
Laser Treatment of Peri-Implantitis: A Systematic Review of Radiographic Outcomes

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Focus Question
2.2. Literature Search and Study Design
2.3. Inclusion Criteria
- Patients diagnosed with peri-implantitis, reported as inflamed peri-implant pockets 4 mm or more in depth and/or loss of supporting peri-implant bone, were included.
- Clinical studies with high-intensity laser therapy of peri-implant defects were included. High intensity laser usage that results in ablation and removal of gingival crevicular epithelium were categorized as surgical treatments.
- Studies with sufficient radiographic data for at least five patients were included.
- Clinical trials reporting radiographic effects of laser treatment on human peri-implant diseased periodontium were included.
- Non-English articles were included, but were selected for full-text analysis only if an English translation were available.
2.4. Exclusion Criteria
- All in vitro, cadaver, and animal studies were excluded.
- Photodynamic therapy studies were excluded.
- Non-surgical studies with low-intensity laser therapy that do not result in ablation or removal of gingival epithelium were excluded.
- Conference abstracts and posters were excluded.
2.5. Screening, Selection, and Data Extraction
2.6. Risk of Bias Assessment
3. Results
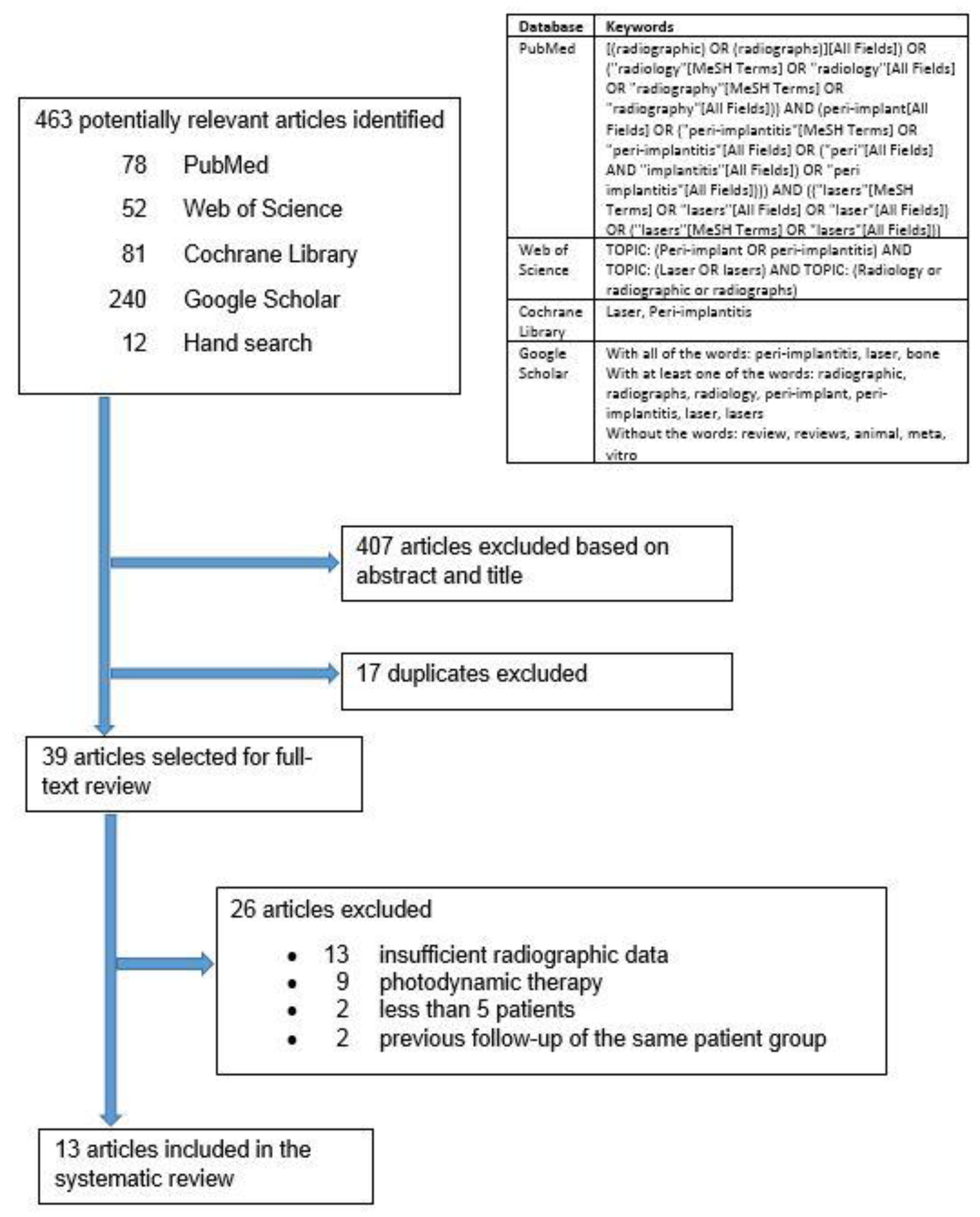
3.1. Search Results
3.2. Quality of Evidence
3.3. Study Characteristics
3.4. Primary Outcomes
- For the five Er:YAG laser studies, two reported RBL gain [27,31] compared to baseline but did not analyze the statistical significance of the change. One study [32] showed RBL loss compared to baseline and less RBL loss compared to control; the statistical significance of both results was not analyzed. Another reported RBL loss compared to baseline and control that was not significant [22]. One investigation reported no significant RBL change compared to either baseline or control [19]. Another study [33] reported RBL gain compared to control that was not significant, and RBL gain compared to baseline without analyzing the significance.
3.5. Secondary Outcomes
4. Discussion
4.1. Recommendations for Laser Treatment Protocols
4.2. Recommendations for Future Studies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Albrektsson, T.; Isidor, F. Consensus Report of Session IV. In Proceedings of the 1st European Workshop on Periodontology, Charter House of Ittingen, Thurgau, Switzerland, 1–4 February 1993; Lang, N.P., Karring, T., Eds.; Quintessence: London, UK, 1994; pp. 365–369, ISBN 1-85097-035-1. [Google Scholar]
- Lindhe, J.; Meyle, J.; Group D of European Workshop on Periodontology. Peri-Implant Diseases: Consensus Report of the Sixth European Workshop on Periodontology. J. Clin. Periodontol. 2008, 35, 282–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heitz-Mayfield, L.J.A.; Salvi, G.E. Peri-Implant Mucositis. J. Periodontol. 2018, 89, S257–S266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zitzmann, N.U.; Berglundh, T. Definition and Prevalence of Peri-Implant Diseases. J. Clin. Periodontol. 2008, 35, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Derks, J.; Monje, A.; Wang, H.L. Peri-Implantitis. J. Periodontol. 2018, 89, S267–S290. [Google Scholar] [CrossRef]
- Derks, J.; Tomasi, C. Peri-Implant Health and Disease. A Systematic Review of Current Epidemiology. J. Clin. Periodontol. 2015, 42, S158–S171. [Google Scholar] [CrossRef]
- Ting, M.; Craig, J.; Balkin, B.E.; Suzuki, J.B. Peri-Implantitis: A Comprehensive Overview of Systematic Reviews. J. Oral Implantol. 2018, 44, 225–247. [Google Scholar] [CrossRef]
- Romanos, G.E.; Javed, F.; Delgado-Ruiz, R.A.; Calvo-Guirado, J.L. Peri-Implant Diseases: A Review of Treatment Interventions. Dent. Clin. N. Am. 2015, 59, 157–178. [Google Scholar] [CrossRef]
- Renvert, S.; Roos-Jansåker, A.M.; Claffey, N. Non-Surgical Treatment of Peri-Implant Mucositis and Peri-Implantitis: A Literature Review. J. Clin. Periodontol. 2008, 35, 305–315. [Google Scholar] [CrossRef]
- Claffey, N.; Clarke, E.; Polyzois, I.; Renvert, S. Surgical Treatment of Peri-Implantitis. J. Clin. Periodontol. 2008, 35, 316–332. [Google Scholar] [CrossRef]
- Schou, S.; Holmstrup, P.; Jørgensen, T.; Skovgaard, L.T.; Stoltze, K.; Hjorting-Hansen, E.; Wenzel, A. Anorganic Porous Bovine-Derived Bone Mineral (Bio-Oss) and ePTFE Membrane in the Treatment of Peri-Implantitis in Cynomolgus Monkeys. Clin. Oral Implant. Res. 2003, 14, 535–547. [Google Scholar] [CrossRef]
- Mizutani, K.; Aoki, A.; Coluzzi, D.; Yukna, R.; Wang, C.Y.; Pavlic, V.; Izumi, Y. Lasers in Minimally Invasive Periodontal and Peri-Implant Therapy. Periodontology 2000 2016, 71, 185–212. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, I.; Aoki, A.; Takasaki, A.A.; Mizutani, K.; Sasaki, K.M.; Izumi, Y. Application of Lasers in Periodontics: True Innovation or Myth? Periodontology 2000 2009, 50, 90–126. [Google Scholar] [CrossRef] [PubMed]
- Romanos, G.E.; Nentwig, G.H. Regenerative Therapy of Deep Peri-Implant Infrabony Defects After CO2 Laser Implant Surface Decontamination. Int. J. Periodontics Restor. Dent. 2008, 28, 245–255. [Google Scholar]
- Romanos, G.E.; Everts, H.; Nentwig, G.H. Effects of Diode and Nd:YAG Laser Irradiation on Titanium Discs: A Scanning Electron Microscope Examination. J. Periodontol. 2000, 71, 810–815. [Google Scholar] [CrossRef] [PubMed]
- Giannini, R.; Vassalli, M.; Chellini, F.; Polidori, L.; Dei, R.; Giannelli, M. Neodymium:Yttrium Aluminum Garnet Laser Irradiation with Low Pulse Energy: A Potential Tool for the Treatment of Peri-Implant Disease. Clin. Oral Implant. Res. 2006, 17, 638–643. [Google Scholar] [CrossRef]
- Kreisler, M.; Götz, H.; Duschner, H.; d’Hoedt, B. Effect of Nd:YAG, Ho:YAG, Er:YAG, CO2, and GaAIAs Laser Irradiation on Surface Properties of Endosseous Dental Implants. Int. J. Oral Maxillofac. Implant. 2002, 17, 202–211. [Google Scholar]
- Schwarz, F.; Bieling, K.; Nuesry, E.; Sculean, A.; Becker, J. Clinical and Histological Healing Pattern of Peri-Implantitis Lesions Following Non-Surgical Treatment with an Er:YAG Laser. Lasers Surg. Med. 2006, 38, 663–671. [Google Scholar] [CrossRef]
- Schwarz, F.; Bieling, K.; Bonsmann, M.; Latz, T.; Becker, J. Nonsurgical Treatment of Moderate and Advanced Periimplantitis Lesions: A Controlled Clinical Study. Clin. Oral Investig. 2006, 10, 279–288. [Google Scholar] [CrossRef]
- Schwarz, F.; Sahm, N.; Iglhaut, G.; Becker, J. Impact of the Method of Surface Debridement and Decontamination on the Clinical Outcome Following Combined Surgical Therapy of Peri-Implantitis: A Randomized Controlled Clinical Study. J. Clin. Periodontol. 2011, 38, 276–284. [Google Scholar] [CrossRef]
- Persson, G.R.; Roos-Jansåker, A.M.; Lindahl, C.; Renvert, S. Microbiologic Results After Non-Surgical Erbium-Doped:Yttrium, Aluminum, and Garnet Laser or Air-Abrasive Treatment of Peri-Implantitis: A Randomized Clinical Trial. J. Periodontol. 2011, 82, 1267–1278. [Google Scholar] [CrossRef]
- Renvert, S.; Lindahl, C.; Roos Jansåker, A.M.; Persson, G.R. Treatment of Peri-Implantitis Using an Er:YAG Laser or an Air-Abrasive Device: A Randomized Clinical Trial. J. Clin. Periodontol. 2011, 38, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Rooney, A.A.; Boyles, A.L.; Wolfe, M.S.; Bucher, J.R.; Thayer, K.A. Systematic Review and Evidence Integration for Literature-Based Environmental Health Science Assessments. Environ. Health Perspect. 2014, 122, 711–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abduljabbar, T.; Javed, F.; Kellesarian, S.V.; Vohra, F.; Romanos, G.E. Effect of Nd:YAG Laser-Assisted Non-Surgical Mechanical Debridement on Clinical and Radiographic Peri-Implant Inflammatory Parameters in Patients with Peri-Implant Disease. J. Photochem. Photobiol. B 2017, 168, 16–19. [Google Scholar] [CrossRef] [PubMed]
