
Access to Dental Care for Children and Young People in Care and Care Leavers: A Global Scoping Review

 , , , , , ,
, , , , , ,
Abstract
1. Introduction
2. Methods
2.1. Inclusion and Exclusion Criteria
2.2. Search Strategy
2.3. Study Records
2.3.1. Data Management/Selection Process
2.3.2. Data Extraction
2.3.3. Data Synthesis
2.4. Patient and Public Involvement (PPI)
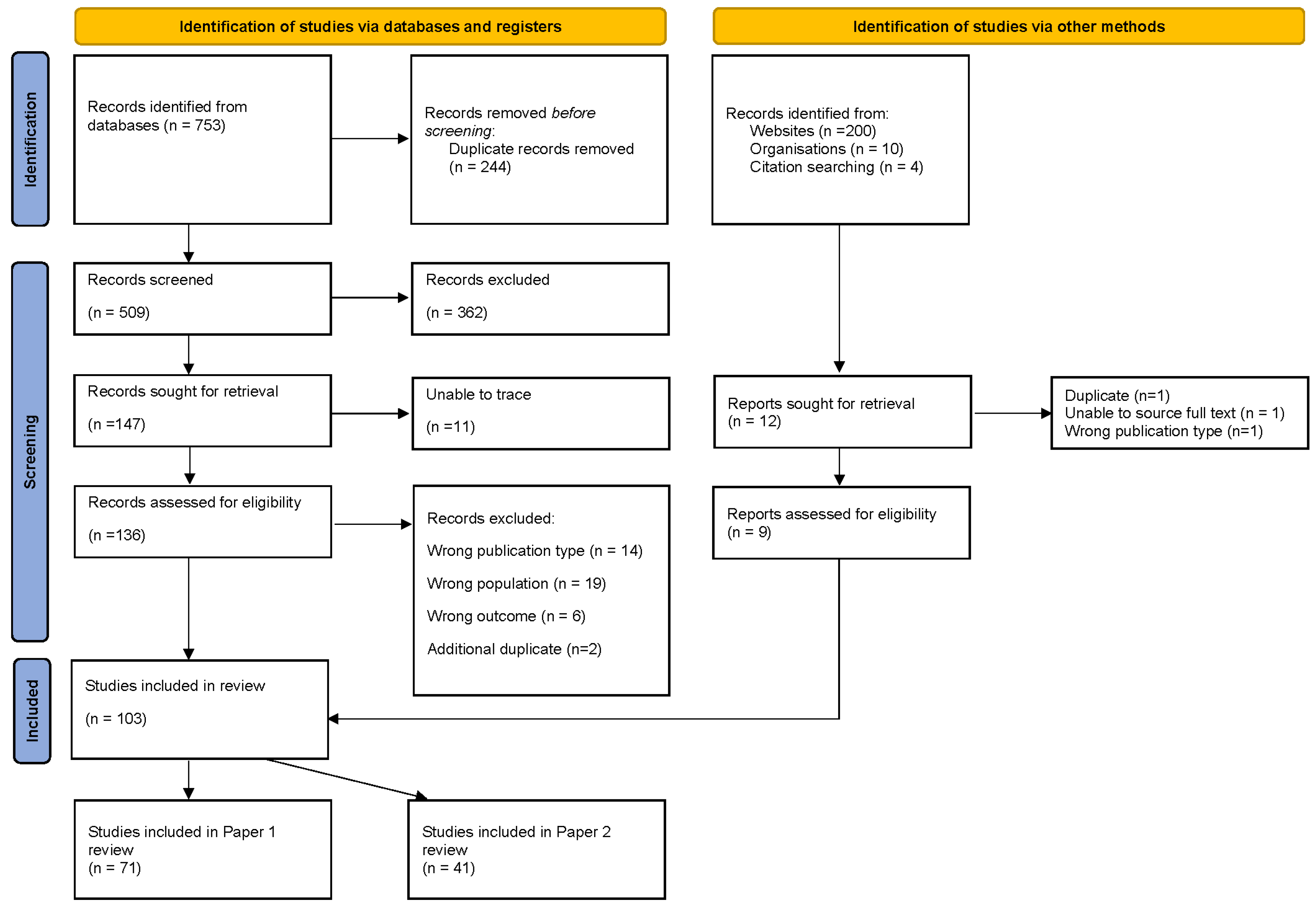
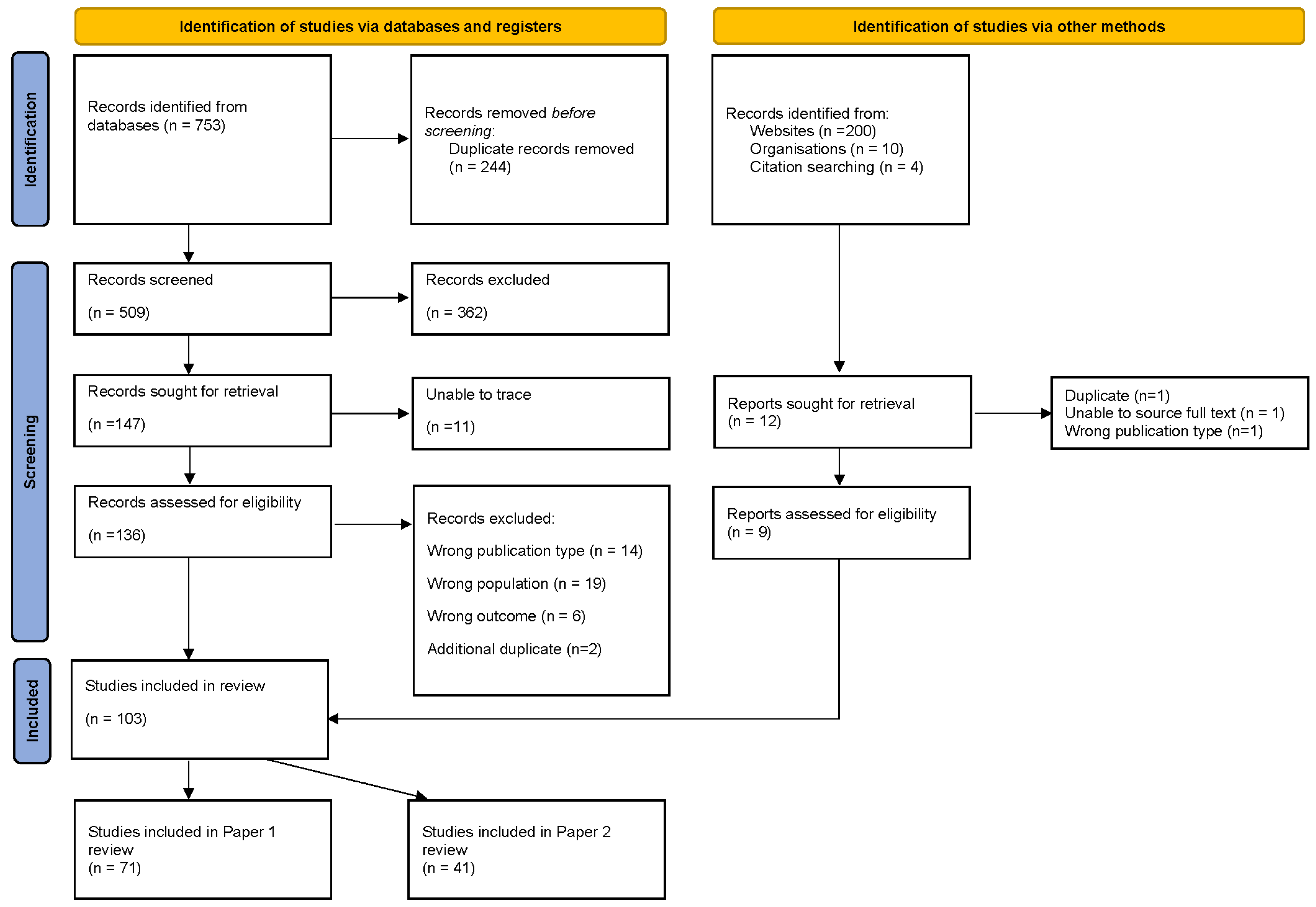
3. Results
3.1. Study Characteristics
3.2. RQ1: What Is the Dental Access of Children and Young People in Care and Care Leavers?
3.3. RQ2: What Factors Influence Care-Experienced Children and Young People’s Access to Dental Care?
3.4. Organisational Factors Affecting Access to Dental Care
3.4.1. Carers and Health/Social Care Professionals Lack of Knowledge of the Process for Obtaining Access to Dental Care for the Children and Young People in Their Care
3.4.2. Insufficient Sharing of CYP’s Oral Health Information between Foster Carers, Health and Social Care Professionals
3.4.3. CYP in Care and Care Leavers’ Changes in Location and Duration of Placement
3.4.4. Social Worker and Health Professionals’ Role in Facilitating Access to Dental Care
3.5. Psycho/Social Factors
3.5.1. Type of Placement
3.5.2. Dental Neglect
3.5.3. Barriers to Foster Carers Facilitating Access to Dental Care
3.5.4. CYP’s Negative Attitude toward Dental Care
3.5.5. CYP’s Anxiety about Visiting the Dentist
3.6. Logistical and Financial Factors
3.6.1. Geographical Location
3.6.2. Distance to Travel
3.6.3. Cost and Availability of Medical Insurance
3.7. Factors Affecting CYP in Care and Care Leavers’ Dental Experience
3.7.1. The Additional Needs of CYP in Care and Care Leavers
3.7.2. Meeting the Additional Needs of CYP in Care and Care Leavers
3.8. RQ 3: What Pathways Have Been Developed to Improve Access to Oral Health Care for Children and Young People in Care and Care Leavers?
