1. Introduction
Dental treatment should be conducted so morphological and functional harmony is attained, promoting good short- and long-term prognosis. In this context, occlusion and a maxillomandibular relationship, e.g., with regard to occlusal contacts and the interocclusal distance, during mastication, speech, mandibular rest position, and others, are important aspects to assess during the diagnostic phase and considered while delivering dental interventions.
The closest speaking space is the minimum space found between teeth while the patient is speaking, with its name and definition being linked to Pound [
1,
2] and Silverman [
3]. Its assessment is most frequently performed using speaking tests consisting of the patient saying the letter “S” or words containing it. Based on the current knowledge, the closest speaking space exhibits less variability than the freeway space [
4] and is reproducible to about 1 to 2 mm [
5] but with variations in the amount depending on the patient’s particularities, such as occlusion and skeletal features [
2], and dental status, such as tooth wear [
6]. The closest speaking space has clinical value, considering that oral rehabilitations, such as prosthetic ones, should be made with preservation of the closest speaking space in order to achieve an optimal functional outcome. Among its clinical applications, the closest speaking space is used to establish the vertical dimension of occlusion in edentulous patients [
7,
8] or establish the increase in the vertical dimension of occlusion, such as in patients with severe tooth wear [
9]. In this regard, in edentulous patients, phonetic tests are used differently but often in conjunction to establish the functional vertical dimension of occlusion, i.e., tests with the letter “M” are used for determining it from the rest position, and tests with the letter “S” are used to assess its accuracy. In a study on this theme by Yamagata et al. [
10], it was suggested that speech adaptation with an impact on the freeway space and the closest speaking space occurs due to different oral conditions, this being an aspect that needs to be further researched. Information is needed to establish the best parameters of these phonetic tests that provide the most accurate results.
Even if information on the closest speaking space is used nowadays in clinical practice, current evidence on it is scarce. Studies are performed using either clinical methods, which assess the interocclusal distance using interocclusal records [
11] or the movement of the mandible during a phonetic test [
10,
12], or using instrumental methods, with the usage of the kineograph [
13]. Digital analysis in dentistry in general, compared to physical analysis, frequently has the advantage of offering the possibility of an in-depth and more precise way of assessing the phenomenon. To the best of our knowledge, there are no reported studies using digital analysis of the closest speaking space in particular, nor other interocclusal spaces, the freeway space included, in general. The methods proposed in this research are new and have forward ways of improvement, but digital analysis of this aspect seems to be appropriate due to providing more precise and broader information on the closest speaking space, a theme that is important from a clinical point of view but supported by little scientific evidence.
The main study aim is to present some of the identified methods of digital analysis of the closest speaking space in dentate persons, exemplified by a case report. The secondary aim is to assess the particularities of the closest speaking space in dentate persons, following digital analysis of a case series.
2. Materials and Methods
This research received approval from The Scientific Research Ethics Commission of “Carol Davila” University of Medicine and Pharmacy, Bucharest (PO-35-F-03, No. 8366/2024). Study inclusion was confirmed after participants were informed about the research and signed an informed consent form to certify their agreement of participation.
Participants. This study was conducted on a convenience sample of adult participants with natural permanent dentition, all with occupations related to the dental field (dental students or dental technicians, with previous knowledge on dental procedures, phonetic tests included). Exclusion criteria included the following: impaired mandibular movement related to oral pain, temporomandibular disorders, or other factors; dental prosthetic restorations; coronal restorations with composite resin in the anterior teeth, fixed orthodontic appliances; previous allergic reactions to dental materials; severe speech defects.
Data collection. For all patients, traditional dental impressions using a universal tray and alginate were taken, then poured with Moldano dental gypsum (Kulzer, Hanau, Germany) to obtain maxillary and mandibular dental casts. Interocclusal records of the maximal intercuspal position and closest speaking space were created using polyvinyl siloxane (Occlufast, Zhermack, Badia Polesine, Italy). The same operator conducted this procedure for all patients included. The closest speaking space was recorded using a method based on the speaking test proposed by Silverman [
12]. Participants were seated in an upright position without using a headrest; therefore, the head was unsupported. The impression material was placed on occlusal surfaces of the mandibular teeth. Afterwards, the participants, as previously instructed, pronounced the phonetic sound “S” and tried to maintain the corresponding mandibular position, without closing or moving the mandible, until the hardening of the material was complete.
Afterwards, dental casts were scanned using Swing DOF (DOF, Seoul, Republic of Korea) dental laboratory scanner, firstly in the position corresponding to maximal intercuspal position, and secondly in the position corresponding to closest speaking space.
