
Current Molecular, Cellular and Genetic Aspects of Peri-Implantitis Disease: A Narrative Review


Abstract
1. Introduction
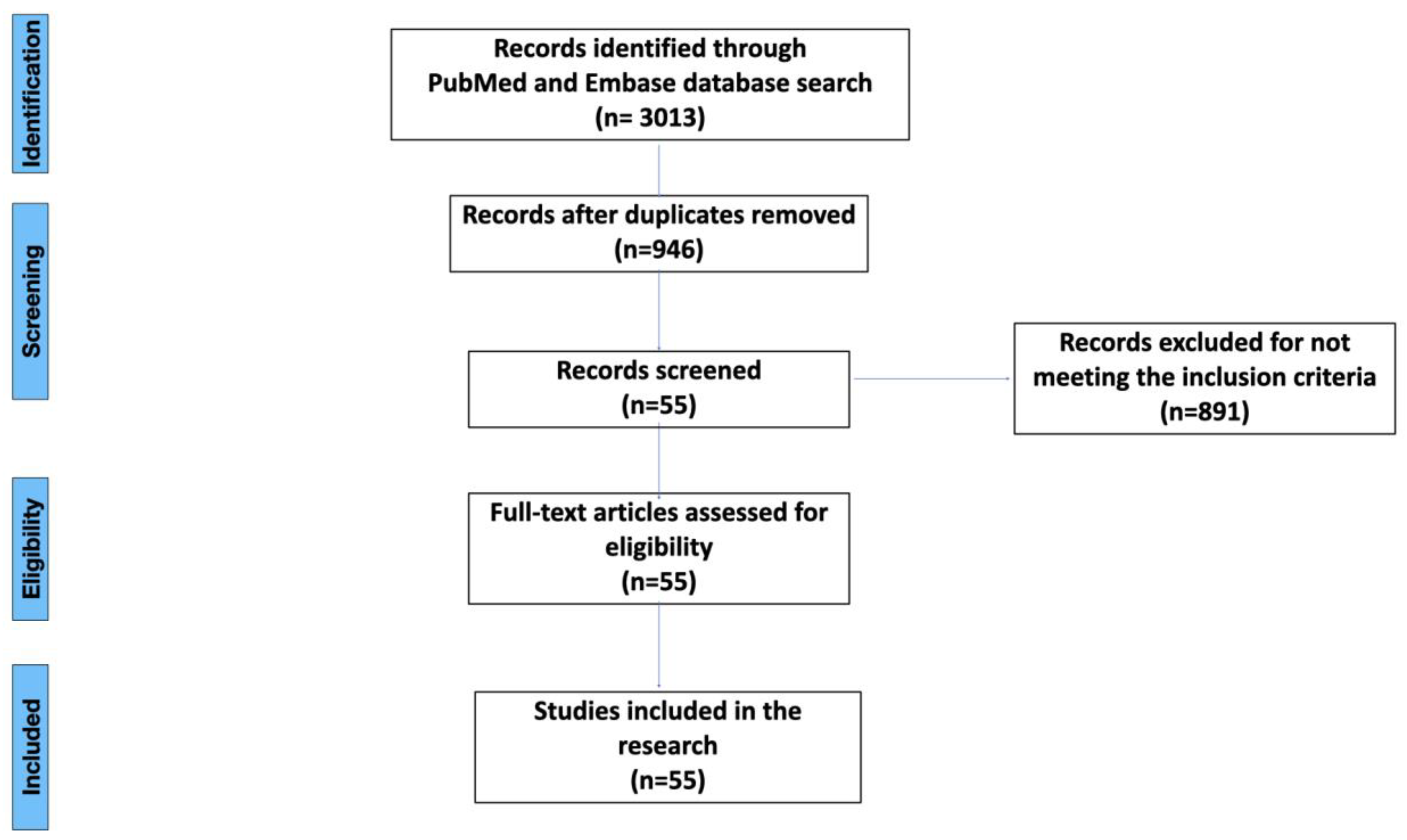
2. Materials and Methods
3. Literature Search Results
3.1. Types of Peri-Implant Disease and Criteria for Implant Health and Peri-Implantitis
3.2. Risk Factors Associated with Peri-Implantitis
3.3. Molecular Factors Contributing to Peri-Implantitis Development
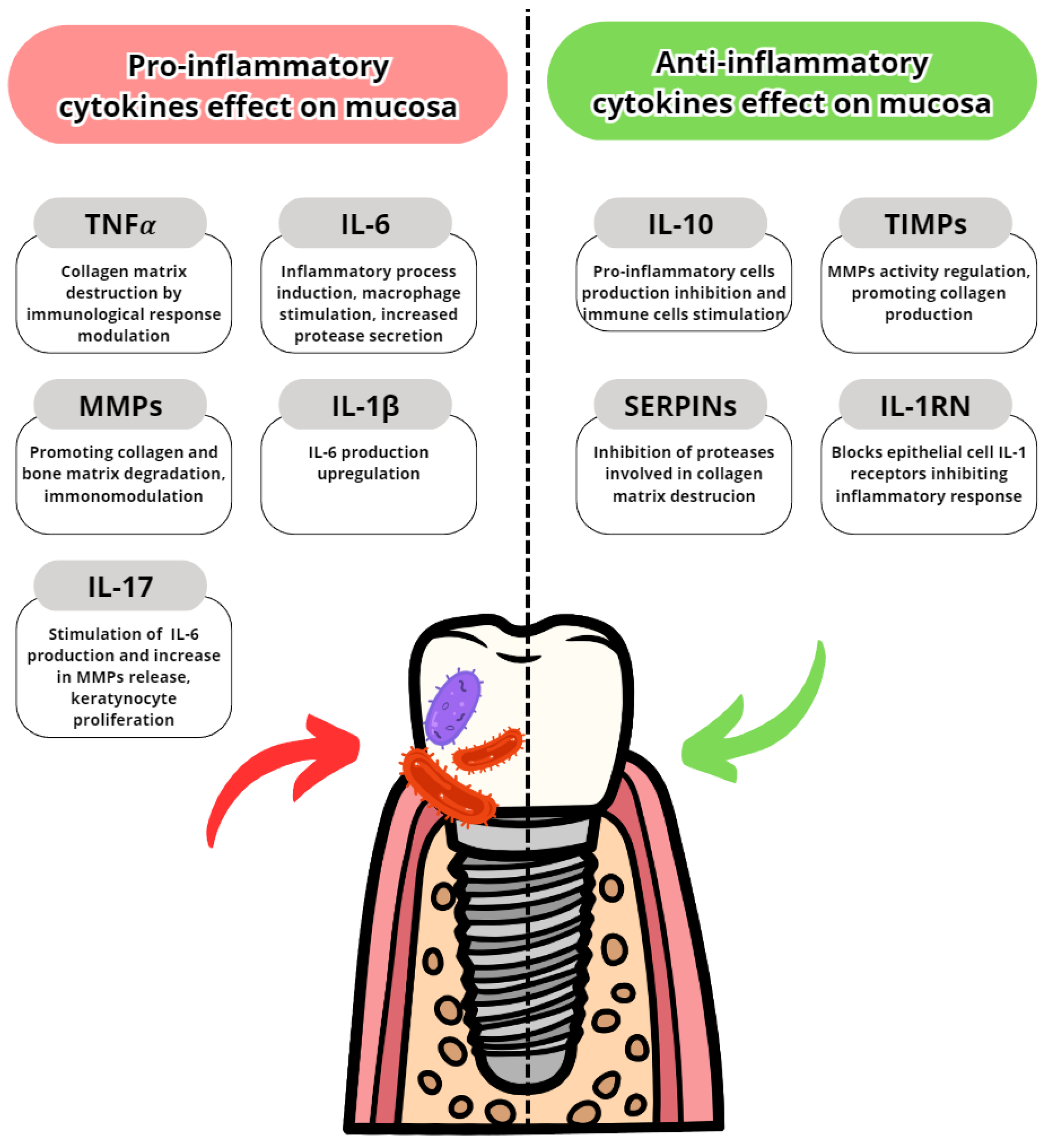
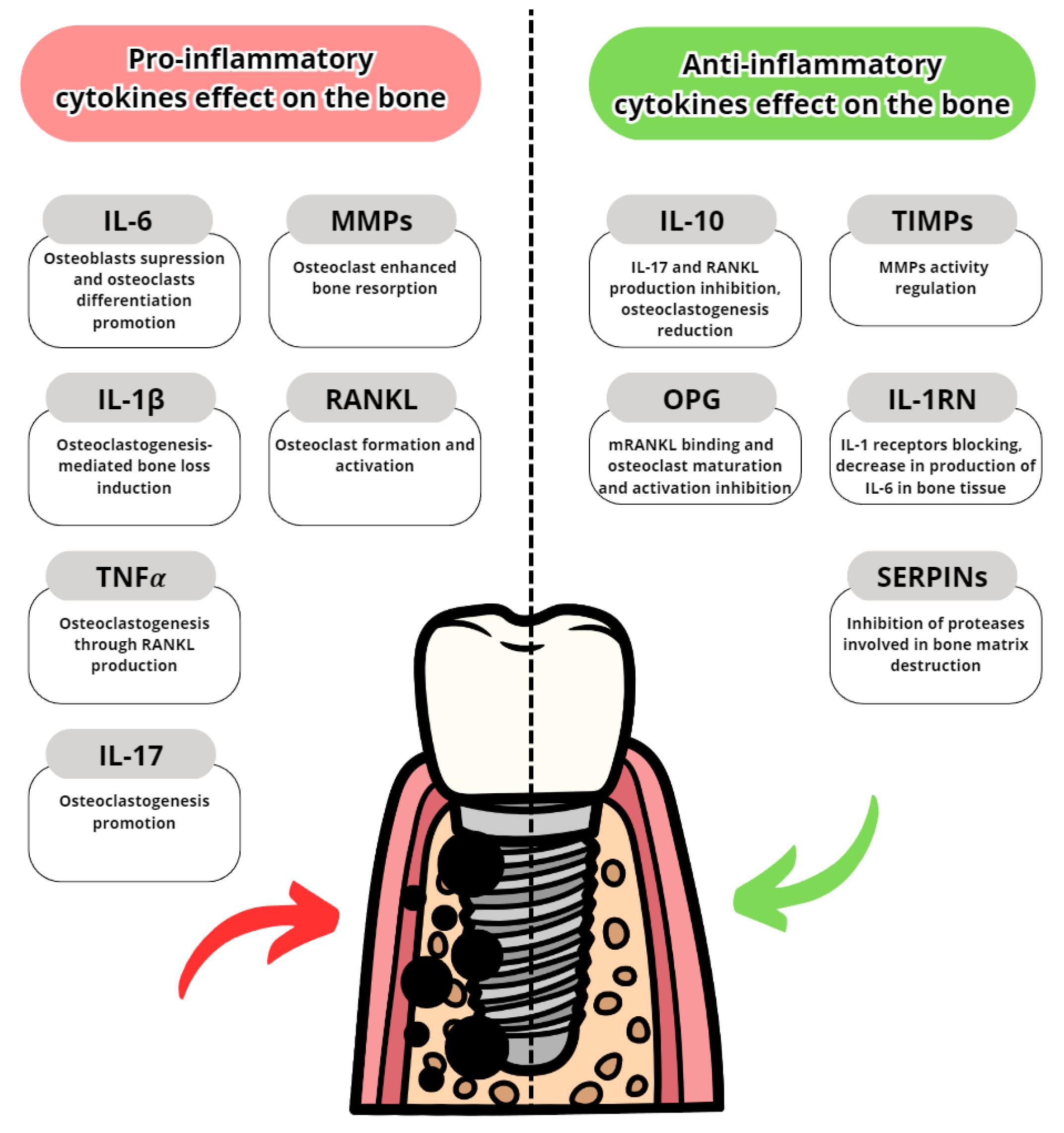
3.3.1. Pro-Inflammatory Cytokines
Interleukin-6 (IL-6)
Interleukin-1β (IL-1β)
Tumor Necrosis Factor α (TNFα)
Interleukin-8 (IL-8)
Interleukin-17 (IL-17)
Collagenase-2 (MMP-8/aMMP-8)
Other Metalloproteinases and Activated Metalloproteinases (MMPs/aMMPs)
3.3.2. Anti-Inflammatory Cytokines
Interleukin-10 (IL-10)
Tissue Metalloproteinase Inhibitors (TIMPs)
RANKL, OPG and RANKL/OPG Ratio
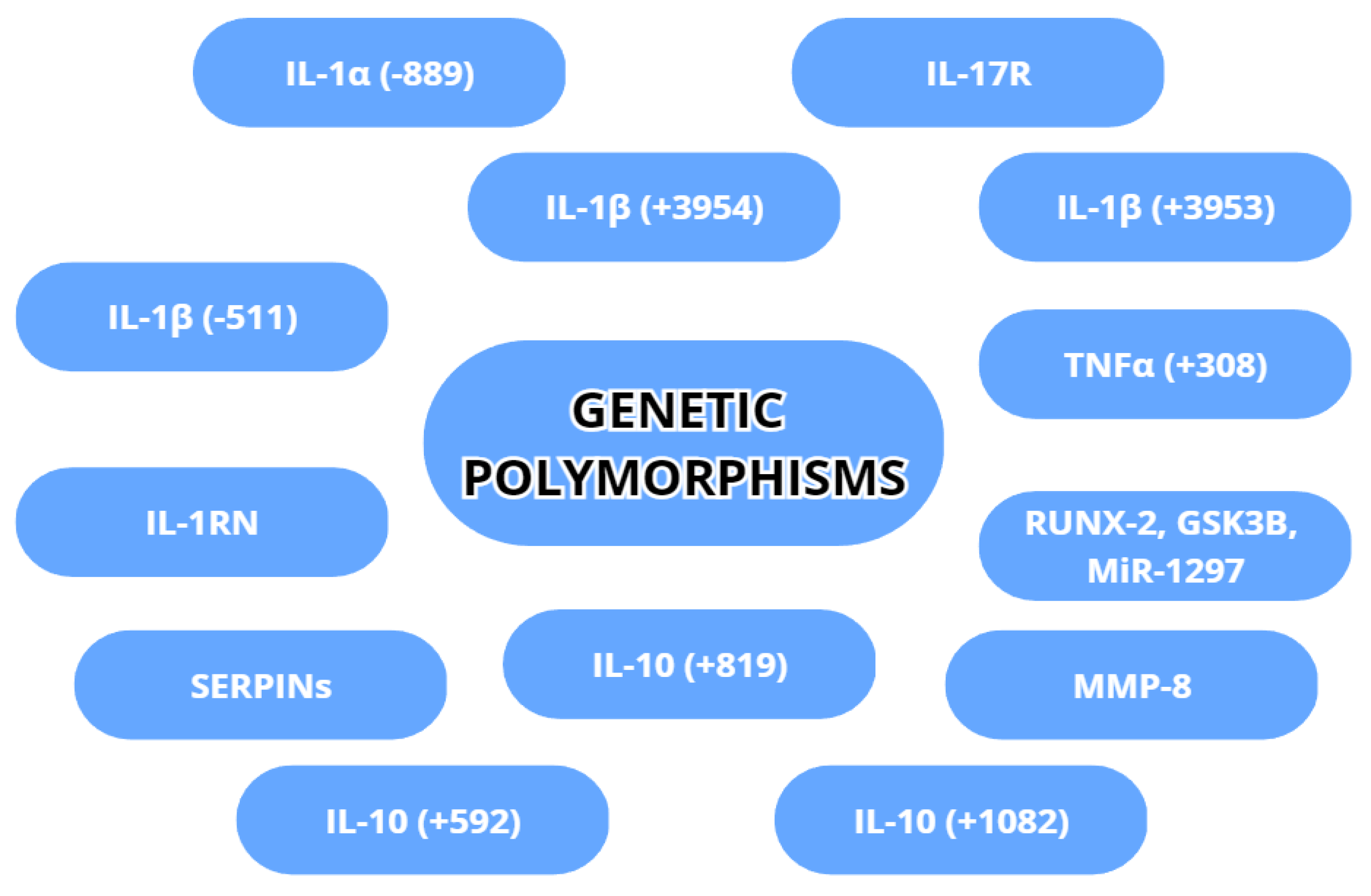
3.4. Genetic Differences Increasing Risk of Peri-Implantitis
3.4.1. IL-1β (+3953/+3954)
3.4.2. IL-1β (−511)
3.4.3. IL-1α (−889)
3.4.4. TNFα (+308)
3.4.5. MMP-8
3.4.6. IL-10 (+1082), (+819) and (+592)
3.4.7. IL-17R and IL-1RN
3.4.8. SERPINs
3.4.9. Other Important Genetic Factors: RUNX-2, GSK3B and MiR-1297
3.4.10. Peri-Implantitis’ Genetic Link to Other Diseases
3.5. Cellular Factors
3.6. Diagnostic Opportunities (aMMP-8, TNFα, IL-1β, IL-6)
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cervino, G.; Fiorillo, L.; Iannello, G.; Santonocito, D.; Risitano, G.; Cicciù, M. Sandblasted and acid etched titanium dental implant surfaces systematic review and confocal microscopy evaluation. Materials 2019, 12, 1763. [Google Scholar] [CrossRef]
- Moraschini, V.; Poubel, L.A.; Ferreira, V.F.; Barboza Edos, S. Evaluation of survival and success rates of dental implants reported in longitudinal studies with a follow-up period of at least 10 years: A systematic review. Int. J. Oral Maxillofac. Surg. 2015, 44, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Avila-Ortiz, G.; Gonzalez-Martin, O.; Couso-Queiruga, E.; Wang, H.L. The peri-implant phenotype. J. Periodontol. 2020, 91, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Smeets, R.; Henningsen, A.; Jung, O.; Heiland, M.; Hammächer, C.; Stein, J.M. Definition, etiology, prevention and treatment of peri-implantitis—A review. Head Face Med. 2014, 10, 34. [Google Scholar] [CrossRef] [PubMed]
- Socransky, S.S.; Haffajee, A.D.; Cugini, M.A.; Smith, C.; Kent, R.L., Jr. Microbial complexes in subgingival plaque. J. Clin. Periodontol. 1998, 25, 134–144. [Google Scholar] [CrossRef]
- Sahrmann, P.; Gilli, F.; Wiedemeier, D.B.; Attin, T.; Schmidlin, P.R.; Karygianni, L. The Microbiome of Peri-Implantitis: A Systematic Review and Meta-Analysis. Microorganisms 2020, 8, 661. [Google Scholar] [CrossRef]
- Liu, C.; Chu, D.; Kalantar-Zadeh, K.; George, J.; Young, H.A.; Liu, G. Cytokines: From Clinical Significance to Quantification. Adv. Sci. 2021, 8, e2004433. [Google Scholar] [CrossRef]
- Brinkmann, J.; Zeißler, E.-C.; Scharrenberg, J.S.; Schenk, J.; Majjouti, M.; Oberste, M.; Yagdiran, A.; Scheyerer, M.J.; Jung, N.; Siewe, J.; et al. The diagnostic value of cytokines for the discrimination of vertebral osteomyelitis and degenerative diseases of the spine. Cytokine 2022, 150, 155782. [Google Scholar] [CrossRef]
- Ma, Y.M.; Zhang, Y.; Bi, Y.; He, L.; Li, D.; Wang, D.; Wang, M.; Wang, X.M. Diagnostic value of carcinoembryonic antigen combined with cytokines in serum of patients with colorectal cancer. Medicine 2022, 101, e30787. [Google Scholar] [CrossRef]
- Karakike, E.; Giamarellos-Bourboulis, E.J. Macrophage Activation-Like Syndrome: A Distinct Entity Leading to Early Death in Sepsis. Front. Immunol. 2019, 10, 55. [Google Scholar] [CrossRef]
- Brockman, M.; Kwon, D.S.; Tighe, D.P.; Pavlik, D.F.; Rosato, P.C.; Sela, J.; Porichis, F.; Le Gall, S.; Waring, M.T.; Moss, K.; et al. IL-10 is up-regulated in multiple cell types during viremic HIV infection and reversibly inhibits virus-specific T cells. Blood 2009, 114, 346–356. [Google Scholar] [CrossRef]
- Plemmenos, G.; Evangeliou, E.; Polizogopoulos, N.; Chalazias, A.; Deligianni, M.; Piperi, C. Central Regulatory Role of Cytokines in Periodontitis and Targeting Options. Curr. Med. Chem. 2021, 28, 3032–3058. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.L.; Garaicoa-Pazmino, C.; Collins, A.; Ong, H.S.; Chudri, R.; Giannobile, W.V. Protein biomarkers and microbial profiles in peri-implantitis. Clin. Oral Implant. Res. 2016, 27, 1129–1136. [Google Scholar] [CrossRef]
- Kirkwood, K.L.; Cirelli, J.A.; Rogers, J.E.; Giannobile, W.V. Novel host response therapeutic approaches to treat periodontal diseases. Periodontology 2007, 43, 294–315. [Google Scholar] [CrossRef] [PubMed]
- Acharya, A.; Koh, M.L.; Kheur, S.; Watt, R.M.; Jin, L.; Mattheos, N. Salivary IL-1β and red complex bacteria as predictors of the inflammatory status in sub-peri-implant niches of subjects with peri-implant mucositis. Clin. Oral Implant. Res. 2016, 27, 662–667. [Google Scholar] [CrossRef]
- Duarte, P.M.; Serrão, C.R.; Miranda, T.; Zanatta, L.C.S.; Bastos, M.F.; Faveri, M.; Figueiredo, L.C.; Feres, M. Could cytokine levels in the peri-implant crevicular fluid be used to distinguish between healthy implants and implants with peri-implantitis? A systematic review. J. Periodontal. Res. 2016, 51, 689–698. [Google Scholar] [CrossRef]
- Faot, F.; Nascimento, G.G.; Bielemann, A.M.; Campão, T.D.; Leite, F.R.; Quirynen, M. Can peri-implant crevicular fluid assist in the diagnosis of peri-implantitis? A systematic review and meta-analysis. J. Periodontol. 2015, 86, 631–645. [Google Scholar] [CrossRef]