3.9. Referral Processes and Interagency Working
3.10. Providing a Designated Pathway to Dental Care
4. Discussion
4.1. Statement of Principal Findings
4.2. Comparison with Existing Literature
4.3. Implications for Policy and Practice
4.4. Unanswered Questions and Future Research
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| 1 | (child* or youth* or adolescen* or teen* or young people).tw. |
| 2 | care leaver*.tw. |
| 3 | leaving care.tw. |
| 4 | (transit* adj3 (care or services)).tw. |
| 5 | Child* in care.tw. |
| 6 | looked after child*.tw. |
| 7 | accommodated child.tw. |
| 8 | (“out of home care” or “out of home placement”).tw. |
| 9 | kinship care.tw. |
| 10 | ((adoption or adopted) adj3 child*).tw. |
| 11 | adopted child/ |
| 12 | (custod* adj3 care).tw. |
| 13 | Orphan*tw. |
| 14 | (placement adj3 care).tw. |
| 15 | public care.tw. |
| 16 | (foster adj1 (care* or home* or family or parent*)).tw. |
| 17 | (institutional* adj3 (care or home*)).tw. |
| 18 | (group adj1 home*).tw. |
| 19 | (residential adj3 (care or home* or facilit*)).tw. |
| 20 | (welfare adj3 (care or system*)).tw. |
| 21 | statutory care.tw. |
| 22 | (care ajd3 local authority).tw. |
| 23 | care order*tw. |
| 24 | (substitute adj1 (care or famil*)).tw. |
| 25 | special guardian*.tw. |
| 26 | Kafalah.tw. |
| 27 | (unaccompanied adj3 asylum).tw. |
| 28 | (unaccompanied adj3 refugee*).tw. |
| 29 | (“Children Act 1989” or “Children Northern Ireland Order 1995” or “Children Scotland Act 1995”).tw. |
| 30 | or/5–29 |
| 31 | dental health/ |
| 32 | dental procedure/ |
| 33 | exp tooth disease/ |
| 34 | exp dentist/ |
| 35 | (oral adj3 (health* or hygiene or care)).ab,kw,ti. |
| 36 | dental.ab,kw,ti. |
| 37 | ((tooth adj3 (health* or hygiene or care or brush* or floss*)) or toothbrush*).ab,kw,ti. |
| 38 | (teeth adj3 (health* or hygiene or care or brush* or floss*)).ab,kw,ti. |
| 39 | dentist*.ab,kw,ti. |
| 40 | or/31–39 |
| 41 | (1 or 2 or 3) and 30 and 40 |
References
- World Health Organization. Global Oral Health Status Report: Towards Universal Health Coverage for Oral Health by 2030; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Kassebaum, N.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global burden of untreated caries: A systematic review and metaregression. J. Dent. Res. 2015, 94, 650–658. [Google Scholar] [CrossRef]
- Williams, A.; Mackintosh, J.; Bateman, B.; Holland, S.; Rushworth, A.; Brooks, A.; Geddes, J. The development of a designated dental pathway for looked after children. Br. Dent. J. 2014, 216, E6. [Google Scholar] [CrossRef] [PubMed]
- Moeller-Saxone, M.; McCutcheon, L.; Halperin, S.; Herrman, H.; Chanen, A. Meeting the primary care needs of young people in residential care. Aust. Fam. Physcian 2016, 45, 706–711. [Google Scholar]
- Randsalu, L.S.; Laurell, L. Children in out-of-home care are at high risk of somatic, dental and mental ill health. Acta Paediatr. Int. J. Paediatr. 2018, 107, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Negro, K.S.; Scott, J.M.; Marcenko, M.; Chi, D.L. Assessing the Feasibility of Oral Health Interventions Delivered by Social Workers to Children and Families in the Foster Care System. Pediatr. Dent. 2019, 41, 48–51. [Google Scholar] [PubMed]
- Acharya, R.; George, A.; Ng Chok, H.; Maneze, D.; Blythe, S. Exploring the experiences of foster and kinship carers in Australia regarding the oral healthcare of children living in out-of-home care. Adopt. Foster. 2022, 46, 466–476. [Google Scholar] [CrossRef]
- Child Welfare Information Gateway. Health-Care Coverage for Children and Youth in Foster Care—And After; U.S. Department of Health and Human Services, Administration for Children and Families: Washington, DC, USA, 2022. [Google Scholar]