- Arısan, V.; Karabuda, Z.C.; Arıcı, S.V.; Topçuoğlu, N.; Külekçi, G. A Randomized Clinical Trial of an Adjunct Diode Laser Application for the Nonsurgical Treatment of Peri-Implantitis. Photomed. Laser Surg. 2015, 33, 547–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bach, G. Integration of Diode Laser Surface Decontamination in Periimplantitis Therapy—A Twelve Year Review of a Fit for Practice Concept. Laser 2009, 1, 20–24. [Google Scholar]
- Clem, D.; Gunsolley, J.C. Peri-Implantitis Treatment Using Er:YAG Laser and Bone Grafting. A Prospective Consecutive Case Series Evaluation: 1 Year Posttherapy. Int. J. Periodontics Restor. Dent. 2019, 39, 479–489. [Google Scholar] [CrossRef] [PubMed]
- Deppe, H.; Horch, H.H.; Greim, H.; Brill, T.; Wagenpfeil, S.; Donath, K. Peri-Implant Care with the CO2 Laser: In Vitro and In Vivo Results. Med. Laser Appl. 2005, 20, 61–70. [Google Scholar] [CrossRef]
- Deppe, H.; Horch, H.H.; Neff, A. Conventional Versus CO2 Laser-Assisted Treatment of Peri-Implant Defects with the Concomitant Use of Pure-Phase Beta-Tricalcium Phosphate: A 5-Year Clinical Report. Int. J. Oral Maxillofac. Implant. 2007, 22, 79–86. [Google Scholar]
- Nicholson, D.; Blodgett, K.; Braga, C.; Finkbeiner, L.; Fourrier, J.; George, J.; Gregg, R., II; Honigman, A.; Houser, B.; Lamas, W.; et al. Pulsed Nd:YAG Laser Treatment for Failing Dental Implants Due to Peri-Implantitis. In Lasers in Dentistry XX; Rechmann, P., Fried, D., Eds.; Proc. SPIE 8929; Society of Photo-Optical Instrumentation Engineers: Bellingham, WA, USA, 2014; p. 89290H. [Google Scholar] [CrossRef]
- Norton, M.R. Efficacy of Er:YAG Laser in the Decontamination of Peri-Implant Disease: A One-Year Prospective Closed Cohort Study. Int. J. Periodontics Restor. Dent. 2017, 37, 781–788. [Google Scholar] [CrossRef] [Green Version]
- Peng, T.; Tomov, G. The Use of the Lite Touch Er:YAG Laser in Peri-Implantitis Treatment. Laser 2012, 4, 22–28. [Google Scholar]
- Wang, C.W.; Ashnagar, S.; Gianfilippo, R.D.; Arnett, M.; Kinney, J.; Wang, H.L. Laser-Assisted Regenerative Surgical Therapy for Peri-Implantitis: A Randomized Controlled Clinical Trial. J. Periodontol. 2021, 92, 378–388. [Google Scholar] [CrossRef] [PubMed]
- Al-Falaki, R.; Cronshaw, M.; Hughes, F.J. Treatment Outcome Following Use of the Erbium, Chromium:Yttrium, Scandium, Gallium, Garnet Laser in the Non-Surgical Management of Peri-Implantitis: A Case Series. Br. Dent. J. 2014, 217, 453–457. [Google Scholar] [CrossRef] [PubMed]
- Bach, G.; Neckel, C.; Mall, C.; Krekeler, G. Conventional Versus Laser-Assisted Therapy of Periimplantitis: A Five-Year Comparative Study. Implant. Dent. 2000, 9, 247–251. [Google Scholar] [CrossRef] [PubMed]
- Bach, G.; Neckel, C.P. A 5-Year Comparative Study on Conventional and Laser Assisted Therapy of Periimplantitis and Periodontitis. In Lasers in Dentistry VI; Featherstone, J.D.B., Rechmann, P., Fried, D., Eds.; Proc. SPIE 3910; Society of Photo-Optical Instrumentation Engineers: Bellingham, WA, USA, 2000; pp. 12–17. [Google Scholar] [CrossRef]
- Schwarz, F.; Herten, M.; Sager, M.; Bieling, K.; Sculean, A.; Becker, J. Comparison of Naturally Occurring and Ligature-Induced Peri-Implantitis Bone Defects in Humans and Dogs. Clin. Oral Implant. Res. 2007, 18, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Hegewald, A.; John, G.; Sahm, N.; Becker, J. Four-Year Follow-Up of Combined Surgical Therapy of Advanced Peri-Implantitis Evaluating Two Methods of Surface Decontamination. J. Clin. Periodontol. 2013, 40, 962–967. [Google Scholar] [CrossRef]
- Schwarz, F.; John, G.; Schmucker, A.; Sahm, N.; Becker, J. Combined Surgical Therapy of Advanced Peri-Implantitis Evaluating Two Methods of Surface Decontamination: A 7-Year Follow-Up Observation. J. Clin. Periodontol. 2017, 44, 337–342. [Google Scholar] [CrossRef]
- Papadopoulos, C.A.; Vouros, I.; Menexes, G.; Konstantinidis, A. The Utilization of a Diode Laser in the Surgical Treatment of Peri-Implantitis. A Randomized Clinical Trial. Clin. Oral Investig. 2015, 19, 1851–1860. [Google Scholar] [CrossRef]
- Schwarz, F.; Sahm, N.; Schwarz, K.; Becker, J. Impact of Defect Configuration on the Clinical Outcome Following Surgical Regenerative Therapy of Peri-Implantitis. J. Clin. Periodontol. 2010, 37, 449–455. [Google Scholar] [CrossRef]
- Schwarz, F.; Sculean, A.; Rothamel, D.; Schwenzer, K.; Georg, T.; Becker, J. Clinical Evaluation of an Er:YAG Laser for Nonsurgical Treatment of Peri-Implantitis: A Pilot Study. Clin. Oral Implant. Res. 2005, 16, 44–52. [Google Scholar] [CrossRef]
- Schwarz, F.; John, G.; Mainusch, S.; Sahm, N.; Becker, J. Combined Surgical Therapy of Peri-Implantitis Evaluating Two Methods of Surface Debridement and Decontamination. A Two-Year Clinical Follow Up Report. J. Clin. Periodontol. 2012, 39, 789–797. [Google Scholar] [CrossRef]
- Maiorana, C.; Salina, S.; Santoro, F. Treatment of Periimplantitis with Diode Laser: A Clinical Report. J. Oral Laser Appl. 2002, 2, 121–127. [Google Scholar]
- Bassetti, M.; Schar, D.; Wicki, B.; Eick, S.; Ramseier, C.A.; Arweiler, N.B.; Sculean, A.; Salvi, G.E. Anti-Infective Therapy of Peri-Implantitis with Adjunctive Local Drug Delivery or Photodynamic Therapy: 12-Month Outcomes of a Randomized Controlled Clinical Trial. Clin. Oral Implant. Res. 2014, 25, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Bombeccari, G.P.; Guzzi, G.; Gualini, F.; Gualini, S.; Santoro, F.; Spadari, F. Photodynamic Therapy to Treat Periimplantitis. Implant. Dent. 2013, 22, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Caccianiga, G.; Rey, G.; Baldoni, M.; Paiusco, A. Clinical, Radiographic and Microbiological Evaluation of High Level Laser Therapy, a New Photodynamic Therapy Protocol, in Peri-Implantitis Treatment; A Pilot Experience. Biomed. Res. Int. 2016, 2016, 6321906. [Google Scholar] [CrossRef] [Green Version]
- Deppe, H.; Mucke, T.; Wagenpfeil, S.; Kesting, M.; Sculean, A. Nonsurgical Antimicrobial Photodynamic Therapy in Moderate vs. Severe Peri-Implant Defects: A Clinical Pilot Study. Quintessence Int. 2013, 44, 609–618. [Google Scholar] [CrossRef]
- Dörtbudak, O.; Haas, R.; Bernhart, T.; Mailath-Pokorny, G. Lethal Photosensitization for Decontamination of Implant Surfaces in the Treatment of Peri-Implantitis. Clin. Oral Implant. Res. 2001, 12, 104–108. [Google Scholar] [CrossRef] [Green Version]
- Haas, R.; Baron, M.; Dörtbudak, O.; Watzek, G. Lethal Photosensitization, Autogenous Bone, and e-PTFE Membrane for the Treatment of Peri-Implantitis: Preliminary Results. Int. J. Oral Maxillofac. Implant. 2000, 15, 374–382. [Google Scholar]
- Poli, P.P.; Souza, F.A.; Ferrario, S.; Maiorana, C. Adjunctive Application of Antimicrobial Photodynamic Therapy in the Prevention of Medication-Related Osteonecrosis of the Jaw Following Dentoalveolar Surgery: A Case Series. Photodiagnosis Photodyn 2019, 27, 117–123. [Google Scholar] [CrossRef]
- Wang, H.; Li, W.; Zhang, D.; Li, W.; Wang, Z. Adjunctive Photodynamic Therapy Improves the Outcomes of Peri-Implantitis: A Randomized Controlled Trial. Aust. Dent. J. 2019, 64, 256–262. [Google Scholar] [CrossRef]
- Leretter, M.; Cândea, A.; Topala, F. Photodynamic Therapy in Peri-Implantitis. In Proceedings of the Fifth International Conference on Lasers in Medicine: Biotechnologies Integrated in Daily Medicine, Timisoara, Romania, 19–21 September 2013. [Google Scholar] [CrossRef]
- Roncati, M.; Lucchese, A.; Carinci, F. Non-Surgical Treatment of Peri-Implantitis with the Adjunctive Use of an 810-nm Diode Laser. J. Indian Soc. Periodontol. 2013, 17, 812–815. [Google Scholar] [CrossRef]
- Soldatos, N.; Romanos, G.E.; Michaiel, M.; Sajadi, A.; Angelov, N.; Weltman, R. Management of Retrograde Peri-Implantitis Using an Air-Abrasive Device, Er, Cr: YSGG Laser, and Guided Bone Regeneration. Case Rep. Dent. 2018, 2018, 7283240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.-W. Laser-Assisted Regenerative Surgical Therapy for Peri-Implantitis. U.S. National Library of Medicine. Available online: https://clinicaltrials.gov/ct2/show/NCT03127228 (accessed on 5 December 2021).