- Delucchi, F.; Canepa, C.; Canullo, L.; Pesce, P.; Isola, G.; Menini, M. Biomarkers from Peri-Implant Crevicular Fluid (PICF) as Predictors of Peri-Implant Bone Loss: A Systematic Review. Int. J. Mol. Sci. 2023, 24, 3202. [Google Scholar] [CrossRef]
- Kido, R.; Kido, J.I.; Nishikawa, Y.; Sakamoto, E.; Tomotake, Y.; Yumoto, H. Diagnosis of inflammatory peri-implant diseases using an immunochromatographic assay for calprotectin in peri-implant crevicular fluid. Int. J. Implant. Dent. 2021, 7, 106. [Google Scholar] [CrossRef]
- Sakamoto, E.; Kido, R.; Tomotake, Y.; Naitou, Y.; Ishida, Y.; Kido, J.I. Calprotectin and cross-linked N-telopeptides of type I collagen levels in crevicular fluid from implant sites with peri-implant diseases: A pilot study. Int. J. Implant. Dent. 2018, 4, 26. [Google Scholar] [CrossRef]
- Giannobile, W.V.; McDevitt, J.T.; Niedbala, R.S.; Malamud, D. Translational and clinical applications of salivary diagnostics. Adv. Dent. Res. 2011, 23, 375–380. [Google Scholar] [CrossRef]
- Silva, R.C.E.; Reis, M.B.L.; Arid, J.; Flores, E.K.B.; Cruz, G.V.; Marañón-Vásquez, G.A.; De Souza, L.K.F.; Novaes, A.B., Jr.; De Queiroz, A.M.; Küchler, E.C. Association between Genetic Polymorphisms in RANK, RANKL and OPG and Peri-Implant Diseases in Patients from the Amazon Region. Braz. Dent. J. 2020, 31, 63–68. [Google Scholar] [CrossRef]
- Thierbach, R.; Maier, K.; Sorsa, T.; Mäntylä, P. Peri-Implant Sulcus Fluid (PISF) Matrix Metalloproteinase (MMP)-8 Levels in Peri-Implantitis. J. Clin. Diagn. Res. 2016, 10, ZC34–ZC38. [Google Scholar] [CrossRef]
- Astolfi, V.; Ríos-Carrasco, B.; Gil-Mur, F.J.; Ríos-Santos, J.V.; Bullón, B.; Herrero-Climent, M.; Bullón, P. IIncidence of Peri-Implantitis and Relationship with Different Conditions: A Retrospective Study. Int. J. Environ. Res. Public Health 2022, 19, 4147. [Google Scholar] [CrossRef]
- Plemmenos, G.; Piperi, C. Pathogenic Molecular Mechanisms in Periodontitis and Peri-Implantitis: Role of Advanced Glycation End Products. Life 2022, 12, 218. [Google Scholar] [CrossRef]
- Petkovic-Curcin, A.; Zeljic, K.; Cikota-Aleksic, B.; Dakovic, D.; Tatic, Z.; Magic, Z. Association of Cytokine Gene Polymorphism with Peri-implantitis Risk. Int. J. Oral Maxillofac. Implant. 2017, 32, e241–e248. [Google Scholar] [CrossRef]
- Insua, A.; Monje, A.; Wang, H.L.; Miron, R.J. Basis of bone metabolism around dental implants during osseointegration and peri-implant bone loss. J. Biomed. Mater. Res. A 2017, 105, 2075–2089. [Google Scholar] [CrossRef]
- D’Ambrosio, F.; Caggiano, M.; Schiavo, L.; Savarese, G.; Carpinelli, L.; Amato, A.; Iandolo, A. Chronic Stress and Depression in Periodontitis and Peri-Implantitis: A Narrative Review on Neurobiological, Neurobehavioral and Immune-Microbiome Interplays and Clinical Management Implications. Dent. J. 2022, 10, 49. [Google Scholar] [CrossRef]
- Mancini, L.; Americo, L.M.; Pizzolante, T.; Donati, R.; Marchetti, E. Impact of COVID-19 on Periodontitis and Peri-Implantitis: A Narrative Review. Front. Oral Health 2022, 3, 822824. [Google Scholar] [CrossRef]
- Sahoo, S.K.; Jalaluddin, M.; Bhuyan, L.; Dash, K.C.; Mishra, S.; Mishra, P. Assessment of Cytokine and Herpesvirus Level in Peri-implantitis and Healthy Patients. J. Pharm. Bioallied. Sci. 2021, 13 (Suppl. S2), S1418–S1421. [Google Scholar] [CrossRef]
- Baseri, M.; Radmand, F.; Hamedi, R.; Yousefi, M.; Kafil, H.S. Immunological Aspects of Dental Implant Rejection. BioMed Res. Int. 2020, 2020, 7279509. [Google Scholar] [CrossRef]
- Corrêa, M.G.; Pimentel, S.P.; Ribeiro, F.V.; Cirano, F.R.; Casati, M.Z. Host response and peri-implantitis. Braz. Oral. Res. 2019, 33 (Suppl. S1), e066. [Google Scholar] [CrossRef]
- Al-Majid, A.; Alassiri, S.; Rathnayake, N.; Tervahartiala, T.; Gieselmann, D.R.; Sorsa, T. Matrix Metalloproteinase-8 as an Inflammatory and Prevention Biomarker in Periodontal and Peri-Implant Diseases. Int. J. Dent. 2018, 2018, 7891323. [Google Scholar] [CrossRef]
- Nickles, K.; Krebs, M.; Schacher, B.; Petsos, H.; Eickholz, P. Long-Term Results after Placing Dental Implants in Patients with Papillon-Lefèvre Syndrome: Results 2.5–20 Years after Implant Insertion. J. Clin. Med. 2022, 11, 2438. [Google Scholar] [CrossRef] [PubMed]
- Al-Askar, M.; Ajlan, S.; Alomar, N.; Al-Daghri, N.M. Clinical and Radiographic Peri-Implant Parameters and Whole Salivary Interleukin-1β and Interleukin-6 Levels among Type-2 Diabetic and Nondiabetic Patients with and without Peri-Implantitis. Med. Princ. Pract. 2018, 27, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, M.H.; Gomes, P.S. Bone Cells Dynamics during Peri-Implantitis: A Theoretical Analysis. J. Oral Maxillofac. Res. 2016, 7, e6. [Google Scholar] [CrossRef] [PubMed]
- Alassy, H.; Parachuru, P.; Wolff, L. Peri-Implantitis Diagnosis and Prognosis Using Biomarkers in Peri-Implant Crevicular Fluid: A Narrative Review. Diagnostics 2019, 9, 214. [Google Scholar] [CrossRef]
- Martins, L.R.L.; Grzech-Leśniak, K.; dos Santos, N.C.; Suárez, L.J.; Giro, G.; Bastos, M.F.; Shibli, J.A. Transcription Factor AhR, Cytokines IL-6 and IL-22 in Subjects with and without Peri-Implantitis: A Case Control-Study. Int. J. Environ. Res. Public Health 2022, 19, 7434. [Google Scholar] [CrossRef]
- Lähteenmäki, H.; Tervahartiala, T.; Räisänen, I.T.; Pärnänen, P.; Mauramo, M.; Gupta, S.; Sampson, V.; Rathnayake, N.; Heikkinen, A.; Alassiri, S.; et al. Active MMP-8 point-of-care (PoC)/chairside enzyme-test as an adjunctive tool for early and real-time diagnosis of peri-implantitis. Clin. Exp. Dent. Res. 2022, 8, 485–496. [Google Scholar] [CrossRef]
