
An In-Vitro Evaluation of Articulation Accuracy for Digitally Milled Models vs. Conventional Gypsum Casts


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chun, J.; Pae, A.; Kim, S. Polymerization Shrinkage Strain of Interocclusal Recording Materials. Dent. Mater. 2009, 25, 115–120. [Google Scholar] [CrossRef]
- Vergos, V.K.; Tripodakis, A.-P.D. Evaluation of Vertical Accuracy of Interocclusal Records. Int. J. Prosthodont. 2003, 16, 365–368. [Google Scholar]
- Lassila, V. Comparison of Five Interocclusal Recording Materials. J. Prosthet. Dent. 1986, 55, 215–218. [Google Scholar] [CrossRef]
- Corso, M.; Abanomy, A.; Di Canzio, J.; Zurakowski, D.; Morgano, S.M. The Effect of Temperature Changes on the Dimensional Stability of Polyvinyl Siloxane and Polyether Impression Materials. J. Prosthet. Dent. 1998, 79, 626–631. [Google Scholar] [CrossRef]
- Millstein, P.L.; Clark, R.E. Differential Accuracy of Silicone-Body and Self-Curing Resin Interocclusal Records and Associated Weight Loss. J. Prosthet. Dent. 1981, 46, 380–384. [Google Scholar] [CrossRef]
- Millstein, P.L.; Clark, R.E.; Myerson, R.L. Differential Accuracy of Silicone-Body Interocclusal Records and Associated Weight Loss Due to Volatiles. J. Prosthet. Dent. 1975, 33, 649–654. [Google Scholar] [CrossRef]
- Strohaver, R.A. A Comparison of Articulator Mountings Made with Centric Relation and Myocentric Position Records. J. Prosthet. Dent. 1972, 28, 379–390. [Google Scholar] [CrossRef]
- Freilich, M.A.; Altieri, J.V.; Wahle, J.J. Principles for Selecting Interocclusal Records for Articulation of Dentate and Partially Dentate Casts. J. Prosthet. Dent. 1992, 68, 361–367. [Google Scholar] [CrossRef]
- Naumovski, B.; Kapushevska, B. Dimensional Stability and Acuracy of Silicone—Based Impression Materials Using Different Impression Techniques—A Literature Review. Prilozi 2017, 38, 131–138. [Google Scholar] [CrossRef] [Green Version]
- Thongthammachat, S.; Moore, B.K.; Barco, M.T.; Hovijitra, S.; Brown, D.T.; Andres, C.J. Dimensional Accuracy of Dental Casts: Influence of Tray Material, Impression Material, and Time. J. Prosthodont. 2002, 11, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Macarthur, R.X.; Gallucci, G.O. An Evaluation of Student and Clinician Perception of Digital and Conventional Implant Impressions. J. Prosthet. Dent. 2013, 110, 420–423. [Google Scholar] [CrossRef]
- Lee, S.J.; Gallucci, G.O. Digital vs. Conventional Implant Impressions: Efficiency Outcomes. Clin. Oral Implants Res. 2013, 24, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Jamjoom, F.Z.; Le, T.; Radics, A.; Gallucci, G.O. A Clinical Study Comparing Digital Scanning and Conventional Impression Making for Implant-Supported Prostheses: A Crossover Clinical Trial. J. Prosthet. Dent. 2021. [Google Scholar] [CrossRef] [PubMed]