- Buser, D.; Weber, H.P.; Lang, N.P. Tissue Integration of Non-Submerged Implants. 1-Year Results of a Prospective Study with 100 ITI Hollow-Cylinder and Hollow-Screw Implants. Clin. Oral Implant. Res. 1990, 1, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Mellonig, J.T.; Bowers, G.M. Regenerating Bone in Clinical Periodontics. J. Am. Dent. Assoc. 1990, 121, 497–502. [Google Scholar] [CrossRef]
- Nevins, M.L.; Camelo, M.; Lynch, S.E.; Schenk, R.K.; Nevins, M. Evaluation of Periodontal Regeneration Following Grafting Intrabony Defects with Bio-Oss Collagen: A Human Histologic Report. Int. J. Periodontics Restor. Dent. 2003, 23, 9–17. [Google Scholar]
- Yukna, R.A.; Carr, R.L.; Evans, G.H. Histologic Evaluation of an Nd:YAG Laser-Assisted New Attachment Procedure in Humans. Int. J. Periodontics Restor. Dent. 2007, 27, 577–587. [Google Scholar]
- Schwarz, F.; Jepsen, S.; Herten, M.; Sager, M.; Rothamel, D.; Becker, J. Influence of Different Treatment Approaches on Non-Submerged and Submerged Healing of Ligature Induced Peri-Implantitis Lesions: An Experimental Study in Dogs. J. Clin. Periodontol. 2006, 33, 584–595. [Google Scholar] [CrossRef]
- Nevins, M.; Nevins, M.L.; Yamamoto, A.; Yoshino, T.; Ono, Y.; Wang, C.W.; Kim, D.M. Use of Er:YAG Laser to Decontaminate Infected Dental Implant Surface in Preparation for Reestablishment of Bone-to-Implant Contact. Int. J. Periodontics Restor. Dent. 2014, 34, 461–466. [Google Scholar] [CrossRef] [Green Version]
- Lin, G.H.; Suárez López Del Amo, F.; Wang, H.L. Laser Therapy for Treatment of Peri-Implant Mucositis and Peri-Implantitis: An American Academy of Periodontology Best Evidence Review. J. Periodontol. 2018, 89, 766–782. [Google Scholar] [CrossRef]
- Hausmann, E. Radiographic and Digital Imaging in Periodontal Practice. J. Periodontol. 2000, 71, 497–503. [Google Scholar] [CrossRef]
- Nackaerts, O.; Jacobs, R.; Horner, K.; Zhao, F.; Lindh, C.; Karayianni, K.; van der Stelt, P.; Pavitt, S.; Devlin, H. Bone Density Measurements in Intra-Oral Radiographs. Clin. Oral. Investig. 2007, 11, 225–229. [Google Scholar] [CrossRef]
- Park, H.S.; Lee, Y.J.; Jeong, S.H.; Kwon, T.G. Density of the Alveolar and Basal Bones of the Maxilla and the Mandible. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Wang, W.; Xin, H.; Zang, S.; Zhang, Z.; Wu, Y. The Remodeling of Alveolar Bone Supporting the Mandibular First Molar with Different Levels of Periodontal Attachment. Med. Biol. Eng. Comput. 2013, 51, 991–997. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Bieling, K.; Latz, T.; Nuesry, E.; Becker, J. Healing of Intrabony Peri-Implantitis Defects Following Application of a Nanocrystalline Hydroxyapatite (Ostim) or a Bovine-Derived Xenograft (Bio-Oss) in Combination with a Collagen Membrane (Bio-Gide). A Case Series. J. Clin. Periodontol. 2006, 33, 491–499. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| OHAT Domain and Questions | Abduljabbar et al., 2017 [24] | Arısan et al., 2015 [25] | Bach 2009 [26] | Clem and Gunsolley 2019 [27] | Deppe et al., 2005 [28] | Deppe et al., 2007 [29] | Nicholson et al., 2014 [30] | Norton 2017 [31] | Peng and Tomov 2012 [32] | Renvert et al., 2011 [22] | Romanos et al., 2008 [14] | Schwarz et al., 2006 [19] | Wang et al., 2020 [33] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Selection Bias | |||||||||||||
| 1. Was administered dose or exposure duration level adequately randomized? | ++ | ++ | N/A | N/A | N/A | N/A | N/A | N/A | ++ | ++ | N/A | ++ | ++ |
| 2. Was allocation to study groups adequately concealed? | + | NR | N/A | N/A | N/A | N/A | N/A | N/A | NR | ++ | N/A | NR | ++ |
| 3. Did the selection of study participants result in appropriate comparison groups? | N/A | N/A | + | + | NR | NR | + | NR | N/A | N/A | + | N/A | N/A |
| Confounding Bias | |||||||||||||
| 4. Did the study design or analysis account for important confounding and modifying variables? | N/A | N/A | NR | NR | NR | NR | NR | + | N/A | N/A | NR | N/A | N/A |
| Performance Bias | |||||||||||||
| 5. Were the research personnel and human subjects blinded to the study group during the study? | + | NR | N/A | N/A | N/A | N/A | N/A | N/A | NR | ++ | N/A | NR | ++ |
| Attrition/Exclusion Bias | |||||||||||||
| 6. Were outcome data complete without attrition or exclusion from the analysis? | ++ | ++ | ++ | ++ | − | − | + | + | ++ | ++ | ++ | ++ | ++ |
| Detection Bias | |||||||||||||
| 7. Can we be confident in the exposure characterization? | ++ | ++ | ++ | ++ | ++ | ++ | NR | NR | ++ | ++ | NR | ++ | ++ |
| 8. Can we be confident in the outcome assessment? | ++ | NR | NR | −− | NR | NR | NR | −− | NR | ++ | NR | NR | ++ |
| Selective Reporting Bias | |||||||||||||
| 9. Were all measured outcomes reported? | + | ++ | ++ | ++ | ++ | −− | −− | ++ | + | ++ | ++ | ++ | ++ |
| Other Bias | |||||||||||||
| 10. Were statistical methods appropriate? | ++ | ++ | NR | −− | ++ | ++ | NR | NR | ++ | ++ | NR | ++ | ++ |
| 11. Did researchers adhere to the study protocol? | + | + | + | + | + | + | + | + | + | + | + | + | + |
| 12. Did the study design or analysis account for important confounding and modifying variables (including unintended co-exposures) in experimental studies? | + | + | N/A | N/A | N/A | N/A | N/A | N/A | + | + | N/A | + | + |
| Study | Study Design | Duration | Follow-Up | Sample Size | Gender | Age Range (Mean) | Health Status | Clinical Parameters |
|---|---|---|---|---|---|---|---|---|
| Abduljabbar et al., 2017 [24] | Prospective, parallel design, single-blinded, randomized, controlled trial | 6 mos | 3 mos 6 mos | 63 patients: 32 control gp: nonsurgical mechanical debridement [MD], 39 implants 31 laser gp: MD and single application of Nd:YAG laser, 35 implants | 63 males | Group 1 (MD): 31–58 yrs (43.6 yrs) Group 2 (MD + laser): 29–60 yrs (40.5 yrs) | Systemically healthy, no smokers | Plaque Index (PI) Bleeding on probing (BOP) Probing depth (PD) Suppuration Peri-implant crestal bone loss Radiographic analysis |
| Arısan et al., 2015 [25] | Prospective, parallel design, split-mouth, randomized, controlled trial | 6 mos, February 2010 to May 2013 | 1 mo 6 mos | 10 patients: 5 control gp: MD, 24 implants 5 laser gp: MD and single application of 810-nm diode laser, 24 implants | 3 males 7 females | 54–76 yrs (55.1 yrs) | Systemically healthy, no smokers | PI BOP PD Marginal bone loss Microbial analysis Radiographic analysis |
| Bach 2009 [26] | Prospective, longitudinal study | 12 yrs, 1995–2007 | 4 wks 6 mos 1 yr Every yr | 10 patients, 17 implants | 5 males 5 females | 20–70 yrs | Not specified | Microbial analysis Radiographic analysis |
| Clem and Gunsolley 2019 [27] | Prospective, consecutive, longitudinal study | 2+ yrs, June 2014 to November 2016 | 6 mos 12 mos | 20 patients, 23 implants | 11 males 9 females | 56–85 yrs | Systemically healthy except for: Type II controlled diabetes: 2 Cardiovascular disease: 8 Bisphosphonates therapy: 2 Self-reported smoker: 1 | PD Implant bone levels and fill Radiographic analysis |
| Deppe et al., 2005 [28] | Prospective, controlled, longitudinal study | 3 yrs, February 1999 to February 2002 | 4 mos 6–38 mos (mean 17 mos) | 16 patients: 6 control gp: air-powder abrasive [APA], 19 implants 10 laser gp: APA and single application of CO2 laser, 22 implants | Not specified | Not specified | Not specified | PI BOP PD Distance between implant shoulder and marginal mucosa (DIM) Attachment level (PD + DIM) Radiographic analysis of distance between implant and bone (DIB) |
| Deppe et al., 2007 [29] | Prospective, controlled, longitudinal study | 5+ yrs, January 1999–May 2004 | 5–59 mos (mean 37 mos) | 32 patients: 13 control gp: air-powder abrasive [APA], 34 implants 19 laser gp: APA and single application of CO2 laser, 39 implants | Not specified | Not specified | Not specified | PI BOP PD Distance between implant shoulder and mucosa (DIM) Clinical attachment level (CAL) Distance from implant shoulder to first bone contact (DIB) Radiographic analysis |
| Nicholson et al., 2014 [30] | Retrospective longitudinal study | 3 mos–16 yrs | 2 mos 8 mos 36 mos 48 mos | 16 patients, number of implants not specified | 7 males 9 females | 32–79 yrs (54 yrs) | Not specified | Radiographic analysis |
| Norton 2017 [31] | Prospective, longitudinal study | 1+ yrs, October 2013–February 2015 | 1 yr | 20 patients, 27 implants | Not specified | Not specified | Smoking did not preclude inclusion | BOP PD Suppuration Radiographic analysis |
| Peng and Tomov 2012 [32] | Prospective, parallel design, single-blinded, randomized, controlled trial | 1 yr, September 2010 to August 2011 | 6 mos | 68 patients, 128 implants Mechanical therapy gp (number of patients not specified) Laser therapy gp (number of patients not specified) | Not specified | Not specified | Not specified | BOP PD Radiographic analysis |
| Renvert et al., 2011 [22] | Prospective, parallel design, single-blinded, randomized, controlled trial | 2 yrs, October 2007 to September 2009 | 6 mos | 42 patients: 21 air abrasive gp: 45 implants 21 laser gp: 55 implants | Not specified | (Control: 68.9 yrs, Laser: 68.5 yrs) | Not specified | BOP PD Suppuration Radiographic analysis |
| Romanos et al., 2008 [14] | Prospective longitudinal study | 27.10 mos (±17.83) | 1 mo 3 mos 6 mos 9 mos then every year | 15 patients, 19 implants | 5 males 10 females | (57.21 yrs) | Not specified | PI BOP PD Width of keratinized tissue Bone loss Radiographic analysis of bone fill |
| Schwarz et al., 2006 [19] | Prospective, parallel design, randomized, controlled trial | 12 mos | 3 mos 6 mos 12 mos | 20 patients: 10 control gp: mechanical debridement, 20 implants 10 laser gp: 20 implants | Control: 5 males 5 females Laser: 4 males 6 females | (Control: 52 yrs, Laser: 56 yrs) | No systemic diseases Patients who smoked occasionally were not categorized as smokers | PI BOP PD Gingival recession CAL Radiographic analysis |