- Kalsi, A.S.; Moreno, F.; Petridis, H. Biomarkers associated with periodontitis and peri-implantitis: A systematic review. J. Periodontal. Implant. Sci. 2021, 51, 3–17. [Google Scholar] [CrossRef]
- Jiang, J.; Gao, G.; Wang, Q. Levels of SERPIN family proteins in peri-implant crevicular fluid in patients with peri-implantitis. J. Clin. Lab. Anal. 2021, 35, e23926. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, L.C.; Bueno-Silva, B.; Nogueira, C.F.P.; Valadares, L.C.; Garcia, K.M.M.; Filho, G.C.D.L.; Milanello, L.; Esteves, F.M.; Shibli, J.A.; Miranda, T.S. Levels of Gene Expression of Immunological Biomarkers in Peri-Implant and Periodontal Tissues. Int. J. Environ. Res. Public Health 2020, 17, 9100. [Google Scholar] [CrossRef] [PubMed]
- Ata-Ali, J.; Flichy-Fernández, A.J.; Alegre-Domingo, T.; Ata-Ali, F.; Palacio, J.; Peñarrocha-Diago, M. Clinical, microbiological, and immunological aspects of healthy versus peri-implantitis tissue in full arch reconstruction patients: A prospective cross-sectional study. BMC Oral Health 2015, 15, 43. [Google Scholar] [CrossRef]
- Gleiznys, D.; Gleiznys, A.; Abraškevičiūtė, L.; Vitkauskienė, A.; Šaferis, V.; Sakalauskienė, J. Interleukin-10 and Interleukin-1β Cytokines Expression in Leukocytes of Patients with Chronic Peri-Mucositis. Med. Sci. Monit. 2019, 25, 7471–7479. [Google Scholar] [CrossRef]
- Aleksandrowicz, P.; Brzezińska-Błaszczyk, E.; Kozłowska, E.; Żelechowska, P.; Borgonovo, A.E.; Agier, J. Analysis of IL-1β, CXCL8, and TNF-α levels in the crevicular fluid of patients with periodontitis or healthy implants. BMC Oral Health 2021, 21, 120. [Google Scholar] [CrossRef] [PubMed]
- Ghassib, I.; Chen, Z.; Zhu, J.; Wang, H.L. Use of IL-1 β, IL-6, TNF-α, and MMP-8 biomarkers to distinguish peri-implant diseases: A systematic review and meta-analysis. Clin. Implant. Dent. Relat. Res. 2019, 21, 190–207. [Google Scholar] [CrossRef]
- Yaghobee, S.; Khorsand, A.; Paknejad, M. Comparison of interleukin-1β levels in gingival crevicular fluid and peri-implant crevicular fluid and its relationship with clinical indexes. J. Dent. 2013, 10, 1. [Google Scholar]
- Gao, X.; Zhou, J.; Sun, Y.; Wang, L.; Zhou, Y. Differential expressions of biomarkers in gingival crevicular fluid of Han and Uygur populations with peri-implantitis. Medicine 2018, 97, e0471. [Google Scholar] [CrossRef]
- Eckert, M.; Mizgalska, D.; Sculean, A.; Potempa, J.; Stavropoulos, A.; Eick, S. In vivo expression of proteases and protease inhibitor, a serpin, by periodontal pathogens at teeth and implants. Mol. Oral Microbiol. 2018, 33, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Darabi, E.; Kadkhoda, Z.; Amirzargar, A. Comparison of the levels of tumor necrosis factor-α and interleukin-17 in gingival crevicular fluid of patients with peri-implantitis and a control group with healthy implants. Iran. J. Allergy Asthma Immunol. 2013, 12, 75–80. [Google Scholar]
- Gomes, A.M.; Douglas-de-Oliveira, D.W.; Ferreira, S.D.; Silva, T.A.D.; Cota, L.O.M.; Costa, F.O. Periodontal disease, peri-implant disease and levels of salivary biomarkers IL-1β, IL-10, RANK, OPG, MMP-2, TGF-β and TNF-α: Follow-up over 5 years. J. Appl. Oral Sci. 2019, 27, e20180316. [Google Scholar] [CrossRef] [PubMed]
- Alassiri, S.; Parnanen, P.; Rathnayake, N.; Johannsen, G.; Heikkinen, A.-M.; Lazzara, R.; Van Der Schoor, P.; Van Der Schoor, J.G.; Tervahartiala, T.; Gieselmann, D.; et al. The Ability of Quantitative, Specific, and Sensitive Point-of-Care/Chair-Side Oral Fluid Immunotests for aMMP-8 to Detect Periodontal and Peri-Implant Diseases. Dis. Markers 2018, 2018, 1306396. [Google Scholar] [CrossRef] [PubMed]
- Farhad, S.Z.; Rezazadeh, F.; Mohammadi, M. Interleukin-17 and Interleukin-10 as Inflammatory and Prevention Biomarkers in Periimplant Diseases. Int. J. Prev. Med. 2019, 10, 137. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zhang, X.; Huang, J.; Fan, X. Identification of key genes and pathways for peri-implantitis through the analysis of gene expression data. Exp. Ther. Med. 2017, 13, 1832–1840. [Google Scholar] [CrossRef]
- Zhang, X.; Wang, Z.; Hu, L.; Shen, X.; Liu, C. Identification of Potential Genetic Biomarkers and Target Genes of Peri-Implantitis Using Bioinformatics Tools. BioMed Res. Int. 2021, 2021, 1759214. [Google Scholar] [CrossRef]
- Mohammadi, H.; Roochi, M.M.; Sadeghi, M.; Garajei, A.; Heidar, H.; Meybodi, A.A.; Dallband, M.; Mostafavi, S.; Mostafavi, M.; Salehi, M.; et al. Association between Interleukin-1 Polymorphisms and Susceptibility to Dental Peri-Implant Disease: A Meta-Analysis. Pathogens 2021, 10, 1600. [Google Scholar] [CrossRef]
- Jin, Q.; Teng, F.; Cheng, Z. Association between common polymorphisms in IL-1 and TNFα and risk of peri-implant disease: A meta-analysis. PLoS ONE 2021, 16, e0258138. [Google Scholar] [CrossRef]
- Mo, Y.Y.; Zeng, X.T.; Weng, H.; Cen, Y.; Zhao, Q.; Wen, X. Association between tumor necrosis factor-alpha G-308A polymorphism and dental peri-implant disease risk: A meta-analysis. Medicine 2016, 95, e4425. [Google Scholar] [CrossRef]
- Hamdy, A.A.; Ebrahem, M.A. The effect of interleukin-1 allele 2 genotype (IL-1a(−889) and IL-1b(+3954)) on the individual’s susceptibility to peri-implantitis: Case-control study. J. Oral Implantol. 2011, 37, 325–334. [Google Scholar] [CrossRef] [PubMed]
- Lafuente-Ibáñez de Mendoza, I.; Setien-Olarra, A.; García-De la Fuente, A.M.; Aguirre-Urizar, J.M.; Marichalar-Mendia, X. Role of proinflammatory mutations in peri-implantitis: Systematic review and meta-analysis. Int. J. Implant. Dent. 2022, 8, 2. [Google Scholar] [CrossRef]
