
Prevalence and Classification of C-Shaped Canal and Radix in Mandibular Molars Using Cone-Beam Computed Tomography on Mexican Population

 ,
,  , and
, and
Abstract

1. Introduction
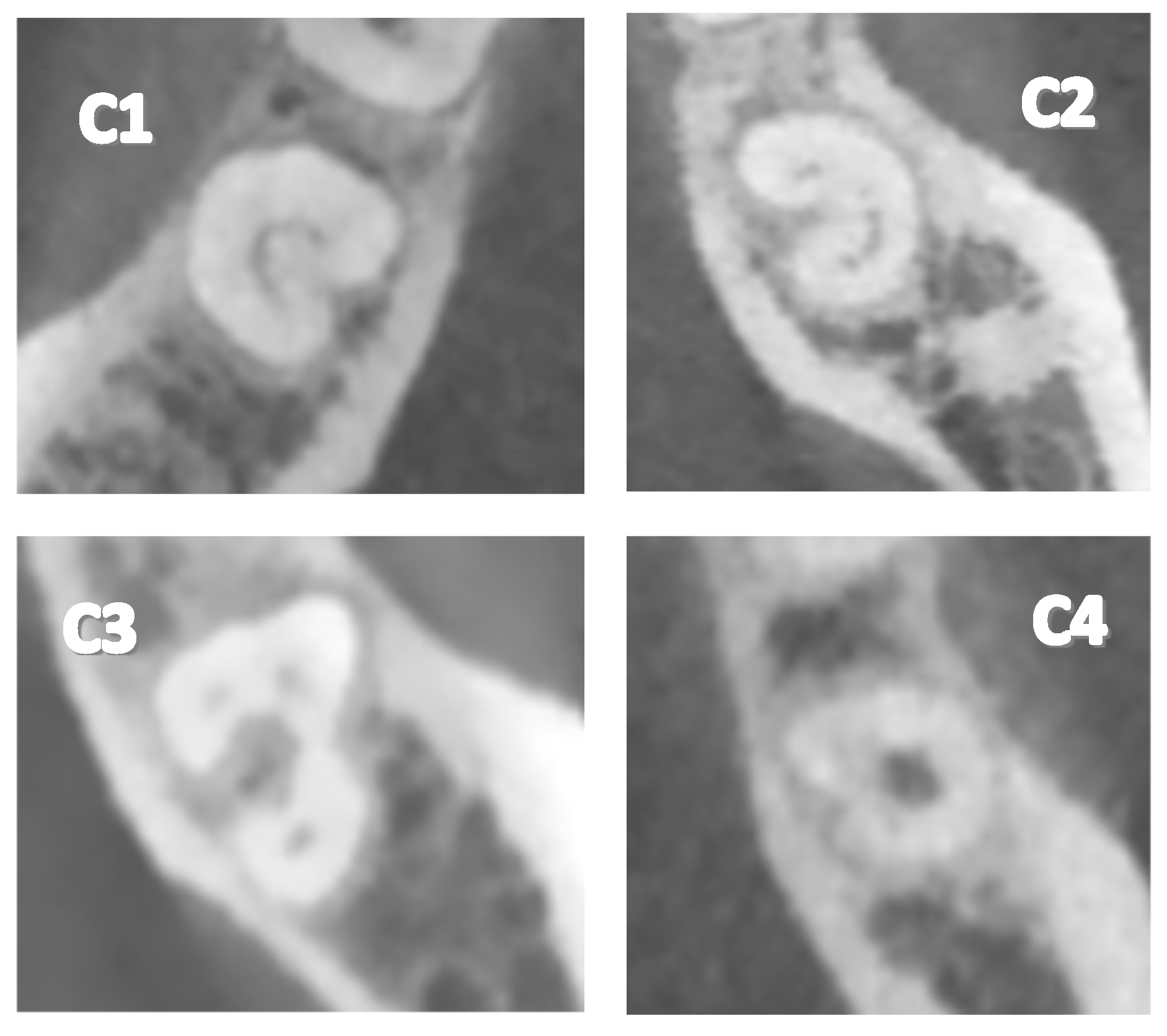
- Type 1 (C1): The C-shape is observed continuously without interruptions or separations.
- Type 2 (C2): The C-shape is observed interrupted, resembling a semicolon, but angles α and β are less than 60°.
- Type 3 (C3): Two or three separate canals are observed, with both angles α and β being less than 60°.
