
Clinical Use of Paraprobiotics for Pregnant Women with Periodontitis: Randomized Clinical Trial

 ,
,  , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
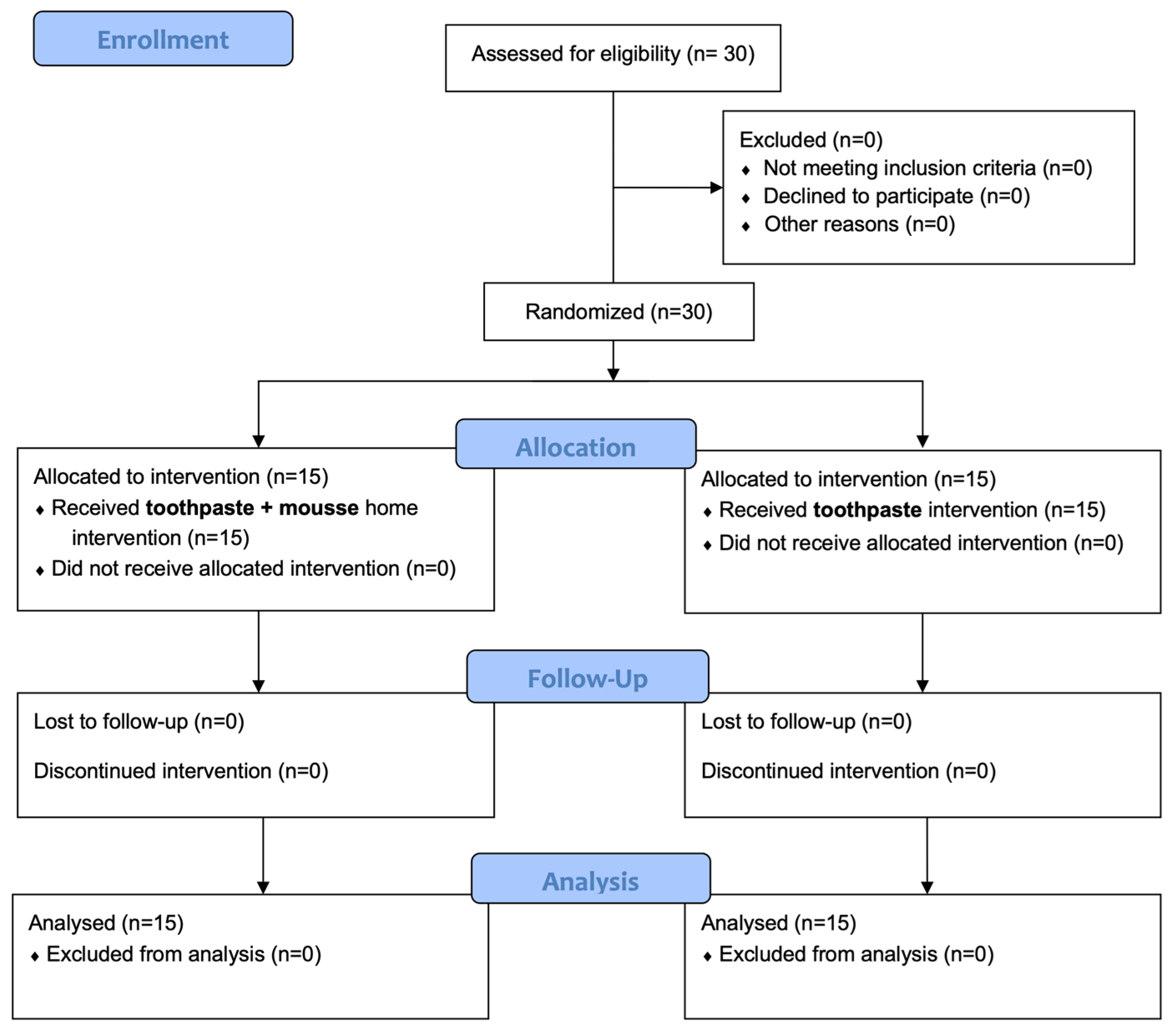
2.1. Study Design
2.2. Participants
2.3. Interventions and Outcomes
2.4. Sample Size
2.5. Randomization and Blinding
2.6. Statistical Analysis
3. Results
3.1. Participants Flow and Baseline Data
3.2. Clinical Attachment Loss (CAL)
3.3. Probing Pocket Depth (PPD)
3.4. Plaque Control Record (PCR)
3.5. Bleeding on Probing (BOP)
3.6. Modified Marginal Gingival Index (mMGI)
3.7. Papillary Marginal Gingival Index (PMGI)
3.8. Recession (R)
3.9. Harms and Adverse Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kandelman, D.; Petersen, P.E.; Ueda, H. Oral health, general health, and quality of life in older people. Spec. Care Dent. 2008, 28, 224–236. [Google Scholar] [CrossRef] [PubMed]
- Kwon, T.; Lamster, I.B.; Levin, L. Current Concepts in the Management of Periodontitis. Int. Dent. J. 2021, 71, 462–476. [Google Scholar] [CrossRef] [PubMed]
- Kajiya, M.; Kurihara, H. Molecular Mechanisms of Periodontal Disease. Int. J. Mol. Sci. 2021, 22, 930. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Oral Health; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Michaud, D.S.; Fu, Z.; Shi, J.; Chung, M. Periodontal Disease, Tooth Loss, and Cancer Risk. Epidemiol. Rev. 2017, 39, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Kinane, D.F. Causation and pathogenesis of periodontal disease. Periodontol. 2000 2001, 25, 8–20. [Google Scholar] [CrossRef] [PubMed]
- Page, R.C.; Offenbacher, S.; Schroeder, H.E.; Seymour, G.J.; Kornman, K.S. Advances in the pathogenesis of periodontitis: Summary of developments, clinical implications and future directions. Periodontol. 2000 1997, 14, 216–248. [Google Scholar] [CrossRef] [PubMed]
- Camelo-Castillo, A.J.; Mira, A.; Pico, A.; Nibali, L.; Henderson, B.; Donos, N.; Tomás, I. Subgingival microbiota in health compared to periodontitis and the influence of smoking. Front. Microbiol. 2015, 6, 119. [Google Scholar] [CrossRef] [PubMed]
- Mealey, B.L.; Oates, T.W. Diabetes mellitus and periodontal diseases. J. Periodontol. 2006, 77, 1289–1303. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Hong, F.; Yu, X. Prevalence of periodontal disease in pregnancy: A systematic review and meta-analysis. J. Dent. 2022, 125, 104253. [Google Scholar] [CrossRef] [PubMed]
- Vivares-Builes, A.M.; Rangel-Rincon, L.J.; Botero, J.E.; Agudelo-Suarez, A.A. Gaps in knowledge about the association between maternal periodontitis and adverse obstetric outcomes: An umbrella review. J. Evid. Based Dent. Pract. 2018, 18, 1–27. [Google Scholar] [CrossRef]
- Laine, M.A. Effect of pregnancy on periodontal and dental health. Acta Odontol. Scand. 2002, 60, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Iida, H. Oral Health Interventions During Pregnancy. Dent. Clin. N. Am. 2017, 61, 467–481. [Google Scholar] [CrossRef] [PubMed]