- Kelly, Á. Factors Associated with the Ability of the Care System to Meet the Physical and Mental Health Needs of Young People Looked after in England: A Mixed-Methods Study. Ph.D. Thesis, University of Oxford, Oxford, UK, 2022. [Google Scholar]
- Mensah, T.; Hjern, A.; Håkanson, K.; Johansson, P.; Jonsson, A.K.; Mattsson, T.; Tranaeus, S.; Vinnerljung, B.; Östlund, P.; Klingberg, G. Organisational models of health services for children and adolescents in out-of-home care: Health technology assessment. Acta Paediatrica. Int. J. Paediatr. 2020, 109, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Rauter, M.; Jayakar, A.; Clemens, T. Findings from comprehensive health screening of children in out-of-home care: The health of 4-6year olds in Southern Tasmania compared to peers. Intern. Med. J. 2014, 44, 18. [Google Scholar]
- Oliván-Gonzalvo, G.; de la Parte-Serna, A.C. Prevalence of untreated dental caries in Latin American children in the Spanish child protection system. Iberoam. J. Med. 2020, 2, 261–267. [Google Scholar] [CrossRef]
- Thetakala, R.K.; Sunitha, S.; Chandrashekar, B.R.; Sharma, P.; Krupa, N.C.; Srilatha, Y. Periodontal and Dentition Status among Orphans and Children with Parents in Mysore City, India: A Comparative Study. J. Clin. Diagn. Res. JCDR 2017, 11, ZC115–ZC118. [Google Scholar] [CrossRef]
- Xu, J.; Zhu, Y.; Wang, C.; Wang, C. The Dental Health of Orphan and Non-orphan Children in Fuyang City, China. Oral Health Prev. Dent. 2021, 19, 523–528. [Google Scholar]
- Rubin, P.F.; Winocur, E.; Erez, A.; Birenboim-Wilensky, R.; Peretz, B. Dental Treatment Needs among Children and Adolescents Residing in an Ugandan Orphanage. J. Clin. Pediatr. Dent. 2016, 40, 486–489. [Google Scholar] [CrossRef] [PubMed]
- Sarri, G.; Evans, P.; Stansfeld, S.; Marcenes, W. A school-based epidemiological study of dental neglect among adolescents in a deprived area of the UK. Br. Dent. J. 2012, 213, E17. [Google Scholar] [CrossRef] [PubMed]
- Carrellas, A.; Day, A.; Cadet, T. Oral Health Care Needs of Young Adults Transitioning from Foster Care. Health Soc. Work. 2018, 43, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Local Government Association. Healthy Futures: Supporting and Promoting the Health Needs of Looked after Children 2016; Local Government Association: London, UK, 2016. [Google Scholar]
- Seehra, J.; Fleming, P.S.; Newton, T.; DiBiase, A.T. Bullying in orthodontic patients and its relationship to malocclusion, self-esteem and oral health-related quality of life. J. Orthod. 2011, 38, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Department of Health and Human Services. Oral Health in America: A Report of the Surgeon General; U.S. Department of Health and Human Services, National Institute of Dental and Craniofacial Research, National Institutes of Health: Rockville, MD, USA, 2000. [Google Scholar]
- Rebelo, M.A.B.; Rebelo Vieira, J.M.; Pereira, J.V.; Quadros, L.N.; Vettore, M.V. Does oral health influence school performance and school attendance? A systematic review and meta-analysis. Int. J. Paediatr. Dent. 2019, 29, 138–148. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.; Keat, R. Does dental appearance impact on employability in adults? A scoping review of quantitative and qualitative evidence. Br. Dent. J. 2020. [Google Scholar] [CrossRef] [PubMed]
- Levesque, J.-F.; Harris, M.F.; Russell, G. Patient-centred access to health care: Conceptualising access at the interface of health systems and populations. Int. J. Equity Health 2013, 12, 18. [Google Scholar] [CrossRef] [PubMed]
- Gulliford, M.; Figueroa-Munoz, J.; Morgan, M.; Hughes, D.; Gibson, B.; Beech, R.; Hudson, M. What does ‘access to health care’ mean? J. Health Serv. Res. Policy 2002, 7, 186–188. [Google Scholar] [CrossRef]
- Public Health England. National Dental Epidemiology Programme for England: Oral Health Survey of Five-Year-Old Children 2017: A Report on the Inequalities Found in Prevalence and Severity of Dental Decay; Public Health England: London, UK, 2018. [Google Scholar]