- Type 4 (C4): A single round or oval canal is observed in the cross-section.
- Type 5 (C5): No canal lumen is observed (it may only be visible near the apex).
2. Materials and Methods
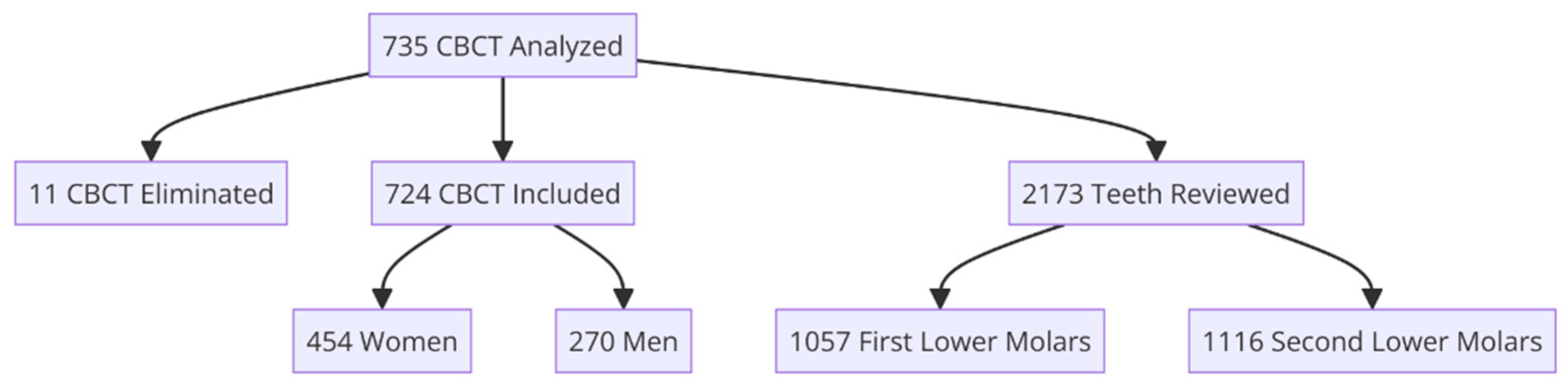
2.1. Study Design and Sample Collection
2.2. Ethics Approval
2.3. Statistical Analysis
2.4. Location
2.5. Dental Nomenclature
2.6. Inclusion Criteria
2.7. Exclusion Criteria
- Teeth that have undergone root canal treatment.
- Retained, impacted, or embedded teeth.
- Teeth with developmental anomalies.
- Teeth with open apices.
- Calcified teeth or canal obliteration.
- Third molars.
2.8. Elimination Criteria
- Tomographic images with inadequate resolution.
- Tomographic images lacking patient data.
3. Results
4. Discussion
5. Conclusions
Limitations of This Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ordinola-Zapata, R.; Noblett, W.C.; Perez-Ron, A.; Ye, Z.; Vera, J. Present status and future directions of intracanal medicaments. Int. Endod. J. 2022, 55 (Suppl. S3), 613–636. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.; Sun, T.; Gao, X.; Zhou, X.; Huang, D. Tooth anatomy risk factors influencing root canal working length accessibility. Int. J. Oral Sci. 2011, 3, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.; Pacheco-Yanes, J.; Siqueira, J.F., Jr.; Oliveira, A.C.S.; Gazzaneo, I.; Amorim, C.A.; Santos, P.H.B.; Alves, F.R.F. Association between missed canals and apical periodontitis. Int. Endod. J. 2019, 52, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Karabucak, B.; Bunes, A.; Chehoud, C.; Kohli, M.R.; Setzer, F. Prevalence of Apical Periodontitis in Endodontically Treated Premolars and Molars with Untreated Canal: A Cone-beam Computed Tomography Study. J. Endod. 2016, 42, 538–541. [Google Scholar] [CrossRef] [PubMed]
- Kolarkodi, S.H. The importance of cone-beam computed tomography in endodontic therapy: A review. Saudi Dent. J. 2023, 35, 780–784. [Google Scholar] [CrossRef] [PubMed]
- Cotti, E.; Schirru, E. Present status and future directions: Imaging techniques for the detection of periapical lesions. Int. Endod. J. 2022, 55 (Suppl. S4), 1085–1099. [Google Scholar] [CrossRef]
- Chan, F.; Brown, L.F.; Parashos, P. CBCT in contemporary endodontics. Aust. Dent. J. 2023, 68 (Suppl. S1), S39–S55. [Google Scholar] [CrossRef] [PubMed]
- Cooke, H.G.; Cox, F.L. C-shaped canal configurations in mandibular molars. J. Am. Dent. Assoc. 1979, 99, 836–839. [Google Scholar] [CrossRef] [PubMed]