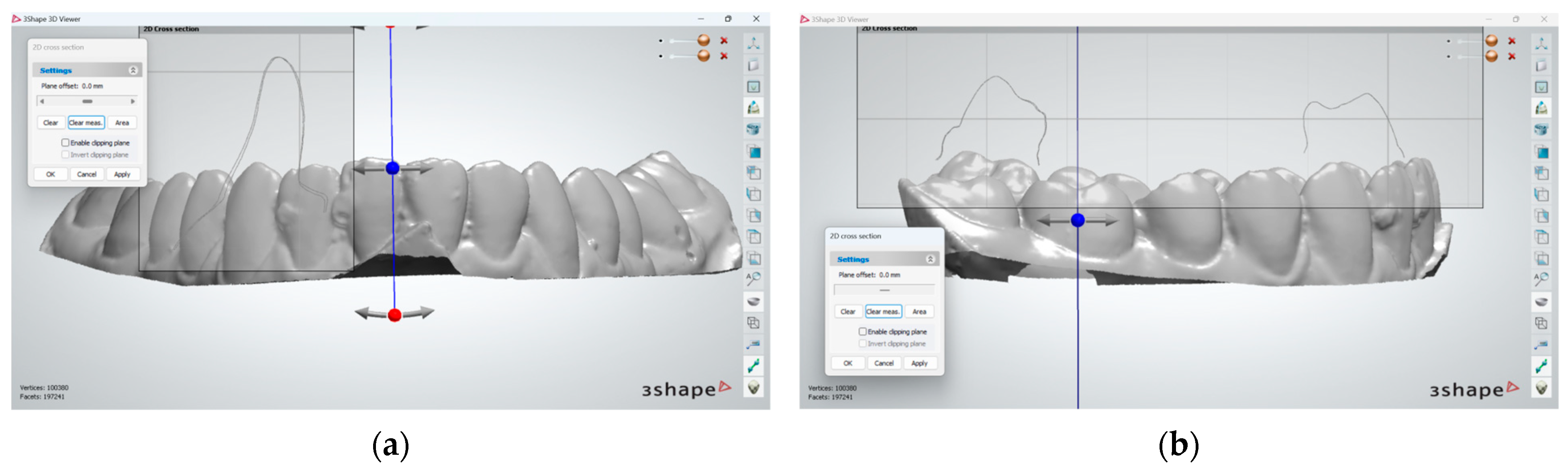
The closest speaking space was digitally analyzed using the 3Shape 3D viewer software version 1.4. (3Shape) and occlusion map tool of 3Shape Ortho Analyzer (3Shape). Digital analysis followed the same two directions that are traditionally seen in clinical assessments of the closest speaking space, firstly by recording the absolute value of the closest speaking space, i.e., the minimum interocclusal distance between maxillary and mandibular teeth [
11,
13], and secondly by recording the amplitude of tooth movement during phonetic testing, representing the range of motion of the mandible for this specific situation, usually conducted by looking at the mandibular central incisors [
12]. The different methods for digital analysis of the closest speaking space are presented below with the aid of a case report, followed by a presentation of the results of our analysis of a case series.
Data analysis. SPSS Statistics version 29 was used for data analysis. Group comparison was conducted using nonparametric test, i.e., Friedman and Wilkoxon test. Statistical significance was set at p < 0.05.
4. Discussion
This study proposes methods for digital analysis of the closest speaking space that can also be applied for other functional spaces, such as freeway space. These methods of digital analysis can be used for both clinical practice and research. With regard to closest speaking space, the main findings of this research (while taking its limitations into account) are related to two aspects, which are important from a clinical point of view. Firstly, it is suggested that when oral rehabilitations are conducted (such as conventional or implant prosthetic rehabilitations), it is important to assess the preservation of the closest speaking space, not only in the central incisors but also in the most distally placed teeth, those being the instances where the closest speaking space registers its lowest values. Secondly, it is suggested that mandibular movement that occurs during phonetic testing should be better researched; our results show that both lateral and forward movement of the mandible occurs, which likely impacts the value of the closest speaking space recorded as the interocclusal distance.
When conducting dental treatments, obtaining a functional outcome is very important for the short- and long-term prognosis [
14,
15,
16]. Existing means for obtaining information on oral functionality still present certain gaps and uncertainties but can be augmented using digital methods of analysis, with the latter promoting a more in-depth assessment compared to traditionally used physical methods. More so, gaining knowledge via digital assessment is increasingly feasible nowadays; its use has considerably changed dentistry in other areas of focus and registers an accelerated increase in use generally.
