


Understanding the Quality of Life and Its Related Factors in Orthodontics Postgraduate Students: A Mixed Methods Approach



Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Quantitative Sub-Study (Cross-Sectional)
2.3. Qualitative Sub-Study (Focused Ethnographic Perspective)
2.4. The Methods Integration Approach
2.5. Ethics
3. Results
3.1. Quantitative Findings
3.1.1. General Profile of Participants
3.1.2. Relationships between QOL and Sociodemographic, Academic, Occupational, and Health Variables
3.1.3. Potential Explanatory Factors for QOL Dimensions
3.2. Qualitative Findings
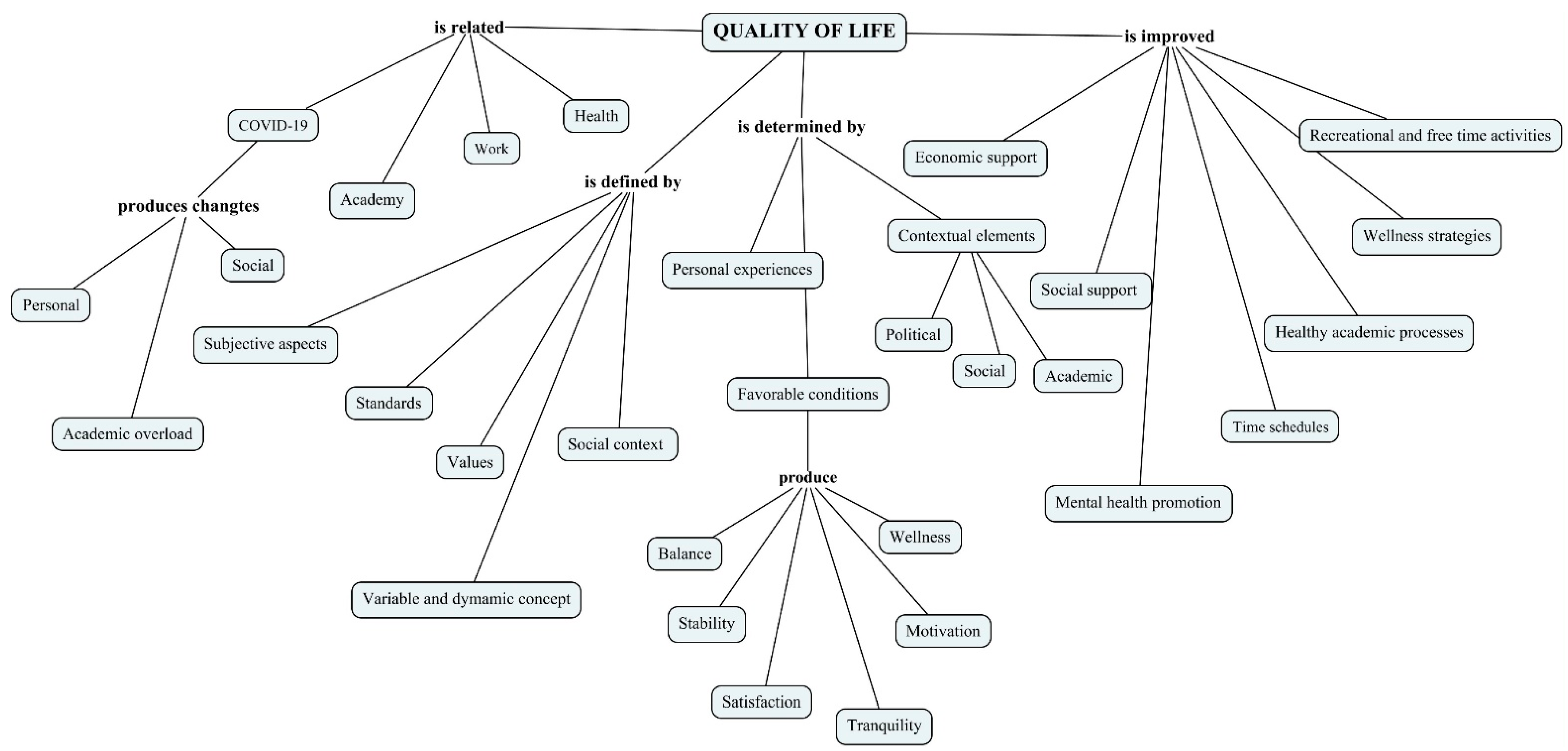
3.2.1. Quality of Life: Definitions, Determinants, and Satisfiers
“So those specific life conditions and those specific commitments from the, let’s say, personal point of view are the most important factor that makes the difference between the quality-of-life perception of different residents, considering that we all have something in common at this moment, which is the residency or the postgraduate degree, but there are certain things in each one’s life that can create those differences in regard to the perception of quality”.(FG 3)
3.2.2. A Roller Coaster Ride: The Postgraduate Training as a Personal and Academic Life Project
“I want to say something that has to do with the academic part obviously and it’s the patients, because I don’t know if in your universities it is like this, but in mine we have to get the patients, so you have to constantly be after people, looking for someone to be your patient and in the university, supposedly people goes there, but that’s a lie, no one goes there and it doesn’t matter to them if you got them, if you paid to them, if you didn’t, but is very difficult”.(FG 2)
4. Discussion
4.1. Main Findings
4.2. Possible Explanations of the Findings: What the Scientific Literature Tells Us on This Topic
4.3. Scope of This Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Karimi, M.; Brazier, J. Health, Health-Related Quality of Life, and Quality of Life: What is the Difference? Pharmacoeconomics 2016, 34, 645–649. [Google Scholar] [CrossRef] [PubMed]
- Haraldstad, K.; Wahl, A.; Andenæs, R.; Andersen, J.R.; Andersen, M.H.; Beisland, E.; Borge, C.R.; Engebretsen, E.; Eisemann, M.; Halvorsrud, L.; et al. A systematic review of quality of life research in medicine and health sciences. Qual. Life Res. 2019, 28, 2641–2650. [Google Scholar] [CrossRef] [PubMed]