- Genovese, F.; Marsico, E. Maxillary Central Incisor with Two Roots: A Case Report. J. Endod. 2003, 29, 220–221. [Google Scholar] [CrossRef]
- Kim, Y.; Lee, D.; Kim, D.; Kim, S. Analysis of cause of endodontic failure of C-Shaped root canals. Scanning 2018, 2018, 2516832. [Google Scholar] [CrossRef]
- Von Zuben, M.; Martins, J.N.; Berti, L.; Cassim, I.; Flynn, D.; Gonzalez, J.A.; Gu, Y.; Kottoor, J.; Monroe, A.; Aguilar, R.R.; et al. Worldwide prevalence of mandibular second molar C-Shaped morphologies evaluated by Cone-Beam Computed Tomography. J. Endod. 2017, 43, 1442–1447. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Q.; Zhang, L.; Zhou, X.; Wang, Q.; Wang, Y.; Tang, L.; Song, F.; Huang, D. C-shaped root canal system in mandibular second molars in a Chinese population evaluated by cone-beam computed tomography. Int. Endod. J. 2011, 44, 857–862. [Google Scholar] [CrossRef] [PubMed]
- Martins, J.N.R.; Mata, A.; Marques, D.; Caramês, J. Prevalence of C-shaped mandibular molars in the Portuguese population evaluated by cone-beam computed tomography. Eur. J. Dent. 2016, 10, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Fan, B.; Cheung, G.; Fan, M.; Gutmann, J.; Bian, Z. C-shaped canal system in mandibular second molars: Part I—Anatomical features. J. Endod. 2004, 30, 899–903. [Google Scholar] [CrossRef] [PubMed]
- Carlsen, O.; Alexandersen, V. Radix paramolaris in permanent mandibular molars: Identification and morphology. Eur. J. Oral Sci. 1991, 99, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, H.; Abbott, P. Accessory roots in maxillary molar teeth: A review and endodontic considerations. Aust. Dent. J. 2012, 57, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Martins, J.N.; Nole, C.; Ounsi, H.F.; Parashos, P.; Plotino, G.; Ragnarsson, M.F.; Aguilar, R.R.; Santiago, F.; Seedat, H.C.; Vargas, W.; et al. Worldwide Assessment of the Mandibular First Molar Second Distal Root and Root Canal: A Cross-sectional Study with Meta-analysis. J. Endod. 2022, 48, 223–233. [Google Scholar] [CrossRef] [PubMed]
- Carlsen, O.; Alexandersen, V. Radix entomolaris: Identification and morphology. Eur. J. Oral Sci. 1990, 98, 363–373. [Google Scholar] [CrossRef] [PubMed]
- Essential Endodontology: Prevention and Treatment of Apical Periodontitis, 3rd ed.; Wiley: Hoboken, NJ, USA, 2020; Available online: https://www.wiley.com/en-us/Essential+Endodontology%3A+Prevention+and+Treatment+of+Apical+Periodontitis%2C+3rd+Edition-p-9781119271956 (accessed on 1 January 2024).
