N) | 1.4308 | 0.4240 | (0.5998, 2.2618) | 3.3743472 | 0.00087 | *** |
| Smoke/use chewing tobacco (Y/N) | 0.2242 | 0.3675 | (−0.4961, 0.9445) | 0.6101076 | 0.54240 | |
| Location is maxilla (Y/N) | 0.0758 | 0.3060 | (−0.524, 0.6756) | 0.2476545 | 0.80460 | |
| Classification is molar (Y/N) | −0.2434 | 0.3993 | (−1.026, 0.5392) | −0.6095559 | 0.54280 | |
| Classification is anterior (Y/N) | −0.1647 | 0.3199 | (−0.7917, 0.4623) | −0.5148864 | 0.60710 | |
| Num. of appts. to complete RCT | 0.0222 | 0.1270 | (−0.2267, 0.2711) | 0.1749472 | 0.86130 | |
| Pre-existing radiolucency (Y/N) | −0.7448 | 0.2835 | (−1.3005, −0.1891) | −2.6273969 | 0.00921 | ** |
| Periodontal status of tooth | −0.9138 | 0.1462 | (−1.2004, −0.6272) | −6.2482193 | 0.00000 | *** |
| Type of restoration | 0.5177 | 0.2520 | (0.0238, 1.0116) | 2.0545722 | 0.04110 | * |
| Restoration is intact (Y/N) | 3.5411 | 0.4311 | (2.6961, 4.3861) | 8.2132800 | 0.00000 | *** |
| Metal post (Y/N) | −0.1156 | 0.4762 | (−1.049, 0.8178) | −0.2428246 | 0.80840 | |
| Fiber post (Y/N) | −0.1695 | 0.3725 | (−0.8996, 0.5606) | −0.4550398 | 0.64950 | |
| Post in straight canal (Y/N) | 0.9451 | 0.3961 | (0.1687, 1.7215) | 2.3859882 | 0.01788 | * |
| Post in curved canal (Y/N) | 0.5328 | 0.5786 | (−0.6013, 1.6669) | 0.9207637 | 0.35820 | |
| Radiographic eval | 0.0909 | 0.1420 | (−0.1874, 0.3692) | 0.6403563 | 0.52260 | |
| Intercept | Est. | Std. Error | 95% CI | stat | -value | Sig. |
| 01 | 0.5360 | 0.9799 | (−1.3845, 2.4566) | 0.5471 | 0.5843 | |
| 12 | 0.7573 | 0.9749 | (−1.1536, 2.6682) | 0.7768 | 0.4373 | |
| 23 | 0.8564 | 0.9732 | (−1.0511, 2.7638) | 0.8800 | 0.3789 | |
| 34 | 0.9476 | 0.9715 | (−0.9566, 2.8519) | 0.9754 | 0.3294 | |
| 45 | 1.1171 | 0.9691 | (−0.7824, 3.0165) | 1.1527 | 0.2490 | |
| 56 | 2.1192 | 0.9676 | (0.2227, 4.0157) | 2.1902 | 0.0285 | * |
| 67 | 2.7850 | 0.9762 | (0.8716, 4.6984) | 2.8529 | 0.0043 | *** |
| 78 | 3.5558 | 0.9886 | (1.6182, 5.4934) | 3.5969 | 0.0003 | *** |
| 89 | 4.2135 | 0.9980 | (2.2574, 6.1696) | 4.2219 | 0.0000 | *** |
| 910 | 5.0653 | 1.0117 | (3.0823, 7.0484) | 5.0065 | 0.0000 | *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Jallad, N.; Sun, E.; Wu, T.; Cui, S.; Basmaji, A.; Thakkar, R.; Aboelmagd, S.; Naik, N.; Tzouma, K.; Xiao, J.; et al. The Success of Endodontic Treatments Performed by Dental Residents in Advanced Education in General Dentistry Program: A 10-Year Retrospective Study. Dent. J. 2025, 13, 306. https://doi.org/10.3390/dj13070306
Al Jallad N, Sun E, Wu T, Cui S, Basmaji A, Thakkar R, Aboelmagd S, Naik N, Tzouma K, Xiao J, et al. The Success of Endodontic Treatments Performed by Dental Residents in Advanced Education in General Dentistry Program: A 10-Year Retrospective Study. Dentistry Journal. 2025; 13(7):306. https://doi.org/10.3390/dj13070306
Chicago/Turabian StyleAl Jallad, Nisreen, Eli Sun, Tongtong Wu, Shasha Cui, Amer Basmaji, Radhika Thakkar, Shahenda Aboelmagd, Neha Naik, Konstantina Tzouma, Jin Xiao, and et al. 2025. "The Success of Endodontic Treatments Performed by Dental Residents in Advanced Education in General Dentistry Program: A 10-Year Retrospective Study" Dentistry Journal 13, no. 7: 306. https://doi.org/10.3390/dj13070306
APA StyleAl Jallad, N., Sun, E., Wu, T., Cui, S., Basmaji, A., Thakkar, R., Aboelmagd, S., Naik, N., Tzouma, K., Xiao, J., & Malmstrom, H. (2025). The Success of Endodontic Treatments Performed by Dental Residents in Advanced Education in General Dentistry Program: A 10-Year Retrospective Study. Dentistry Journal, 13(7), 306. https://doi.org/10.3390/dj13070306