In this research, we proposed relatively simple methods of assessment of the closest speaking space that could be used for acquiring information, which is important from both a clinical and research point of view.
The first digital method proposed assesses the absolute value of closest speaking space recorded as the interocclusal space, by using impression material, as done in previous research [
11,
13]. The interocclusal distance can be measured more precisely digitally and can be easily achieved at the level of all teeth of the dental arch, ranging from the anterior to the posterior teeth. Nonetheless, difficulties arise in identifying the teeth landmarks required to register the true minimum value. The solution which was identified for this shortcoming is to use digitally generated occlusion maps for the position corresponding to the closest speaking space.
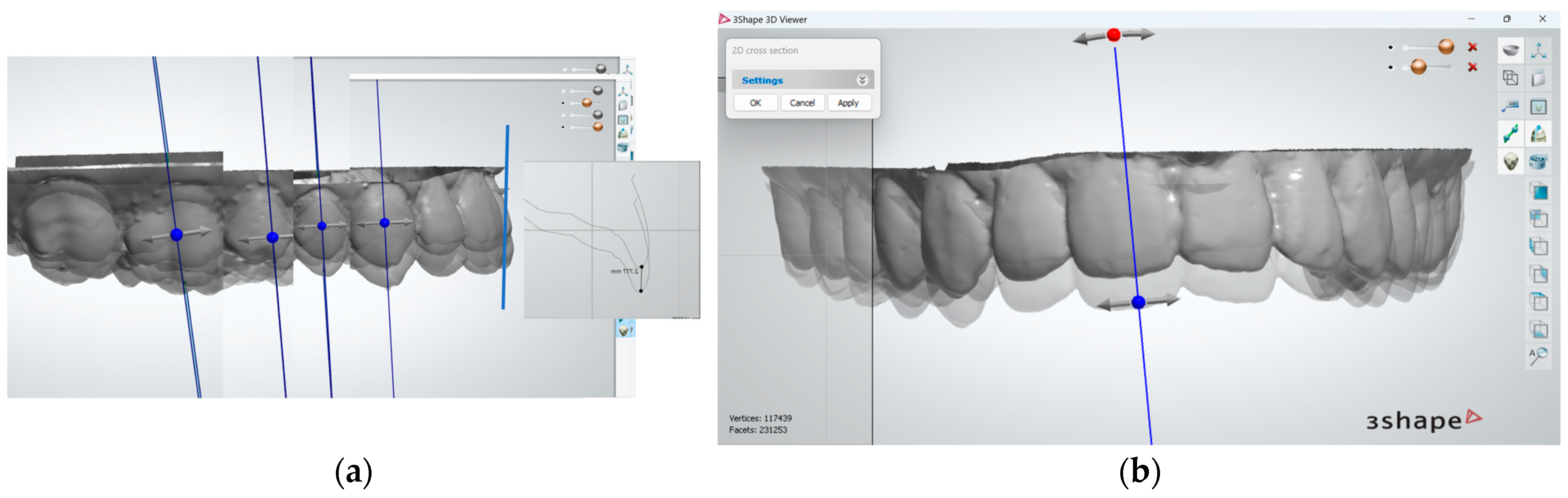
The second digital method proposed was based on the assessment of the tooth movement from the maximal intercuspal position to the position considered as being the one corresponding to the closest speaking space. In order to conduct this analysis, superimposition on one dental arch is required. Digital superimposition is increasingly used in dentistry to gain important clinical information [
17], e.g., when assessing tooth movement during orthodontic treatment [
18], or when assessing the occurrence and magnitude of tooth wear [
19]. When compared to the previously mentioned applications, superimposition in this case is simpler, as no changes to dental arches occurred. Even so, it should be noted that, using this method, the actual closest speaking space (which is minimum interocclusal distance) is not assessed but, rather, the amplitude and direction of tooth movement between two positions during speaking tests. Even so, this component of analysis is important, considering that mandibular movement influences the value of the closest speaking space (the interocclusal distance) and that the pattern of mandibular movement during the speaking tests is related to the patient’s particularities, such as their occlusion and skeletal features [
20,
21].