- Alves de Carvalho, I.F.; Santos Marques, T.M.; Araújo, F.M.; Azevedo, L.F.; Donato, H.; Correia, A. Clinical Performance of CAD/CAM Tooth-Supported Ceramic Restorations: A Systematic Review. Int J. Periodontics Restor. Dent. 2018, 38, e68–e78. [Google Scholar] [CrossRef] [PubMed]
- Wittneben, J.-G.; Wright, R.F.; Weber, H.-P.; Gallucci, G.O. A Systematic Review of the Clinical Performance of CAD/CAM Single-Tooth Restorations. Int. J. Prosthodont. 2009, 22, 466–471. [Google Scholar]
- Zimmermann, M.; Ender, A.; Attin, T.; Mehl, A. Accuracy of Buccal Scan Procedures for the Registration of Habitual Intercuspation. Oper. Dent. 2018, 43, 573–580. [Google Scholar] [CrossRef]
- Iwauchi, Y.; Tanaka, S.; Kamimura-Sugimura, E.; Baba, K. Clinical Evaluation of the Precision of Interocclusal Registration by Using Digital and Conventional Techniques. J. Prosthet. Dent. 2021. [Google Scholar] [CrossRef]
- Ries, J.M.; Grünler, C.; Wichmann, M.; Matta, R.-E. Three-Dimensional Analysis of the Accuracy of Conventional and Completely Digital Interocclusal Registration Methods. J. Prosthet. Dent. 2021. [Google Scholar] [CrossRef]
- Millstein, P.; Maya, A. An Evaluation of Occlusal Contact Marking Indicators. A Descriptive Quantitative Method. J. Am. Dent. Assoc. 2001, 132, 1280–1286, quiz 1319. [Google Scholar] [CrossRef]
- Yamamura, M.; Takahashi, A.; Aoki, H.; Takeuchi, N.; Endo, Y.; Tamaki, K.; Sano, Y.; Fujiwara, S.; Fujita, T.; Kusunoki, S. A study on display and accuracy of occlusal contacts by means of T-Scan System. Kanagawa Shigaku 1990, 25, 236–241. [Google Scholar]
- Cerna, M.; Ferreira, R.; Zaror, C.; Navarro, P.; Sandoval, P. In Vitro Evaluation of T-Scan®III through Study of the Sensels. Cranio 2015, 33, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Maness, W.L.; Podoloff, R. Distribution of Occlusal Contacts in Maximum Intercuspation. J. Prosthet. Dent. 1989, 62, 238–242. [Google Scholar] [CrossRef]
- Reza Moini, M.; Neff, P.A. Reproducibility of Occlusal Contacts Utilizing a Computerized Instrument. Quintessence Int. 1991, 22, 357–360. [Google Scholar]
- Garrido García, V.C.; García Cartagena, A.; González Sequeros, O. Evaluation of Occlusal Contacts in Maximum Intercuspation Using the T-Scan System. J. Oral Rehabilit. 1997, 24, 899–903. [Google Scholar] [CrossRef] [PubMed]
- Koos, B.; Godt, A.; Schille, C.; Göz, G. Precision of an Instrumentation-Based Method of Analyzing Occlusion and Its Resulting Distribution of Forces in the Dental Arch. J. Orofac. Orthop. 2010, 71, 403–410. [Google Scholar] [CrossRef]
- Qadeer, S.; Özcan, M.; Edelhoff, D.; Van Pelt, H. Accuracy, Reliability and Clinical Implications of Static Compared to Quantifiable Occlusal Indicators. Eur. J. Prosthodont. Restor. Dent. 2021, 29, 130–141. [Google Scholar] [CrossRef]