- Laine, M.L.; Leonhardt, A.; Roos-Jansåker, A.-M.; Pena, A.S.; van Winkelhoff, A.J.; Winkel, E.G.; Renvert, S. IL-1RN gene polymorphism is associated with peri-implantitis. Clin. Oral Implant. Res. 2006, 17, 380–385. [Google Scholar] [CrossRef]
- Jamshidy, L.; Tadakamadla, S.K.; Choubsaz, P.; Sadeghi, M.; Tadakamadla, J. Association of IL-10 and TNF-α Polymorphisms with Dental Peri-Implant Disease Risk: A Meta-Analysis, Meta-Regression, and Trial Sequential Analysis. Int. J. Environ. Res. Public Health 2021, 18, 7697. [Google Scholar] [CrossRef] [PubMed]
- Schminke, B.; Vom Orde, F.; Gruber, R.; Schliephake, H.; Bürgers, R.; Miosge, N. The pathology of bone tissue during peri-implantitis. J. Dent. Res. 2015, 94, 354–361. [Google Scholar] [CrossRef]
- Kadkhodazadeh, M.; Ebadian, A.R.; Amid, R.; Youssefi, N.; Mehdizadeh, A.R. Interleukin 17 receptor gene polymorphism in periimplantitis and chronic periodontitis. Acta Med. Iran. 2013, 51, 353–358. [Google Scholar] [PubMed]
- Ingendoh-Tsakmakidis, A.; Mikolai, C.; Winkel, A.; Szafrański, S.P.; Falk, C.S.; Rossi, A.; Walles, H.; Stiesch, M. Commensal and pathogenic biofilms differently modulate peri-implant oral mucosa in an organotypic model. Cell. Microbiol. 2019, 21, e13078. [Google Scholar] [CrossRef]
- Mijiritsky, E.; Ferroni, L.; Gardin, C.; Peleg, O.; Gultekin, A.; Saglanmak, A.; Delogu, L.G.; Mitrecic, D.; Piattelli, A.; Tatullo, M.; et al. Presence of ROS in Inflammatory Environment of Peri-Implantitis Tissue: In Vitro and In Vivo Human Evidence. J. Clin. Med. 2019, 9, 38. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zheng, J.; Gong, C.; Lan, K.; Shen, Y.; Ding, X. Development of an immunogenomic landscape for the competing endogenous RNAs network of peri-implantitis. BMC Med. Genet. 2020, 21, 208. [Google Scholar] [CrossRef] [PubMed]
- Yu, T.; Acharya, A.; Mattheos, N.; Li, S.; Ziebolz, D.; Schmalz, G.; Haak, R.; Schmidt, J.; Sun, Y. Molecular mechanisms linking peri-implantitis and type 2 diabetes mellitus revealed by transcriptomic analysis. PeerJ 2019, 7, e7124. [Google Scholar] [CrossRef] [PubMed]
- Dionigi, C.; Larsson, L.; Carcuac, O.; Berglundh, T. Cellular expression of DNA damage/repair and reactive oxygen/nitrogen species in human periodontitis and peri-implantitis lesions. J. Clin. Periodontol. 2020, 47, 1466–1475. [Google Scholar] [CrossRef]
- Li, Y.; Ling, J.; Jiang, Q. Inflammasomes in Alveolar Bone Loss. Front. Immunol. 2021, 12, 691013. [Google Scholar] [CrossRef]
- Galarraga-Vinueza, M.E.; Obreja, K.; Ramanauskaite, A.; Magini, R.; Begic, A.; Sader, R.; Schwarz, F. Macrophage polarization in peri-implantitis lesions. Clin. Oral Investig. 2021, 25, 2335–2344. [Google Scholar] [CrossRef]
- Tzach-Nahman, R.; Nashef, R.; Fleissig, O.; Palmon, A.; Shapira, L.; Wilensky, A.; Nussbaum, G. Oral fibroblasts modulate the macrophage response to bacterial challenge. Sci. Rep. 2017, 7, 11516. [Google Scholar] [CrossRef]
- Aleksandrowicz, P.; Żelechowska, P.; Agier, J.; Starska, K.; Kędzierski, K.; Wysokińska-Miszczuk, J.; Brzezińska-Błaszczyk, E. Evaluation of Metalloproteinase-8 Levels in Crevicular Fluid of Patients with Healthy Implants or Periodontitis. Mediat. Inflamm. 2017, 2017, 4920847. [Google Scholar] [CrossRef]
- Guarnieri, R.; Zanza, A.; D’Angelo, M.; Di Nardo, D.; Del Giudice, A.; Mazzoni, A.; Reda, R.; Testarelli, L. Correlation between Peri-Implant Marginal Bone Loss Progression and Peri-Implant Sulcular Fluid Levels of Metalloproteinase-8. J. Pers. Med. 2022, 12, 58. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S286–S291. [Google Scholar] [CrossRef] [PubMed]
- Buser, D.; Weber, H.P.; Lang, N.P. Tissue integration of non-submerged implants. 1-year results of a prospective study with 100 ITI hollow-cylinder and hollow-screw implants. Clin. Oral Implant. Res. 1990, 1, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Misch, C.E.; Perel, M.L.; Wang, H.-L.; Sammartino, G.; Galindo-Moreno, P.; Trisi, P.; Steigmann, M.; Rebaudi, A.; Palti, A.; Pikos, M.A.; et al. Implant success, survival, and failure: The International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference. Implant. Dent. 2008, 17, 5–15. [Google Scholar] [CrossRef]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S1–S8. [Google Scholar] [CrossRef]
- Araujo, M.G.; Lindhe, J. Peri-implant health. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S230–S236. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89 (Suppl. S1), S159–S172, Erratum in J. Periodontol. 2018, 89, 1475. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.A.; Salvi, G.E. Peri-implant mucositis. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S237–S245. [Google Scholar] [CrossRef]
- Schwarz, F.; Derks, J.; Monje, A.; Wang, H.-L. Peri-implantitis. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S246–S266. [Google Scholar] [CrossRef] [PubMed]
- Renvert, S.; Persson, G.R.; Pirih, F.Q.; Camargo, P.M. Peri-implant health, peri-implant mucositis, and peri-implantitis: Case definitions and diagnostic considerations. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S278–S285. [Google Scholar] [CrossRef] [PubMed]
- Naruishi, K.; Nagata, T. Biological effects of interleukin-6 on Gingival Fibroblasts: Cytokine regulation in periodontitis. J. Cell. Physiol. 2018, 233, 6393–6400. [Google Scholar] [CrossRef]
- Luchian, I.; Goriuc, A.; Sandu, D.; Covasa, M. The Role of Matrix Metalloproteinases (MMP-8, MMP-9, MMP-13) in Periodontal and Peri-Implant Pathological Processes. Int. J. Mol. Sci. 2022, 23, 1806. [Google Scholar] [CrossRef]