The analyses, measurements, and superimpositions were conducted on 3D dental casts, the latter being an application previously used in research for different purposes [
22]. Both digital analyses were conducted using 3Shape dental system software (3Shape 3D Viewer and 3Shape Ortho Analyzer) and could probably be conducted using other product variants. There are a range of applications which can be used for studying the range of mandibular movement [
23], 3Shape included [
24], but for the purposes of studying the closest speaking space, the options of recording and measuring the interocclusal distance should be available. In addition, the proposed method has the advantage of being relatively affordable and, therefore, promotes wider use. Several improvements in the proposed method could be tested, such as using an intraoral scanner for registering the position corresponding to the closest speaking space. Although digital analysis of the closest speaking space poses its own requirements and challenges, it seems to be a good alternative to existing physical methods used clinically. Shortcomings of the latter include aspects, such as lower precision of the measurement instruments used, occasional inaccuracy of measurement of interocclusal distance based on interocclusal records due to the consistency of the material used and sometimes due to voids, and difficulties in registering the amplitude of tooth movement for distally placed teeth and others. Such shortcomings can be overcome by using digital analysis, which is overall more precise and allows for a broader range of analysis.
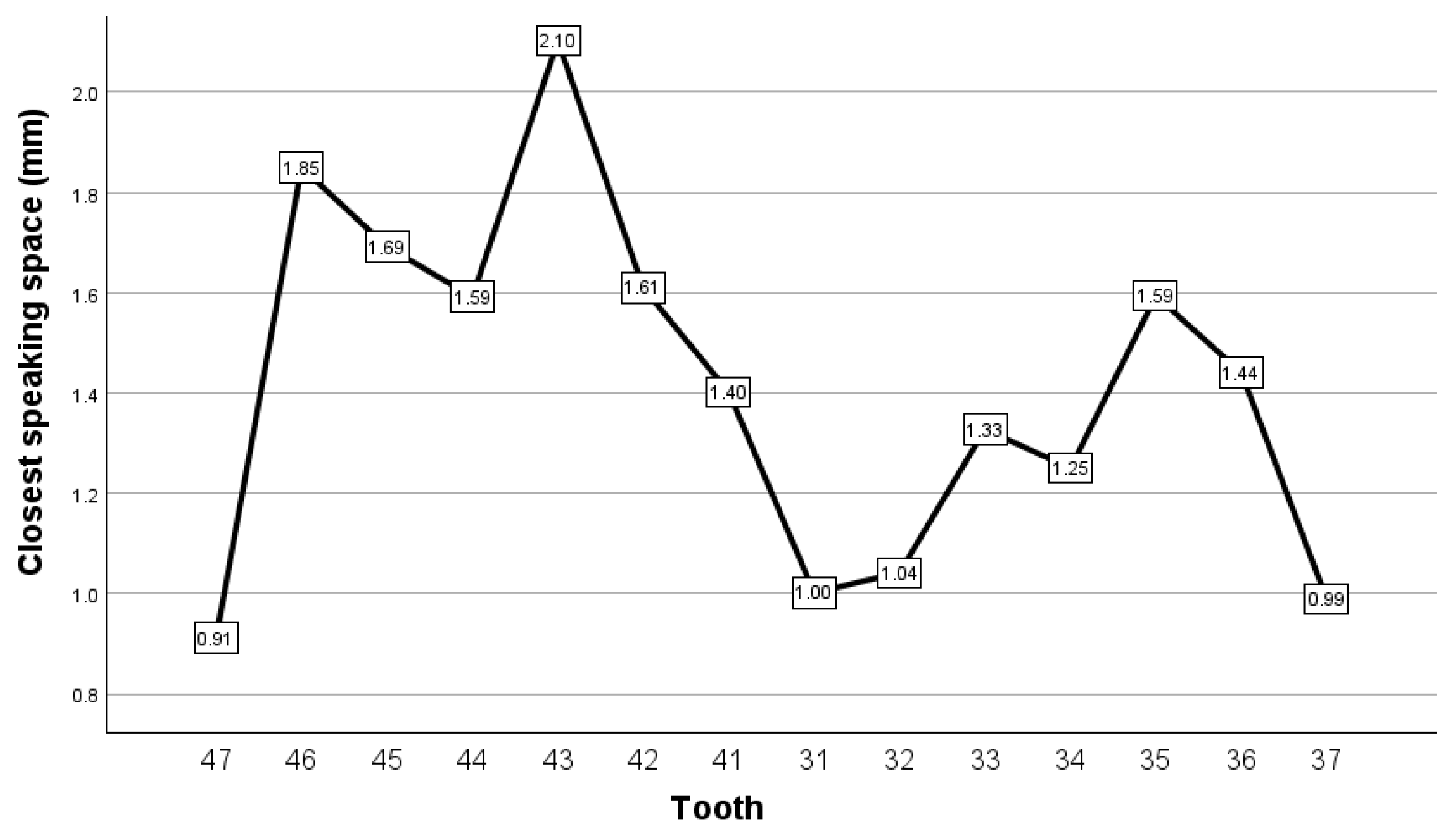
The information on the closest speaking space gathered during our research confirms previous knowledge and raises new questions, which are important for clinical practice. As previous research suggests, values of the closest speaking space at the level of central incisors (where it is usually assessed) pose a certain degree of variability, which, in this research, range from approximately 1 to 4 mm. According to Pound [
2], mentioned also in the Glossary of Prosthodontic terms [
5], the value of the closest speaking space is usually around 1 to 2 mm. In previous research, values outside this range were found, with their variability being linked to patient features [
11,
20]. According to Sakar et al. [
11], the closest speaking space shows larger values in dentate persons with Angle class II division 2 anomalies (mean = 2.66 mm; SD = 1.16 mm) and lower values in Angle class III anomalies (mean = 1.92 mm; SD = 0.95 mm). According to Souza et al. [
