
Salivary Scca1, Scca2 and Trop2 in Oral Cancer Patients—A Cross-Sectional Pilot Study

 ,
,  , ,
, ,
Abstract
:
1. Introduction
2. Materials and Methods
- Not eating or drinking at least 8 h before sampling
- Not brushing teeth or using a mouthwash at least 1 h before sampling
- No salivary, jaw and oral mucosal tissue diseases or conditions (apart from gingivitis and periodontitis)
- No history of radiation therapy of the head and neck
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Ma’Aita, J.K. Oral cancer in Jordan: A retrospective study of 118 patients. Croat. Med. J. 2000, 41, 64–69. [Google Scholar] [PubMed]
- Radman, M.; Glavina, A.; Sabol, I.; Mravak-Stipetić, M. Knowledge of Oral Cancer among the Fourth and Fifth Year Dental Students. Acta Stomatol. Croat. 2018, 52, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Shao, Y.; Song, Y.; Xu, S.; Li, S.; Zhou, H. Expression Profile of Circular RNAs in Oral Squamous Cell Carcinoma. Front. Oncol. 2020, 10, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Derakhshan, S.; Poosti, A.; Razavi, A.E.; Moosavi, M.A.; Mahdavi, N.; Naieni, F.B.; Hesari, K.K.; Rahpeima, A. Evaluation of squamous cell carcinoma antigen 1 expression in oral squamous cell carcinoma (tumor cells and peritumoral T-lymphocytes) and verrucous carcinoma and comparison with normal oral mucosa. J. Appl. Oral Sci. 2021, 29, e20210374. [Google Scholar] [CrossRef]
- Shao, T.; Huang, J.; Zheng, Z.; Wu, Q.; Liu, T.; Lv, X. SCCA, TSGF, and the Long Non-Coding RNA AC007271.3 are Effective Biomarkers for Diagnosing Oral Squamous Cell Carcinoma. Cell. Physiol. Biochem. 2018, 47, 26–38. [Google Scholar] [CrossRef]
- Li, S.; Gao, Y.; Yang, B.; Liang, Z.; Wang, Y.; Zhai, D.; Jing, L.; Liu, T.; Wang, F.; Du, Z. Squamous cell carcinoma antigen 1 and 2 mRNA and a new variant expressed in hepatocellular carcinoma. Neoplasma 2014, 61, 718–723. [Google Scholar] [CrossRef] [Green Version]
