
Concordance of Fathers and Mothers in the Assessment of Their 5-Year-Old Child’s Dental Fear

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| When Response Option ”No Experience” Was Not Included | ||||||||
|---|---|---|---|---|---|---|---|---|
| Mothers | Fathers | |||||||
| Item | n | Mean | SD | Median | n | Mean | SD | Median |
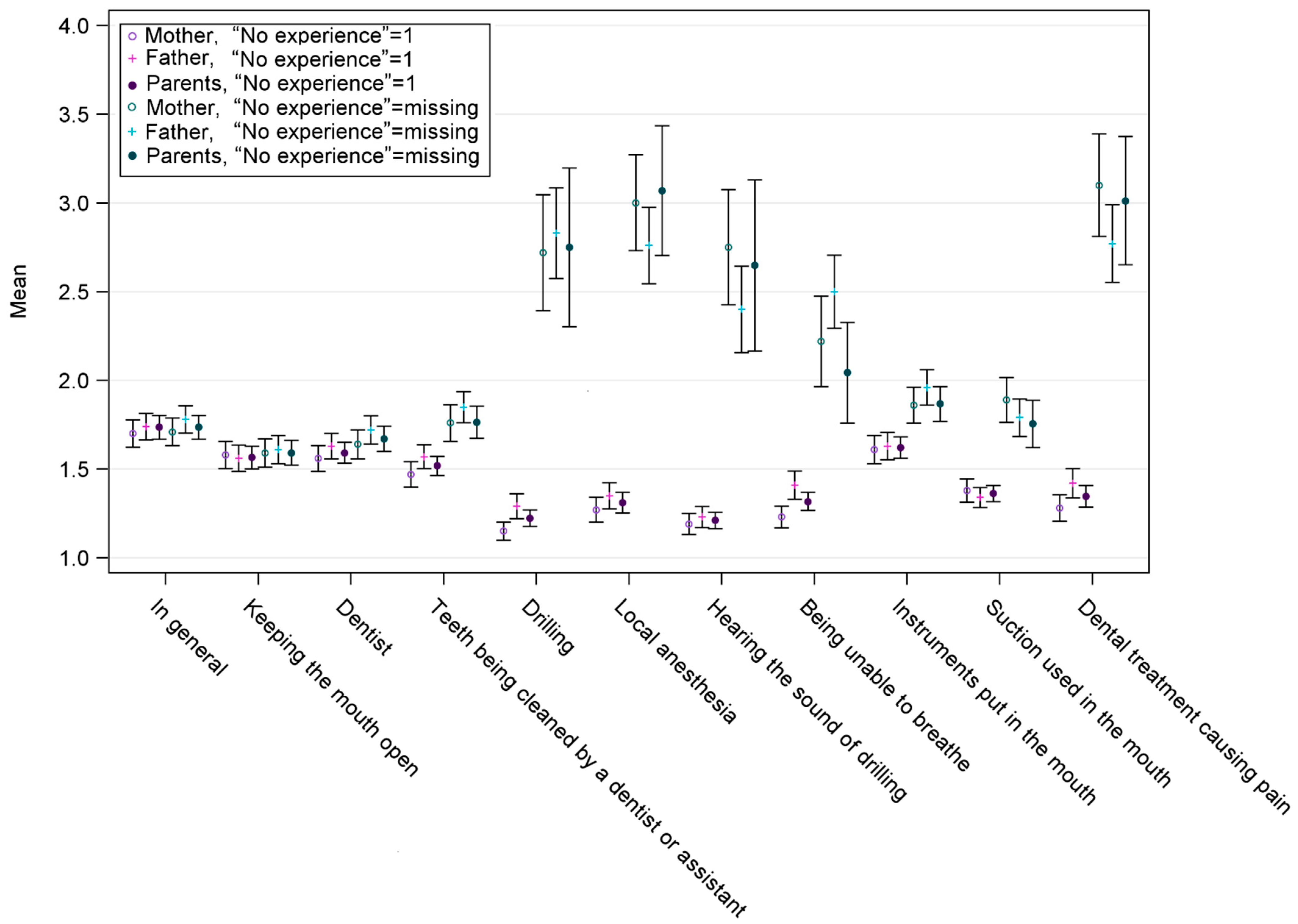
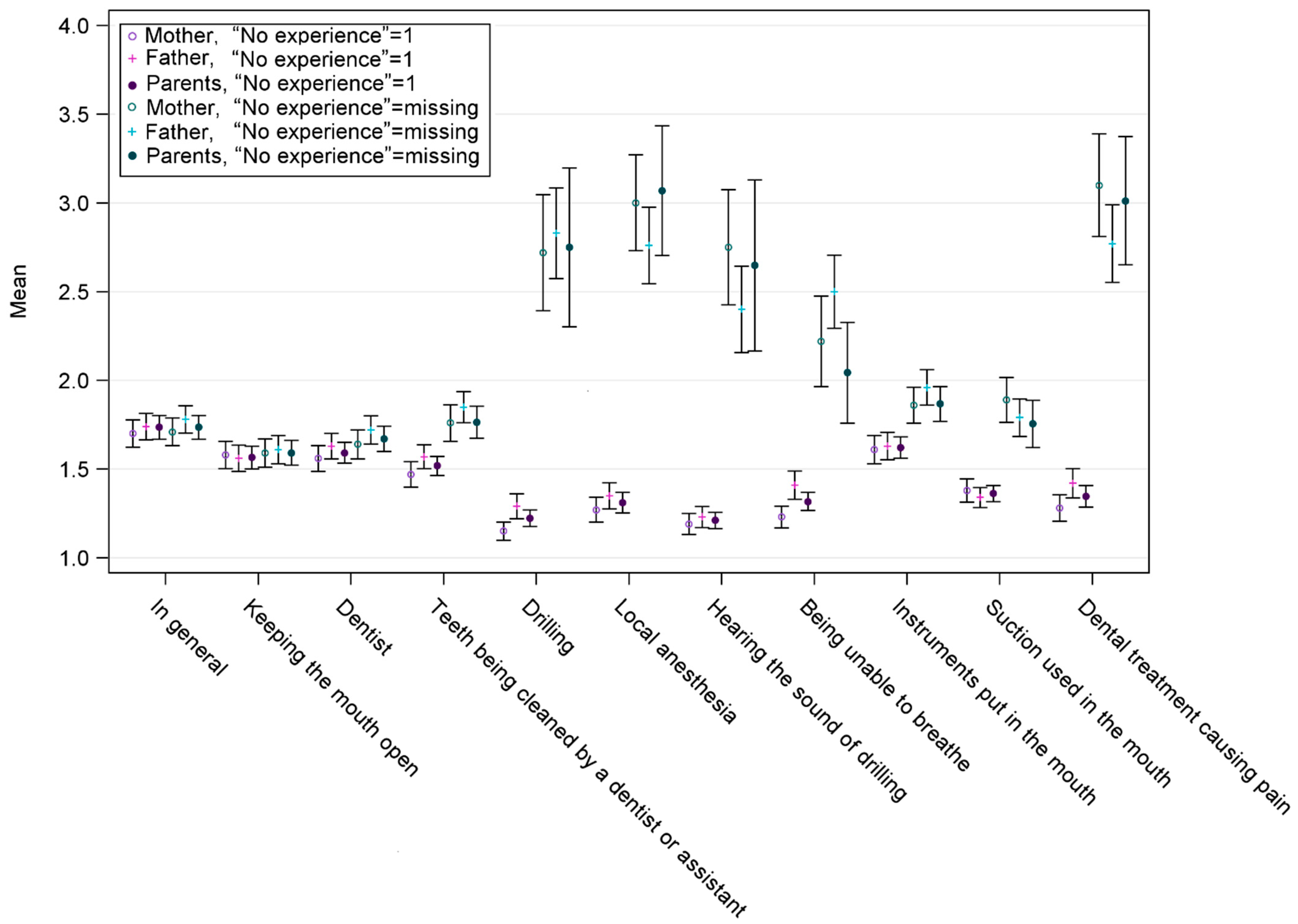
| In general | 503 | 1.7 | 0.89 | 1 | 484 | 1.8 | 0.86 | 2 |
| Keeping the mouth open | 496 | 1.6 | 0.91 | 1 | 468 | 1.6 | 0.86 | 1 |
| Dentist | 447 | 1.6 | 0.87 | 1 | 445 | 1.7 | 0.85 | 2 |
| Teeth being cleaned by a dentist or assistant | 317 | 1.8 | 0.95 | 2 | 345 | 1.8 | 0.83 | 2 |
| Drilling | 46 | 2.7 | 1.13 | 3 | 81 | 2.8 | 1.17 | 3 |
| Local anesthesia | 70 | 3.0 | 1.16 | 3 | 101 | 2.8 | 1.11 | 3 |
| Hearing the sound of drilling | 56 | 2.8 | 1.24 | 3 | 83 | 2.4 | 1.13 | 2 |
| Being unable to breathe | 95 | 2.2 | 1.27 | 2 | 138 | 2.5 | 1.23 | 2 |
| Instruments put in the mouth | 362 | 1.9 | 0.99 | 2 | 336 | 2.0 | 0.94 | 2 |
| Suction used in the mouth | 219 | 1.9 | 0.95 | 2 | 220 | 1.8 | 0.79 | 2 |
| Dental treatment causing pain | 68 | 3.1 | 1.22 | 3 | 121 | 2.8 | 1.22 | 3 |
| When Response Option ”No Experience” Was Included (6 = 1) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Mothers | Fathers | |||||||
| Item | n | Mean | SD | Median | n | Mean | SD | Median |
| In general | 514 | 1.7 | 0.9 | 1 | 514 | 1.7 | 0.9 | 2 |
| Keeping the mouth open | 513 | 1.6 | 0.9 | 1 | 512 | 1.6 | 0.9 | 1 |
| Dentist | 514 | 1.6 | 0.8 | 1 | 514 | 1.6 | 0.8 | 1 |
| Teeth being cleaned by a dentist or assistant | 513 | 1.5 | 0.8 | 1 | 514 | 1.6 | 0.9 | 1 |
| Drilling | 510 | 1.2 | 0.6 | 1 | 513 | 1.3 | 0.8 | 1 |
| Local anesthesia | 511 | 1.3 | 0.8 | 1 | 511 | 1.3 | 0.9 | 1 |
| Hearing the sound of drilling | 510 | 1.2 | 0.7 | 1 | 512 | 1.2 | 0.7 | 1 |
| Being unable to breathe | 511 | 1.2 | 0.8 | 1 | 511 | 1.4 | 0.9 | 1 |
| Instruments put in the mouth | 510 | 1.6 | 0.9 | 1 | 510 | 1.6 | 0.9 | 1 |
| Suction used in the mouth | 510 | 1.4 | 0.8 | 1 | 511 | 1.3 | 0.6 | 1 |