- Chaniotis, A.; Ordinola-Zapata, R. Present status and future directions: Management of curved and calcified root canals. Int. Endod. J. 2022, 55 (Suppl. S3), 656–684. [Google Scholar] [CrossRef] [PubMed]
- Vertucci, F.J. Root canal morphology and its relationship to endodontic procedures. Endod. Top. 2005, 10, 3–29. [Google Scholar] [CrossRef]
- Ahmad, I.A.; Alenezi, M.A. Root and root canal morphology of Maxillary first premolars: A Literature review and clinical considerations. J. Endod. 2016, 42, 861–872. [Google Scholar] [CrossRef]
- Baruwa, A.O.; Martins, J.N.; Meirinhos, J.; Pereira, B.; Gouveia, J.; Quaresma, S.A.; Monroe, A.; Ginjeira, A. The influence of missed canals on the prevalence of periapical lesions in endodontically treated teeth: A cross-sectional study. J. Endod. 2020, 46, 34–39.e1. [Google Scholar] [CrossRef]
- Ahmed, H.M.A.; Dummer, P.M.H. A new system for classifying tooth, root and canal anomalies. Int. Endod. J. 2017, 51, 389–404. [Google Scholar] [CrossRef]
- Coutinho, T.; Lenzi, M.; Simões, M.; Campos, V. Duplication of a permanent maxillary incisor root caused by trauma to the predecessor primary tooth: Clinical case report. Int. Endod. J. 2011, 44, 688–695. [Google Scholar] [CrossRef]
- Joshi, N.; Shrestha, S.; Sundas, S.; Prajapati, K.; Wagle, S.D.; Gharti, A. C-Shaped Canal in Second Molar of Mandible among Cases of Cone Beam Computed Tomography in Tertiary Care Centres: A Descriptive Cross-sectional Study. J. Nepal Med. Assoc. 2021, 59, 649–652. [Google Scholar] [CrossRef]
- Seo, M.S.; Park, D.S. C-shaped root canals of mandibular second molars in a Korean population: Clinical observation and in vitro analysis. Int. Endod. J. 2004, 37, 139–144. [Google Scholar] [CrossRef]
- Janani, M.; Rahimi, S.; Jafari, F.; Johari, M.; Nikniaz, S.; Ghasemi, N. Anatomic features of C-shaped mandibular second molars in a selected Iranian population using CBCT. PubMed 2018, 13, 120–125. [Google Scholar] [CrossRef]
- Qian, Y.; Li, Y.; Song, J.; Zhang, P.; Chen, Z. Evaluation of C-shaped canals in maxillary molars in a Chinese population using CBCT. BMC Med. Imaging 2022, 22, 104. [Google Scholar] [CrossRef]
- Mohan, S.; Thakur, J. Prevalence of radix entomolaris in India and its comparison with the rest of the world. Minerva Dent. Oral Sci. 2022, 71, 117–122. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 3.7 | 4.7 | 3.6 | 4.6 | p * | |
|---|---|---|---|---|---|
| n | 560 | 556 | 539 | 518 | <0.001 |
| Absence | 85.2% | 86.5% | 99.8% | 99.8% | |
| Presence | 14.8% | 13.5% | 0.2% | 0.2% |
| Women (454) | Men (270) | p * | OR ** | |
|---|---|---|---|---|
| Absence | 82.15% | 90% | 0.004 | 1.78 (1.18–2.68) |
| Presence | 17.8% | 10% |
| 3.7 | p * | 4.7 | p * | 3.6 | p * | 4.6 | p * | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Women | Men | Women | Men | Women | Men | Women | Men | |||||
| Absence | 86.3% | 92.2% | 0.016 | 86.7% | 94.4% | 0.001 | 99.7% | 100% | 0.998 | 99.7% | 100% | 0.993 |
| Presence | 13.6% | 7.7% | 13.2% | 5.5% | 0.2% | 0% | 0.2% | 0% | ||||
| Type | N° of Teeth | Percentage |
|---|---|---|
| C1 | 42 | 26.3% |
| C2 | 63 | 39.3% |
| C3 | 30 | 18.8% |
| C4 | 25 | 15.6% |
| C5 | 0 | 0% |
| 3.7 | 4.7 | 3.6 | 4.6 | p * | |
|---|---|---|---|---|---|
| n = 560 | n = 556 | n = 539 | n = 518 | <0.001 | |
| Absence | 85.2% | 86.5% | 99.8% | 99.8% | |
| C1 | 4.3% | 3.2% | 0% | 0% | |
| C2 | 5.5% | 5.4% | 0.2% | 0.2% | |
| C3 | 2.7% | 2.7% | 0% | 0% | |
| C4 | 2.3% | 2.2% | 0% | 0% | |
| C5 | 0% | 0% | 0% | 0% |