| Wang et al., 2020 [33] | Prospective, parallel design, double-blinded, randomized, controlled trial | 24 wks, June 2017 to November 2018 | 24 wks | 24 patients: 12 control gp: open flap mechanical debridement, bone grafting and membrane, 12 implants 12 laser gp: 12 implants | Control: 7 males 5 females Laser: 7 males 5 females | (Control: 63.41 yrs, Laser: 66.41 yrs) | American Society of Anesthesiologists (ASA) I or II Not on medications modifying bone metabolism No smokers or smokers who quit <6 mos | PI BOP PD GR CAL Gingival index Radiographic analysis of bone fillRadiographic analysis of linear bone gain |
| Study | Type of Laser | Manufacturer and Model | Beam Delivery System | Cooling during Laser Treatment | Laser Parameters | Method of Laser Use | Disclosure and Commercial Support |
|---|---|---|---|---|---|---|---|
| Abduljabbar et al., 2017 [24] | Nd:YAG, 1064 nm | Genius Dental, Tureby, Denmark | 300-micron optical fiber | Air and water cooling | 4.0 W, 80 mJ per pulse, 50 Hz pulse rate, 350-ms pulse width | After mechanical debridement with plastic curette, 300-micron fiber inserted into peri-implant pocket almost parallel to the implant, then moved in a mesial-distal direction for 60 to 120 s | Research group funded by Deanship of Scientific Research at King Saud University, Riyadh, Saudi Arabia |
| Arısan et al., 2015 [25] | Diode, 810 nm | Denlase 810/7, Beijing, China | Standard, uninitiated 400-micron optical fiber tip | Not specified | 1.0 W, pulsed mode, 3 J/cm2, 400 mW/cm2, 1.5 J | After mechanical debridement with plastic curette, uninitiated tip inserted parallel to the long axis of the implant, about 1 mm from the most apical level of the peri-implant sulci Tip moved in a mesiodistal and apicocoronal direction around the implant for 60 s Laser spot diameter 1 mm | Study supported by a grant from the Istanbul University Research Fund |
| Bach 2009 [26] | Diode, 810 nm | Oralia 01 IST, Constance, Germany | Optical fiber, contact | Not specified | 1.0 W, emission mode not specified | After mucoperiosteal flap and removal of granulation tissue, decontamination for 20 s | Not specified |
| Clem and Gunsolley 2019 [27] | Er:YAG, 2940 nm | J. Morita AdvErL EVO, Osaka, Japan | Radial firing tipWorking distance not specified | Sterile water 5 mL/min | 50 mJ/mm2, 20 Hz | After full-thickness mucoperiosteal flap, granulomatous tissue within defects removed with laser, then implant surfaces irradiated with at least two complete passes or until a change in the reflective quality of the implant surface or dark gray discoloration of the implant surface was observed | J Morita Corp. provided laser equipment and support for creation of manuscript Study partially supported by an educational grant from J Morita Corp. |
| Deppe et al., 2005 [28] | CO2, 10,600 nm | DEKA 20C, Freising, Germany | Articulated arm and handpiece with focus distance of 125 mm, working distance not specified | Not specified | CW, 2.5 W | After full-thickness flap, granulation tissue removal, and air-powder treatment of implant surfaces for 60 s, implant decontamination for 12 × 5 s laser irradiation. Laser spot diameter 200 microns when focused | Not specified |
| Deppe et al., 2007 [29] | CO2, 10,600 nm | DEKA 20C with Swiftlase scanner, Freising, Germany | Articulated arm, scanner and handpiece focal length 125 mm, spot diameter Working distance not specified Angled mirrors (90 and 120 degrees) mounted on handpiece | Not specified | CW, 2.5 W | After full-thickness flap, implant decontamination for 12 × 5 s laser irradiation Laser spot diameter 200 microns when focused Scanner used in CW mode, energy density of 175 J/cm2, exposure time 5 s, to reduce local heat accumulation by sweeping a focused CO2 laser beam in 0.1 s over an area of 3.0 mm diameter, (resulting in a total of 7.06 mm2). Dwell time on each point was less than 1 ms | Research project supported by Friadent |
| Nicholson et al., 2014 [30] | Nd:YAG, 1064 nm | Millennium Dental Technologies PerioLase MVP-7, Cerritos, California | Optical fiber | Not specified | Not specified Light dosage about one-third the energy applied around teeth | Laser first used to remove inflamed pocket epithelium, open the pocket for access, and decontaminate implant After removal of accretions from implant surface with hand instruments and ultrasonic scaler, and after decortication, laser then used to form a stable fibrin clot | Study supported by Millennium Dental Technologies One author received consulting fees from Millennium, 3 authors are principals of Millennium Manuscript represented the best submitted cases from responders |
| Norton 2017 [31] | Er:YAG, 2940 nm | J. Morita AdvErL EVO, Osaka, Japan | Tip not specified Working distance not specified | Not specified | Initial settings of 50 mJ, 25 Hz | After flap reflection and removal of fibrous tissue capsule surrounding the implants and gross hard deposits with curettes, contaminated implant surfaces treated with laser. Settings were occasionally varied according to need to ensure comprehensively debrided, cleaned, and decontaminated implant surfaces | Study funded by a grant from Morita, Inc. |
| Peng and Tomov 2012 [32] | Er:YAG, 2940 nm | Syneron LiteTouch, Yokneam Illit, Israel | Laser-in-handpiece, 1300-micron tip, contact or noncontact (working distance 1.5 mm) Flap incision: Contact, 0.4 × 17 mm tip Granulation tissue ablation: Noncontact, 1.3 × 14 mm tip Bone remodeling: Noncontact, 1.3 × 19 mm tip Implant decontamination: Noncontact, 1.3 × 17 mm tip Decortication: Noncontact, 1.3 × 19 mm tip | Water spray levels settings 5–8, depending on procedure: Flap incision: 5–6 Granulation tissue ablation: 6 Bone remodeling: 8 Implant decontamination: 6 Decortication: 8 | Flap incision: 200 mJ, 35 Hz Granulation tissue ablation: 400 mJ, 17 Hz Bone remodeling: 300 mJ, 25 Hz Implant decontamination: 150 mJ, 45 Hz Decortication: 300 mJ, 25 Hz | Flap incision with laser, reflection, noncontact tip to remove granulation tissue, and clean implant surface by systematically moving tip along surface Laser tip in constant motion | Not specified |
| Renvert et al., 2011 [22] | Er:YAG. 2940 nm | KaVo Key Laser 3, Biberach, Germany | Cone-shaped sapphire tip, working distance not specified | Not specified | 100 mJ/pulse, 10 Hz (12.7 J/cm2) | Tip used in parallel mode using a semicircular motion around the circumferential pocket | Study sponsored by EMS, KAVO, Philips Oral Healthcare |
| Romanos et al., 2008 [14] | CO2, 10,600 nm | Weil Dental SC 20 or DEKA Smart US-20D, Freising, Germany | Articulated arm and handpiece, noncontact Working distance not specified Tip not specified | Not specified | 2.84 ± 0.83 W. Emission mode not specified | After full-thickness mucoperiosteal flap, granulomatous tissue removed with titanium curettes, and exposed implant surfaces irradiated for 1 min | Not specified |
| Schwarz et al., 2006 [19] | Er:YAG, 2940 nm | KaVo KEY 3, Biberach, Germany | Specially designed periodontal handpiece, and cone-shaped glass fiber tip emitting a radial and axial laser beam, contact | Water irrigation | 10 Hz, 100 mJ/pulse (12.7 J/cm2), pulse energy at tip approximately 85 mJ/pulse | Semicircular motion from coronal to apical parallel to implant surface Both control and laser: 6 min avg per implant | Study supported by grant from Arbeitsgemeinschaft für Kieferchirurgie innerhalb der Deutschen Gesselschaft für Zahn-, Mund- und Kieferheilkunde |
| Wang et al., 2020 [33] | Er:YAG, 2940 nm | Morita AdvErL EVO, Kyoto, Japan | Optical transmission cable with metal-shelf tips PS600T, PSM600T, R600T | Not specified | 50 mJ/pulse, 25 Hz, 0.5 mm/s for granulation tissue removal and implant decontamination 30 mJ/pulse, 20 Hz, 0.5 mm/s for irradiation of implant defect and tissue | Debridement and surface decontamination of implant surfaces and removal of inflamed tissue with laser Slow linear motion of 0.5 mm/s vertically and horizontally for 3–5 min After implantoplasty for peri-implant suprabony defect, infrabony defect debrided with laser | Study supported by grants from J Morita (Tokyo, Japan) and University of Michigan School of Dentistry Department of Periodontics and Oral Medical Clinical Research Fund BioHorizons (Birmingham, Alabama) provided biomaterials Co-author Wang HL has lectured for J Morita and received honoraria |
| Study | Control | Non-Surgical Intervention before Laser Treatment | Surgical Therapy in Conjunction with Laser Treatment | Use of Biomaterials | Use of Antibiotics | Use of Oral Irrigant | Follow-Up Care |
|---|---|---|---|---|---|---|---|
| Abdul-jabbar et al., 2017 [24] | Nonsurgical mechanical debridement using plastic curettes | Nonsurgical mechanical debridement using plastic curettes, plaque removed from implant surfaces | No surgical therapy | Not used | Not used | Not used | Not mentioned |
| Arısan et al., 2015 [25] | Nonsurgical mechanical debridement using plastic curettes | Nonsurgical mechanical debridement using plastic curettes Supragingival plaque removed by sterile gauze | No surgical therapy | Not used | Not used | Intraoperative: Peri-implant sulci of all implants were washed with sterile saline solution to remove debris | Not mentioned |
| Bach 2009 [26] | No control | Cleaning and polishing | Mucoperiosteal flap, removal of granulation tissue, decontamination with diode laser, soft tissues apically positioned. Bone augmentation and mucogingival corrections when needed | Materials used for bone augmentation not specified | Not mentioned | Preoperative: Application of disinfecting agents | 4 wks, 6 mos, 1 yr, and annually: exposed implant surfaces decontaminated with diode laser |