- Pequeno, N.P.F.; Cabral, N.L.D.A.; Marchioni, D.M.; Lima, S.C.V.C.; Lyra, C.D.O. Quality of life assessment instruments for adults: A systematic review of population-based studies. Health Qual. Life Outcomes 2020, 18, 208. [Google Scholar] [CrossRef] [PubMed]
- Ryali, S.; Kumar, A.; Bhat, P.S. Study of quality of life among health workers and psychosocial factors influencing it. Ind. Psychiatry J. 2018, 27, 96–102. [Google Scholar] [CrossRef]
- Caicedo Fandiño, H.Y. Calidad de vida laboral en trabajadores de la salud en países latinoamericanos: Metaanálisis. Quality of working life in health workers in Latin American countries: A meta-analysis. SIGNOS-Investig. En Sist. De Gestión 2019, 11, 41–62. [Google Scholar] [CrossRef]
- Muñoz-Pino, N.; Tibaná-Guisao, A.E.; Cardona-Hincapié, J.D.; Hurtado-Aristizábal, A.; Agudelo-Suárez, A.A. Factors associated to quality of life of orthodontists graduated from a public university (1993-2016): A mixed-methods approach. Dent. Press J. Orthod. 2020, 25, 23e1–23e12. [Google Scholar] [CrossRef]
- Ghahramani, S.; Kasraei, H.; Hayati, R.; Tabrizi, R.; Marzaleh, M.A. Health care workers’ mental health in the face of COVID-19: A systematic review and meta-analysis. Int. J. Psychiatry Clin. Pract. 2022, 1–10. [Google Scholar] [CrossRef]
- Abraham, S.B.; Amini, A.M.A.; Khorshed, N.E.; Awad, M. Quality of life of dentists. Eur. J. Dent. 2018, 12, 111–115. [Google Scholar] [CrossRef][Green Version]
- Doshi, D.; Jain, A.; Vinaya, K.; Kotian, S. Quality of life among dentists in teaching hospitals in South Canara, India. Indian J. Dent. Res. 2011, 22, 552–555. [Google Scholar] [CrossRef]
- Nunes, M.D.F.; Freire, M.D.C.M. Quality of life among dentists of a local public health service. Rev. Saude Publica 2006, 40, 1019–1026. [Google Scholar] [CrossRef]
- World Health Organization. Division of mental health and prevention of substance abuse. In WHOQOL User Manual (Rev 2012); World Health Organization: Geneva, Geneva, 1998. [Google Scholar]
- López, R.V.; Sierra, J.L.; Díaz, S.P.; Agudelo, H.B. Calidad de vida laboral de los odontólogos en Antioquia 2011–2012 [Quality of working life for dentists in Antioquia 2011–2012]. Rev. Saude Publica 2020, 20, 684–691. [Google Scholar] [CrossRef]
- Machado, A.V.; Castro, C.O.; Filho, C.R.B.; Bruzamolin, C.D.; Scariot, R.; Pizzatto, E.; Gabardo, M.C.L. Anxiety and Sleep Quality in Dental Students at a Private Brazilian University. Bull. Tokyo Dent. Coll. 2020, 61, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Harrison, P.L.; Dds, L.M.S.; Garvan, C.W.; Behar-Horenstein, L.S. Wellness Among Dental Students: An Institutional Study. J. Dent. Educ. 2016, 80, 1119–1125. [Google Scholar] [CrossRef] [PubMed]