| 3.7 | 4.7 | 3.6 | 4.6 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Women (352) | Men (208) | p * 0.171 | Women (346) | Men (210) | p * 0.015 | Women (332) | Men (207) | Women (319) | Men (199) | |
| Absence | 82.3% | 89.9% | 82.6% | 92.8% | 99.6% | 100% | 99.6% | 100% | ||
| C1 | 5.1% | 2.8% | 3.7% | 2.3% | 0% | 0% | 0% | 0% | ||
| C2 | 6.2% | 4.3% | 6.6% | 3.3% | 0.4% | 0% | 0.4% | 0% | ||
| C3 | 3.1% | 1.9% | 3.7% | 0.9% | 0% | 0% | 0% | 0% | ||
| C4 | 3.1% | 0.9% | 3.1% | 0.4% | 0% | 0% | 0% | 0% | ||
| C5 | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | ||
| 3.7 (559) | 4.7 (556) | 3.6 (539) | 4.6 (518) | p * | |
|---|---|---|---|---|---|
| Absence | 99.1% | 98% | 96.7% | 96.5% | 0.0264 |
| Presence | 0.9% | 2% | 3.3% | 3.5% |
| Women (454) | Men (270) | p * | |
|---|---|---|---|
| Absence | 92.9% | 92.2% | 0.788 |
| Presence | 7.0% | 7.7% |
| 3.7 | 4.7 | 3.6 | 4.6 | |||||
|---|---|---|---|---|---|---|---|---|
| Women (352) | Men (208) | Women (346) | Men (210) | Women (332) | Men (207) | Women (319) | Men (199) | |
| Absence | 98.5% | 99.5% | 98.2% | 97.6% | 96.6% | 96.6% | 96.8% | 95.9% |
| Presence | 1.4% | 0.4% | 1.7% | 2.3% | 3.3% | 3.3% | 3.1% | 4.0% |
| Type | Number of Teeth | Percentage | p * |
|---|---|---|---|
| Entomolaris | 50 | 94.3% | <0.001 |
| Paramolaris | 3 | 5.6% |
| 3.7 (560) | 4.7 (556) | 3.6 (539) | 4.6 (518) | p * | |
|---|---|---|---|---|---|
| Absence | 98.9% | 98% | 96.7% | 96.5% | 0.1657 |
| Entomolaris | 1.1% | 1.6% | 3.3% | 3.3% | |
| Paramolaris | 0% | 0.4% | 0% | 0.2% |
| 3.7 | p * | 4.7 | p * | 3.6 | 4.6 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Women (553) | Men (208) | 0.42 | Women (346) | Men (210) | 0.57 | Women (332) | Men (207) | Women (319) | Men (199) | |
| Absence | 98.5% | 99.8% | 98.2% | 97.6% | 96.6% | 96.6% | 96.8% | 95.9% | ||
| Entomolaris | 1.4% | 0.4% | 1.4% | 1.9% | 3.3% | 3.3% | 2.8% | 4% | ||
| Paramolaris | 0% | 0% | 0.2% | 0.4% | 0% | 0% | 0.3% | 0% | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Armenta, H.B.; Mireles, A.G.R.; Martinez, J.S.; Alvarez, J.P.; Herrera, Y.R.; Maldonado, O.T.; Ojeda, O.A.; Pacheco, J.S.; Sarabia, G.O.; Castellanos-Juarez, F.X.; et al. Prevalence and Classification of C-Shaped Canal and Radix in Mandibular Molars Using Cone-Beam Computed Tomography on Mexican Population. Dent. J. 2024, 12, 212. https://doi.org/10.3390/dj12070212
Armenta HB, Mireles AGR, Martinez JS, Alvarez JP, Herrera YR, Maldonado OT, Ojeda OA, Pacheco JS, Sarabia GO, Castellanos-Juarez FX, et al. Prevalence and Classification of C-Shaped Canal and Radix in Mandibular Molars Using Cone-Beam Computed Tomography on Mexican Population. Dentistry Journal. 2024; 12(7):212. https://doi.org/10.3390/dj12070212
Chicago/Turabian StyleArmenta, Hugo Bojorquez, Angel Gustavo Romo Mireles, Javier Solis Martinez, Jesus Pescador Alvarez, Yarely Ramos Herrera, Omar Tremillo Maldonado, Oscar Almeda Ojeda, Jose Salas Pacheco, Gamaliel Ortiz Sarabia, Francisco Xavier Castellanos-Juarez, and et al. 2024. "Prevalence and Classification of C-Shaped Canal and Radix in Mandibular Molars Using Cone-Beam Computed Tomography on Mexican Population" Dentistry Journal 12, no. 7: 212. https://doi.org/10.3390/dj12070212
APA StyleArmenta, H. B., Mireles, A. G. R., Martinez, J. S., Alvarez, J. P., Herrera, Y. R., Maldonado, O. T., Ojeda, O. A., Pacheco, J. S., Sarabia, G. O., Castellanos-Juarez, F. X., & Pacheco, S. S. (2024). Prevalence and Classification of C-Shaped Canal and Radix in Mandibular Molars Using Cone-Beam Computed Tomography on Mexican Population. Dentistry Journal, 12(7), 212. https://doi.org/10.3390/dj12070212