- Verd, S.; Aguiló, G.; Kraemer, M.; Fernández, M.; Servera, C.; Colom, M.; Palmer, P.; López-Sureda, M.; Juan, M.; Ripoll, J.; et al. Past medical history: A comparison between children at the point of entry into the care system and children at home. J. Child Custody 2018, 15, 228–240. [Google Scholar] [CrossRef]
- Office of the Director of Public Health Plymouth City Council. Plymouth Oral Health Needs Assessment 2019; Health Plymouth City Council: Plymouth, UK, 2019. [Google Scholar]
- Watt, R.G.; Venturelli, R.; Daly, B. Understanding and tackling oral health inequalities in vulnerable adult populations: From the margins to the mainstream. Br. Dent. J. 2019, 227, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Public Health England. Inequalities in Oral Health in England; Public Health England: London, UK, 2021. [Google Scholar]
- Office for Health Improvement and Disparaties (OHID). Child Oral health: Applying All Our Health; Office for Health Improvement and Disparaties (OHID): London, UK, 2022. [Google Scholar]
- Williams, J.; Jackson, S.; Maddocks, A.; Cheung, W.Y.; Love, A.; Hutchings, H. Case–control study of the health of those looked after by local authorities. Arch. Dis. Child. 2001, 85, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.; Hill, M. The Health of Looked after and Accommodated Children and Young People in Scotland; Social Work Inspection Agency: Edinburgh, UK, 2006. [Google Scholar]
- Keene, E.J.; Skelton, R.; Day, P.F.; Munyombwe, T.; Balmer, R.C. The dental health of children subject to a child protection plan. Int. J. Paediatr. Dent. 2015, 25, 428–435. [Google Scholar] [CrossRef] [PubMed]
- McMahon, A.D.; Elliott, L.; Macpherson, L.M.; Sharpe, K.H.; Connelly, G.; Milligan, I.; Wilson, P.; Clark, D.; King, A.; Wood, R.; et al. Inequalities in the dental health needs and access to dental services among looked after children in Scotland: A population data linkage study. Arch. Dis. Child. 2018, 103, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Council on Foster Care Adoption and Kinship Care and Committee on Early Childhood. Health care of youth aging out of foster care. Pediatrics 2012, 130, 1170–1173.
- Khare, V.; Koshy, A.; Rani, P.; Srilatha, S.; Kapse, S.C.; Agrawal, A. Prevalence of dental caries and treatment needs among the orphan children and adolescents of Udaipur district, Rajasthan, India. J. Contemp. Dent. Pract. 2012, 13, 182–187. [Google Scholar]
- Al-Maweri, S.A.; Al-Soneidar, W.A.; Halboub, E.S. Oral lesions and dental status among institutionalized orphans in Yemen: A matched case-control study. Contemp. Clin. Dent. 2014, 5, 81–84. [Google Scholar] [CrossRef]
- Gu, S.; Lin, J.; Wang, M.; Qian, W.; Wu, Y.; Zhu, X.; Wu, Y. Oral health status of 4–17-year-old orphan children and adolescents of Chongqing. Hua Xi Kou Qiang Yi Xue Za Zhi 2014, 32, 378–381. [Google Scholar]
- Goswami, M.; Bhardwaj, S. Assessment of Traumatic Dental Injuries among Institutionalized Orphan Children: A Cross-sectional Study. Jaypees Int. J. Clin. Pediatr. Dent. 2022, 15, 124–127. [Google Scholar]
- Hurry, K.J.; Ridsdale, L.; Davies, J.; Muirhead, V.E. The Dental Health of Looked After Children in the UK and Dental Care Pathways: A Scoping Review. Community Dent. Health 2023, 40, 1–8. [Google Scholar]
- National Institute for Health and Care Excellence (NICE). Public Health Guidelines on Looked–After Children and Young People; 2021. Available online: https://www.nice.org.uk/guidance/ng205/chapter/Recommendations#health-and-wellbeing (accessed on 24 January 2024).
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- World Population Review. Human Development Index (HDI) by Country 2023. 2023. Available online: https://worldpopulationreview.com/country-rankings/hdi-by-country (accessed on 24 January 2024).