- Seelbach, P.; Brueckel, C.; Wöstmann, B. Accuracy of Digital and Conventional Impression Techniques and Workflow. Clin. Oral Investig. 2013, 17, 1759–1764. [Google Scholar] [CrossRef]
- Tsirogiannis, P.; Reissmann, D.R.; Heydecke, G. Evaluation of the Marginal Fit of Single-Unit, Complete-Coverage Ceramic Restorations Fabricated after Digital and Conventional Impressions: A Systematic Review and Meta-Analysis. J. Prosthet. Dent. 2016, 116, 328–335.e2. [Google Scholar] [CrossRef]
- Tabesh, M.; Nejatidanesh, F.; Savabi, G.; Davoudi, A.; Savabi, O.; Mirmohammadi, H. Marginal Adaptation of Zirconia Complete-Coverage Fixed Dental Restorations Made from Digital Scans or Conventional Impressions: A Systematic Review and Meta-Analysis. J. Prosthet. Dent. 2021, 125, 603–610. [Google Scholar] [CrossRef]
- Edher, F.; Hannam, A.G.; Tobias, D.L.; Wyatt, C.C.L. The Accuracy of Virtual Interocclusal Registration during Intraoral Scanning. J. Prosthet. Dent. 2018, 120, 904–912. [Google Scholar] [CrossRef]
- Abdulateef, S.; Edher, F.; Hannam, A.G.; Tobias, D.L.; Wyatt, C.C.L. Clinical Accuracy and Reproducibility of Virtual Interocclusal Records. J. Prosthet. Dent. 2020, 124, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Vögtlin, C.; Schulz, G.; Jäger, K.; Müller, B. Comparing the Accuracy of Master Models Based on Digital Intra-Oral Scanners with Conventional Plaster Casts. Phys. Med. 2016, 1, 20–26. [Google Scholar] [CrossRef] [Green Version]
- Abduo, J. Accuracy of Casts Produced from Conventional and Digital Workflows: A Qualitative and Quantitative Analyses. J. Adv. Prosthodont. 2019, 11, 138–146. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Master | Conventional | Digital | p Values | |
|---|---|---|---|---|
| #11 | 163.27 ± 36.92 | 157.60 ± 37.70 | 208.63 ± 19.23 | p < 0.001 * |
| #12 | 312.23 ± 89.99 | 281.20 ± 23.43 | 279.13 ± 84.96 | p = 0.148 |
| #14 | 588.63 ± 97.78 | 634.77 ± 140.52 | 612 ± 154.94 | p = 0.411 |
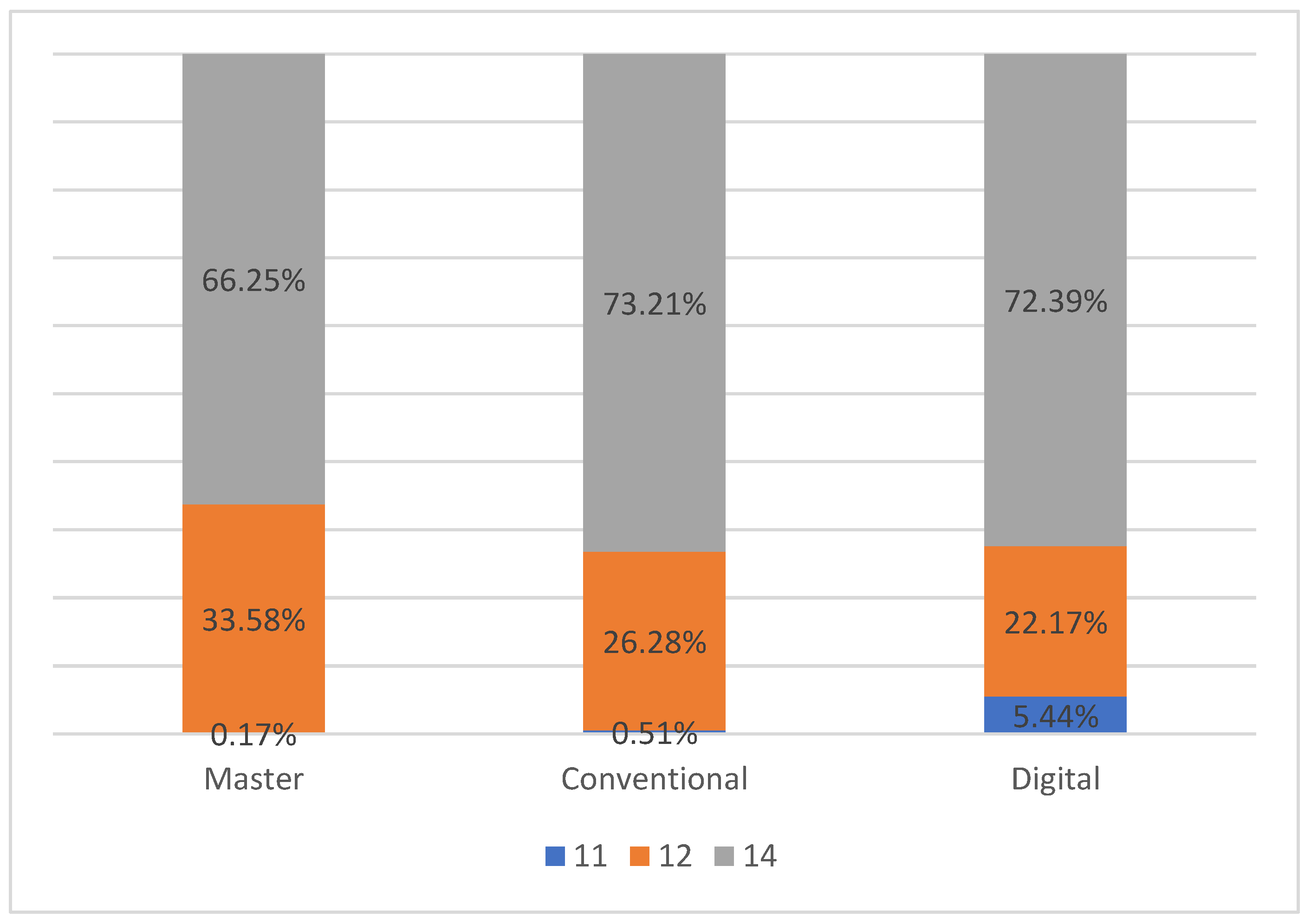
| Master | Conventional | Digital | |
|---|---|---|---|
| #11 | 0.17% | 0.51% | 5.44% |
| #12 | 33.58% | 26.28% | 22.17% |
| #14 | 66.25% | 73.21% | 72.39% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.D.; Gallucci, G.O.; Lee, S.J. An In-Vitro Evaluation of Articulation Accuracy for Digitally Milled Models vs. Conventional Gypsum Casts. Dent. J. 2022, 10, 11. https://doi.org/10.3390/dj10010011
Lee JD, Gallucci GO, Lee SJ. An In-Vitro Evaluation of Articulation Accuracy for Digitally Milled Models vs. Conventional Gypsum Casts. Dentistry Journal. 2022; 10(1):11. https://doi.org/10.3390/dj10010011
Chicago/Turabian StyleLee, Jason D., German O. Gallucci, and Sang J. Lee. 2022. "An In-Vitro Evaluation of Articulation Accuracy for Digitally Milled Models vs. Conventional Gypsum Casts" Dentistry Journal 10, no. 1: 11. https://doi.org/10.3390/dj10010011
APA StyleLee, J. D., