
Appointments Needed for Complete Denture for Frail Older Adults Residing in Long-Term Care Facilities: A Cross-Sectional Study


Abstract

1. Introduction
2. Materials and Methods
3. Results
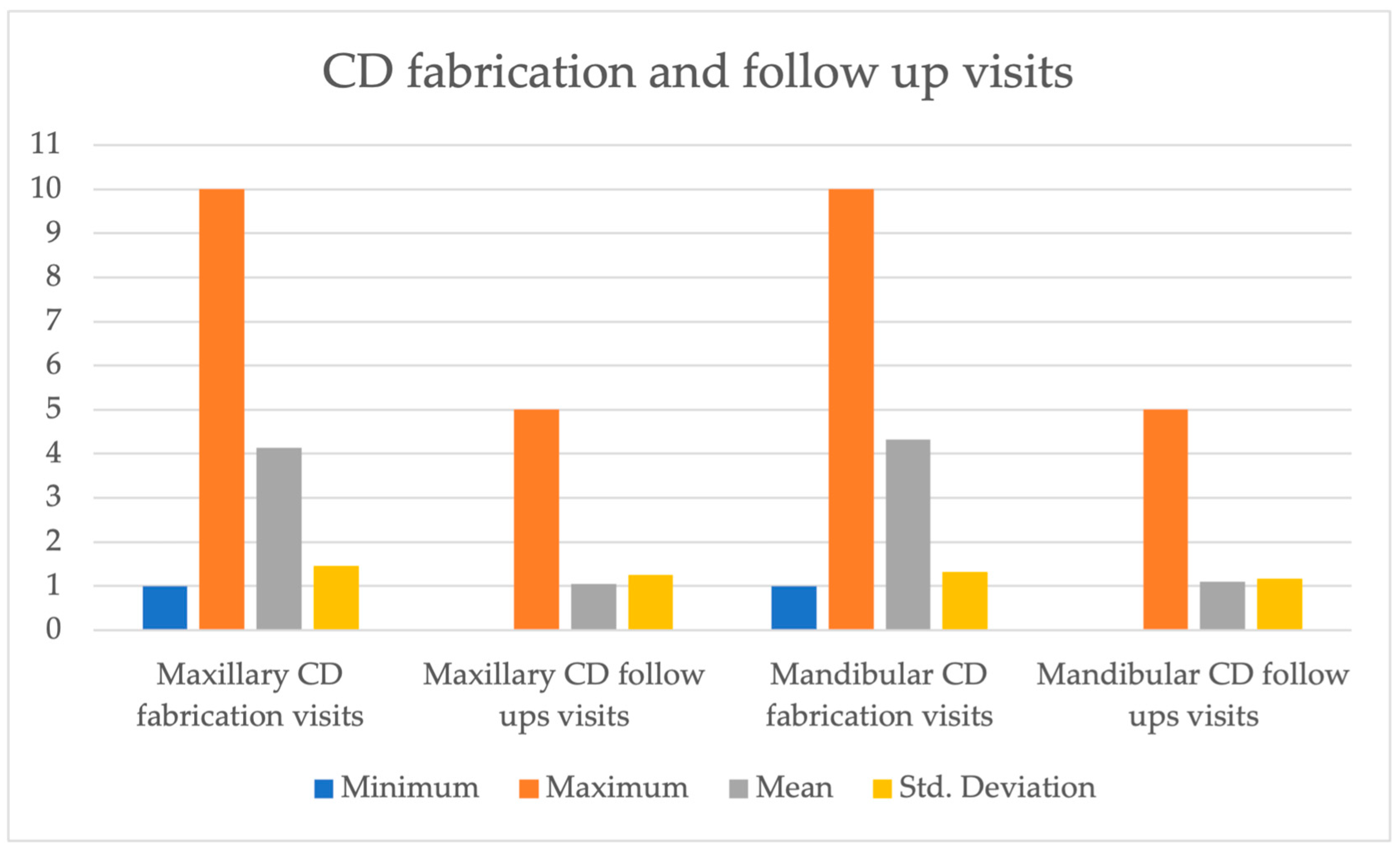
3.1. Number of Appointments Required for Complete Denture Fabrication
3.2. Number of Appointments Required for Post-Insertion Follow-Up
4. Discussion
4.1. Number of Appointments Required for Complete Denture Fabrication
4.2. Number of Appointments Required for Post-Insertion Follow-Up
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Statistics Canada. Census in Brief: A Portrait of the Population Aged 85 and Older in 2016 in Canada. Updated 2018. Available online: https://www12.statcan.gc.ca/census-recensement/2016/as-sa/98-200-x/2016004/98-200-x2016004-eng.cfm (accessed on 4 December 2018).