| Dental treatment causing pain | 508 | 1.3 | 0.8 | 1 | 513 | 1.4 | 1.0 | 1 |
| When Response Option ”No Experience” Was Not Included | ||||
|---|---|---|---|---|
| Mean Sum of Mothers and Fathers | ||||
| Item | n | Mean | SD | Median |
| In general | 475 | 1.7 | 0.76 | 1.5 |
| Keeping the mouth open | 455 | 1.6 | 0.78 | 1.5 |
| Dentist | 397 | 1.7 | 0.726 | 1.5 |
| Teeth being cleaned by a dentist or assistant | 236 | 1.8 | 0.716 | 1.5 |
| Drilling | 16 | 2.8 | 0.916 | 2.8 |
| Local anesthesia | 29 | 3.1 | 1.01 | 3.0 |
| Hearing the sound of drilling | 17 | 2.6 | 1.01 | 3.0 |
| Being unable to breathe | 35 | 2.0 | 0.86 | 2.0 |
| Instruments put in the mouth | 247 | 1.9 | 0.78 | 1.5 |
| Suction used in the mouth | 110 | 1.8 | 0.71 | 1.5 |
| Dental treatment causing pain | 28 | 3.0 | 0.98 | 3.0 |
| When Response Option ”No Experience” Was Included 6 = 1 | ||||
|---|---|---|---|---|
| Mean Sum of Mothers and Fathers | ||||
| Item | n | Mean | SD | Median |
| In general | 475 | 1.7 | 0.75 | 1.5 |
| Keeping the mouth open | 512 | 1.6 | 0.76 | 1.5 |
| Dentist | 512 | 1.6 | 0.68 | 1.5 |
| Teeth being cleaned by a dentist or assistant | 513 | 1.5 | 0.63 | 1.5 |
| Drilling | 509 | 1.2 | 0.53 | 1.0 |
| Local anesthesia | 508 | 1.3 | 0.67 | 1.0 |
| Hearing the sound of drilling | 508 | 1.2 | 0.52 | 1.0 |
| Being unable to breathe | 508 | 1.3 | 0.59 | 1.0 |
| Instruments put in the mouth | 506 | 1.6 | 0.69 | 1.5 |
| Suction used in the mouth | 507 | 1.4 | 0.53 | 1.0 |
| Dental treatment causing pain | 507 | 1.3 | 0.69 | 1.0 |
References
- Klingberg, G.; Broberg, A.G. Dental fear/anxiety and dental behaviour management problems in children and adolescents: A review of prevalence and concomitant psychological factors. Int. J. Paediatr. Dent. 2007, 17, 391–406. [Google Scholar] [CrossRef]
- Kroniņa, L.; Rasčevska, M.; Care, R. Psychosocial factors correlated with children’s dental anxiety. Stomatologija 2017, 19, 84–90. [Google Scholar]