- Basavaraju, A.; Durga, S.V.; Vanitha, B. Variations in the oral anaerobic microbial flora in relation to pregnancy. J. Clin. Diagn. Res. 2012, 6, 1489–1491. [Google Scholar] [CrossRef] [PubMed]
- Usin, M.M.; Tabares, S.M.; Parodi, R.J.; Sembaj, A. Periodontal conditions during the pregnancy associated with periodontal pathogens. J. Investig. Clin. Dent. 2013, 4, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Morelli, E.L.; Broadbent, J.M.; Leichter, J.W.; Thomson, W.M. Pregnancy, parity and periodontal disease. Aust. Dent. J. 2018, 63, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Sarlati, F.; Akhondi, N.; Jahanbakhsh, N. Effect of general health and sociocultural variables on periodontal status of pregnant women. J. Int. Acad. Periodontol. 2004, 6, 95–100. [Google Scholar] [PubMed]
- Geurs, N.C.; Jeffcoat, M.K.; Tanna, N.; Geisinger, M.L.; Parry, S.; Biggio, J.R.; Doyle, M.J.; Grender, J.M.; Gerlach, R.W.; Reddy, M.S. A Randomized Controlled Clinical Trial of Prenatal Oral Hygiene Education in Pregnancy-Associated Gingivitis. J. Midwifery Womens Health 2023, 68, 507–516. [Google Scholar] [CrossRef] [PubMed]
- Bushehab, N.M.E.; Sreedharan, J.; Reddy, S.; D’souza, J.; Abdelmagyd, H. Oral Hygiene Practices and Awareness of Pregnant Women about the Effects of Periodontal Disease on Pregnancy Outcomes. Int. J. Dent. 2022, 2022, 5195278. [Google Scholar] [CrossRef]
- Egić, B. Impact of school for future parents and first preventive examination in the first year of life on oral habits. J. Clin. Pediatr. Dent. 2023, 47, 94–99. [Google Scholar] [PubMed]
- Gadzhula, N.G.; Cherepakha, O.L.; Lezhnova, O.V. Efficiency of Treatment of Inflammatory Periodontal Diseases in Pregnant Women. Wiad. Lek. 2021, 74, 1065–1068. [Google Scholar] [CrossRef] [PubMed]
- Vasiliauskiene, I.; Milciuviene, S.; Bendoraitiene, E.; Narbutaite, J.; Slabsinskiene, E.; Andruskeviciene, V. Dynamics of pregnant women’s oral health status during preventive programme. Stomatologija 2007, 9, 129–136. [Google Scholar] [PubMed]
- Hill, C.; Guarner, F.; Reid, G.; Gibson, G.R.; Merenstein, D.J.; Pot, B.; Morelli, L.; Canani, R.B.; Flint, H.J.; Salminen, S.; et al. The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 506–514. [Google Scholar] [CrossRef] [PubMed]
- Butera, A.; Gallo, S.; Maiorani, C.; Molino, D.; Chiesa, A.; Preda, C.; Esposito, F.; Scribante, A. Probiotic Alternative to Chlorhexidine in Periodontal Therapy: Evaluation of Clinical and Microbiological Parameters. Microorganisms 2020, 9, 69. [Google Scholar] [CrossRef] [PubMed]
- Kamińska, K.; Stenclik, D.; Błażejewska, W.; Bogdański, P.; Moszak, M. Probiotics in the Prevention and Treatment of Gestational Diabetes Mellitus (GDM): A Review. Nutrients 2022, 14, 4303. [Google Scholar] [CrossRef] [PubMed]
- Mu, J.; Guo, X.; Zhou, Y.; Cao, G. The Effects of Probiotics/Synbiotics on Glucose and Lipid Metabolism in Women with Gestational Diabetes Mellitus: A Meta-Analysis of Randomized Controlled Trials. Nutrients 2023, 15, 1375. [Google Scholar] [CrossRef] [PubMed]
- Barker, M.; Peters, M.D.J.; Adelson, P.; Steen, M. Probiotics and human lactational mastitis: A scoping review protocol. JBI Evid. Synth. 2020, 18, 1341–1348. [Google Scholar] [CrossRef] [PubMed]
- Mirghafourvand, M.; Homayouni Rad, A.; Mohammad Alizadeh Charandabi, S.; Fardiazar, Z.; Shokri, K. The Effect of Probiotic Yogurt on Constipation in Pregnant Women: A Randomized Controlled Clinical Trial. Iran. Red. Crescent Med. J. 2016, 18, e39870. [Google Scholar] [CrossRef] [PubMed]
- Toh, M.P.S.; Yang, C.Y.; Lim, P.C.; Loh, H.L.J.; Bergonzelli, G.; Lavalle, L.; Mardhy, E.; Samuel, T.M.; Suniega-Tolentino, E.; Silva Zolezzi, I.; et al. A Probiotic Intervention with Bifidobacterium longum NCC3001 on Perinatal Mood Outcomes (PROMOTE Study): Protocol for a Decentralized Randomized Controlled Trial. JMIR Res. Protoc. 2023, 12, e41751. [Google Scholar] [CrossRef] [PubMed]
- Menichini, D.; Chiossi, G.; Monari, F.; De Seta, F.; Facchinetti, F. Supplementation of Probiotics in Pregnant Women Targeting Group B Streptococcus Colonization: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 4520. [Google Scholar] [CrossRef] [PubMed]
- McDougall, A.; Nguyen, R.; Nguyen, P.Y.; Allan, C.; Cheang, S.; Makama, M.; Mills, K.; Hastie, R.; Ammerdorffer, A.; Gulmezoglu, A.M.; et al. The effects of probiotics administration during pregnancy on preeclampsia and associated maternal, fetal and newborn outcomes: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. MFM 2024, 6, 101322. [Google Scholar] [CrossRef] [PubMed]
- Ang, X.Y.; Chung, F.Y.; Lee, B.K.; Azhar, S.N.A.; Sany, S.; Roslan, N.S.; Ahmad, N.; Yusof, S.M.; Abdullah, N.; Nik Ab Rahman, N.N.; et al. Lactobacilli reduce recurrences of vaginal candidiasis in pregnant women: A randomized, double-blind, placebo-controlled study. J. Appl. Microbiol. 2022, 132, 3168–3180. [Google Scholar] [CrossRef] [PubMed]
- Mokkala, K.; Röytiö, H.; Ekblad, U.; Laitinen, K. Opportunities for probiotics and polyunsaturated fatty acids to improve metabolic health of overweight pregnant women. Benef. Microbes. 2017, 8, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Gomez Arango, L.F.; Barrett, H.L.; Callaway, L.K.; Nitert, M.D. Probiotics and pregnancy. Curr. Diabetes Rep. 2015, 15, 567. [Google Scholar] [CrossRef] [PubMed]
- Sheyholislami, H.; Connor, K.L. Are Probiotics and Prebiotics Safe for Use during Pregnancy and Lactation? A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 2382. [Google Scholar] [CrossRef] [PubMed]
- Siciliano, R.A.; Reale, A.; Mazzeo, M.F.; Morandi, S.; Silvetti, T.; Brasca, M. Paraprobiotics: A New Perspective for Functional Foods and Nutraceuticals. Nutrients 2021, 13, 1225. [Google Scholar] [CrossRef] [PubMed]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Maiorani, C.; Milone, A.; Alovisi, M.; Scribante, A. Paraprobiotics in Non-Surgical Periodontal Therapy: Clinical and Microbiological Aspects in a 6-Month Follow-Up Domiciliary Protocol for Oral Hygiene. Microorganisms 2022, 10, 337. [Google Scholar] [CrossRef] [PubMed]
- Scribante, A.; Gallo, S.; Pascadopoli, M.; Frani, M.; Butera, A. Ozonized gels vs chlorhexidine in non-surgical periodontal treatment: A randomized clinical trial. Oral Dis. 2023, in press. [Google Scholar] [CrossRef] [PubMed]