- Andre, A.; Pierre, G.C.; McAndrew, M. Quality of Life Among Dental Students: A Survey Study. J. Dent. Educ. 2017, 81, 1164–1170. [Google Scholar] [CrossRef]
- Masood, M.; Masood, Y.; Newton, T.J. Methods of Qualitative Research in Dentistry: A Review. Dent. Updat. 2010, 37, 326–336. [Google Scholar] [CrossRef]
- Nicolau, B.; Castonguay, G.; Levine, A.; Hong, Q.N.; Pluye, P.; Afrashtehfar, K.I.; Al-Sahan, M.; Amin, M.; Benbow, P.; de Oliveira, A.C.B.; et al. Applied Mixed Methods in Oral Health Research: Importance and Example of a Training Program. JDR Clin. Transl. Res. 2017, 2, 206–210. [Google Scholar] [CrossRef]
- Gupta, A. Use and misuse of mixed methods in population oral health research: A scoping review. Community Dent. Health 2018, 35, 109–118. [Google Scholar] [CrossRef]
- Abu Bakar, N.; Lim, S.L.; Basri, N.A.; Ludin, S.M. Mental Health and Well-Being of Undergraduate Dental Students: A Systematic Review. Int. J. CARE Sch. 2021, 4, 56–70. [Google Scholar] [CrossRef]
- Shetty, A.; Shetty, A.; Hegde, M.N.; Narasimhan, D.; Shetty, S. Stress and burnout assessment among post graduate dental students. J. Health Allied Sci. NU 2015, 05, 031–036. [Google Scholar] [CrossRef]
- Goldberg, D.; Williams, P. Cuestionario de Salud General. In GHQ General Health Questionnaire; GHQ; Masson: Barcelona, Spain, 1996. [Google Scholar]
- Bellón Saameño, J.A.; Delgado Sánchez, A.; Del del Castillo, J.D.; Lardelli Claret, P. Validity and reliability of the Duke-UNC-11 questionnaire of functional social support. Aten. Primaria 1996, 18, 153–156, 158–163. [Google Scholar]
- Carter, N.; Bryant-Lukosius, D.; DiCenso, A.; Blythe, J.; Neville, A.J. The Use of Triangulation in Qualitative Research. Oncol. Nurs. Forum 2014, 41, 545–547. [Google Scholar] [CrossRef] [PubMed]
- Yap, A.U.; Mah, E.X.Y.; Neo, A.S.K.; Leong, A.W.T. Perceived quality of life among oral health therapy and dental students: A cross-cultural comparison. Int. J. Dent. Hyg. 2021, 19, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Ghazanfar, H.; Iqbal, S.; Naseem, S. Quality of life of post-graduate medical students working in private and public hospitals in Punjab as measured by WHOQOL-BREF questionnaire. J. Pak. Med. Assoc. 2018, 68, 908–913. [Google Scholar] [PubMed]
- Bergmann, C.; Muth, T.; Loerbroks, A. Medical students’ perceptions of stress due to academic studies and its interrelationships with other domains of life: A qualitative study. Med. Educ. Online 2019, 24, 1603526. [Google Scholar] [CrossRef]