- Busato, P.; Garbín, R.R.; Santos, C.N.; Paranhos, L.R.; Rigo, L. Influence of maternal anxiety on child anxiety during dental care: Cross-sectional study. Sao Paulo Med. J. 2017, 135, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Wong, H.M.; Zhang, Y.Y.; Perfecto, A.; McGrath, C.P.J. Dental fear association between mothers and adolescents—A longitudinal study. PeerJ 2020, 8, e9154. [Google Scholar] [CrossRef]
- Majstorovic, M.; Morse, D.; Do, D.; Lim, L.; Herman, N.; Moursi, A. Indicators of Dental Anxiety in Children Just Prior to Treatment. J. Clin. Pediatr. Dent. 2014, 39, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Šimunović, L.; Špiljak, B.; Radulović, M.; Vlahovljak, A.; Ostojić, M.; Krlev, J.; Ibrahimpašić, A.; Vranić, L.; Negovetić Vranić, D. Relationship between Children’s and Parents’ Dental Anxiety: A Cross-Sectional Study on the Six European Countries. Dent. J. 2022, 10, 209. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Gao, X. Children’s dental fear and anxiety: Exploring family related factors. BMC Oral Health 2018, 18, 100. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, A.; Arnrup, K.; Broberg, A.G.; Bodin, L.; Berggren, U. Child dental fear as measured with the Dental Subscale of the Children’s Fear Survey Schedule: The impact of referral status and type of informant (child versus parent). Community Dent. Oral Epidemiol. 2010, 38, 256–266. [Google Scholar] [CrossRef] [PubMed]
- McNeil, D.W.; Randall, C.L.; Cohen, L.L.; Crout, R.J.; Weyant, R.J.; Neiswanger, K.; Marazita, M.L. Transmission of dental fear from parent to adolescent in an Appalachian sample in the USA. Int. J. Paediatr. Dent. 2019, 29, 720–727. [Google Scholar] [CrossRef] [PubMed]
- Fu, S.-W.; Li, S.; Shi, Z.-Y.; He, Q.-L. Interrater agreement between children’s self-reported and their mothers’ proxy-reported dental anxiety: A Chinese cross-sectional study. BMC Oral Health 2023, 23, 139. [Google Scholar] [CrossRef]
- Luoto, A.; Tolvanen, M.; Pohjola, V.; Rantavuori, K.; Karlsson, L.; Lahti, S. A longitudinal study of changes and associations in dental fear in parent/adolescent dyads. Int. J. Paediatr. Dent. 2017, 27, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Patel, H.; Reid, C.; Wilson, K.; Girdler, N.M. Inter-rater agreement between children’s self-reported and parents’ proxy-reported dental anxiety. Br. Dent. J. 2015, 218, E6. [Google Scholar] [CrossRef]