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Shanbhog, R.; Godhi, B.S.; Nandlal, B.; Kumar, S.S.; Raju, V.; Rashmi, S. Clinical consequences of untreated dental caries evaluated using PUFA index in orphanage children from India. J. Int. Oral Health 2013, 5, 1–9. [Google Scholar]
- Finlayson, T.L.; Chuang, E.; Baek, J.D.; Seidman, R. Dental Service Utilization Among Children in the Child Welfare System. Matern. Child Health J. 2018, 22, 753–761. [Google Scholar] [CrossRef]
- Khattab, N.M.A.; Abd-Elsabour, M.A.A. Assessment of dental caries among a group of institutionalized orphan children compared to parented school children: Case–control study. BMC Oral Health 2023, 23, 202. [Google Scholar] [CrossRef] [PubMed]
- Espeleta, H.C.; Schelbe, L.; Ruggiero, K.J.; Klika, J.B. Initial Health Outcomes of a Community-Based Collaboration for Children in Foster Care. Health Soc. Work 2023, 49, 25–33. [Google Scholar] [CrossRef] [PubMed]
- McLean, K.; Hiscock, H.; Goldfeld, S. Timeliness and extent of health service use by Victorian (Australian) children within first year after entry to out-of-home care: Retrospective data linkage cohort study. Child. Youth Serv. Rev. 2022, 134. [Google Scholar] [CrossRef]
- Kamran, R.; Farooq, W.; Faisal, M.R.; Jahangir, F. Clinical consequences of untreated dental caries assessed using PUFA index and its covariates in children residing in orphanages of Pakistan. BMC Oral health 2017, 17, 108. [Google Scholar] [CrossRef]
- Teh, C.; Peet, H. Longitudinal health outcomes of looked after children (LAC). Arch. Dis. Child. 2021, 106, A17. [Google Scholar]
- Muirhead, V.; Subramanian, S.K.; Wright, D.; Wong, F.S.L. How do foster carers manage the oral health of children in foster care? A qualitative study. Community Dent. Oral Epidemiol. 2017, 45, 529–537. [Google Scholar] [CrossRef]
- Leck, R.; Parkes, R.; Williams, A.; Collard, M. Community Dentistry: A Service Evaluation Study for ‘Looked After Children’ in England and Wales. Oral Health Prev. Dent. 2019, 17, 303–308. [Google Scholar]
- Breneol, S.; Rose, H.; Brown, M.; Andreou, P.; Bishop, A.; Mitchell, C. Exploring the health care utilization of children and youth in the care of child welfare: A retrospective matched cohort study. Fam. Pract. 2022, 39, 360–366. [Google Scholar] [CrossRef]
- American Academy of Pediatric Dentistry. Periodicity of examination, preventive dental services, anticipatory guidance/counseling, and oral treatment for infants, children, and adolescents. Ref. Man. Pediatr. Dent. 2022, 40, 253–265. [Google Scholar]
- Melbye, M.L.; Chi, D.L.; Milgrom, P.; Huebner, C.E.; Grembowski, D. Washington state foster care: Dental utilization and expenditures. J. Public Health Dent. 2014, 74, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Berlin, M.; Mensah, T.; Lundgren, F.; Klingberg, G.; Hjern, A.; Vinnerljung, B.; Cederlund, A. Dental healthcare utilisation among young adults who were in societal out-of-home care as children: A Swedish National Cohort Study. Int. J. Soc. Welf. 2018, 27, 325–336. [Google Scholar] [CrossRef]
- Chikkala, J.; Chandrabhatla, S.K.; Vanga, N.R. Variation in levels of anxiety to dental treatment among nonorphan and orphan children living under different systems. J. Nat. Sci. Biol. Med. 2015, 6, S13–S16. [Google Scholar] [CrossRef] [PubMed]
- Baron, A.M.; Baron, Y.M.; Spencer, N.J. The care and health needs of children in residential care in the Maltese Islands. Child Care Health Dev. 2001, 27, 251–262. [Google Scholar] [CrossRef] [PubMed]
- Szilagyi, M.A.; Rosen, D.S.; Rubin, D.; Zlotnik, S. Health care issues for children and adolescents in foster care and kinship care. Pediatrics 2015, 136, e1131–e1140. [Google Scholar] [CrossRef] [PubMed]
- Carabez, R. Health and education passport and the role of the foster care public health nurse. Public Health Nurs. 2022, 39, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.R.; Cosgrove, J.A. The role of care coordination and out-of-home placement in youth dental and vision care visits. Int. J. Soc. Welf. 2018, 27, 388–396. [Google Scholar] [CrossRef]
- Baidwan, S.K. Initial health assessments for unaccompanied asylum-seeking children: Advice and good practice. Paediatr. Child Health 2022, 33, 11–16. [Google Scholar] [CrossRef]
- Rosenbach, M. Children in Foster Care: Challenges of Meeting Their Health Care Needs through Medicaid; Mathematica Policy Research, Inc.: Princeton, NJ, USA, 2001. [Google Scholar]
- Melbye, M.; Huebner, C.E.; Chi, D.L.; Hinderberger, H.; Milgrom, P. A first look: Determinants of dental care for children in foster care. Spec. Care Dent. 2013, 33, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Carabez, R.; Kim, J.E. Part I: The role of public health nursing in addressing health care needs of children in foster care. Public Health Nurs. 2019, 36, 702–708. [Google Scholar] [CrossRef]
- Hunter, D.; McCartney, G.; Fleming, S.; Guy, F. Improving the health of looked after children in Scotland: 1. Using a specialist nursing service to improve the health care of children in residential accommodation. Adopt. Foster. 2008, 32, 51–56. [Google Scholar] [CrossRef]
- Dubowitz, H.; Feigelman, S.; Zuravin, S.; Tepper, V.; Davidson, N.; Lichenstein, R. The physical health of children in kinship care. Am. J. Dis. Child. 1992, 146, 603–610. [Google Scholar] [CrossRef]
- American Academy of Pediatric Dentistry. Guideline on adolescent oral healthcare. Pediatr. Dent. 2005, 27, 72–79.