- Chechlinska, M.; Kowalewska, M.; Brzoska-Wojtowicz, E.; Radziszewski, J.; Ptaszyński, K.; Rys, J.; Kaminska, J.; Nowak, R. Squamous cell carcinoma antigen 1 and 2 expression in cultured normal peripheral blood mononuclear cells and in vulvar squamous cell carcinoma. Tumor Biol. 2010, 31, 559–567. [Google Scholar] [CrossRef] [Green Version]
- Schneider, S.S.; Schick, K.E.; Fish, E.; Miller, J.C.; Pena, D.S.; Treter, S.M.; Hui, G.A.; Silverman, A. A serine proteinase inhibitor locus at 18q21.3 contains a tandem duplication of the human squamous cell carcinoma antigen gene. Proc. Natl. Acad. Sci. USA 1995, 92, 3147–3151. [Google Scholar] [CrossRef] [Green Version]
- Stenman, J.; Hedström, J.; Grénman, R.; Leivo, I.; Finne, P.; Palotie, A.; Orpana, A. Relative levels of SCCA2 and SCCA1 mRNA in primary tumors predicts recurrent disease in squamous cell cancer of the head and neck. Int. J. Cancer 2001, 95, 39–43. [Google Scholar] [CrossRef]
- Guerra, E.N.S.; Rêgo, D.F.; Elias, S.T.; Coletta, R.D.; Mezzomo, L.A.M.; Gozal, D.; Canto, G.D.L. Diagnostic accuracy of serum biomarkers for head and neck cancer: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2016, 101, 93–118. [Google Scholar] [CrossRef] [PubMed]
- Fong, D.; Spizzo, G.; Gostner, J.M.; Gastl, G.; Moser, P.; Krammel, C.; Gerhard, S.; Rasse, M.; Laimer, K. TROP2: A novel prognostic marker in squamous cell carcinoma of the oral cavity. Mod. Pathol. 2008, 21, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.J.; Lu, Z.H.; Wang, G.Q.; Pan, Z.Z.; Zhou, Z.W.; Yun, J.P.; Zhang, M.F.; Wan, D.S. Elevated expressions of MMP7, TROP2, and survivin are associated with survival, disease recurrence, and liver metastasis of colon cancer. Int. J. Color. Dis. 2009, 24, 875–884. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Liu, Y.; Bao, X.; Tian, J.; Liu, Y.; Yang, X. Overexpression of TROP2 Predicts Poor Prognosis of Patients with Cervical Cancer and Promotes the Proliferation and Invasion of Cervical Cancer Cells by Regulating ERK Signaling Pathway. PLoS ONE 2013, 8, e75864. [Google Scholar] [CrossRef]