- Ruiz Muñoz, N.L.; Illesca Pretty, M.; González Osorio, L. Calidad de vida percibida durante los estudios de posgrado por profesionales egresados. Rev. Cubana Edu. Superior 2020, 39, 1–15. [Google Scholar]
- Barrera Herrera, A.; Neira Cofré, M.; Raipán Gómez, P.; Riquelme Lobos, P.; Escobar, B. Apoyo social percibido y factores sociodemográficos en relación con los síntomas de ansiedad, depresión y estrés en universitarios chilenos, Perceived social support and socio-demographic factors in relation to symptoms of anxiety, depression and stress in Chilean university students. Rev. De Psicopatología Y Psicol. Clínica 2019, 24, 105–115. [Google Scholar]
- Muirhead, V.; Locker, D. Canadian dental students perceptions of stress and social support. Eur. J. Dent. Educ. 2008, 12, 144–148. [Google Scholar] [CrossRef]
- Peker, K.; Bermek, G.; Uysal, O. Factors Related to Sense of Coherence Among Dental Students at Istanbul University. J. Dent. Educ. 2012, 76, 774–782. [Google Scholar] [CrossRef]
- Hou, Y.; Mei, G.; Liu, Y.; Xu, W. Physical Fitness with Regular Lifestyle Is Positively Related to Academic Performance among Chinese Medical and Dental Students. BioMed Res. Int. 2020, 2020, 5602395. [Google Scholar] [CrossRef]
- Smith, C.S.; Carrico, C.K.; Goolsby, S.; Hampton, A.C. An analysis of resilience in dental students using the Resilience Scale for Adults. J. Dent. Educ. 2020, 84, 566–577. [Google Scholar] [CrossRef]
- Muñoz, C.O.; Restrepo, D.; Cardona, D. Evolution of the concept of positive mental health: A systematic review. Rev. Panam. Salud. Publica. 2016, 39, 166–173. [Google Scholar]
- Demirekin, Z.B.; Buyukcavus, M.H. Effect of distance learning on the quality of life, anxiety and stress levels of dental students during the COVID-19 pandemic. BMC Med. Educ. 2022, 22, 309. [Google Scholar] [CrossRef]
- Løset, I.H.; Lægreid, T.; Rodakowska, E. Dental Students’ Experiences during the COVID-19 Pandemic—A Cross-Sectional Study from Norway. Int. J. Environ. Res. Public Health 2022, 19, 3102. [Google Scholar] [CrossRef] [PubMed]
- Klaassen, H.; Ashida, S.; Ms, C.L.C.; Xie, X.J.; Smith, B.M.; Tabrizi, M.; Arsenault, K.; Capin, O.R.; Scully, A.C.; da Mata, C.; et al. COVID-19 pandemic and its impact on dental students: A multi-institutional survey. J. Dent. Educ. 2021, 85, 1280–1286. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | WHOQOL-BREF Dimensions (QOL) | |||
|---|---|---|---|---|