- Hienz, S.A.; Paliwal, S.; Ivanovski, S. Mechanisms of Bone Resorption in Periodontitis. J. Immunol. Res. 2015, 2015, 615486. [Google Scholar] [CrossRef] [PubMed]
- Groeger, S.; Meyle, J. Oral Mucosal Epithelial Cells. Front. Immunol. 2019, 10, 208. [Google Scholar] [CrossRef]
- Abusleme, L.; Moutsopoulos, N.M. IL-17: Overview and role in oral immunity and microbiome. Oral Dis. 2017, 23, 854–865. [Google Scholar] [CrossRef]
- Bunte, K.; Beikler, T. Th17 Cells and the IL-23/IL-17 Axis in the Pathogenesis of Periodontitis and Immune-Mediated Inflammatory Diseases. Int. J. Mol. Sci. 2019, 20, 3394. [Google Scholar] [CrossRef]
- Wang, P.-L.; Shirasu, S.; Shinohar, M.; Azuma, Y.; Daito, M.; Yasuda, H.; Ohura, K. IL-10 inhibits Porphyromonas gingivalis LPS-stimulated human gingival fibroblasts production of IL-6. Biochem. Biophys. Res. Commun. 1999, 263, 372–377. [Google Scholar] [CrossRef]
- Gettins, P.G.; Olson, S.T. Inhibitory serpins. New insights into their folding, polymerization, regulation and clearance. Biochem. J. 2016, 473, 2273–2293. [Google Scholar] [CrossRef] [PubMed]
- García-Delaney, C.; Sánchez-Garcés, M.Á.; Figueiredo, R.; Sánchez-Torres, A.; Gay-Escoda, C. Clinical significance of interleukin-1 genotype in smoking patients as a predictor of peri-implantitis: A case-control study. Med. Oral Patol. Oral Cir. Bucal. 2015, 20, e737–e743. [Google Scholar] [CrossRef] [PubMed]
- Kormas, I.; Pedercini, C.; Pedercini, A.; Raptopoulos, M.; Alassy, H.; Wolff, L.F. Peri-Implant Diseases: Diagnosis, Clinical, Histological, Microbiological Characteristics and Treatment Strategies. A Narrative Review. Antibiotics 2020, 9, 835. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number [Citation] | Authors | Journal | Date of Publication | Type | Results |
|---|---|---|---|---|---|
| 1 [7] | Liu C. et al. | Advanced Science | 2021 | Review | Most well-known pro-inflammatory cytokines are IL-1, IL-6, IL-8, IL-12, IL-18, IFN-α/γ, and TNF- α. The anti-inflammatory cytokines are IL-1 RA, IL-4, IL-6, IL-10, IL-11, IL-13, and TGF-β. There are many ways of cytokine detection like ELISA assay, PoC testing, multiplex detection, flow cytometry, Luminex assays and MSD assays. |
| 2 [22] | E Silva R. et al. | Brazilian Dental Journal | 2020 | Article | Smoking, alcoholism, lack of hygene, type 2 diabetes and thin gingival biotype increase the risk of peri-implantitis. RANK, RANKL and OPG polymorphisms did not increase the risk of peri-implantitis in amazon population. |
| 3 [23] | Thierbach R. et al. | Journal of Clinical and Diagnostic Research | 2016 | Article | Although treatment decreases MMP-8 levels, the inflammatory levels are still present. Risk alleles were present in 54% examined patients. |
| 4 [24] | Astolfi V. et al. | International Journal of Environmental Research and Public Health | 2022 | Article | Smoking, lack of regular follow-up visits and previous periodontal problems increase the chance of peri-implantitis, external abutment connection increases the risk of peri-implantitis |
| 5 [25] | Plemmenos G. et al. | Life | 2022 | Review | Hyperglycemia and smoking have an adverse effect on peri-implant tissues, type 2 diabetes promotes AGE production, past periodontal problems make peri-implant tissues more sensitive to AGE and oxidative stress |
| 6 [26] | Petkovic-Curcin A. et al. | The International Jounral of Oral & Maxillofacial Implants | 2017 | Article | Smoking and previous periodontitis increase the chance of peri-implantitis. Patients with peri-implantitis had more frequently IL-10 (−1082), IL-1RN and TNFα (308) genetic polymorphisms. Smoking elevates the risk if combined with mentioned polymorphisms. |
| 7 [27] | Insua A. et al. | Journal of Biomedical Materials Research | 2017 | Narrative Review | The effects of systemic levels of cholesterol, fatty acids and vitamin D may be responsible factors for early implant loss and long-term implant stability. Immune cells have prolific impact on dental implant osseointegration and maintenance. |
| 8 [28] | D’Ambrosio F. et al. | Dentistry Journal | 2022 | Review | Tobacco smoking, alcohol consumption, unhealthy diets, chronic stress and depression are promoting dysbiosis, immunologic deficiencies and inflammatory environment, increasing the chance of peri-implantitis. SARS-CoV-2 virus promoted disregulated production of especially IL-1beta, IL-6 and IFN-γ. |
| 9 [29] | Mancini L. et al. | Frontiers in Oral Health | 2022 | Mini Review | COVID-19 infection may increase the production of MMP-8, leading to increased chance of peri-implant diseases when combined with poor oral hygene |
| 10 [30] | Sahoo S.K. et al. | Journal of Pharmacy & Bioallied Sciences | 2021 | Article | In peri-implantitis IL-1β level is greatly increased. IL-8 and MMP-1 is decreased compared with healthy patients. Herpesviridae (HHV-4, HHV-6 and HHV-7) increase the expression of pro-inflammatory cytokines. |
| 11 [31] | Baseri M. et al. | BioMed Research International | 2020 | Review | Increase in local macrophage and T-limphocytes may be due to type 4 hypersensitivity towards titanium particles, in periimplantitis macrophages balance shift towards pro-inflammatory M1 form, levels of IL-1β, IL-2, IL-8, IL-17, MMP-7, MMP-8, MMP-9 are increased in peri-implantitis, the RANKL/OPG ratio favours osteoclastogenesis, IL-1β can be used as earl diagnostic cytokine |