| Clem and Gunsolley 2019 [27] | No control | Antimicrobial therapy starting the day before surgery | Full thickness mucoperiosteal flaps, laser removal of granulomatous tissue. Implant surfaces irradiated. Bone grafting for vertical defects | Patient received one of the three options: (1) mineralized freeze-dried bone allograft (FDBA; creos™ allo.gain, Nobel Biocare) with recombinant human platelet-derived growth factor-BB (rhPDGF-BB; creos™ allo.gain, Nobel Biocare) (2) 70/30 mix of mineralized FDBA/demineralized FDBA (DFDBA) with PDGF (OraGraft® DGC1, LifeNet Health) with rhPDGF-BB (GEM 21S®, Lynch Biologics) (3) DFDBA and enamel matrix derivative (EMD; Emdogain®, Straumann) Rapidly absorbing collagen membrane used only when facial or lingual defects were present | Metronidazole 500 mg and amoxicillin 500 mg for 10 days bid starting the day before surgery | Intraoperative: H2O2 soaked gauze in the defects for about 10 s and irrigated with sterile saline Postoperative: Chlorhexidine 0.12% swabs | 2 wks: Patients to use soft toothbrush and light dental tape 4 wks: Reinforced oral hygiene instruction on more aggressive brushing or a modified plaque control approach |
| Deppe et al., 2005 [28] | Conventional decontamination with air-powder abrasive | Chlorhexidine 0.3% for 3 weeks before treatment | Both groups: full thickness flaps, granulation tissue removal, implant decontamination, implant surfaces treated with air-powder-abrasive, then flaps resected, re-positioned, and sutured | Not mentioned | Not used | Preoperative: Chlorhexidine 0.3% | Not mentioned |
| Deppe et al., 2007 [29] | Soft tissue resection after conventional decontamination | Chlorhexidine 0.3% for 3 weeks before treatment | Full-thickness flaps, granulation tissue removal and implant decontamination, bone augmentation when recommended, then flaps resected, re-positioned, and sutured | Bone augmentation recommended only for screw-retained prosthetics 50–50 mix of resorbable beta-tricalcium phosphate (βTCP or Cerasorb®, Curasan) with bone harvested from mandibular retromolar region Implants were submerged and covered by nonresorbable membrane (GORE-TEX® G 4, W. L. Gore) | Not used | Preoperative: Chlorhexidine 0.3% | Not mentioned |
| Nicholson et al., 2014 [30] | No control | None | Surgical therapy in conjunction with laser treatment as part of the LAPIP protocol | No biomaterials used | Antimicrobial therapy post-treatment as part of the LAPIP protocol | Intraoperative: 0.12% chlorohexidine as part of the LAPIP protocol Postoperative: 0.12% chlorohexidine as part of the LAPIP protocol | Not mentioned |
| Norton 2017 [31] | No control | None | Open flap surgical debridement, fibrous tissue and hard deposits removed using curettes, laser implant decontamination, regeneration therapy with bone graft and membrane, flap sutured | Regenerative Therapy: Defects grafted with anorganic bovine bone mineral, rehydrated in sterile saline (Bio-Oss®, Geistlich) and confined by use of a resorbable collagen barrier membrane (Bio-Gide®, Geistlich) fixed in position with titanium tacks (FRIOS, Dentsply) | No antibiotics were prescribed | Intraoperative: No chlorohexidine used Postoperative: Chlorhexidine 0.2% mouthrinse, 10 mL twice a day for 1 min for 1 wk | Not mentioned |
| Peng and Tomov 2012 [32] | Conventional mechanical therapy with sharp curettes and ultrasonic device, followed by chemical debridement with tetracycline solution | Nonsurgical hygiene phase to reduce inflammation | Flap raised to access implant surface, granulation tissue removed with laser, laser in noncontact mode if calculus, rinsed with sterile saline, bone augmentation when required | Bone augmentation when required with deproteinized bovine bone (Bio-Oss®, Gesitlich) and bone allograft (Dembone®) with or without an absorbable biomembrane, material not specified | Clindamycin 150 mg, 50 tabs and Antibacterial periodontal treatment was repeated if inflammation recurred | Postoperative: Chlorhexidine 0.2% starting the next day for two weeks three times per day | Supportive phase to maintain long-term results. Inflammation detected on recall visit was treated with repeated antibacterial periodontal treatment |
| Renvert et al., 2011 [22] | Non-surgical debridement with air-abrasive device | None | No surgical therapy | Not mentioned | Not mentioned | Not mentioned | At all study time points, patients received individualized oral hygiene instructions. After 3 mos: Patients also received a sonic toothbrush and additional brush heads |
| Romanos et al., 2008 [14] | No control | None | Full-thickness mucoperiosteal flap elevated, granulomatous tissue removed with titanium curettes, laser was used, flaps were sutured | 10 bony lesions were augmented with autogenous bone 9 defects with cancellous bone graft (Bio-Oss®, Osteohealth) Augmented sites were covered with collagen membranes (Bio-Gide®, Osteohealth) fixed with titanium pins (FRIOS®, FRIADENT) Mucoperiosteal flaps were closed with 4-0 silk sutures (RESORBA®) | Not used | Not mentioned | Not mentioned |
| Schwarz et al., 2006 [19] | Nonsurgical mechanical debridement using plastic curettes and antiseptic therapy | All patients: For 2 weeks before treatment, supragingival professional implant/tooth cleaning using rubber cups and polishing paste and oral hygiene instructions Patients with chronic periodontitis: Additional scaling and root planing using hand instruments | No surgical therapy | Not mentioned | Not mentioned | Intraoperative: In control only, pocket irrigation with 0.2% chlorhexidine digluconate solution, then subgingival application of 0.2% chlorohexidine gel Postoperative: Chlorohexidine rinse twice a day for 2 min for 2 weeks | In control group: Chlorohexidine rinse twice a day for 2 wks post-treatment Both groups: Supragingival professional implant/tooth cleaning and oral hygiene also at baseline, 1, 3, 6, 12 mos Both groups: Due to increased BOP and CAL, all patients were discontinued from study at 12 mos, and treated with Er:YAG laser therapy and bone augmentation |
| Wang et al., 2020 [33] | Surgical regenerative therapy including mechanical debridement and guided bone regeneration same as test gp, but no laser therapy | Full mouth prophylaxis or periodontal maintenance with piezo-instruments and stainless-steel hand scalers without subgingival implant debridement | Both test and control groups received open flap mechanical debridement, supracrestal implantoplasty, bone grafting, and acellular dermal matrix membrane Laser group used Er:YAG laser to modulate and remove inflammatory tissue and decontaminate implant surfaces | Bone grafting and regenerative therapy of infrabony defects. Mineralized bone allograft used in both groups Composite graft included 3:1 ratio of allograft and demineralized bone fibers (MinerOss and Grafton, BioHorizons) Absorbable acellular dermal matrix (ADM) membrane (Alloderm GBR, BioHorizons) was used Flap was sutured with polytetrafluorethylene (PTFE) sutures (Cytoplast, BioHorizons) Sutures were left for at least 14 days A periodontal dressing (Coe-Pak Periodontal Dressing, Patterson Dental) was used | Postoperatively, all patients were prescribed 500 mg Amoxicillin tid for 10 days; if patients were allergic, Azithromycin 500 mg for the first day and 250 mg for the next 3 days Ibuprofen 600 nm as needed for pain control | Postoperative: Chlorohexidine rinse twice a day for 1 min, bid for 1 week | Patients in both groups avoided brushing or touching the operated area for 2 weeks. 3 and 6 mos: Maintenance was performed All patients completed the 6 mos clinical trial and follow-up |
| Study | Number of Implant and Implant Type | Loading Protocol Initial Placement or after Peri-Implant Treatment | Duration of Implant Function before Treatment [Mean (Range)] | Implant-Restoration Connection | Occlusal Adjustments | Implant Crown Removed during Treatment | Implantoplasty in Conjunction with Laser Treatment |
|---|---|---|---|---|---|---|---|
| Abdul-jabbar et al., 2017 [24] | Group 1 (MD): 39 platform-switched Straumann® Bone Level implants Group 2 (laser): 35 platform-switched Straumann® Bone Level implants | Delayed-loaded: Loaded about 4 mos after initial implant placement | Group 1: 4.4 yrs (2–6.5 yrs) Group 2: 4.8 years (1–5.3 yrs) | All implants: Cement-retained | Not done | Not done | Not done |
| Arısan et al., 2015 [25] | Two-piece, tapered root form, rough surface (acid etched and sand blasted) implants: 48 (15 MIS®, 12 CAMLOG Biotechnologies, 8 Nobel Biocare™ Replace®, 7 BioHorizons®, 6 not mentioned) | Not mentioned | 19.4 mos (12.2–25.2 mos) | All implants:Cement-retained | Occlusal contacts were checked to ensure the absence of overloading | All superstructures were removed, then recemented after treatment with a polycarboxylate cement An acrylic-based temporary crown was cemented on the treated implants if the permanent restoration was faulty | Not done |
| Bach 2009 [26] | 17 implants: - implant details not specified - 2 implants lost in the 12 yr period | Not mentioned | Not mentioned | Not mentioned | Not mentioned | Not mentioned | Not mentioned |
| Clem and Gunsolley 2019 [27] | Enhanced titanium surface implants: 17 Machined surface implants: 6 | Not mentioned | 14 of 23 implants in function >5 yrs Implants in function: 6 < 5 yrs 9 > 5 yrs 3 > 10 yrs 2 > 15 yrs | 11 stock-cemented 7 custom-cemented 2 screw-retained | Not done | Not done | Not done |
| Deppe et al., 2005 [28] | Group 1 (control): 19 (17 IMZ®, 2 Frialit 2®) - 3 implants lost Group 2 (laser): 22 (13 IMZ®, 4 Frialit 2®, 2 Brånemark®, 3 ITI-screw implants®) - 3 implants lost | Not mentioned | Not mentioned | Not mentioned | Not mentioned | Shown in clinical photos but not mentioned in treatment | Done in clinical photos but not mentioned in treatment |