| Physical a | Psychological a | Social Relationships a | Environment a | |
| Age | −0.076 | −0.070 | 0.017 | −0.093 |
| Years of experience as a dentist | −0.013 | −0.050 | −0.043 | −0.098 |
| Daily hours of face-to-face academic schedule | −0.091 | 0.079 | 0.025 | 0.004 |
| Weekly study hours | −0.025 | 0.199 | 0.094 | 0.098 |
| Resting days per week | −0.044 | −0.081 | 0.071 | −0.091 |
| Annual frequency of events of academic training | −0.011 | 0.033 | 0.104 | −0.067 |
| Variables | WHOQOL-BREF Dimensions (QOL) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Physical | Psychological | Social Relationships | Environment | |||||||||
| Me | IQR | p-Value a | Me | IQR | p-Value a | Me | IQR | p-Value a | Me | IQR | p-Value a | |
| Sociodemographics | ||||||||||||
| Sex | ||||||||||||
| Females | 48.2 | 21.4 | 0.663 | 66.7 | 16.7 | 0.219 | 58.3 | 25.0 | 0.702 | 59.4 | 15.6 | 0.094 |
| Males | 50.0 | 18.8 | 60.4 | 21.9 | 54.2 | 35.4 | 53.2 | 24.2 | ||||
| Marital status | ||||||||||||
| Single | 46.4 | 21.4 | 0.735 | 62.5 | 20.8 | 0.128 | 58.3 | 25.0 | 0.767 | 57.8 | 18.0 | 0.866 |
| Single/Cohabitated | 50.0 | 19.6 | 66.7 | 20.8 | 58.3 | 33.3 | 56.3 | 32.8 | ||||
| Separate | 50.0 | --- | 54.2 | --- | 50.0 | --- | 56.3 | --- | ||||
| Socioeconomic status | ||||||||||||
| Low-Middle | 48.2 | 17.9 | 0.630 | 62.5 | 17.7 | 0.068 | 54.2 | 25.0 | 0.233 | 54.7 | 15.6 | 0.025 |
| High | 50.0 | 25.0 | 66.7 | 16.7 | 66.7 | 33.3 | 62.5 | 29.7 | ||||
| Housing | ||||||||||||
| Own | 50.0 | 21.4 | 0.236 | 62.5 | 20.8 | 0.339 | 66.7 | 33.3 | 0.239 | 59.4 | 18.0 | 0.150 |
| Rented | 46.4 | 10.7 | 66.7 | 18.8 | 50.0 | 37.5 | 53.1 | 26.6 | ||||
| Other | 46.4 | 16.1 | 58.3 | 14.6 | 50.0 | 29.2 | 53.1 | 23.4 | ||||
| Vehicle | ||||||||||||
| Yes | 53.6 | 62.5 | 0.041 | 62.5 | 20.8 | 0.215 | 58.3 | 25.0 | 0.757 | 59.4 | 25.0 | 0.028 |
| No | 46.4 | 10.7 | 62.5 | 20.8 | 58.3 | 37.5 | 53.1 | 15.6 | ||||
| Type of Family | ||||||||||||
| Nuclear | 50.0 | 18.8 | 0.068 | 66.7 | 20.8 | 0.264 | 62.5 | 33.3 | 0.024 | 59.4 | 21.9 | 0.011 |
| Assembled | --- | --- | 68.8 | --- | 75.0 | --- | 62.6 | --- | ||||
| Extended | 42.9 | --- | 62.5 | --- | 58.3 | --- | 62.5 | --- | ||||
| Single-parent | 48.2 | 26.8 | 60.4 | 14.6 | 66.7 | 27.1 | 64.1 | 16.4 | ||||
| Live alone | 39.3 | 14.3 | 54.2 | 12.5 | 41.7 | 16.7 | 46.9 | 15.6 | ||||
| Labor conditions | ||||||||||||
| Currently working | ||||||||||||
| No | 46.4 | 21.4 | 0.529 | 66.7 | 16.7 | 0.274 | 66.7 | 33.3 | 0.62 | 56.3 | 15.6 | 0.507 |
| Yes | 50.0 | 19.6 | 62.5 | 20.8 | 58.3 | 25.0 | 59.4 | 21.9 | ||||