- Department of Health and Department for Education. Promoting the Health and Well-Being of Looked-After Children Statutory Guidance for Local Authorities, Clinical Commissioning Groups and NHS England; Department of Health and Department for Education: London, UK, 2015. [Google Scholar]
- NICE. Child Abuse and Neglect; NICE: London, UK, 2017. [Google Scholar]
- Dahlander, A.; Soares, F.; Grindefjord, M.; Dahllöf, G. Factors Associated with Dental Fear and Anxiety in Children Aged 7 to 9 Years. Dent. J. 2019, 7, 68. [Google Scholar] [CrossRef]
- Arora, N.; Kaltner, M.; Williams, J. Health needs of regional Australian children in out-of-home care. J. Paediatr. Child Health 2014, 50, 782–786. [Google Scholar] [CrossRef]
- McLean, K.; Hiscock, H.; Scott, D.; Goldfeld, S. Foster and kinship carer survey: Accessing health services for children in out-of-home care. J. Paediatr. Child Health 2021, 57, 132–139. [Google Scholar] [CrossRef]
- Landers, G.; Snyder, A.; Zhou, M. Comparing preventive visits of children in foster care with other children in Medicaid. J. Health Care Poor Underserved 2013, 24, 802–812. [Google Scholar] [CrossRef]
- Bright, M.A.; Alford, S.M.; Hinojosa, M.S.; Knapp, C.; Fernandez-Baca, D.E. Adverse childhood experiences and dental health in children and adolescents. Community Dent. Oral Epidemiol. 2015, 43, 193–199. [Google Scholar] [CrossRef]
- Alyce, S.; Taggart, D.; Montaque, I. Avoiding psychological (re)traumatisation in dentistry when working with patients who are adult survivors of child sex abuse. Br. Dent. J. 2022, 233, 666–670. [Google Scholar] [CrossRef]
- Vinnerljung, B.; Kling, S.; Hjern, A. Health problems and healthcare needs among youth in Swedish secure residential care. Int. J. Soc. Welf. 2018, 27, 348–357. [Google Scholar] [CrossRef]
- Chambers, M.F.; Saunders, A.M.; New, B.D.; Williams, C.L.; Stachurska, A. Assessment of children coming into care: Processes, pitfalls and partnerships. Clin. Child Psychol. Psychiatry 2010, 15, 511–527. [Google Scholar] [CrossRef]
- Raman, S.; Reynolds, S.; Khan, R. Addressing the well-being of Aboriginal children in out-of-home care: Are we there yet? J. Paediatr. Child Health 2011, 47, 806–811. [Google Scholar] [CrossRef]
- Thompson, V. How State Medicaid Programs Serve Children and Youth in Foster Care; National Academy for State Health Policy: Portland, ME, USA, 2021. [Google Scholar]
- Sinclair, E.; Verykaki, E.; Kerr, K.; John, J. Dental Public Health in Action: Oral Health Advice for Looked-After-Children: A pilot care pathway in Buckinghamshire, UK. Community Dent. Health 2023, 40, 199–205. [Google Scholar]
- Taylor, D.J.; Albers, B.; Mann, G.; Chakraborty, S.; Lewis, J.; Mendes, P.; Macdonald, G.; Williams, K.; Shlonsky, A.R. Systematic Review and Meta-Analysis of Policies, Programmes and Interventions That Improve Outcomes for Young People Leaving the Out-of Home Care System; Centre for Evidence and Implementation: Carlton, VA, USA, 2021; p. 177. [Google Scholar]
- Vinnerljung, B.; Hjern, A. Health and health care for children in out-of-home care. Int. J. Soc. Welf. 2018, 27, 321–324. [Google Scholar] [CrossRef]
- Jones, R.; Everson-Hock, E.S.; Guillaume, L. The effectiveness of interventions aimed at improving access to health and mental health services for looked-after children and young people: A systematic review. Fam. Relatsh. Soc. 2012, 1, 71–85. [Google Scholar] [CrossRef]
- Marcus, K.; Balasubramanian, M.; Short, S.; Sohn, W. Barriers and facilitators to dental care among culturally and linguistically diverse carers: A mixed-methods systematic review. Community Dent. Oral Epidemiol. 2023, 51, 327–344. [Google Scholar] [CrossRef] [PubMed]