| 12 [32] | Corrêa M. et al. | Brazilian Oral Research | 2019 | Review | In peri-implantitis there are elevated levels of IL-1β, TNFα, IL-8, IL-17, IL-23, MMP-1, MMP-8, RANKL and decreased levels of PPARγ, IL-10, TIMP-1, OPG, BMP-7, RUNX, IL-1RA. Furthermore, the polymorphisms of IL-1β (−511), MMP-1 (G-1607GG), TNFα (308) may increase the risk of peri-implantitis. TNFα and IL-1β can have diagnostic potential. |
| 13 [33] | Al-Majid A. et al. | International Journal of Dentistry | 2018 | Review | aMMP-8 can detect subclinical periimplantitis stages, MMP-8 levels correlate positively with the bacteria infection, TIMP/MMP-8 tests are more sensitive and precise than sole MMP-8 tests, smokers have decreased levels of MMP-8, obesity increases MMP-8 levels |
| 14 [34] | Nickles K. et al. | Journal of Clinical Medicine | 2022 | Case Report | In patients with Papillon-Lefevre syndrome, regular dental appointments delay the peri-implantitis |
| 15 [35] | Al.-Askar M. et al. | Medical Principles and Practise | 2018 | Article | Increased Hb1c levels and improper oral hygene lead to increased IL-1β and IL-6 levels in saliva. |
| 16 [36] | Fernandes M.H. et al. | Journal of Oral and Maxillofacial Research | 2016 | Review | Bone loss process is both direct and indirect. IL-1β, IL-6, TNFα, IL-17, IL-12, IL-8 are elevated, whereas IL-4, OPG and IL-10 are decreased. RUNX2, BMP-7 production is decreased, MMP-8 and MMP-7 are increased. Fibroblasts can restrain the immunological response, however LPS increases the production of IL-1, IL-6 and IL-8. |
| 17 [37] | Alassy H. et al. | Diagnostics | 2019 | Review | PICF in peri-implantitis contains more aMMP-8, IL-6, TNFα and IL-1β. IL-10 levels decreased in peri-implantitis. The disproportion between MMP-1/TIMP-1 and MMP-8 levels can serve for diagnostic purposes. IL-1β levels can serve as predictor marker for peri-implantitis. Peri-implantitis tissues contain more CD138, CD68 and MPO-positive cells than in periodontitis. |
| 18 [38] | Martins L. et al. | International Journal of Environmental Research and Public Health | 2022 | Brief Report | Increased level of AhR, IL-6 and GAPDH gene expression in peri-implantitis group |
| 19 [39] | Lähteenmäki H. et al. | Clinical and Experimental Dental Research | 2022 | Article | The levels of IL-6, MMP-8, aMMP-8, calprotectin was elevated in peri-implantitis, MMP-8 has the best diagnostic value from the measured cytokines |
| 20 [40] | Kalsi A.S. et al. | Journal of Periodontal and Implant Science | 2021 | Review | In peri-implantitis there are elevated levels of RANKL/sRANKL, TNFα, IL-6, IL-8, MMP-8, MMP-1 and decrease in IL-10, TIMP-1, TIMP-2, OPG, IL-10. Additionally, aquaporin-1 disregulation inhibits cell growth and cell homeostasis. |
| 21 [41] | Jiang J. et al. | Journal of Clinical Laboratory Analysis | 2021 | Article | SERPINs taking part in inflammatory process in peri-implantitis are SERPINB1, SERPINB3, SERPINB4 and SERPINB5. The increase in IL-6 and TNFα is positively correlated with SERPINs level increase. |
| 22 [41] | Jiang J. et al. | Journal of Clinical Laboratory Analysis | 2021 | Article | SERPINs taking part in inflammatory process in peri-implantitis are SERPINB1, SERPINB3, SERPINB4 and SERPINB5. The increase in IL-6 and TNFα is positively correlated with SERPINs level increase. |
| 23 [42] | Figueiredo L. et al. | International Journal of Environmental Research and Public Health | 2020 | Article | IL-1β levels are significantly more elevated in peri-implantitis than in periodontitis or control group. IL-6, TNFα, MMP-1, MMP-8, MMP-2, MMP-9, TIMP-1 and TIMP-2 levels are similar between peri-implantitis and periodontitis. |
| 24 [43] | Ata-Ali J. et al. | BMC Oral Health | 2015 | Article | Peri-implantitis group showed increased levels of IL-1β, IL-6, TNFα. The IL-1β/IL-10 ratio was significantly higher in peri-implantitis. Improper microbial control can lead to increased bone loss through inflammation. |
| 25 [44] | Gleiznys D. et al. | Medical Science Monitor | 2019 | Article | In peri-implant tissues IL-10 levels decrease and IL-1β increase. Highest increase of IL-1 is in the beginning of inflammatory process. |
| 26 [45] | Aleksandrowicz P. et al. | BMC Oral Health | 2021 | Article | The levels of IL-1β and TNFα are higher in periodontitis than in peri-implantitis, CXCL8 is dependent on the stage of periodontitis/ peri-implantitis and on patient susceptibility. Both IL-1β and TNFα can be used as diagnostic markers in periodontics |
| 27 [46] | Ghaasib I. et al. | Clinical Implant Dentistry and Related Research | 2019 | Systematic Review | Il-1β, IL-6, TNFα and MMP-8 levels were elevated in PICF. IL-1β and IL-6 level measurements can be used to differentiate healthy patients, mucositis and peri-implantitis. |
| 28 [47] | Yaghobee S. et al. | Journal of Dentistry of Teheran University of Medical Science | 2013 | Article | IL-1β levels positively correlate with PD, GI, BL, PL. The levels of IL-1β in PICF is higher than in GCF. |
| 29 [48] | Gao X. et al. | Medicine | 2018 | Observational Study | Higher levels of IL-1β and MMP-8 were detected in Han population than in Uygr population, whereas MMP-13 levels was higher in Uygr population. This may lead to different progression of peri-implantitis between the two groups. |
| 30 [49] | Eckert M. et al. | Molecular Oral Microbiology | 2018 | Pilot Study | Comparing teeth with implants, the levels of IL-1β in periodontitis exceeded those in peri-implantitis. The anti-inflammatory IL-10 was lower in periodontitis and peri-implantitis in comparison with gingivitis and mucositis. Expression of miropsin-1 was positively associated with levels of IL-1β and negatively associated with those of IL-10. Additionally, miropin may play a regulatory role in a multispecies dysbiotic biofilm forming on teeth and implant surfaces and may contribute to the initiation and/or progression of both periodontal and peri-implant diseases. |