| Deppe et al., 2007 [29] | Group 1 (control): - 19 (17 IMZ®, 2 Frialit-2®) - 3 implants lost Group 2 (bone augmentation, no laser): 15 (7 IMZ®, 5 Frialit-2®, 2 Brånemark®) - 4 implants lost Group 3 (laser and soft tissue resection): 22 (13 IMZ®, 4 Frialit-2®, 2 Brånemark®, 3 Straumann® screw-type) - 2 implants lost Group 4 (laser and bone augmentation) :17 (11 IMZ®, 3 Frialit-2®, 2 Brånemark®, 1 Straumann® screw-type) - 4 implants lost | Patients with screw-retained prostheses received bone augmentation, implants were submerged with healing time of 4 mos before the implants were reloaded For patients with cemented restorations, soft tissue was resected following decontamination, and implants reloaded immediately after the decontamination | Not mentioned | Screw-retained or cement-retained | Not done | All screw-retained prostheses were removed Cemented prostheses were left in situ | Not done |
| Nicholson et al., 2014 [30] | Not specified | Not mentioned | 3 mos to 16 yrs | Not mentioned | Occlusal adjustment is part of the LAPIP protocol | Not mentioned | Not done |
| Norton 2017 [31] | 27 implants, 2 patients were lost to final follow-up: 1 patient with 2 implants after her 3-mos review, and 1 patient with 1 implant after implant removal due to persistent discomfort at 6 mos | Not mentioned | Not mentioned | Not mentioned | Not done | Documented clinical case showed prosthesis removed, but not mentioned for other cases | Not done |
| Peng and Tomov 2012 [32] | 128 implants: - implant details not specified - no implants were lost | Not mentioned | Not mentioned | Not mentioned | Not done | Suprastructures removed before baseline measurements and before surgical phase | Not done |
| Renvert et al., 2011 [22] | Air abrasive gp: 45 (29 machined surface, 16 medium rough surface) Laser gp: 55 (41 machined surface, 14 medium rough surface) - no implants were lost | Superstructures replaced and loaded right after treatment | Not mentioned | Not mentioned | Not mentioned | Suprastructures removed before baseline measurements and for treatments Remounted after treatment | Not mentioned |
| Romanos et al., 2008 [14] | 19 implants: 14 Ankylos®, 3 ITI®, 2 IMZ® | 4 implants immediately loaded with final restoration after bone graft 12 implants submerged after bone graft | Not mentioned | Not mentioned | Not mentioned | Not mentioned | Not mentioned |
| Schwarz et al., 2006 [19] | Control: 20 (2 IMZ Twin Plus®, 2 ITI SLA TPS®, 8 Spline Twist MTX®, 4 ZL-Duraplant Ticer®, 4 CAMLOG Screw Line®) Laser gp: 20 (2 IMZ Twin Plus®, 6 ITI SLA TPS®, 6 Spline Twist MTX®, 4 ZL-Duraplant Ticer®, 2 CAMLOG Screw Line®) | Not mentioned | Control: 4.2 yrs Laser gp: 5.1 yrs | Not mentioned | Not mentioned | Not mentioned | Not mentioned |
| Wang et al., 2020 [33] | Control: 12 Laser: 12 Only implants with rough surfaces were included | Not mentioned | At least 6 mos | Not mentioned | Not mentioned | Not done | Supracrestal implantoplasty for peri-implant suprabony defects and infrabony defects debrided with dental scalers or laser prior to bone grafting, bone wax was adapted and fixed in defect to capture the titanium particles |
| Study | Method of Radiographic Assessment | Radiographic Standardizations | Radiographic Assessment | Radiographic Outcome Compared to Baseline | Radiographic Outcome Compared to Control |
|---|---|---|---|---|---|
| Abdul-jabbar et al., 2017 [24] | Mean mesial and distal crestal bone loss (CBL) were recorded in millimeters on digital radiographs using a precalibrated software program (Scion Image, Scion Corp., Fredrick, MD) CBL (peri-implant crestal bone loss): Distance from the widest supracrestal part of the implant to the alveolar crest. Total CBL was determined by averaging the mesial and distal scores of CBL | Standardized digital radiographs using the radiographic paralleling technique and a guiding device at follow-up Calibration of software used was performed using the predefined implant length | Baseline 6 mos | CBL compared to baseline (statistical analysis performed using SPSS v. 18 software, IBM) Control gp 6 mos: Not statistically significant Laser gp 6 mos: Not statistically significant | CBL compared to control Laser gp 6 mos: Not statistically significant Control: Nonsurgical mechanical debridement with plastic curettes |
| Arısan et al., 2015 [25] | Panoramic radiographs were scanned and visualized using Image J software (NIH, Bethesda, MD) MBL (marginal bone loss): Distance between the implant shoulder and the marginal peri-implant crestal bone was repeated in the distal and mesial of all implants. Measurements were repeated twice, and averaged to yield final values | Measuring tool was calibrated using the known implant length | Baseline 6 mos | MBL compared to baseline (statistical analysis performed using Graphpad Prism 6.0 software, Graphpad Software) Control gp 6 mos: significantly increased Laser gp 6 mos: significantly increased | MBL compared to control Laser gp 6 mos: Significantly increased Control: Conventional scaling and debridement with plastic implant curette |
| Bach 2009 [26] | Orthopantomograms and dental films assessed visually by clinician | Orthopantomo-grams and dental films in parallel technique, not standardized | Orthopantomo-grams: Baseline Immediate post-op 1 yr Every 2 yrs Dental films: Baseline 4 wks 6 mos 1 yr Every yr | Compared to baseline (no statistical analysis) 1 yr: bone gain in all 17 implants to first thread and implant cervix 5 yrs: bone gain in 12 implants 10 yrs: bone gain in 10 implants >12 yrs: bone gain in 9 implants, horizontal tissue loss in 6 implants at first/second thread In 2 implants a successive loss of the bony supporting tissue led to removal of the artificial abutment in one case after 7 yrs and in another case after 9 yrs | No control |
| Clem and Gunsolley 2019 [27] | Periapical digital radiographs assessed visually by clinician | Standardized periapical digital radiographs using the Rinn positioner (Dentsply Sirona) | Baseline 3 mos 6 mos 12 mos Every yr | Bone fill compared to baseline (no statistical analysis) 12 mos: positive bone fill in 17 implants (>50% bone fill in 9 implants, 50% bone fill in 3 implants, <50% bone fill in 5 implants, no bone fill in 3 implants, unknown in 3 implants) | No control |
| Deppe et al., 2005 [28] | Orthopantomograms evaluations for information on the peri-implant marginal bone. Measurements were made with calipers on a back-lit screen in a darkened room. The implant upper edge to the tip of the implant was used as the reference lengthDIB: distance between implant and bone | Standardized orthopantomo-grams, method of standardization not mentioned | Baseline 4 mos 17 mos (6–38 mos) | DIB compared to baseline (statistical analysis performed using Microsoft Excel® version 97) Control gp 4 mos: Improved by 0.4 mm 17 mos: Worsened by 0.3 mm Laser gp 4 mos: Improved by 0.3 mm 17 mos: Improved by 0.4 mm | DIB compared to control Laser gp 4 mos: Not statistically significant 17 mos: Significantly improved Implants lost: Laser gp: 5 Control: 3 Control: conventional decontamination with air-powder abrasive (Prophy-Jet®, Denstply) |
| Deppe et al., 2007 [29] | Radiographic measurements from orthopantomograms of crestal bone level at mesial and distal sites according to Buser et al., [57] Radiographs were not obtained routinely for all patients, since many refused consent DIB: distance from implant shoulder to first bone contact | Standardized orthopantomo-grams taken if consent given, method of standardization not mentioned | Baseline 4 mos 37 mos (5–59 mos) | DIB compared to baseline (statistical analysis performed using MS Excel) Implants in residual bone Laser gp 4 mos: Improved by 0.3 mm 37 mos: Improved by 0.4 mm Control gp 4 mos: Improved by 0.4 mm 37 mos: Worsened by 0.3 mm Implants in augmented bone Laser gp 4 mos: Improved by 4.4 mm 37 mos: Improved by 2.2 mm Control gp 4 mos: Improved by 2.7 mm 37 mos: Improved by 2.1 mm | DIB compared to control Implants in residual bone Laser gp 4 mos: Not significantly different 37 mos: Significantly improved Implants in augmented bone Laser gp 4 mos: Significantly improved 37 mos: Not significantly different Control: conventional decontamination with air-powder abrasive (Prophy-Jet®, Dentsply) |
| Nicholson et al., 2014 [30] | At least two bitewing radiographs, some cases mandibular CT scan or periapical films A technician skilled at reading dental radiographs, identified the baseline alveolar crest and outlined the “areas of changes in radiolucencies” in subsequent images To be more objective a criteria for gray-level to define the boundary of the lesion was identified | Not mentioned | Baseline 2–48 mos | No statistical analysis Rate of recovery range: 0.1–2.4 mm2/mon (mean rate: 1.24 mm2/mon or 15 mm2/yr)Definite trend for larger lesions to heal faster | No control |
| Norton 2017 [31] | Marginal bone loss on periapical radiographs measured using only contrast, brightness, and sharpness tools in the i-Dixel 3DX software (version 2.2.0.3, Morita) | Periapical radiographs standardized using Rinn device | Baseline 1 yr | Compared to baseline (no statistical analysis) Mesial mean depth reduction: 1.34 mm Distal mean depth reduction: 1.52 mm Mesial defect fill: 27% Distal defect fill: 28% | No control |
| Peng and Tomov 2012 [32] | Intraoral periapical radiographs analyzed by two calibrated investigators | Intraoral standardized periapical radiographs, holders were used for standardization | Baseline 6 mos | Compared to baseline (no statistical report) Laser gp - Mean bone height loss: 0.1 mm - Proportion with radiographic bone loss (0.1–2.0 mm): 49.3% - Proportion with no radiographic bone change (0.0 mm): 29.3% - Proportion with radiographic bone gain (0.1–3.0 mm): 29.4% Control gp - Mean bone height loss: 0.5 mm - Proportion with radiographic bone loss (0.1–2.0 mm): 74.9% - Proportion with no radiographic bone change (0.0 mm): 4.2% - Proportion with radiographic bone gain (0.1–3.0 mm): 20.9% | Compared to control (no statistical analysis) Laser gp (6 mos): - Less mean bone height loss - Smaller proportion with radiographic bone loss - Larger proportion with no radiographic bone change - Larger proportion with radiographic bone gain Control: Conventional mechanical therapy using ultrasonic device at low settings (PI tip, Piezon® ultrasonic device, EMS) followed by chemical debridement with tetracycline solution |