- Khalid, G.; Metzner, F.; Pawils, S. Prevalence of dental neglect and associated risk factors in children and adolescents-A systematic review. Int. J. Paediatr. Dent. 2022, 32, 436–446. [Google Scholar] [CrossRef] [PubMed]
- Shanthi, M.; Goud, E.; Kumar, G.; Rajguru, J.; Ratnasothy, S.; Ealla, K. Risk Factors and Treatment Needs among Orphan School Children. J. Contemp. Dent. Pract. 2017, 18, 893–898. [Google Scholar] [CrossRef]
- Deutsch, S.A.; Fortin, K. Physical Health Problems and Barriers to Optimal Health Care Among Children in Foster Care. Curr. Probl. Pediatr. Adolesc. Health Care 2015, 45, 286–291. [Google Scholar] [CrossRef]
- Webster, S.M. Children and young people in out-of-home care: Canaries in the coal mine of healthcare commissioning. Aust. J. Prim. Health 2016, 22, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Greiner, M.V.; Beal, S.J.; Dexheimer, J.W.; Divekar, P.; Patel, V.; Hall, E.S. Improving Information Sharing for Youth in Foster Care. Pediatrics 2019, 144, e20190580. [Google Scholar] [CrossRef] [PubMed]
- Mekonnen, R.; Noonan, K.; Rubin, D. Achieving better health care outcomes for children in foster care. Pediatr. Clin. N. Am. 2009, 56, 405–415. [Google Scholar] [CrossRef]
- Alcalá, H.E.; Valdez-Dadia, A.; von Ehrenstein, O.S. Adverse childhood experiences and access and utilization of health care. J Public Health 2018, 40, 684–692. [Google Scholar] [CrossRef]
- Raja, S.; Hoersch, M.; Rajagopalan, C.F.; Chang, P. Treating patients with traumatic life experiences: Providing trauma-informed care. J. Am. Dent. Assoc. 2014, 145, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Kling, S.; Vinnerljung, B.; Hjern, A. Somatic assessments of 120 Swedish children taken into care reveal large unmet health and dental care needs. Acta Paediatr. Int. J. Paediatr. 2016, 105, 416–420. [Google Scholar] [CrossRef]
- Battersby, A.; French, J.; Brennan, K.; Eisen, S.; Ward, A.; Fitzgerald, F.; Williams, B.; Nijman, R. Evaluation of the health needs of unaccompanied asylum seeking children. Arch. Dis. Child. 2019, 104, A116. [Google Scholar]
- Ridsdale, L.; Johnston, L.; James, N.; Balmer, R. Looked after children: An overview for the dental team. Br. Dent. J. 2023, 234, 34–38. [Google Scholar] [CrossRef]
- Smales, M.; Savaglio, M.; Webster, S.; Skouteris, H.; Pizzirani, B.; O’Donnell, R.; Green, R. Are the voices of young people living in out-of-home care represented in research examining their health?: A systematic review of the literature. Child. Youth Serv. Rev. 2020, 113, 104966. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Erwin, J.; Horrell, J.; Wheat, H.; Axford, N.; Burns, L.; Booth, J.; Witton, R.; Shawe, J.; Doughty, J.; Kaddour, S.; et al. Access to Dental Care for Children and Young People in Care and Care Leavers: A Global Scoping Review. Dent. J. 2024, 12, 37. https://doi.org/10.3390/dj12020037
Erwin J, Horrell J, Wheat H, Axford N, Burns L, Booth J, Witton R, Shawe J, Doughty J, Kaddour S, et al. Access to Dental Care for Children and Young People in Care and Care Leavers: A Global Scoping Review. Dentistry Journal. 2024; 12(2):37. https://doi.org/10.3390/dj12020037
Chicago/Turabian StyleErwin, Jo, Jane Horrell, Hannah Wheat, Nick Axford, Lorna Burns, Joelle Booth, Robert Witton, Jill Shawe, Janine Doughty, Sarah Kaddour, and et al. 2024. "Access to Dental Care for Children and Young People in Care and Care Leavers: A Global Scoping Review" Dentistry Journal 12, no. 2: 37. https://doi.org/10.3390/dj12020037
APA StyleErwin, J., Horrell, J., Wheat, H., Axford, N., Burns, L., Booth, J., Witton, R., Shawe, J., Doughty, J., Kaddour, S., Boswell, S., Devalia, U., Nelder, A., & Paisi, M. (2024). Access to Dental Care for Children and Young People in Care and Care Leavers: A Global Scoping Review. Dentistry Journal, 12(2), 37. https://doi.org/10.3390/dj12020037