- Van Holland De Graaf, J.; Hoogenboom, M.; De Roos, S.; Bucx, F. Socio-demographic Correlates of Fathers’ and Mothers’ Parenting Behaviors. J. Child Fam. Stud. 2018, 27, 2315–2327. [Google Scholar] [CrossRef]
- Jerrim, J.; Prieto-Latorre, C.; Lopez-Agudo, L.A.; Marcenaro-Gutierrez, O.D. Do school preferences differ between mothers and fathers? International evidence from PISA. Oxf. Rev. Educ. 2023, 1–18. [Google Scholar] [CrossRef]
- Riina, E.M.; Feinberg, M.E. Involvement in Childrearing and Mothers’ and Fathers’ Adjustment. Fam. Relat. 2012, 61, 836–850. [Google Scholar] [CrossRef]
- Boonk, L.; Gijselaers, H.J.M.; Ritzen, H.; Brand-Gruwel, S. A review of the relationship between parental involvement indicators and academic achievement. Educ. Res. Rev. 2018, 24, 10–30. [Google Scholar] [CrossRef]
- Dockery, A.M.; Koshy, P.; Li, I.W. Parental expectations of children’s higher education participation in Australia. Br. Educ. Res. J. 2022, 48, 617–639. [Google Scholar] [CrossRef]
- Tollili, C.; Katsouda, M.; Coolidge, T.; Kotsanos, N.; Karagiannis, V.; Arapostathis, K.N. Child dental fear and past dental experience: Comparison of parents’ and children’s ratings. Eur. Arch. Paediatr. Dent. 2020, 21, 597–608. [Google Scholar] [CrossRef]
- Lara, A.; Crego, A.; Romero-Maroto, M. Emotional contagion of dental fear to children: The fathers’ mediating role in parental transfer of fear: Emotional contagion of dental fear to children. Int. J. Paediatr. Dent. 2012, 22, 324–330. [Google Scholar] [CrossRef]
- Bögels, S.; Phares, V. Fathers’ role in the etiology, prevention and treatment of child anxiety: A review and new model. Clin. Psychol. Rev. 2008, 28, 539–558. [Google Scholar] [CrossRef] [PubMed]
- Lahti, S.; Tuutti, H.; Honkala, V. The relationship of parental dental anxiety and child’s caries status. ASDC J. Dent. Child. 1989, 56, 191–195. [Google Scholar]