- Almiñana-Pastor, P.J.; Segarra-Vidal, M.; López-Roldán, A.; Alpiste-Illueca, F.M. A controlled clinical study of periodontal health in anticoagulated patients: Assessment of bleeding on probing. J. Clin. Exp. Dent. 2017, 9, e1431–e1438. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, T.J.; Drake, R.B.; Naylor, J.E. The plaque control record. J. Periodontol. 1972, 43, 38. [Google Scholar] [CrossRef] [PubMed]
- He, T.; Qu, L.; Chang, J.; Wang, J. Gingivitis models-relevant approaches to assess oral hygiene products. J. Clin. Dent. 2018, 29, 45–51. [Google Scholar] [PubMed]
- Rosa, M.; Sturzenberger, O.P. Clinical reduction of gingivitis through the use of a mouthwash containing two quaternary ammonium compounds. J. Periodontol. 1976, 47, 535–537. [Google Scholar] [CrossRef] [PubMed]
- Graziani, F.; Cei, S.; Tonetti, M.; Paolantonio, M.; Serio, R.; Sammartino, G.; Gabriele, M.; D’Aiuto, F. Systemic inflammation following non-surgical and surgical periodontal therapy. J. Clin. Periodontol. 2010, 37, 848–854. [Google Scholar] [CrossRef] [PubMed]
- Yarkac, F.U.; Gokturk, O.; Demir, O. Effect of non-surgical periodontal therapy on the degree of gingival inflammation and stress markers related to pregnancy. J. Appl. Oral Sci. 2018, 26, e20170630. [Google Scholar] [CrossRef] [PubMed]
- Piepho, H.P. An Algorithm for a Letter-Based Representation of All-Pairwise Comparisons. J. Comput. Graph. Stat. 2004, 13, 456–466. [Google Scholar] [CrossRef]
- Haas, J.S.; Jackson, R.A.; Fuentes-Afflick, E.; Stewart, A.L.; Dean, M.L.; Brawarsky, P.; Escobar, G.J. Changes in the health status of women during and after pregnancy. J. Gen. Intern. Med. 2005, 20, 45–51. [Google Scholar] [CrossRef]
- O’Dowd, L.K.; Durham, J.; McCracken, G.I.; Preshaw, P.M. Patients’ experiences of the impact of periodontal disease. J. Clin. Periodontol. 2010, 37, 334–339. [Google Scholar] [CrossRef] [PubMed]
- Musskopf, M.L.; Milanesi, F.C.; Rocha, J.M.; Fiorini, T.; Moreira, C.H.C.; Susin, C.; Rösing, C.K.; Weidlich, P.; Oppermann, R.V. Oral health related quality of life among pregnant women: A randomized controlled trial. Braz. Oral Res. 2018, 32, e002. [Google Scholar] [CrossRef] [PubMed]
- Togoo, R.A.; Al-Almai, B.; Al-Hamdi, F.; Huaylah, S.H.; Althobati, M.; Alqarni, S. Knowledge of Pregnant Women about Pregnancy Gingivitis and Children Oral Health. Eur. J. Dent. 2019, 13, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Lazaridi, I.; Zekeridou, A.; Schaub, L.; Prudente, D.; Razban, M.; Giannopoulou, C. A Survey on Oral Health Knowledge, Attitudes and Practices of Pregnant Women Attending Four General Health Hospitals in Switzerland. Oral Health Prev. Dent. 2022, 20, 33. [Google Scholar] [PubMed]
- Liu, P.; Wen, W.; Yu, K.F.; Gao, X.; Lo, E.C.M.; Wong, M.C.M. Effectiveness of a family-centered behavioral and educational counselling approach to improve periodontal health of pregnant women: A randomized controlled trial. BMC Oral Health 2020, 20, 284. [Google Scholar] [CrossRef] [PubMed]