| 31 [50] | Darabi E. et al. | Iranian Journal of Allergy, Asthma and Immunology | 2013 | Article | TNFα and IL-17 levels were greatly increased compared with healthy patients, IL-17 levels are positively correlated with probing depth |
| 32 [51] | Gomes A.M. et al. | Journal of Applied Oral Science | 2019 | Article | The peri-implant maintenance therapy significantly lowered TNFα levels. Increased salivary TNFα levels was associated with worse peri-implant clinical condition. |
| 33 [52] | Alassiri S. et al. | Disease Markers | 2018 | Review | Periimplantitis site has elevated MMP-8 levels, MMP-8 PoC/Chairside tests have 76–90% sensitivity and 96% specificity |
| 34 [53] | Farhad S.Z. et al. | International Journal of Preventive Denstistry | 2019 | Article | The highest levels of IL-17 were detected in peri-implant mucositis, followed by peri-implantitis. IL-10 level was the highest in peri-implantitis group. |
| 35 [54] | Zhang H. et al. | Experimental and Therapeutic Medicine | 2017 | Article | IL-6, TLR-4, N1, IL1β, MMP9, CXCL8, CXCR4, CXCL1, PECAM1, and SPP1 genes are upregulated in peri-implantitis. Key genes in peri-implantitis are IL-6 and IL-1β |
| 36 [55] | Zhang X. et al. | BioMed Research International | 2021 | Research Article | In periimplantitis there are 2 upregulated DEGs that are also upregulated in Alzheimer's Disease, HSP90AA1 and NFκB are also upregulated modulating osteoclasts, OPG and RANK |
| 37 [56] | Mohammadi H. et al. | Pathogens | 2021 | Review | Periimplantitis is noted more frequently if IL-1β (+3954), IL-1α (−889) are present. |
| 38 [57] | Jin Q. et al. | PLoS ONE | 2021 | Research Article | IL-1α (−889), IL-1β (+3954) and IL-1β (−511) may be more frequently found in periimplantitis. TNFα genotypes did not have direct influence in increasing periimplantitis risk. |
| 39 [58] | Mo Y.Y. et al. | Medicine | 2016 | Systematic Review | TNFα (308) gene polymorphism is associated with higher risk of peri-implantitis. The risk is of implant failure is further elevated by smoking. IL-1α (−889) and IL-1β (+3954) are potentially seen as risk factors in peri-implantitis. |
| 40 [59] | Hamdy A.A. et al. | Journal of Oral Implantology | 2011 | Article | Combination of IL-1α (−889) and Il-1β (+3954) polymorphisms may act as risk factor for tissue destruction and peri-implantitis. Furthermore, IL-1 gene polymorphisms can have negative effect on treatment response and result in genotype-positive patients. |
| 41 [60] | Lafuente-Ibáñez de Mendoza I. et al. | International Journal of Implant Dentistry | 2022 | Review | There is no direct evidence that IL-1β (+3954), IL-10 (−1081), IL-6 (−174) or TNFα (308) have higher risk of developing peri-implantitis, however composite genotypes IL-1α(−889)/IL-1β (+3954) IL-1α(−889)/IL-1β (+3953) combined with smoking >20 cigarettes a day significantly increase the bone loss and contributes to peri-implantitis. |
| 42 [61] | Laine M.L. et al. | Clinical Oral Implants Research | 2006 | Article | IL-1β (+3954), IL-1α (−889), IL-1RN polymorphisms were detected more often in peri-implantitis patients and can be assumed to represent as risk factors for peri-implantitis. Smoking increases the chance of peri-implantitis. |
| 43 [62] | Jamshidy L. et al. | International Journal of Environmental Research and Public Health | 2021 | Review | TNFα (308) gene polymorphism is associated with higher risk of peri-implantitis, especially in Asian ethnicity population |
| 44 [63] | Schminke B. et al. | Journal of Dental Resarch | 2015 | Research Report | In periimplantitis IL-8, MMP-8 and -9 are upregulated, BMP-9 and PPARγ are downregulated, RUNX levels decrease with the bone destruction progression |
| 45 [64] | Kadkhodazadeh M. et al. | Acta Medica Iranica | 2013 | Report | IL-17RA polymorphism doesn't increase the chance of periimplantitis incidence |
| 46 [65] | Ingendoh-Tsakmakidis A. et al. | Cellular Microbiology | 2019 | Research Article | In peri-implantitis, upregulated genes were related either linked to cell division (FIGN, HMGA2, CDC25A, and ERCC6L) or to DNA repair/damage (CLSPN, POLQ, and FANCA). The pathway analysis of the downregulated genes related to this signal transduction (MDM2, IL2RG, TLR4, and F2R). S. oralis modulated response of tissues in a way to modulate the peri-implant tissue process. |
| 47 [66] | Mijiritsky E. et al. | Journal of Clinical Medicine | 2020 | Article | Connective tissue in peri-implantitis has a large number of neutrophils and the structure of the tissue is disorganized, collagen type III production is increased, osteogenic pathways were downregulated, ROS pathways were upregulated |
| 48 [67] | Li Y. et al. | BMC Medical Genetics | 2020 | Research Article | GSK3B and miR-1297 may have important significance in the immune microenvironment and pathogenesis of peri-implantitis. |
| 49 [68] | Yu T. et al. | PeerJ | 2019 | Article | There are 92 common genes between periimplantitis and type 2 diabetes, 3 of which (IL6, NFKB1, PIK3CG) are the same, IL-17 expression |
| 50 [69] | Dionigi C. et al. | Journal of Clinical Periodontology | 2020 | Article | Compared to periodontitis, periimplantitis has increased neutrophil, macrophage and iNOS-positive cells. Epithelium and connective tissue were thicker in periimplantitis than periodontitis. |
| 51 [70] | Li Y. et al. | Frontiers in Immunology | 2021 | Review | Inflammasomes can be a target point for drugs, periimplantitis tissues have elevated IL-1β and IL-18. Increased NLRP3 levels if P. gingivalis or C. albicans are present |