- Statistics Canada. June 2010, Catalogue No. 91-520-X, Population Projections for Canada, Provinces and Territories 2009 to 2036; Statistics Canada: Ottawa, ON, Canada, 2010; ISBN 0-660-19525-9. Available online: https://www150.statcan.gc.ca/n1/pub/91-520-x/91-520-x2010001-eng.pdf#shr-pg-pnl1 (accessed on 2 July 2019).
- Zhang, W.; Wu, Y.Y.; Wu, B. Does oral health predict functional status in late life? Findings from a national sample. J. Aging Healthy 2017, 30, 924–944. [Google Scholar] [CrossRef]
- Maupomé, G.; Wyatt, C.C.L.; Williams, P.M.; Aickin, M.; Gullion, C.M. Oral disorders in institution-dwelling elderly adults: A graphic representation. Spec. Care Dent. 2002, 22, 194–200. [Google Scholar] [CrossRef]
- Friedman, P.K.; Kaufman, L.B.; Karpas, S.L. Oral health disparity in older adults: Dental decay and tooth loss. Dent. Clin. N. Am. 2014, 58, 757. [Google Scholar] [CrossRef]
- Ardenghi, D.M.; Wyatt, C. Exploring the views of relatives of frail elderly patients about participating in a geriatric dentistry program. Spec. Care Dent. 2017, 37, 140–146. [Google Scholar] [CrossRef]
- British Columbia Ministry of Health. Residential Care Staffing Review; British Columbia Ministry of Health: Victoria, BC, Canada, 2017. Available online: https://www.health.gov.bc.ca/library/publications/year/2017/residential-care-staffing-review.pdf (accessed on 2 July 2019).
- Ettinger, R.L.; Beck, J.D. Geriatric dental curriculum and the needs of the elderly. Spec. Care Dent. 1984, 4, 207–213. [Google Scholar] [CrossRef]
- Thomson, W.M.; Ma, S. An ageing population poses dental challenges. Singap. Dent. J. 2014, 35, 3–8. [Google Scholar] [CrossRef]
- Statistics Canada. Catalogue No. 82-625-X, Health Fact Sheets Oral Health: Edentulous People in Canada 2007 to 2009 January 2010; Statistics Canada: Ottawa, ON, Canada, 2010. Available online: https://www150.statcan.gc.ca/n1/pub/82-625-x/2010001/article/11087-eng.pdf (accessed on 2 July 2019).