- Figuero, E.; Carrillo-de-Albornoz, A.; Herrera, D.; Bascones-Martínez, A. Gingival changes during pregnancy: I. influence of hormonal variations on clinical and immunological parameters. J. Clin. Periodontol. 2010, 37, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Würtz, P.; Auro, K.; Mäkinen, V.P.; Kangas, A.J.; Soininen, P.; Tiainen, M.; Tynkkynen, T.; Jokelainen, J.; Santalahti, K.; et al. Metabolic profiling of pregnancy: Cross-sectional and longitudinal evidence. BMC Med. 2016, 14, 205. [Google Scholar] [CrossRef] [PubMed]
- Pelzer, E.S.; Allan, J.A.; Theodoropoulos, C.; Ross, T.; Beagley, K.W.; Knox, C.L. Hormone-dependent bacterial growth, persistence and biofilm formation—A pilot study investigating human follicular fluid collected during IVF cycles. PLoS ONE 2012, 7, e49965. [Google Scholar] [CrossRef] [PubMed]
- Balan, P.; Chong, Y.S.; Umashankar, S.; Swarup, S.; Loke, W.M.; Lopez, V.; He, H.G.; Seneviratne, C.J. Keystone Species in Pregnancy Gingivitis: A Snapshot of Oral Microbiome during Pregnancy and Postpartum Period. Front. Microbiol. 2018, 9, 2360. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Kornman, K.; Wgotj, E.A. Periodontitis and adverse pregnancy outcomes: Consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J. Periodontol. 2013, 4, S164–S169. [Google Scholar]
- Erchick, D.J.; Agrawal, N.K.; Khatry, S.K.; Katz, J.; LeClerq, S.C.; Reynolds, M.A.; Mullany, L.C. Adherence to and acceptability of three alcohol-free, antiseptic oral rinses: A community-based pilot randomized controlled trial among pregnant women in rural Nepal. Community Dent. Oral Epidemiol. 2020, 48, 501–512. [Google Scholar] [CrossRef] [PubMed]
- Kraivaphan, P.; Amornchat, C.; Triratana, T. Effects of a triclosan dentifrice on plaque formation, gingivitis and gingival bleeding in pregnant women: Five-month clinical results. Southeast Asian J. Trop. Med. Public. Health 2007, 38, 594–597. [Google Scholar] [PubMed]
- Riley, P.; Lamont, T. Triclosan/copolymer containing toothpastes for oral health. Cochrane Database Syst. Rev. 2013, 2013, CD010514. [Google Scholar] [PubMed]
- Tecco, S.; Nota, A.; D’Amicantonio, T.; Pittari, L.; Monti, M.; Polizzi, E. Effects of an Ozonated Water Irrigator on the Plaque Index and Bleeding Index of Pregnant Women. J. Clin. Med. 2022, 11, 4107. [Google Scholar] [CrossRef] [PubMed]
- Floriani, F.; Jurado, C.A.; Abuhammoud, S.; Vargas, M.; Fischer, N.G.; Rojas-Rueda, S.; Lopes, G.C. A Comparative Study of Shade-Matching Reproducibility Using an Intraoral Scanner and a Spectrophotometer. Dent. J. 2024, 12, 62. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, Y.; Yoshii, D.; Katsuragi, H.; Shinkai, K. Effect of Laser Irradiation Modes and Photosensitizer Types on Antimicrobial Photodynamic Therapy (aPDT) for Streptococcus sobrinus in the Crown Dentin of Bovine Teeth: An Experimental In Vitro Study. Dent. J. 2024, 12, 59. [Google Scholar] [CrossRef] [PubMed]