- Uziel, N.; Meyerson, J.; Kuskasy, M.; Gilon, E.; Eli, I. The Influence of Family Milieu on Dental Anxiety in Adolescents—A Cross Sectional Study. J. Clin. Med. 2023, 12, 2174. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, L.; Tolvanen, M.; Scheinin, N.M.; Uusitupa, H.M.; Korja, R.; Ekholm, E.; Tuulari, J.J.; Pajulo, M.; Huotilainen, M.; Paunio, T.; et al. Cohort Profile: The FinnBrain Birth Cohort Study (FinnBrain). Int. J. Epidemiol. 2018, 47, 15–16j. [Google Scholar] [CrossRef] [PubMed]
- Rantavuori, K.; Tolvanen, M.; Lahti, S. Confirming the factor structure of modified CFSS-DS in Finnish children at different ages. Acta Odontol. Scand. 2012, 70, 421–425. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Rantavuori, K.; Lahti, S.; Hausen, H.; Seppä, L.; Kärkkäinen, S. Dental fear and oral health and family characteristics of Finnish children. Acta Odontol. Scand. 2004, 62, 207–213. [Google Scholar] [CrossRef]
- Suominen-Taipale, A.L.; Widström, E.; Sund, R. Association of Examination Rates with Children’s National Caries Indices in Finland. Open Dent. J. 2009, 3, 59–67. [Google Scholar] [CrossRef]
- Luoto, A.; Tolvanen, M.; Rantavuori, K.; Pohjola, V.; Karlsson, L.; Lahti, S. Individual changes in dental fear among children and parents: A longitudinal study. Acta Odontol. Scand. 2014, 72, 942–947. [Google Scholar] [CrossRef]
- Huttunen, J.; Eerola, P. Finland. In Father Involvement in the Early Years. An International Comparison of Policy and Practice, 1st ed.; Adler, M.A., Lenz, K., Eds.; Bristol University Press: Bristol, UK, 2016; pp. 29–60. [Google Scholar]
- Neshteruk, C.D.; Jones, D.J.; Skinner, A.; Ammerman, A.; Tate, D.F.; Ward, D.S. Understanding the Role of Fathers in Children’s Physical Activity: A Qualitative Study. J. Phys. Act. Health 2020, 17, 540–547. [Google Scholar] [CrossRef]
- Hagqvist, O.; Tolvanen, M.; Rantavuori, K.; Karlsson, L.; Karlsson, H.; Lahti, S. Changes in dental fear and its relations to anxiety and depression in the FinnBrain Birth Cohort Study. Eur. J. Oral Sci. 2020, 128, 429–435. [Google Scholar] [CrossRef]
- Armfield, J.M.; Crego, A.; Schich, H.S.; Luzzi, L. The role of cognitions in short-term temporal changes in dental fear among Australian adults. J. Public Health Dent. 2018, 78, 32–40. [Google Scholar] [CrossRef]