- Zheng, Z.; Dong, X.-J. Clinical value of serum trophoblast cell surface protein 2 (TROP2) antibody in non-small-cell lung cancer patients. Biomarkers 2016, 21, 739–742. [Google Scholar] [CrossRef]
- Salarić, I.; Karmelić, I.; Lovrić, J.; Baždarić, K.; Rožman, M.; Čvrljević, I.; Zajc, I.; Brajdić, D.; Macan, D. Salivary melatonin in oral squamous cell carcinoma patients. Sci. Rep. 2021, 11, 13201. [Google Scholar] [CrossRef]
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. AJCC Cancer Staging Manual, 8th ed.; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar]
- World Health Oragnization Collaborating Centre for Drug Statistics Methodology. WHOCC-ATC/DDD Index. Available online: https://www.whocc.no/atc_ddd_index/ (accessed on 15 January 2021).
- World Health Oragnization. International Statistical Classification of Diseases and Related Health Problems (ICD-11). Available online: https://www.who.int/classifications/icd/en/ (accessed on 17 December 2020).
- Huang, S.-F.; Wei, F.-C.; Liao, C.-T.; Wang, H.-M.; Lin, C.-Y.; Lo, S.; Huang, J.-J.; Chen, I.-H.; Kang, C.-J.; Chien, H.-T.; et al. Risk Stratification in Oral Cavity Squamous Cell Carcinoma by Preoperative CRP and SCC Antigen Levels. Ann. Surg. Oncol. 2012, 19, 3856–3864. [Google Scholar] [CrossRef]
- Kandiloros, D.; Eleftheriadou, A.; Chalastras, T.; Kyriou, L.; Yiotakis, I.; Ferekidis, E. Prospective Study of a Panel of Tumor Markers as Prognostic Factors in Patients with Squamous Cell Carcinoma of Head and Neck. Med. Oncol. 2006, 23, 463–470. [Google Scholar] [CrossRef]
- Banal, A.; Hacene, K.; Berthelot-Ruff, E.; Mahé, E.; Fontana, X.; Pichon, M.F. Comparison of cyfra 21-1 and SCC assays in head and neck tumours. Tumor Biol. 2001, 22, 27–35. [Google Scholar] [CrossRef]
- Hashimoto, K.-I.; Kiyoshima, T.; Matsuo, K.; Ozeki, S.; Sakai, H. Effect of SCCA1 and SCCA2 on the Suppression of TNF-α-Induced Cell Death by Impeding the Release of Mitochondrial Cytochrome c in an Oral Squamous Cell Carcinoma Cell Line. Tumor Biol. 2005, 26, 165–172. [Google Scholar] [CrossRef]
- Chen, I.-H.; Liao, C.-T.; Wang, H.-M.; Huang, J.-J.; Kang, C.-J.; Huang, S.-F. Using SCC Antigen and CRP Levels as Prognostic Biomarkers in Recurrent Oral Cavity Squamous Cell Carcinoma. PLoS ONE 2014, 9, e103265. [Google Scholar] [CrossRef] [Green Version]
- Lin, W.-H.; Chen, I.-H.; Wei, F.-C.; Huang, J.-J.; Kang, C.-J.; Hsieh, L.-L.; Wang, H.-M.; Huang, S.-F.; Huang, S. Clinical significance of preoperative squamous cell carcinoma antigen in oral-cavity squamous cell carcinoma. Laryngoscope 2011, 121, 971–977. [Google Scholar] [CrossRef] [PubMed]
- Travassos, D.C.; Fernandes, D.; Massucato, E.M.S.; Navarro, C.M.; Bufalino, A. Squamous cell carcinoma antigen as a prognostic marker and its correlation with clinicopathological features in head and neck squamous cell carcinoma: Systematic review and meta-analysis. J. Oral Pathol. Med. 2018, 47, 3–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Catanzaro, J.M.; Guerriero, J.L.; Liu, J.; Ullman, E.; Sheshadri, N.; Chen, J.J.; Zong, W.-X. Elevated Expression of Squamous Cell Carcinoma Antigen (SCCA) Is Associated with Human Breast Carcinoma. PLoS ONE 2011, 6, e19096. [Google Scholar] [CrossRef] [PubMed]
- Collie-Duguid, E.S.R.; Sweeney, K.; Stewart, K.N.; Miller, I.D.; Smyth, E.; Heys, S.D. SerpinB3, a new prognostic tool in breast cancer patients treated with neoadjuvant chemotherapy. Breast Cancer Res. Treat. 2012, 132, 807–818. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Gao, Y.; Yang, B.; Jia, X.; Zhai, D.; Li, S.; Zhang, Q.; Jing, L.; Wang, Y.; Du, Z.; et al. Overexpression of Squamous Cell Carcinoma Antigen 1 Is Associated with the Onset and Progression of Human Hepatocellular Carcinoma. Arch. Med. Res. 2015, 46, 133–141. [Google Scholar] [CrossRef]
- Okawa, T.; Yamaguchi, Y.; Kou, K.; Ono, J.; Azuma, Y.; Komitsu, N.; Inoue, Y.; Kohno, M.; Matsukura, S.; Kambara, T.; et al. Serum levels of squamous cell carcinoma antigens 1 and 2 reflect disease severity and clinical type of atopic dermatitis in adult patients. Allergol. Int. 2018, 67, 124–130. [Google Scholar] [CrossRef]
- Ray, R.; Choi, M.; Zhang, Z.; Silverman, G.A.; Askew, D.; Mukherjee, A.B. Uteroglobin Suppresses SCCA Gene Expression Associated with Allergic Asthma. J. Biol. Chem. 2005, 280, 9761–9764. [Google Scholar] [CrossRef] [Green Version]
- Izuhara, K.; Yamaguchi, Y.; Ohta, S.; Nunomura, S.; Nanri, Y.; Azuma, Y.; Nomura, N.; Noguchi, Y.; Aihara, M. Squamous Cell Carcinoma Antigen 2 (SCCA2, SERPINB4): An Emerging Biomarker for Skin Inflammatory Diseases. Int. J. Mol. Sci. 2018, 19, 1102. [Google Scholar] [CrossRef] [Green Version]
- Cataltepe, S.; Gornstein, E.R.; Schick, C.; Kamachi, Y.; Chatson, K.; Fries, J.; Silverman, G.A.; Upton, M.P. Co-expression of the Squamous Cell Carcinoma Antigens 1 and 2 in Normal Adult Human Tissues and Squamous Cell Carcinomas. J. Histochem. Cytochem. 2000, 48, 113–122. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| OSCC Group (N = 29) | Control Group (N = 29) | Statistics | |
|---|---|---|---|
| Only smoked | 3 (10.34%) | 1 (3.45%) | / |
| Only consumed alcohol | 6 (20.69%) | 0 (0%) | / |
| Consumed alcohol and smoked | 14 (48.28%) | 0 (0%) | / |
| Alcohol altogether | Does not drink: 6 (20.69%) 1 a.u./day: 4 (13.79%) 2–4 a.u./day: 6 (20.69%) >5 a.u./day: 13 (44.83%) | Does not drink: 14 (48.28%) 1 a.u./day: 10 (34.48%) 2–4 a.u./day: 3 (10.34%) >5 a.u./day: 2 (6.90%) | U = 206.00; p = 0.0005 |
| Smoking altogether | Does not smoke: 12 (41.38%) 1–5 cig./day: 5 (17.24%) 6–10 cig./day: 0 (0%) 11–20 cig./day: 3 (10.34%) 21–35 cig./day: 8 (27.59%) >36 cig./day: 1 (3.45%) | Does not smoke: 13 (44.83%) 1–5 cig./day: 4 (13.79%) 6–10 cig./day: 6 (20.69%) 11–20 cig./day: 6 (20.69%) 21–35 cig./day: 0 (0%) >36 cig./day: 0 (0%) | U = 349.00; p = 0.244 |
| No risk habits | 9 (31.03%) | 13 (44.83%) | / |
| Systemic Condition or Disease (ICD-11) | OSCC Group (N) | Control Group (N) | Total (N) | Drug (ATC) | OSCC Group (N) | Control Group (N) | Total (N) |
|---|---|---|---|---|---|---|---|
| Healthy/no systemic conditions | / | 18 | 18 | Do not take any medication | 9 | 18 | 27 |
| Hypertension (I10) | 12 | 9 | 19 | Calcium inhibitors (C08) | 4 | 2 | 6 |
| Anxiety (MB24.3) | 7 | 2 | 9 | Proton pump inhibitors (A02BC) | 5 | 0 | 5 |
| Type 2 diabetes mellitus (E11) | 2 | 0 | 0 | Acetylsalicylic acid (B01AC30) | 3 | 1 | 4 |
| Atherosclerosis (I70) | 6 | 2 | 8 | Angiotensin II receptor blockers, plain (C09CA) | 2 | 0 | 2 |
| Chronic kidney disease (GB61) | 1 | 0 | 1 | Benzodiazepine derivatives (N05CD) | 8 | 2 | 10 |
| Hyperlipidaemia (5C80Z) | 7 | 6 | 13 | Antidepressants (N06A) | 3 | 1 | 4 |
| Alcohol-induced psychotic disorder (6C40.6) | 1 | 0 | 1 | Alpha-adrenoreceptor antagonists (C02CA) | 5 | 2 | 7 |
| Osteoporosis (M81) | 1 | 0 | 1 | Vitamin D and analougs (A11CC) | 1 | 3 | 4 |
| Depression (F32) | 3 | 1 | 4 | Beta blocking agents, selective (C07AB) | 10 | 1 | 11 |
| Prostatic hypertrophy (GA90) | 4 | 2 | 6 | Selective beta-2-adrenoreceptor agonists (R03AC) | 1 | 0 | 1 |
| Asthma (J45) | 1 | 0 | 1 | ACE inhibitors, plain (C09AA) | 8 | 4 | 12 |
| Gastro-oesophageal reflux disease (DA22) | 6 | 0 | 6 | H2-receptor antagonists (A02BA) | 5 | 0 | 5 |
| Insomnia (7A00) | 2 | 0 | 2 | HMG CoA reductase inhibitors (C10AA) | 7 | 6 | 13 |
| Blood glucose lowering drugs, excl. insulins (A10B) | 2 | 0 | 2 | ||||
| Bisphosphonates (M05BA) | 1 | 0 | 1 |
| SCCA1 | SCCA2 | |||||||
|---|---|---|---|---|---|---|---|---|
| OSCC Group (N = 29) | Control Group (N = 29) | OSCC Group (N = 29) | Control Group (N = 29) | OSCC Group (N = 29) | Control Group (N = 29) | OSCC Group (N = 29) | Control Group (N = 29) | |
| UWS | SWS | UWS | SWS | |||||
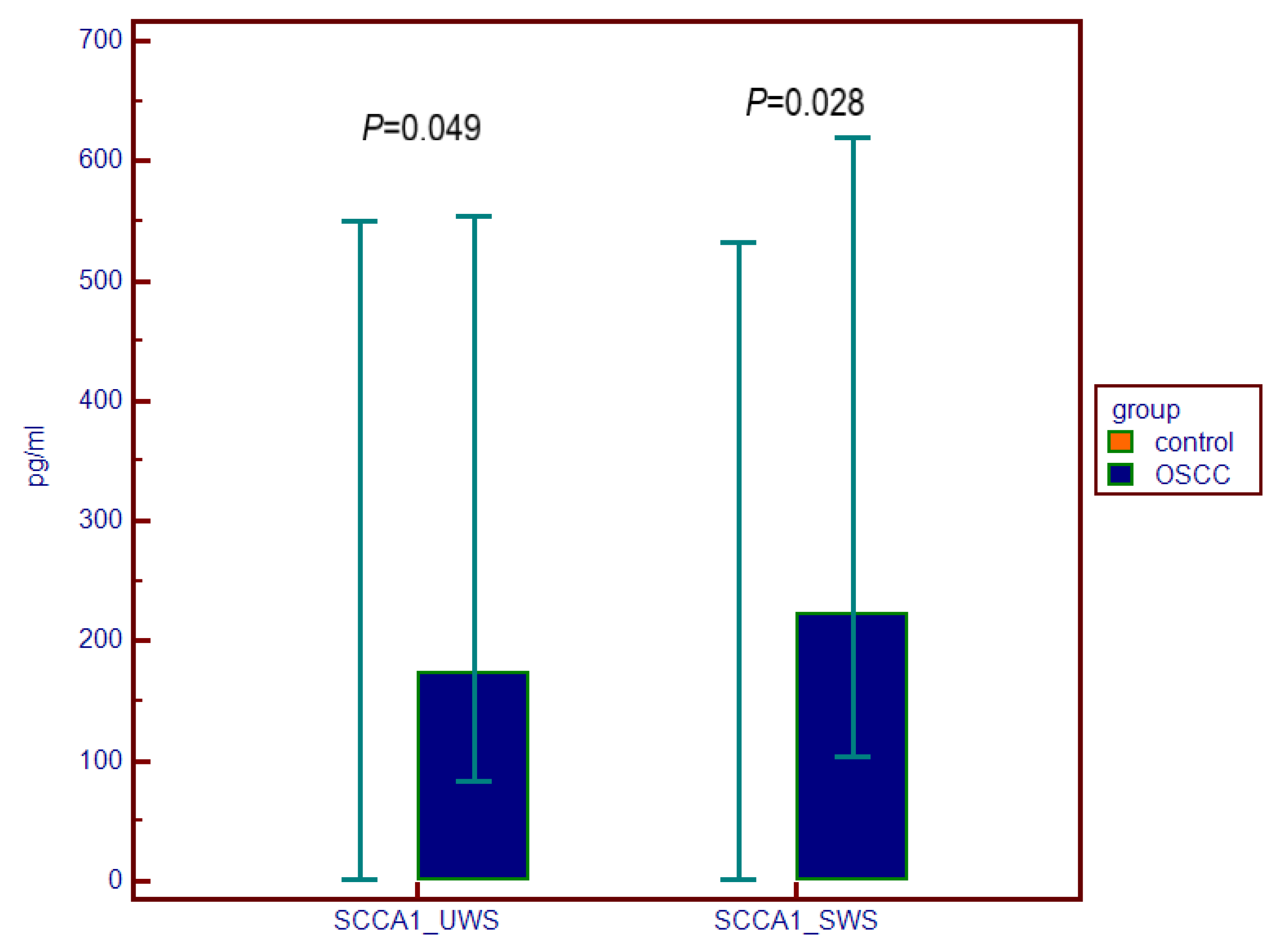