- Baruwa, A.O.; Chasqueira, F.; Arantes-Oliveira, S.; Caramês, J.; Marques, D.; Portugal, J.; Martins, J.N.R. Comparative Analysis of Endodontic 0.15 Stainless-Steel K-Files: Exploring Design, Composition, and Mechanical Performance. Dent. J. 2024, 12, 29. [Google Scholar] [CrossRef] [PubMed]
- Zhong, C.; Ma, K.N.; Wong, Y.S.; So, Y.; Lee, P.C.; Yang, Y. Oral Health Knowledge of Pregnant Women on Pregnancy Gingivitis and Children’s Oral Health. J. Clin. Pediatr. Dent. 2015, 39, 105–108. [Google Scholar] [CrossRef] [PubMed]
- Novozhilova, N.; Andreeva, E.; Polyakova, M.; Makeeva, I.; Sokhova, I.; Doroshina, V.; Zaytsev, A.; Babina, K. Antigingivitis, Desensitizing, and Antiplaque Effects of Alkaline Toothpastes: A Randomized Clinical Trial. Dent. J. 2023, 11, 96. [Google Scholar] [CrossRef] [PubMed]
- Pakarinen, S.; Saarela, R.K.T.; Välimaa, H.; Heikkinen, A.M.; Kankuri, E.; Noponen, M.; Alapulli, H.; Tervahartiala, T.; Räisänen, I.T.; Sorsa, T.; et al. Home-Applied Dual-Light Photodynamic Therapy in the Treatment of Stable Chronic Periodontitis (HOPE-CP)-Three-Month Interim Results. Dent. J. 2022, 10, 206. [Google Scholar] [CrossRef] [PubMed]
- Elbay, M.; Elbay, Ü.Ş.; Kaya, E.; Kalkan, Ö.P. Effects of photobiomodulation with different application parameters on injection pain in children: A randomized clinical trial. J. Clin. Pediatr. Dent. 2023, 47, 54–62. [Google Scholar] [PubMed]
- Butera, A.; Maiorani, C.; Gallo, S.; Pascadopoli, M.; Venugopal, A.; Marya, A.; Scribante, A. Evaluation of Adjuvant Systems in Non-Surgical Peri-Implant Treatment: A Literature Review. Healthcare 2022, 10, 886. [Google Scholar] [CrossRef] [PubMed]
- Butera, A.; Pascadopoli, M.; Pellegrini, M.; Trapani, B.; Gallo, S.; Radu, M.; Scribante, A. Biomimetic hydroxyapatite paste for molar-incisor hypomineralization: A randomized clinical trial. Oral Dis. 2023, 2, 2789–2798. [Google Scholar] [CrossRef] [PubMed]
- Strickland, M.; Mills, S.; Dasari, B.; Markowitz, K.; Cugini, C. Design and Initial Evaluation of a Novel Oral Hygiene Technology for a Special Needs Population: A New Way to Clean. Dent. J. 2023, 11, 224. [Google Scholar] [CrossRef] [PubMed]
- Gururatana, O.; Vejvithee, W.; Ekpatcha, N. Multicenter Randomized Controlled Trial Comparing the Contribution of Proxabrushes with Regular Toothbrushes and Only Regular Toothbrushes to the Oral Health of Thai Elderly. Int. J. Dent. 2022, 2022, 5323092. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Pregnancy Period at the Enrollment (Months) | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|
| Control | 1 (3.33) | 2 (6.67) | 2 (6.67) | 4 (13.33) | 3 (10.00) | 3 (10.00) |
| Test | 4 (13.33) | 3 (10.00) | 2 (6.67) | 1 (3.33) | 3 (10.00) | 2 (6.67) |
| Total | 5 (16.67) | 5 (16.67) | 4 (13.33) | 5 (16.67) | 6 (20.00) | 5 (16.67) |
| Previous Pregnancies (Number) | None (0) | One (1) |
|---|---|---|
| Control | 8 (26.67) | 7 (23.33) |
| Test | 9 (30.00) | 6 (20.00) |
| Total | 17 (56.67) | 13 (43.33) |
| Caesarean delivery (yes/no) | Yes | No |
| Control | 4 (13.33) | 3 (10.00) |
| Test | 2 (6.67) | 4 (13.33) |
| Total | 6 (20.00) | 7 (23.33) |
| Product | Manufacturer | Composition |
|---|---|---|