| Having several workplaces (n = 49) | ||||||||||||
| No | 48.2 | 24.1 | 0.186 | 62.5 | 25.0 | 0.976 | 54.2 | 31.3 | 0.869 | 59.4 | 24.2 | 0.984 |
| Yes | 50.0 | 12.3 | 62.5 | 16.7 | 58.3 | 25.0 | 59.4 | 20.3 | ||||
| Academic conditions | ||||||||||||
| Postgraduate monthly expenses (COP) | ||||||||||||
| ≤de 3.000.000 (≤USD 750) | 46.4 | 21.4 | 0.449 | 66.7 | 16.7 | 0.196 | 58.3 | 25.0 | 0.992 | 59.4 | 18.8 | 0.139 |
| ≥de 3.000.001 (≥USD 751) | 50.0 | 21.4 | 58.3 | 25.0 | 58.3 | 29.2 | 53.1 | 20.3 | ||||
| Study-leisure balance | ||||||||||||
| Balanced | 57.1 | 21.4 | 0.094 | 66.7 | 20.8 | 0.380 | 91.7 | 25.0 | 0.043 | 68.8 | 12.5 | 0.019 |
| Unbalanced | 46.4 | 19.6 | 62.5 | 18.8 | 58.3 | 25.0 | 56.3 | |||||
| Foreign language proficiency | ||||||||||||
| No | 46.4 | 16.1 | 0.238 | 62.5 | 16.7 | 0.089 | 54.2 | 31.3 | 0.506 | 53.1 | 14.8 | 0.013 |
| Yes | 50.0 | 20.5 | 66.7 | 20.8 | 58.3 | 31.3 | 60.9 | 21.1 | ||||
| Satisfaction with the postgraduate experience | ||||||||||||
| Satisfied | 50.0 | 21.4 | 0.099 | 62.5 | 16.7 | 0.345 | 58.3 | 25.0 | 0.527 | 59.4 | 18.0 | 0.027 |
| Unsatisfied | 42.9 | 12.5 | 54.2 | 25.0 | 58.3 | 25.0 | 48.4 | 20.3 | ||||
| Posgraduate stress level | ||||||||||||
| Non-stressful | 62.5 | 18.8 | 0.037 | 75.0 | 24.0 | 0.156 | 83.3 | 41.7 | 0.105 | 70.3 | 19.5 | 0.039 |
| Stressful | 48.4 | 20.5 | 62.5 | 19.8 | 58.3 | 25.0 | 58.3 | 18.0 | ||||
| Health | ||||||||||||
| Sports practice | ||||||||||||
| Yes | 57.1 | 19.6 | 0.006 | 66.7 | 18.8 | 0.009 | 66.7 | 37.5 | 0.064 | 62.5 | 17.2 | <0.001 |
| No | 46.3 | 14.3 | 62.5 | 20.8 | 50.0 | 33.3 | 53.1 | 15.6 | ||||
| Body Mass Index (BMI) | ||||||||||||
| Underweight | 44.6 | 13.4 | 0.156 | 66.7 | 24.0 | 0.773 | 50.0 | 33.3 | 0.32 | 57.8 | 32.8 | 0.676 |
| Normal | 50.0 | 21.4 | 62.5 | 16.7 | 58.3 | 25.0 | 56.3 | 15.6 | ||||
| Overweight/obesity | 50.0 | 16.1 | 62.5 | 29.2 | 58.3 | 50.0 | 56.3 | 31.3 | ||||
| Self-perceived health | ||||||||||||
| Good | 50.0 | 17.9 | 0.038 | 66.7 | 16.7 | 0.084 | 62.5 | 31.3 | 0.009 | 59.4 | 20.3 | 0.009 |
| Poor | 42.9 | 13.4 | 60.4 | 24.0 | 50.0 | 41.7 | 51.6 | 18.0 | ||||
| Mental health (GHQ-12) | ||||||||||||
| Good | 53.6 | 17.9 | 0.005 | 66.7 | 16.7 | 0.121 | 66.7 | 25.0 | 0.152 | 59.4 | 21.9 | 0.009 |
| Poor | 42.9 | 12.5 | 62.5 | 20.8 | 58.3 | 33.3 | 53.1 | 18.8 | ||||
| Social support (Duke-UNC-11) | ||||||||||||
| Normal | 50.0 | 21.4 | 0.020 | 66.7 | 20.8 | 0.001 | 66.7 | 25.0 | 0.001 | 59.4 | 18.8 | <0.001 |
| Low | 42.9 | 14.3 | 45.8 | 20.8 | 41.7 | 33.3 | 37.5 | 15.6 | ||||