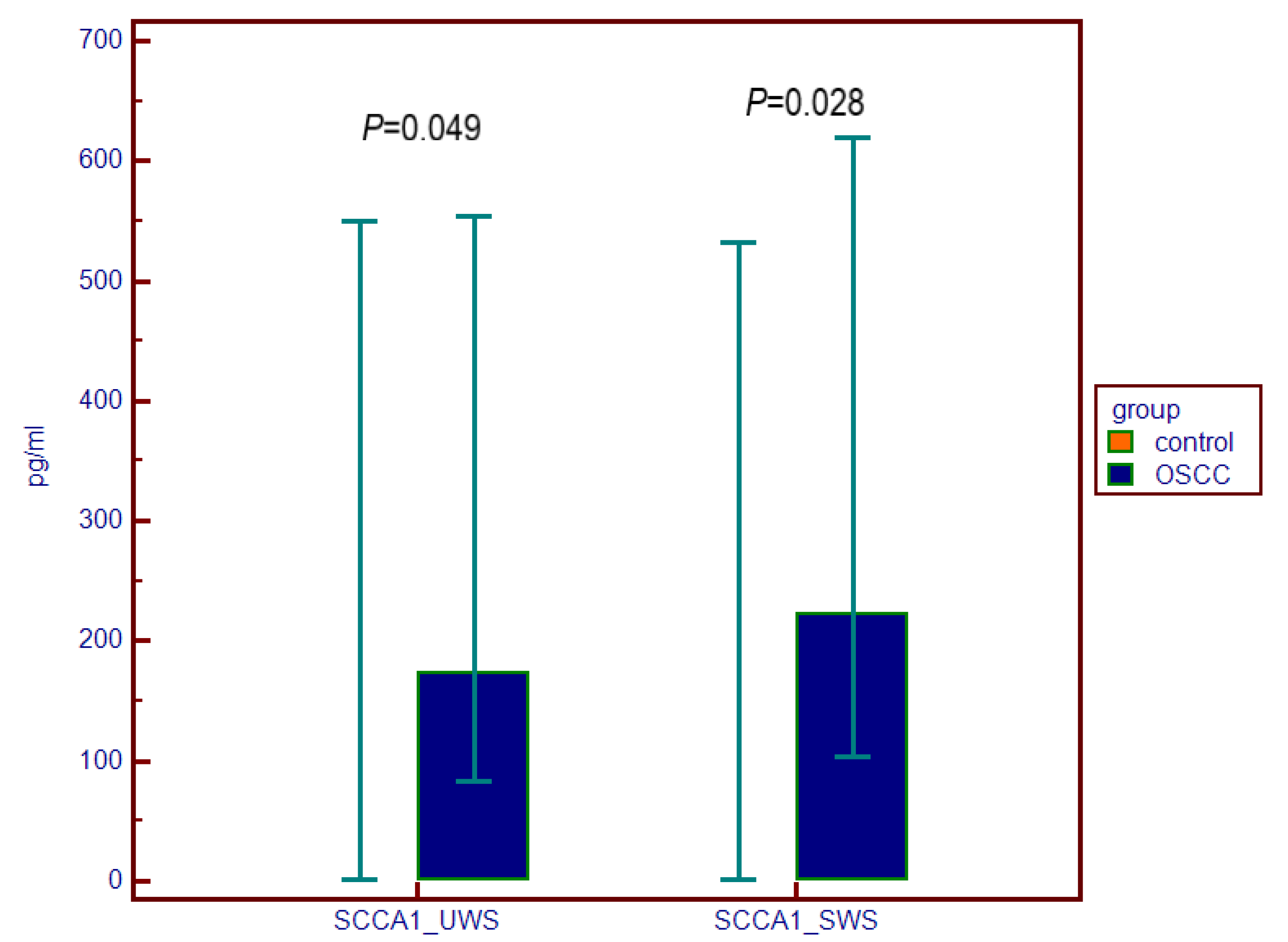
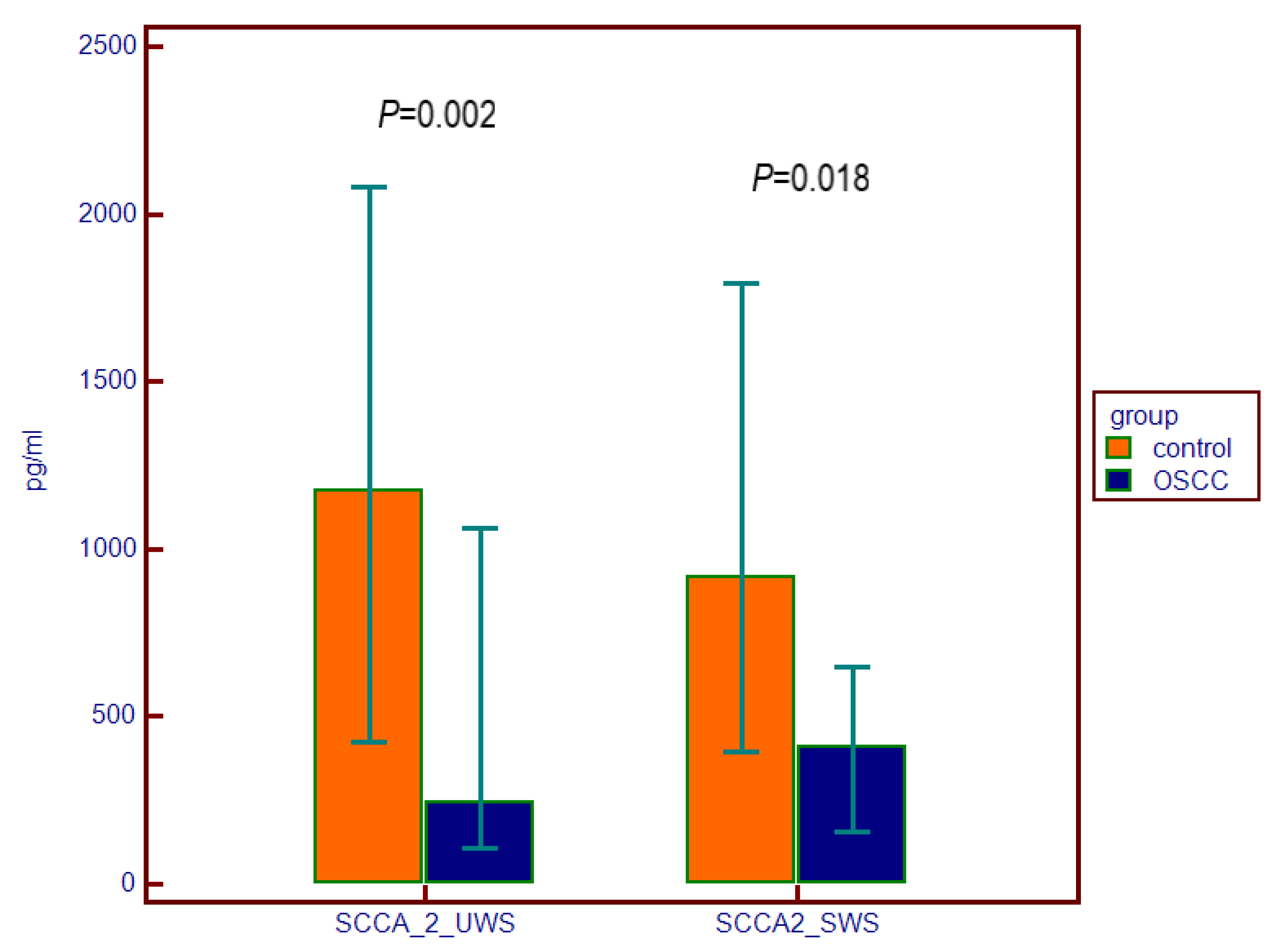
| Minimal value (pg/mL) | 46.47 | 2.00 | 47.84 | 2.00 | 13.51 | 89.23 | 17.86 | 12.25 |
| Maximal value (pg/mL) | 1769.36 | 2497.71 | 1257.25 | 2427.18 | 11,000.00 | 3245.41 | 2623.32 | 11,000.00 |
| Median (95% CI) | 173.06 (99.77–471.14) | 2.00 (2.00–321.47) | 222.79 (111.23–564.69) | 2.00 (2.00–207.46) | 241.46 (165.79–530.08) | 1174.04 (596.67–1922.95 | 408.40 (201.32–593.50 | 915.29 (505.01–1736.08) |
| Interquartile range | 82.98–554.12 | 2.00–550.38 | 103.64–619.18 | 2.00–531.87 | 105.27–1063.51 | 425.63–2082.20 | 156.40–646.14 | 396.58–1794.07 |
| Statistics | U = 295.00 | p = 0.049 | U = 280.00 | p = 0.028 | U = 222.00 | p = 0.002 | U = 268.50 | p = 0.018 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karmelić, I.; Salarić, I.; Baždarić, K.; Rožman, M.; Zajc, I.; Mravak-Stipetić, M.; Bago, I.; Brajdić, D.; Lovrić, J.; Macan, D. Salivary Scca1, Scca2 and Trop2 in Oral Cancer Patients—A Cross-Sectional Pilot Study. Dent. J. 2022, 10, 70. https://doi.org/10.3390/dj10040070
Karmelić I, Salarić I, Baždarić K, Rožman M, Zajc I, Mravak-Stipetić M, Bago I, Brajdić D, Lovrić J, Macan D. Salivary Scca1, Scca2 and Trop2 in Oral Cancer Patients—A Cross-Sectional Pilot Study. Dentistry Journal. 2022; 10(4):70. https://doi.org/10.3390/dj10040070
Chicago/Turabian StyleKarmelić, Ivana, Ivan Salarić, Ksenija Baždarić, Marko Rožman, Ivan Zajc, Marinka Mravak-Stipetić, Ivona Bago, Davor Brajdić, Jasna Lovrić, and Darko Macan. 2022. "Salivary Scca1, Scca2 and Trop2 in Oral Cancer Patients—A Cross-Sectional Pilot Study" Dentistry Journal 10, no. 4: 70. https://doi.org/10.3390/dj10040070
APA StyleKarmelić, I., Salarić, I., Baždarić, K., Rožman, M., Zajc, I., Mravak-Stipetić, M., Bago, I., Brajdić, D., Lovrić, J., & Macan, D. (2022). Salivary Scca1, Scca2 and Trop2 in Oral Cancer Patients—A Cross-Sectional Pilot Study. Dentistry Journal, 10(4), 70. https://doi.org/10.3390/dj10040070