20], the value of the closest speaking space is positively correlated with both vertical and horizontal overlap of the incisors. There are other factors (in addition to those already mentioned) that should be considered for having an impact on the closest speaking space, e.g., other dental occlusal particularities (whether static or dynamic), facial skeletal pattern, posture, and parafunctional habits. While the closest speaking space is variable between different individuals, it is constant and reproducible through phonetic tests in the same individual [
25,
26]. Therefore, in those instances in which the closest speaking space is clinically important to be assessed in dentate patients, a relatively simple way to do so is via digital analysis, as it can be conducted (if desired and considered clinically relevant) at the level of different teeth, as well as before or after treatment or in both moments in time, e.g., in the case of conventional or implant prosthetic rehabilitations. Additionally, considering the limited evidence on the topic, information on the reproducibility of phonetic tests acquired through physical analysis should be confirmed by digital analysis, considering the higher degree of precision of measurements involved in the latter.
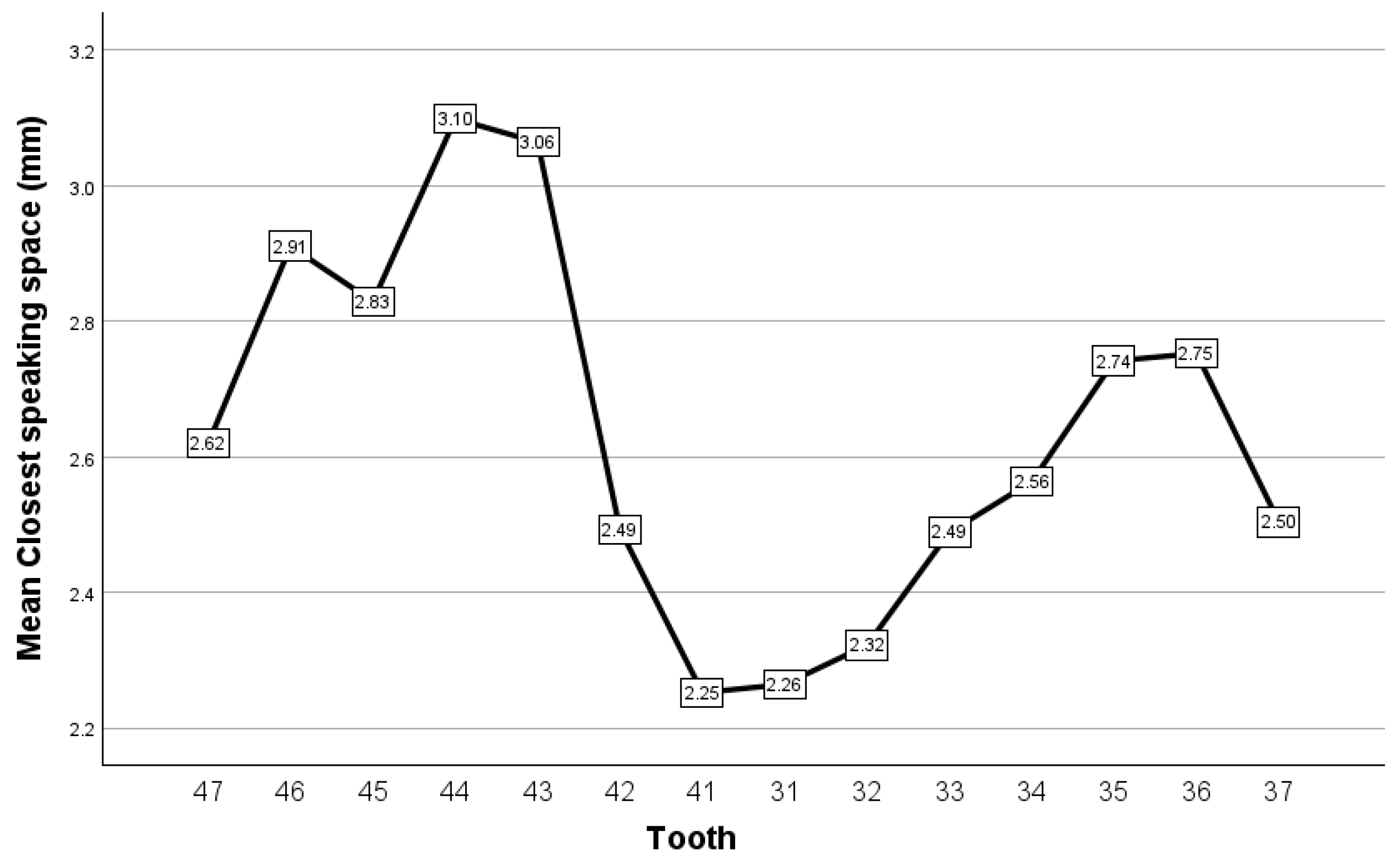
Assessment of the closest speaking space is usually performed at the level of central incisors and recorded as the minimal occlusal distance at this level. By employing digital analysis, it was highlighted (as expected) that the closest speaking space registers different values at the level of different teeth in dentate persons. One important clinical aspect raised by this research, which should be confirmed by other research studies, is that the lower values of the closest speaking space are encountered at the level of both the most anterior and most distally placed teeth, with similar values sometimes being recorded. This information suggests that when prosthetic restorations are made in the most distally placed teeth, the value of the closest speaking space should be assessed at that level; this is especially advisable in patients whose closest speaking space has lower values, as in class III patients [
11].
The values of the observed interocclusal distance (corresponding to closest speaking space) are related to mandibular movement that occurs during the speaking test. Digital analysis conducted during this research reveals that such movement was, as expected, not symmetrical, with a mandibular deviation to the left side occurring most frequently. These findings contradict the study of Zhang et al. [