- Ling, B.C. A practical three visit complete denture system. Ann. R. Australas. Coll. Dent. Surg. 2000, 15, 66. [Google Scholar]
- Mahmood, Z.; Iqbal, Z. Post insertion visits for removable complete dentures made with and without face bow record. Biomedica 2016, 32, 13. [Google Scholar]
- Cinotti, W.R.; Grieder, A.; Biber, C.L. The geriatric patient: One-visit quality complete denture construction technique. Part 2. J. N. J. Dent. Assoc. 1989, 60, 43. [Google Scholar]
- Kulkarni, R.S.; Pawar, R.S. Fabrication of complete dentures in three visits using existing prosthesis—A simplified technique for geriatric patients. Spec. Care Dent. 2017, 37, 99–101. [Google Scholar] [CrossRef]
- Cinotti, W.R.; Grieder, A.; Biber, C.L. The geriatric patient: One- or two-visit complete denture construction technique. Part 1. J. N. J. Dent. Assoc. 1989, 60, 31. [Google Scholar]
- Murthy, S.S.; Prabhu, M.B.; Hegde, M.; Murthy, G.S. Complete Denture Fabrication for Old Denture Wearer in One Day. World 2012, 3, 112–114. [Google Scholar] [CrossRef]
- Villias, A.; Karkazis, H.; Yannikakis, S.; Artopoulou, I.I.; Polyzois, G. Is the Number of Appointments for Complete Denture Fabrication Reduced with CAD-CAM? A Literature Review. Prosthesis 2022, 4, 91–101. [Google Scholar] [CrossRef]
- Ettinger, R. Treatment planning concepts for the ageing patient. Aust. Dent. J. 2015, 60 (Suppl. 1), 71–85. [Google Scholar] [CrossRef]
- MacEntee, M.I.; Wyatt, C.C. An Index of Clinical Oral Disorder in Elders (CODE). Gerodontology 1999, 16, 85–96. [Google Scholar] [CrossRef]
- Palinkas, M.; Nassar, M.S.P.; Cecílio, F.A.; Siéssere, S.; Semprini, M.; Machado-de-Sousa, J.P.; Regalo, S.C.H. Age and gender influence on maximal bite force and masticatory muscles thickness. Arch. Oral Biol. 2010, 55, 797–802. [Google Scholar] [CrossRef]
- Alves, C.P.; Munhoz, M.F.V.; Oliveira Nascimento, G.M.; Nícoli, G.A.; Paleari, A.G.; Camargos, G.D.V. The influence of age, gender, mandibular bone height, previous experience with prostheses, and fabrication methods on masticatory performance of complete denture wearers: Masticatory performance and complete dentures. J. Prosthodont. 2019, 28, e34–e40. [Google Scholar] [CrossRef]
- Gandage Dhananjay, S.; Kini Ashwini, Y.; Gangadhar, S.A.; Lagdive, S.B.; Pai, U.Y. Two-step impression for atrophic mandibular ridge. Gerodontology 2012, 29, e1195–e1197. [Google Scholar] [CrossRef]
- Bernson, J.M.; Elfström, M.L.; Hakeberg, M. Dental coping strategies, general anxiety, and depression among adult patients with dental anxiety but with different dental-attendance patterns. Eur. J. Oral Sci. 2013, 121, 270–276. [Google Scholar] [CrossRef]
- de Lima, D.C.; Nakata, G.C.; Balducci, I.; Almeida, J.D. Oral manifestations of diabetes mellitus in complete denture wearers. J. Prosthet. Dent. 2008, 99, 60–65. [Google Scholar] [CrossRef]