| Item | Not Afraid | A Little Afraid | Afraid to Some Degree | Quite Afraid | Very Afraid | No Experience | Missing | ||
|---|---|---|---|---|---|---|---|---|---|
| n | % | % | % | % | % | % | % | ||
| In general | M | 514 | 49.4 | 32.7 | 12.3 | 1.6 | 1.9 | 2.1 | 0 |
| F | 514 | 42.8 | 33.3 | 14.2 | 3.5 | 0.4 | 5.8 | 0 | |
| Keeping the | M | 513 | 58.6 | 25.3 | 7.8 | 2.9 | 1.9 | 3.3 | 0.2 |
| mouth open | F | 512 | 53.7 | 24.7 | 8.4 | 3.1 | 1.2 | 8.6 | 0.4 |
| Dentist | M | 514 | 47.9 | 26.8 | 9.1 | 1.6 | 1.6 | 13 | 0 |
| F | 514 | 41.2 | 32.3 | 9.3 | 3.1 | 0.6 | 13.4 | 0 | |
| Teeth being cleaned by a | M | 513 | 30.4 | 20.8 | 7.2 | 1.8 | 1.6 | 38.1 | 0.2 |
| dentist or assistant | F | 514 | 26.1 | 27.6 | 11.3 | 1.8 | 0.4 | 32.9 | 0 |
| Drilling | M | 510 | 1.8 | 1.6 | 3.5 | 1.8 | 0.4 | 90.3 | 0.8 |
| F | 513 | 2.3 | 4.1 | 4.5 | 3.7 | 1.2 | 84.0 | 0.2 | |
| Local | M | 511 | 1.9 | 1.8 | 5.6 | 2.9 | 1.4 | 85.8 | 0.6 |
| anesthesia | F | 511 | 3.1 | 4.3 | 7.6 | 3.5 | 1.2 | 79.8 | 0.6 |
| Hearing the sound of | M | 510 | 2.3 | 1.9 | 3.7 | 1.9 | 1.0 | 88.3 | 0.8 |
| drilling | F | 512 | 4.3 | 4.7 | 4.1 | 2.7 | 0.4 | 83.5 | 0.4 |
| Being unable | M | 511 | 7.2 | 4.7 | 3.1 | 2.3 | 1.2 | 80.9 | 0.6 |
| to breathe | F | 511 | 7.2 | 7.0 | 6.4 | 4.5 | 1.8 | 72.6 | 0.6 |
| Instruments put in the | M | 510 | 31.3 | 24.9 | 8.9 | 3.5 | 1.8 | 28.8 | 0.8 |
| mouth | F | 510 | 22.2 | 30.2 | 8.0 | 3.5 | 1.6 | 33.9 | 0.8 |
| Suction used | M | 510 | 17.3 | 15.8 | 7.0 | 1.8 | 0.8 | 56.6 | 0.8 |
| in the mouth | F | 511 | 17.5 | 18.3 | 5.6 | 1.4 | 0 | 56.6 | 0.6 |
| Dental treatment | M | 508 | 1.8 | 2.3 | 3.5 | 4.1 | 1.6 | 85.6 | 1.2 |
| causing pain | F | 513 | 3.5 | 7.4 | 6.6 | 3.1 | 2.9 | 76.3 | 0.2 |
| Item | n | % Agreement | Kappa | % Father > Mother | % Mother > Father | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| A | B | A | B | A | B | A | B | A | B | |
| In general | 514 | 475 | 45.7 | 49.1 | 0.178 | 0.192 | 32.1 | 28.8 | 22.2 | 22.1 |
| Keeping the mouth open | 512 | 455 | 51.4 | 56.9 | 0.203 | 0.229 | 28.9 | 23.7 | 19.7 | 19.3 |