27], which concluded that almost no deviation of the mandible is observed in the left or right direction during phonetic tests, when measurement is conducted using physical methods, with a vernier caliper. This contradiction is unlikely to be explained by a complete absence of lateral deviation of the mandible, as the odds of achieving a perfectly symmetrical movement are very low. Instead, it is suggested that the most probable explanation lies with the difficulty of assessment and recording of the mandibular movement using physical methods, as physical methods have lower precision. This is particularly important in this case, when considering the very low range of mandibular movement. Previous evidence shows that patients with certain features, such as facial skeletal class, are associated with a different pattern of lateral mandibular movement [
21]. In such instances, the amplitude of the mandibular movements, as observed during phonetic testing, should be further investigated to identify those patients in which it is more frequently encountered. In addition, aspects related to the impact of these mandibular movements on the interocclusal distance of the closest speaking space and the extent to which it is clinically relevant should be assessed. Finally, the results of this research suggest that, during phonetic testing, a forward movement of the mandible occurs. This aspect is in accordance with a study conducted by Zhang et al. [
27], which found that during speech, the mandible was more forward compared to the maximal intercuspal position. Pound [
28] also highlighted the importance of acknowledging the degree of forward movement of the mandible, which impacts the value of closest speaking space, especially in the posterior teeth, depending on occlusion particularities. These ideas are supported by the findings of subsequent research studies [
11,
20]. Therefore, it is suggested that digital analysis of mandibular movement during speech is advisable in individual cases, as information on mandibular movement has been previously shown to contribute to a better functional integration of the prosthetic restorations [
24,
29].
This research has several limitations. Among these, we note that there are other digital applications that could be used and should be tested in terms of suitability as a method for studying the closest speaking space; this research highlights certain main features that should be included in them. As a future direction of improvement, intraoral scanning of the position corresponding to the closest speaking space could be used. Other limitations could be linked to measurement or registration errors, the small number of participants, and registration of the closest speaking space through a speaking test. Future research on larger sample sizes is recommended to confirm the information found on this topic.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}