| 52 [71] | Galarraga-Vinuenza M. et al. | Clinical Oral Investigations | 2021 | Article | Enhanced M1 macrophages polarization and higher M1/M2 ratio are found in peri-implantitis sites. M1 phenotype leads to exacerbated osteolysis and inflammatory response, accelerating the peri-implantits progression. |
| 53 [72] | Tzah-Nahman R. et al. | Scientific Reports | 2017 | Article | Increased PDLF levels stimulate TNFα and IL-1β production as well as spontaneous production of IL-6 by macrophages. Blocking IL-6 or IL-10 production reduced fibroblasts modulatory effect and promoted macrophage phagocytosis when bacterial challenge occurred |
| 54 [73] | Aleksandrowicz P. et al. | Medicators of Infammation | 2017 | Research Article | Monitoring of MMP-8 level in PISF could help to diagnose mucositis/peri-implantitis in an early stage, prior to clinical manifestations, which may allow for quick start of appropriate therapy. |
| 55 [74] | Guarneri R. et al. | Journal of Personalized Medicine | 2022 | Article | The initial high level of aMMP8 can be considered as indicators of the subsequent progression of peri-implant bone loss. MMP-8 could be used as biomarker for identifying implants and patients that could present a high bone loss |
| Peri-Implant Health | Peri-Implantitis | Peri-Implantitis in the Absence of Previous Examinations |
|---|---|---|
| No clinical sign of inflammation | No sign or visible inflammation | No sign or visible inflammation |
| No bleeding/suppuration on gentle probing | Bleeding/suppuration on gentle probing | Bleeding/suppuration on gentle probing |
| Stable probing depth between examinations | Increased probing depth compared to previous examinations | Probing depth ≥ 6 mm |
| No crestal bone changes apart from initial bone remodeling | Crestal bone loss other than initial bone remodeling | Bone levels ≥ 3 mm apical of the most coronal portion of the intraosseous part of the implant |
| Pro-Inflammatory Cytokines | Anti-Inflammatory Cytokines |
|---|---|
| Interleukin-6 | Interleukin-10 |
| Interleukin-1 | Tissue Metalloproteinase Inhibitors (TIMPs) |
| Tumor Necrosis Factor α | Osteoprotegrin |
| Interleukin-8 | Interleukin-1RN |
| Interleukin-17 | Serase Protease Inhibitors (SERPINs) |
| Metalloproteinase-8 (MMP-8) and other MMPs |
| Cytokine | Function |
|---|---|
| Interleukin-6 | Stimulating acute phase protein synthesis, neutrophils production, fever mediation, B-cell growth stimulation |
| Interleukin-1α | Part of epithelial barrier, epithelium integrity preservation |
| Interleukin-1β | Modulating inflammatory response, pyrogen, pain hypersensitivity, cell proliferation |
| Tumor Necrosis Factor α | Immune cells modulation, cell signaling, inflammation regulation, response to bacterial lipopolysaccharide |
| Interleukin-8 | Neutrophil chemotaxis, phagocytosis stimulation |
| Interleukin-17 | Recruitment of immune cells (mainly neutrophils and monocytes) via chemokines, promotes inflammatory responses of IL-1β and TNF-α |
| Interleukin-10 | Anti-inflammatory agent, blocks NFkB activity resulting in decrease in osteoclasts formation, TNF-α regulation |
| MMP-8 | Catalyzes the degradation of collagen type III and I |
| MMP-2 | Collagen type IV degradation, cell-cell clustering |
| MMP-9 | Collagen type IV and V degradation, cooperation with MMP-2 in ECM remodeling |
| MMP-7 | Gelatin, fibronectin and proteoglycan degradation, probably plays role in wound healing |
| MMP-13 | Collagen type I, II and III degradation, tissue remodeling |
| TIMP-1 | MMPs inhibition, cell proliferation promotion |
| TIMP-2 | MMPs inhibition, complements TIMP-1 in maintaining tissues hemostasis |
| RANKL | Bone remodeling and regeneration control, cell proliferation, with RANK binding promotes osteoclasts formation and maturation |
| Osteoprotegrin | Suppression of osteoclasts formation by competitive binding to RANK |
| Cells Type | Function and Disfunction |
|---|---|
| Epithelial cells | Apical proliferation, γ-H2AX, iNOS, NOX2, MPO expression |
| Fibroblasts | Lowered collagen production, mainly type I and III |
| Macrophages | Tissue infiltration, cytokine production, phagocytosis |
| Neutrophyls | Tissue infiltration, cytokine production, NETosis, ROS production |
| Osteocytes | Bone matrix production reduction, inability to repair the damages |
| Osteoclasts | Bone destruction, influence the bone metabolism |
| Plasma cells | Maintaining inflammation process, humoral immunity |
| T-type lymphocytes | Maintaining inflammation process, cellular immunity |
| Dendritic cells | Inflammation modulation, affect Langerhans cells response |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chmielewski, M.; Pilloni, A. Current Molecular, Cellular and Genetic Aspects of Peri-Implantitis Disease: A Narrative Review. Dent. J. 2023, 11, 134. https://doi.org/10.3390/dj11050134
Chmielewski M, Pilloni A. Current Molecular, Cellular and Genetic Aspects of Peri-Implantitis Disease: A Narrative Review. Dentistry Journal. 2023; 11(5):134. https://doi.org/10.3390/dj11050134
Chicago/Turabian StyleChmielewski, Marek, and Andrea Pilloni. 2023. "Current Molecular, Cellular and Genetic Aspects of Peri-Implantitis Disease: A Narrative Review" Dentistry Journal 11, no. 5: 134. https://doi.org/10.3390/dj11050134
APA StyleChmielewski, M., & Pilloni, A. (2023). Current Molecular, Cellular and Genetic Aspects of Peri-Implantitis Disease: A Narrative Review. Dentistry Journal, 11(5), 134. https://doi.org/10.3390/dj11050134