| Biorepair® Peribioma® Pro | Coswell S.p.A., Funo di Argelato, BO, Italy | Bifidobacterium*, Lactobacillus*, Zinc Hydroxyapatite*, Sodium Benzoate, Glycerin, Sodium Myristoyl Sarcosinate, Pistacia Lentiscus (Mastic) Gum Oil, Aroma, Sodium Hyaluronate, Hydrated Silica, Sodium Saccharin, Cocamidopropyl Betaine, Maltodextrin, Hamamelis Virginiana Leaf Extract, Helianthus Annuus Seed Oil, Sorbitol, Spirulina Platensis Extract, Benzyl Alcohol, CI 73360, Tocopheryl Acetate, Phenoxyethanol, Calendula Officinalis Flower Extract, Silica, Limonene, Eucaliptus Globulus Leaf Oil, Retynil Palmitate, CI 77891, Ascorbic Acid, Cellulose Gum, Potassium Sorbate. *: microRepair® |
| Mousse Mouthwash Biorepair® Peribioma® | Coswell S.p.A., Funo di Argelato, BO, Italy | Bifidobacterium*, Lactobacillus*, Zinc Hydroxyapatite*, Sodium Hyaluronate, Glycerin, Hamamelis Virginiana Leaf Extract, Eucalyptus Globulus Leaf Oil, Ascorbic Acid, Aqua, Sodium Saccharin, Calendula Officinalis Flower Extract, Pistacia Lentiscus (Mastic) Gum Oil, Tocopheryl Acetate, Maltodextrin, Phenoxyethanol, Retinyl Palmitate, Spirulina Platensis Extract, Helianthus Annuus Seed Oil, Sodium Benzoate, CI 16255, Sorbitol, Cocamidopropyl Betaine, Xylitol, Sodium Benzoate, Potassium Sorbate, PEG-40 Hydrogenated Castor Oil, Aroma, CI 16255, Limonene, BHT. *: microRepair® |
| Group | Time | Mean | St Dev | Min | Median | Max | Significance * |
|---|---|---|---|---|---|---|---|
| Control | T0 | 2.63 | 0.44 | 2.02 | 2.57 | 3.60 | A |
| T1 | 2.50 | 0.49 | 2.00 | 2.40 | 3.31 | A | |
| T2 | 2.62 | 0.46 | 2.00 | 2.66 | 3.26 | A | |
| T3 | 2.44 | 0.40 | 2.00 | 2.50 | 3.04 | A | |
| Test | T0 | 2.73 | 0.29 | 2.17 | 2.78 | 3.18 | A |
| T1 | 2.90 | 0.26 | 2.45 | 2.84 | 3.29 | A | |
| T2 | 2.80 | 0.36 | 2.14 | 2.82 | 3.28 | A | |
| T3 | 2.66 | 0.43 | 2.05 | 2.60 | 3.36 | A |
| Group | Time | Mean | St Dev | Min | Median | Max | Significance * |
|---|---|---|---|---|---|---|---|
| Control | T0 | 2.62 | 0.45 | 1.98 | 2.57 | 3.60 | A |
| T1 | 2.49 | 0.50 | 2.00 | 2.34 | 3.31 | A | |
| T2 | 2.61 | 0.46 | 2.00 | 2.61 | 3.26 | A | |
| T3 | 2.43 | 0.40 | 2.00 | 2.50 | 3.04 | A | |
| Test | T0 | 2.71 | 0.28 | 2.17 | 2.74 | 3.18 | A |
| T1 | 2.88 | 0.26 | 2.45 | 2.84 | 3.29 | A | |
| T2 | 2.78 | 0.36 | 2.14 | 2.82 | 3.28 | A | |
| T3 | 2.65 | 0.45 | 2.00 | 2.60 | 3.36 | A |
| Group | Time | Mean | St Dev | Min | Median | Max | Significance * |
|---|---|---|---|---|---|---|---|
| Control | T0 | 71.60 | 24.86 | 20.00 | 70.00 | 100.00 | A,B |
| T1 | 36.60 | 23.35 | 4,.00 | 34.00 | 76.00 | C | |
| T2 | 28.21 | 23.24 | 0.00 | 20.00 | 75.00 | C | |
| T3 | 32.67 | 17.43 | 4.00 | 34.50 | 60.00 | C | |
| Test | T0 | 76.07 | 28.99 | 26.00 | 100.00 | 100.00 | A |
| T1 | 53.20 | 23.38 | 10.00 | 50.00 | 100.00 | A,B,C | |
| T2 | 48.67 | 20.99 | 16.00 | 50.00 | 100.00 | B,C | |
| T3 | 40.54 | 18.89 | 16.00 | 45.00 | 75.00 | C |
| Group | Time | Mean | St Dev | Min | Median | Max | Significance * |
|---|---|---|---|---|---|---|---|
| Control | T0 | 47.80 | 37.87 | 1.00 | 45.00 | 100.00 | A,B,C |