| WHOQOL-BREF Dimensions (QOL) | Variables Included in the Lineal Regression Model | Determination Coefficient (%) | Change of R2% | p-Value Change of R2% | Non-Standardized Regression Coefficient | Standardized Regression Coefficient | p-Value | F-Value | p-Value (Model) | Durbin–Watson Statistic | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Unadjusted | Adjusted | ||||||||||
| Physical | Social support (low) | 12.3 | 10.5 | 12.3 | 0.013 | −14.075 | −0.351 | 0.013 | 6.62 | 0.013 | 2.006 |
| Psychological | Sport practice (Yes) | 56.1 | 52.1 | 6.7 | 0.013 | 13.71 | 0.483 | <0.001 | 14.029 | <0.001 | 1.824 |
| Social support (low) | −15.332 | −0.331 | 0.002 | ||||||||
| Marital status (married/cohabitated) | 8.996 | 0.290 | 0.006 | ||||||||
| BMI (Normal) | 7.741 | 0.263 | 0.013 | ||||||||
| Social Relationships | Sport practice (Yes) | 24.4 | 21.1 | 9.2 | 0.022 | 14.702 | 0.368 | 0.006 | 7.429 | 0.002 | 1.696 |
| Type of family (live alone) | −18.333 | −0.304 | 0.022 | ||||||||
| Environment | Social support (low) | 56.5 | 51.4 | 6.1 | 0.018 | −21.760 | −0.419 | <0.001 | 11.170 | <0.001 | 1.840 |
| Socioeconomic status (Middle-Low) | −10.657 | −0.273 | 0.011 | ||||||||
| Sport practice (Yes) | 9.693 | 0.305 | 0.005 | ||||||||
| Marital status (married/cohabitated) | 9.287 | 0.267 | 0.012 | ||||||||
| Type of family (live alone) | −12.098 | −0.252 | 0.018 | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Trujillo, L.V.; López-Valencia, S.C.; Agudelo-Suárez, A.A. Understanding the Quality of Life and Its Related Factors in Orthodontics Postgraduate Students: A Mixed Methods Approach. Dent. J. 2023, 11, 39. https://doi.org/10.3390/dj11020039
López-Trujillo LV, López-Valencia SC, Agudelo-Suárez AA. Understanding the Quality of Life and Its Related Factors in Orthodontics Postgraduate Students: A Mixed Methods Approach. Dentistry Journal. 2023; 11(2):39. https://doi.org/10.3390/dj11020039
Chicago/Turabian StyleLópez-Trujillo, Laura V., Sara C. López-Valencia, and Andrés A. Agudelo-Suárez. 2023. "Understanding the Quality of Life and Its Related Factors in Orthodontics Postgraduate Students: A Mixed Methods Approach" Dentistry Journal 11, no. 2: 39. https://doi.org/10.3390/dj11020039
APA StyleLópez-Trujillo, L. V., López-Valencia, S. C., & Agudelo-Suárez, A. A. (2023). Understanding the Quality of Life and Its Related Factors in Orthodontics Postgraduate Students: A Mixed Methods Approach. Dentistry Journal, 11(2), 39. https://doi.org/10.3390/dj11020039