| Renvert et al., 2011 [22] | Radiographic digital images assessed using the ImageJ software program 1:43 r (National Institute of Health, Bethesda, MA, USA) | Intraoral standardized radiographs utilizing Eggen holders | Baseline6 mos | Compared to baseline (statistical analysis performed using SPSS PASW software, Statistics 18.0 for MAC, SPSS, Inc.) Laser gp - No differences in alveolar bone changes - Mean bone loss: 0.3 mm - Proportion with radiographic bone loss (0.1–3.0 mm): 58.3% - Proportion with no radiographic bone change (0.0 mm): 2.1% - Proportion with radiographic bone gain (0.1–2.0 mm): 39.6% Control gp - No differences in alveolar bone changes - Mean bone loss: 0.1 mm - Proportion with radiographic bone loss (0.1–3.0 mm): 56.1% - Proportion with no radiographic bone change (0.0 mm): 2.4% - Proportion with radiographic bone gain (0.1–2.0 mm): 41.5% | Compared to control (statistical analysis performed using SPSS PASW software, Statistics 18.0 for MAC, SPSS, Inc.) Data reported not statistically significant Laser gp (6 mos): - More mean bone height loss - Greater proportion with radiographic bone loss - Smaller proportion with no radiographic bone change - Smaller proportion with radiographic bone gain Control: Air abrasive treatment (PERIOFLOW®) |
| Romanos et al., 2008 [14] | Conventional panoramic or periapical radiographs assessed visually by clinician | Not mentioned | Baseline1 mo 3 mos 6 mos 9 mos 12 mos Entire observation period: 27 mos (±17.83 mos) | Compared to baseline Defects with xenogenic bone: Complete bone fill (no statistical analysis) Defects with only autogenous bone graft: At least two-thirds bone fill because of some bone graft resorption (no statistical analysis) | No control |
| Schwarz et al., 2006 [19] | Periapical radiographs assessed visually by clinician Marginal bone loss as measured from the bone crest to the most coronal bone-to-implant contact | Periapical radiographs were taken using the long-cone parallel technique, standardization not mentioned | Baseline 12 mos | Compared to baseline: No statistical report, no noticeable change in radiographic outcomes | Compared to control: No statistical report, no noticeable change in radiographic outcomes Control: mechanical debridement using plastic curettes followed by pocket irrigation with 0.2% chlorhexidine digluconate solution and 0.2% chlorhexidine gel |
| Wang et al., 2020 [33] | Linear bone gain in periapical radiographs assessed by determining a constant specific radiographic reference for each patient (platform or porcelain to abutment junction) using MiPACS (Medicor Imaging, Charlotte, North Carolina) Peri-implant defect size measurements were superimposed with 3D Slicer software (Version 4.10.1, Bioinformatics and Computational Biology program, National Institute of Health, USA) and ImageJ software (Version 1.8.0, National Institute of Health, USA). | Standardized radiographs using intraoral periapical digital sensors with customized putty bite blocks for each patient to standardize positioning of the sensor and angle | Baseline 24 wks | Compared to baseline: Radiographic linear bone gain Control: 1.08 mm Laser gp: 1.27 mm Defect size change Laser gp - decreased by 24.46% - more bone gain (no statistical analysis) Control gp - decreased by 15.19% - more bone gain (no statistical analysis) | Compared to control: Radiographic linear bone gain Laser gp: slightly increased, not statistically significant Defect size Laser gp: more bone gain, not statistically significant Control: Open flap mechanical debridement, supracrestal implantoplasty, bone grafting, and acellular dermal matrix membrane without laser therapy |
| Study | Bleeding on Probing Compared to Baseline | Bleeding on Probing Compared to Control | Clinical Attachment Level Gain Compared to Baseline | Clinical Attachment Level Gain Compared to Control | Probing Depth Compared to Baseline | Probing Depth Compared to Control | Microbial Analysis Compared to Baseline | Microbial Analysis Compared to Control | Adverse Reactions |
|---|---|---|---|---|---|---|---|---|---|
| Abdul-jabbar et al., 2017 [24] | No statistical analysis Control gp 3 mos: Decreased 32.1% 6 mos: Decreased 39.8% Laser gp 3 mos: Decreased 44.8% 6 mos: Decreased 39.8% Comparative suppuration results not reported | Statistical analysis performed using SPSS v.18 software, IBM Baseline: No significant difference 3 mos: Signifi-cantly lower 6 mos: No significant difference Compara-tive suppura-tion results not reported | Not assessed | Not assessed | No statistical analysis Control gp 3 mos: Decreased 1.1 mm 6 mos: Decreased 1.6 mm Laser gp 3 mos: Decreased 2.9 mm 6 mos: Decreased 2.8 mm | Statistical analysis performed using SPSS v.18 software, IBM Baseline: No significant difference 3 mos: Significantly lower 6 mos: No significant difference | Not done | Not done | Not mentioned |
| Arısan et al., 2015 [25] | Statistical analysis performed with Graphpad Prism 6.0 software, Graphpad Software Control gp 1 mo: Significantly decreased 6 mos: No significant difference Laser gp 1 mo: Significantly decreased 6 mos: No significant difference | Statistical analysis performed with Graphpad Prism 6.0 software, Graphpad Software No significant difference | Not assessed | Not assessed | Statistical analysis performed with Graphpad Prism 6.0 software, Graphpad Software Control gp 1 mo: Significantly decreased 6 mos: Significantly increased Laser gp 1 mo: Significantly decreased 6 mos: Significantly increased | Statistical analysis performed with Graphpad Prism 6.0 software, Graphpad Software Baseline: No significant difference 1 mon: No significant difference 6 mos: No significant difference | Statistical analysis performed with Graphpad Prism 6.0 software, Graphpad Software Control gp 1 mo: No significant difference Laser gp 1 mo: No significant difference | Statistical analysis performed with Graphpad Prism 6.0 software, Graphpad Software Not statistically significant | No complications or negative outcomes |
| Bach 2009 [26] | Not assessed | No control | Not mentioned | No control | Not assessed | No control | P. gingivalis almost completely eliminated during the whole examination period, and a significant reduction of other anaerobe, gram-negative bacteria | No control | Not mentioned |
| Clem and Gunsolley 2019 [27] | Not reported | No control | Not assessed | No control | Statistical analysis with Tukey t-test and ANOVA For probings <6 mm 6 mos: No statistically significant improvement 12 mos: No statistically significant improvement For probings ≥ 6 mm 6 mos: Statistically significant improvement 12 mos: Statistically significant improvement | No control | Not done | No control | Not mentioned |
| Deppe et al., 2005 [28] Data before surgical interven-tion was used as the baseline in this table | No statistical analysis Sulcus Bleeding index (SBI): Control gp 4 mos: Increased 17 mos: Increased Laser gp 4 mos: Increased 17 mos: Increased | No statistical analysis 4 mos: Decreased 17 mos: Increased | Statistical analysis performed with Microsoft Excel version 97 software Control gp 4 mos: Improved 17 mos: Improved Laser gp 4 mos: Improved 17 mos: Improved | Statistical analysis performed with Microsoft Excel version 97 software 4 mos: Significantly better attachment levels 17 mos: No significant difference | No statistical analysis Control gp 4 mos: Decreased 17 mos: Decreased Laser gp 4 mos: Decreased 17 mos: Decreased | No statistical analysis 4 mos: Decreased 17 mos: Decreased | Not done | Not done | No adverse effects |
| Deppe et al., 2007 [29] Data before surgical interven-tion was used as the baseline in this table | No statistical analysis Sulcus Bleeding index (SBI): Implants in residual bone Control gp 4 mos: Increased 37 mos: Increased Laser gp 4 mos: Increased 37 mos: Increased Implants in augmented bone Control gp 4 mos: Increased 37 mos: Increased Laser gp 4 mos: Decreased 37 mos: Increased | No statistical analysis Sulcus Bleeding index (SBI): Implants in residual bone 4 mos: Decreased 37 mos: Increased Implants in augmen-ted bone 4 mos: Increased 37 mos: Decreased | No statistical analysis Implants in residual bone Control gp 4 mos: Decreased 37 mos: No change Laser gp 4 mos: Decreased 37 mos: Decreased Implants in augmented bone Control gp 4 mos: Decreased 37 mos: Decreased Laser gp 4 mos: Decreased 37 mos: Decreased | Statistical analysis performed with MS Excel software Implants in residual bone 4 mos: Significantly improved 37 mos: Significantly improved Implants in augmented bone 4 mos: Significantly improved 37 mos: No significant difference | No statistical analysis Implants in residual bone Control gp 4 mos: Decreased 37 mos: Decreased Laser gp 4 mos: Decreased 37 mos: Decreased Implants in augmented bone Control gp 4 mos: Decreased 37 mos: Decreased Laser gp 4 mos: Decreased 37 mos: Decreased | No statistical analysis Implants in residual bone 4 mos: Decreased 17 mos: Decreased Implants in augmented bone 4 mos: Decreased 17 mos: No difference | Not done | Not done | Typical postoperative edema 1 patient in conventional augmented group developed severe infection, resulting in total loss of augmentation and all 4 implants within the first weeks after surgery In 1 patient in laser augmented treatment, most augmentation and all 4 implants were lost about 10 months after treatment because of a chronic infection |
| Nicholson et al., 2014 [30] | Not mentioned | No control | Not mentioned | No control | Not reported | No control | Not done | Not done | Not mentioned |