- Evren, B.A.; Uludamar, A.; Işeri, U.; Ozkan, Y.K. The association between socioeconomic status, oral hygiene practice, denture stomatitis and oral status in elderly people living different residential homes. Arch. Gerontol. Geriatr. 2008, 53, 252–257. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Mandibular CD Fabrication Visits | |||||
|---|---|---|---|---|---|
| <5 Visits | 5 visits | >5 Visits | Total | Chi-Squared Tests of Independence | |
| Gender | Fisher’s Exact Test | ||||
| Female | 62 (66.7%) | 34 (51.5%) | 9 (42.9%) | 105 (58.3%) | 0.048 |
| Male | 31 (33.3%) | 32 (48.5%) | 12 (57.1%) | 75 (41.7%) | |
| Total | 93 (100%) | 66 (100%) | 21 (100%) | 180 (100%) | |
| Mucosal conditions | Fisher’s Exact Test | ||||
| Good | 74 (79.6%) | 49 (74.2%) | 8 (40.0%) | 131 (73.2%) | 0.006 |
| Moderate | 11 (11.8%) | 12 (18.2%) | 6 (30.0%) | 29 (16.2%) | |
| Severe | 8 (8.6%) | 5 (7.6%) | 6 (30.0%) | 19 (10.6%) | |
| Total | 93 (100%) | 66 (100%) | 20 (100%) | 179 (100%) | |
| Single vs. complete set | Fisher’s Exact Test | ||||
| Single denture | 61 (64.9%) | 24 (36.4%) | 7 (33.3%) | 92 (50.8%) | 0.000 |
| Complete set | 33 (35.1%) | 42 (63.6%) | 14 (66.7%) | 89 (49.2%) | |
| Total | 94 (100%) | 66 (100%) | 21 (100%) | 181 (100%) | |
| Maxillary CD Fabrication Visits | |||||
|---|---|---|---|---|---|
| <5 Visits | 5 Visits | >5 Visits | Total | Chi-Squared Tests of Independence | |
| Behavioral Group | Fisher’s Exact Test | ||||
| No | 69 (71.1%) | 47 (69.1%) | 6 (37.5%) | 122 (67.4%) | 0.033 |
| Yes | 28 (28.9%) | 21 (30.9%) | 10 (62.5%) | 59 (32.6%) | |
| Total | 97 (100%) | 68 (100%) | 16 (100%) | 181 (100%) | |
| Endocrine Group | Fisher’s Exact Test | ||||
| No | 61 (62.9%) | 47 (69.1%) | 15 (93.8%) | 123 (68.0%) | 0.039 |
| Yes | 36 (37.1%) | 21 (30.9%) | 1 (6.3%) | 58 (32.0%) | |
| Total | 97 (100%) | 68 (100%) | 16 (100%) | 181 (100%) | |
| Mucosal conditions | Fisher’s Exact Test | ||||
| Good | 83 (86.5%) | 52 (77.6%) | 6 (37.5%) | 141 (78.8%) | 0.001 |
| Moderate | 5 (5.2%) | 9 (13.4%) | 5 (31.3%) | 19 (10.6%) | |
| Severe | 8 (8.3%) | 6 (9.0%) | 5 (31.3%) | 19 (10.6%) | |
| Total | 96 (100%) | 67 (100%) | 16 (100%) | 179 (100%) | |
| Single vs. complete set | Fisher’s Exact Test | ||||
| Single denture | 64 (66.0%) | 24 (35.3%) | 4 (25.0%) | 92 (50.8%) | 0.000 |
| Complete set | 33 (34.0%) | 44 (64.7%) | 12 (75.0%) | 89 (49.2%) | |
| Total | 97 (100%) | 68 (100%) | 16 (100%) | 181 (100%) | |
| Maxillary CD Post-Insertion Follow Ups | |||||
|---|---|---|---|---|---|
| No Post-Insertion Follow-Up | 1–3 Post-Insertion Follow-Ups | 4–5 Post-Insertion Follow-Ups | Total | Chi-Squared Tests of Independence | |
| OH Group | Fisher’s Exact Test | ||||
| Yes | 43 (58.90%) | 41 (49.39%) | 3 (23.07%) | 87 (51.48%) | 0.027 |
| No | 12 (16.44%) | 26 (31.33%) | 7 (53.85%) | 45 (26.63%) | |
| With assistance | 18 (24.66%) | 16 (19.28%) | 3 (23.08%) | 37 (21.89%) | |
| Total | 73 (100%) | 83 (100%) | 13 (100%) | 169 (100%) | |
| Endocrine Group | Fisher’s Exact Test | ||||