| Dentist | 514 | 397 | 40.3 | 47.4 | 0.133 | 0.131 | 33.3 | 30.5 | 26.5 | 22.2 |
| Teeth being cleaned by a dentist or assistant | 513 | 236 | 40.4 | 50.4 | 0.181 | 0.224 | 29.8 | 30.5 | 29.8 | 19.1 |
| Drilling | 509 | 16 | 79.8 | 43.8 | 0.120 | 0.258 | 6.9 | 31.3 | 13.4 | 25.0 |
| Local anesthesia | 508 | 29 | 74.6 | 37.9 | 0.151 | 0.154 | 9.3 | 24.1 | 16.1 | 37.9 |
| Hearing the sound of drilling | 508 | 17 | 77.6 | 41.2 | 0.102 | 0.213 | 9.3 | 47.1 | 13.2 | 11.8 |
| Being unable to breathe | 508 | 35 | 63.4 | 31.4 | 0.072 | 0.058 | 15.4 | 51.4 | 21.3 | 17.1 |
| Instruments put in the mouth | 506 | 247 | 34.0 | 45.7 | 0.115 | 0.183 | 38.1 | 32.4 | 27.9 | 21.9 |
| Suction used in the mouth | 507 | 110 | 46.5 | 50.9 | 0.126 | 0.231 | 26.0 | 21.8 | 27.4 | 27.3 |
| Dental treatment causing pain | 507 | 28 | 70.8 | 35.7 | 0.114 | 0.163 | 9.5 | 28.6 | 19.7 | 35.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seppänen, S.; Vuorenmaa, K.; Suominen, A.; Ogawa, M.; Pohjola, V.; Rantavuori, K.; Karlsson, H.; Karlsson, L.; Lahti, S. Concordance of Fathers and Mothers in the Assessment of Their 5-Year-Old Child’s Dental Fear. Dent. J. 2024, 12, 53. https://doi.org/10.3390/dj12030053
Seppänen S, Vuorenmaa K, Suominen A, Ogawa M, Pohjola V, Rantavuori K, Karlsson H, Karlsson L, Lahti S. Concordance of Fathers and Mothers in the Assessment of Their 5-Year-Old Child’s Dental Fear. Dentistry Journal. 2024; 12(3):53. https://doi.org/10.3390/dj12030053
Chicago/Turabian StyleSeppänen, Sanna, Kukka Vuorenmaa, Auli Suominen, Mika Ogawa, Vesa Pohjola, Kari Rantavuori, Hasse Karlsson, Linnea Karlsson, and Satu Lahti. 2024. "Concordance of Fathers and Mothers in the Assessment of Their 5-Year-Old Child’s Dental Fear" Dentistry Journal 12, no. 3: 53. https://doi.org/10.3390/dj12030053
APA StyleSeppänen, S., Vuorenmaa, K., Suominen, A., Ogawa, M., Pohjola, V., Rantavuori, K., Karlsson, H., Karlsson, L., & Lahti, S. (2024). Concordance of Fathers and Mothers in the Assessment of Their 5-Year-Old Child’s Dental Fear. Dentistry Journal, 12(3), 53. https://doi.org/10.3390/dj12030053