| Norton 2017 [31] | No statistical analysis 1 yr: BOP: 54% reduction Spontaneous bleeding: 80% reduction Spontaneous suppuration: 50% reduction | No control | Not assessed | No control | No statistical analysis 1 yr: Reduced 2.8 mm | No control | Not done | Not done | Not mentioned |
| Peng and Tomov 2012 [32] | Statistical analysis performed with SPSS software Control gp 6 mos: Significantly reduced Laser gp 6 mos: Significantly reduced | 6 mos: Significantly reduced | Not assessed | Not assessed | No statistical analysis Control gp 6 mos: Reduced 0.8 mm Laser gp 6 mos: Reduced 1.7 mm | Not mentioned | Not assessed | Not assessed | Not mentioned |
| Renvert et al., 2011 [22] | Statistical analysis performed with SPSS PASW Statistics 18.0 for MAC software, SPSS Inc. BOP: Implant level Control gp 6 mos: Significantly decreased Laser gp 6 mos: Significantly decreased Suppuration: Control gp 6 mos: Significantly decreased Laser gp 6 mos: Significantly decreased | Statistical analysis performed with SPSS PASW Statistics 18.0 for MAC software, SPSS Inc. Implant level BOP: Not Statisti-cally significant Subject level BOP: Not statisti-cally significant Suppura-tion: Not statisti-cally significant | Not mentioned | Not mentioned | No statistical analysis Implant level Control gp 6 mos: Reduced 0.9 mm Laser gp 6 mos: Reduced 0.8 mm Subject level Control gp 6 mos ≥ 1 mm reduction: 38% Laser gp 6 mos ≥ 1 mm reduction: 25% | Statistical analysis performed with SPSS PASW Statistics 18.0 for MAC software, SPSS Inc. Not statistically significant | Not mentioned | Not mentioned | No serious adverse events |
| Romanos et al., 2008 [14] | Statistical analysis performed but methodology not described Sulcus bleeding index (SBI): Significantly reduced | No control | Not mentioned | No control | Statistical analysis performed but methodology not described Significantly reduced | No control | Not mentioned | Not mentioned | No peri-implant bleeding or suppuration |
| Schwarz et al., 2006 [19] | Statistical analysis performed with SPSS 14.0 software, SPSS Mean BOP Control gp 3 mos: Significantly reduced 6 mos: Significantly reduced 12 mos: Significantly reduced Laser gp 3 mos: Significantly reduced 6 mos: Significantly reduced 12 mos: Significantly reduced | Statistical analysis performed with SPSS 14.0 software, SPSS 3 mos: Signifi-cantly reduced 6 mos: Signifi-cantly reduced 12 mos: Not mentioned | Statistical analysis performed with SPSS 14.0 software, SPSS Control gp 3 mos: Significant gain 6 mos: Significant gain 12 mos: Not significant Laser gp 3 mos: Significant gain 6 mos: Significant gain 12 mos: Not significant | Statistical analysis performed with SPSS 14.0 software, SPSS 3 mos: Not significant 6 mos: Not significant 12 mos: Not significant | Statistical analysis performed with SPSS 14.0 software, SPSS Control gp 3 mos: Significantly reduced 6 mos: Significantly reduced 12 mos: Significantly reduced Laser gp 3 mos: Significantly reduced 6 mos: Significantly reduced 12 mos: Significantly reduced | Statistical analysis performed with SPSS 14.0 software, SPSS 3 mos: Not significant 6 mos: Not significant 12 mos: Not significant | Not mentioned | Not mentioned | Generally uneventful Pus formation in 2 control patients Laser perforation of buccal keratinized mucosa and gingival recession in 1 laser patient At 12 mos, both groups were discontinued from the study due to increasing BOP and a slight loss of mean CAL. These patients received further periimplantitis laser treatment and subsequent bone augmentation |
| Wang et al., 2020 [33] | Statistical analysis performed with SPSS 20 software (IBM, USA) BOP &GI: Control gp 24 wks: Significantly reduced Laser gp 24 wks: Significantly reduced | Statistical analysis performed with SPSS 20 software (IBM, USA) Laser gp 24 wks: Not significant | Statistical analysis performed with SPSS 20 software (IBM, USA) Control gp 24 wks: Significant increase Laser gp 24 wks: Significant increase | Statistical analysis performed with SPSS 20 software (IBM, USA) Laser gp 24 wks: Increase, not significant | Statistical analysis performed with SPSS 20 software (IBM, USA) Control gp 24 wks: Significantly reduced Laser gp 24 wks: Significantly reduced | Statistical analyses performed using SPSS 20 (IBM, USA). Laser gp 24 wks: Significantly reduced | Not mentioned | Not mentioned | Membrane exposure significantly reduced the PD reduction and CAL gain, this was clinically significant |
| Study | Type of Laser | Inflamma-tion (BOP/SBI and/or Suppuration) Compared to Baseline | Inflamma-tion (BOP/SBI and/or Suppuration) Compared to Control | Probing Depth Compared to Baseline | Probing Depth Compared to Control | Bony Defect Compared to Baseline | Bony Defect Compared to Control | Control |
|---|---|---|---|---|---|---|---|---|
| Abdul-jabbar et al., 2017 [24] | Nd:YAG (at 6 mos) | Reduced, significance not analyzed | Not Significant | Reduced, significance not analyzed | Not Significant | Not Significant bone loss | Not Significant bone loss | Mechanical debridement with plastic curettes |
| Arısan et al., 2015 [25] | 810-nm Diode (at 6 mos) | Not Significant | Not Significant | Significant reduction | Not Significant | Significant bone loss | Significant bone loss | Mechanical debridement with plastic curettes |
| Bach 2009 [26] | 810-nm Diode (at 12 mos) | Not reported | No control | Not reported | No control | Bone gain, significance not analyzed | No control | No control |
| Clem and Gunsolley 2019 [27] | Er:YAG (at 12 mos) | Not reported | No control | Probings < 6 mm: Not Significant | No control | Bone gain, significance not analyzed | No control | No control |
| Probings ≥ 6 mm: Significant reduction | ||||||||
| Deppe et al., 2005 [28] Data before surgical interven-tion was used as the baseline in this table | 10,600-nm CO2 (at mean 17 mos) | Increased, significance not analyzed | Increased, significance not analyzed | Reduced, significance not analyzed | Reduced, significance not analyzed | Bone gain, significance not analyzed | Significant bone gain | Air-powder abrasive |
| Deppe et al., 2007 [29] Data before surgical interven-tion was used as the baseline in this table | 10,600-nm CO2 (at mean 37 mos) | Increased, significance not analyzed | Tissue resection gp: Increased, significance not analyzed Augmented bone gp: Decreased, significance not analyzed | Reduced, significance not analyzed | Tissue resection gp: Reduced, significance not analyzed Augmented bone gp: No change, significance not analyzed | Bone gain, significance not analyzed | Air-powder abrasive | |
| Tissue resection gp: Significant bone gain | ||||||||
| Augmented bone gp: No significant bone gain | ||||||||
| Nicholson et al., 2014 [30] | Nd:YAG (at 2 to 48 mos) | Not reported | No control | Not reported | No control | Bone gain, significance not analyzed | No control | No control |
| Norton 2017 [31] | Er:YAG (at 12 mos) | Reduced, significance not analyzed | No control | Reduced, significance not analyzed | No control | Bone gain, significance not analyzed | No control | No control |
| Peng and Tomov 2012 [32] | Er:YAG (at 6 mos) | Significant reduction | Significant reduction | Reduced, significance not analyzed | Reduced, significance not analyzed | Bone loss, significance not analyzed | Less bone loss, significance not analyzed | Mechanical therapy with ultrasonics followed by chemical debridement |
| Renvert et al., 2011 [22] | Er:YAG (at 6 mos) | Significant reduction | Not Significant | Reduced, significance not analyzed | Not Significant | Not Significant bone loss | Not significant bone loss | Air abrasive treatment |
| Romanos et al., 2008 [14] | 10,600-nm CO2 (at mean 27 mos) | Significant reduction | No control | Significant reduction | No control | Bone gain, significance not analyzed | No control | No control |
| Schwarz et al., 2006 [19] | Er:YAG (at 6 and 12 mos) | Significant reduction | Significant reduction (not reported at 12 mos) | Significant reduction | Not Significant | Not Significant (NR) (at 12 mos) | Not Significant (NR) (at 12 mos) | Mechanical debridement with plastic curettes and chlorhexidine pocket irrigation |
| Wang et al., 2020 [33] | Er:YAG (at 24 wks) | Significant reduction | Reduced, not significant | Significant reduction | Significant reduction | Bone gain, significance not analyzed | Not significant bone gain | Same as test group, but no laser therapy |
 | ||||||||
| Range of Variables That May Apply to Laser-Based Studies of Peri-Implantitis Treatment |
|---|
| Study Design |
|
| Investigators |
|
| Patients |
|
| Clinical Parameters |
|
| Radiographic Analysis |
|
| Implant |
|
| Risk of Bias Assessment |
Selection Bias:
|
| Laser Device Information |
|
| Laser Irradiation Parameters |
|
| Laser Treatment Parameters |
|
| Method of Laser Use during Peri-Implantitis Treatment |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ting, M.; Alluri, L.S.C.; Sulewski, J.G.; Suzuki, J.B.; Paes Batista da Silva, A. Laser Treatment of Peri-Implantitis: A Systematic Review of Radiographic Outcomes. Dent. J. 2022, 10, 20. https://doi.org/10.3390/dj10020020
Ting M, Alluri LSC, Sulewski JG, Suzuki JB, Paes Batista da Silva A. Laser Treatment of Peri-Implantitis: A Systematic Review of Radiographic Outcomes. Dentistry Journal. 2022; 10(2):20. https://doi.org/10.3390/dj10020020
Chicago/Turabian StyleTing, Miriam, Leela Subhashini C. Alluri, John G. Sulewski, Jon B. Suzuki, and Andre Paes Batista da Silva. 2022. "Laser Treatment of Peri-Implantitis: A Systematic Review of Radiographic Outcomes" Dentistry Journal 10, no. 2: 20. https://doi.org/10.3390/dj10020020
APA StyleTing, M., Alluri, L. S. C., Sulewski, J. G., Suzuki, J. B., & Paes Batista da Silva, A. (2022). Laser Treatment of Peri-Implantitis: A Systematic Review of Radiographic Outcomes. Dentistry Journal, 10(2), 20. https://doi.org/10.3390/dj10020020