| No | 45 (56.25%) | 66 (75%) | 12 (92.31%) | 123 (67.96%) | 0.005 |
| Yes | 35 (43.75%) | 22 (25%) | 1 (7.69%) | 58 (32.04%) | |
| Total | 80 (100%) | 88 (100%) | 13 (100%) | 181 (100%) | |
| Mobility | Fisher’s Exact Test | ||||
| Ambulatory | 39 (49.37%) | 34 (39.53%) | 0 (0.0%) | 73 (41.01%) | 0.004 |
| Wheelchair-bound | 37 (46.84%) | 45 (52.33%) | 12 (92.31%) | 94 (52.81%) | |
| Bedridden | 3 (3.79%) | 7 (8.14%) | 1 (7.69%) | 11 (6.18%) | |
| Total | 79 (100%) | 86 (100%) | 13 (100%) | 178 (100%) | |
| Single vs. complete set | Fisher’s Exact Test | ||||
| Single denture | 52 (65%) | 36 (40.91%) | 4 (30.77%) | 92 (50.83%) | 0.002 |
| Complete set | 28 (35%) | 52 (59.09%) | 9 (69.23%) | 89 (49.17%) | |
| Total | 80 (100%) | 88 (100%) | 13 (100%) | 181 (100%) | |
| Mandibular CD Post-Insertion Follow-Ups | |||||
|---|---|---|---|---|---|
| No Post-Insertion Follow-Up | 1–3 Post-Insertion Follow-Ups | 4–5 Post-Insertion Follow-Ups | Total | Chi-Squared Tests of Independence | |
| OH Group | Fisher’s Exact Test | ||||
| Yes | 38 (58.46%) | 55 (57.29%) | 1 (10%) | 94 (54.97%) | 0.010 |
| No | 13 (20%) | 27 (28.13%) | 7 (70%) | 47 (27.49%) | |
| With assistance | 14 (21.54%) | 14 (14.58%) | 2 (20%) | 30 (17.54%) | |
| Total | 65 (100%) | 96 (100%) | 10 (100%) | 171 (100%) | |
| Mobility | Fisher’s Exact Test | ||||
| Ambulatory | 35 (51.47%) | 40 (40.40%) | 0 (0.0%) | 75 (42.37%) | 0.014 |
| Wheelchair-bound | 30 (44.12%) | 50 (50.51%) | 9 (90%) | 89 (50.28%) | |
| Bedridden | 3 (4.41%) | 9 (9.09%) | 1 (10%) | 13 (7.35%) | |
| Total | 68 (100%) | 99 (100%) | 10 (100%) | 177 (100%) | |
| Single vs. complete set | Fisher’s Exact Test | ||||
| Single denture | 40 (58.82%) | 51 (49.51%) | 1 (10%) | 92 (50.83%) | 0.012 |
| Complete set | 28 (41.18%) | 52 (50.49%) | 9 (90%) | 89 (49.17%) | |
| Total | 68 (100%) | 103 (100%) | 10 (100%) | 181 (100%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Altuwaijri, S.H.; Champirat, T.; Wyatt, C. Appointments Needed for Complete Denture for Frail Older Adults Residing in Long-Term Care Facilities: A Cross-Sectional Study. Dent. J. 2024, 12, 36. https://doi.org/10.3390/dj12020036
Altuwaijri SH, Champirat T, Wyatt C. Appointments Needed for Complete Denture for Frail Older Adults Residing in Long-Term Care Facilities: A Cross-Sectional Study. Dentistry Journal. 2024; 12(2):36. https://doi.org/10.3390/dj12020036
Chicago/Turabian StyleAltuwaijri, Sahr H., Tharee Champirat, and Chris Wyatt. 2024. "Appointments Needed for Complete Denture for Frail Older Adults Residing in Long-Term Care Facilities: A Cross-Sectional Study" Dentistry Journal 12, no. 2: 36. https://doi.org/10.3390/dj12020036
APA StyleAltuwaijri, S. H., Champirat, T., & Wyatt, C. (2024). Appointments Needed for Complete Denture for Frail Older Adults Residing in Long-Term Care Facilities: A Cross-Sectional Study. Dentistry Journal, 12(2), 36. https://doi.org/10.3390/dj12020036