| T1 | 35.33 | 33.55 | 0.00 | 28.00 | 100.00 | A,C | |
| T2 | 27.50 | 17.92 | 0.00 | 28.00 | 60.00 | A,C | |
| T3 | 21.92 | 18.61 | 0.00 | 16.00 | 56.00 | A,C | |
| Test | T0 | 68.80 | 37.64 | 5.00 | 100.00 | 100.00 | B |
| T1 | 44.13 | 30.05 | 0.00 | 50.00 | 100.00 | B,C | |
| T2 | 31.33 | 19.10 | 5.00 | 30.00 | 67.00 | C | |
| T3 | 31.08 | 29.42 | 5.00 | 20.00 | 100.00 | C |
| Group | Time | Mean | St Dev | Min | Median | Max | Significance * |
|---|---|---|---|---|---|---|---|
| Control | T0 | 1.79 | 0.55 | 0.83 | 2.00 | 3.00 | A |
| T1 | 1.45 | 0.72 | 0.00 | 1.57 | 3.00 | A | |
| T2 | 1.44 | 0.83 | 0.00 | 1.50 | 2.50 | A | |
| T3 | 1.47 | 0.81 | 0.00 | 1.84 | 2.50 | A | |
| Test | T0 | 1.76 | 0.51 | 1.00 | 2.00 | 2.56 | A |
| T1 | 1.81 | 0.54 | 1.00 | 2.00 | 3.00 | A | |
| T2 | 1.68 | 0.52 | 1.00 | 1.90 | 2.83 | A | |
| T3 | 1.64 | 0.48 | 1.00 | 1.52 | 2.47 | A |
| Group | Time | Mean | St Dev | Min | Median | Max | Significance * |
|---|---|---|---|---|---|---|---|
| Control | T0 | 1.67 | 0.72 | 0.00 | 2.00 | 3.00 | A |
| T1 | 1.53 | 0.85 | 0.00 | 2.00 | 3.00 | A | |
| T2 | 1.43 | 0.83 | 0.00 | 1.50 | 3.00 | A | |
| T3 | 1.42 | 0.90 | 0.00 | 1.50 | 3.00 | A | |
| Test | T0 | 1.67 | 0.44 | 1.00 | 2.00 | 2.00 | A |
| T1 | 1.60 | 0.42 | 1.00 | 1.52 | 2.00 | A | |
| T2 | 1.58 | 0.44 | 1.00 | 1.52 | 2.00 | A | |
| T3 | 1.64 | 0.43 | 1.00 | 2.00 | 2.00 | A |
| Group | Time | Mean | St Dev | Min | Median | Max | Significance * |
|---|---|---|---|---|---|---|---|
| Control | T0 | 0.57 | 0.90 | 0.00 | 0.00 | 2.50 | A |
| T1 | 0.64 | 0.89 | 0.00 | 0.00 | 2.50 | A | |
| T2 | 0.69 | 0.91 | 0.00 | 0.00 | 2.50 | A | |
| T3 | 0.80 | 0.94 | 0.00 | 0.50 | 2.50 | A | |
| Test | T0 | 0.58 | 1.08 | 0.00 | 0.00 | 3.33 | A |
| T1 | 0.53 | 0.96 | 0.00 | 0.00 | 2.60 | A | |
| T2 | 0.52 | 0.93 | 0.00 | 0.00 | 2.40 | A | |
| T3 | 0.53 | 1.01 | 0.00 | 0.00 | 2.60 | A |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Butera, A.; Pascadopoli, M.; Nardi, M.G.; Ogliari, C.; Chiesa, A.; Preda, C.; Perego, G.; Scribante, A. Clinical Use of Paraprobiotics for Pregnant Women with Periodontitis: Randomized Clinical Trial. Dent. J. 2024, 12, 116. https://doi.org/10.3390/dj12040116
Butera A, Pascadopoli M, Nardi MG, Ogliari C, Chiesa A, Preda C, Perego G, Scribante A. Clinical Use of Paraprobiotics for Pregnant Women with Periodontitis: Randomized Clinical Trial. Dentistry Journal. 2024; 12(4):116. https://doi.org/10.3390/dj12040116
Chicago/Turabian StyleButera, Andrea, Maurizio Pascadopoli, Maria Gloria Nardi, Chiara Ogliari, Alessandro Chiesa, Camilla Preda, Giulia Perego, and Andrea Scribante. 2024. "Clinical Use of Paraprobiotics for Pregnant Women with Periodontitis: Randomized Clinical Trial" Dentistry Journal 12, no. 4: 116. https://doi.org/10.3390/dj12040116
APA StyleButera, A., Pascadopoli, M., Nardi, M. G., Ogliari, C., Chiesa, A., Preda, C., Perego, G., & Scribante, A. (2024). Clinical Use of Paraprobiotics for Pregnant Women with Periodontitis: Randomized Clinical Trial. Dentistry Journal, 12(4), 116. https://doi.org/10.3390/dj12040116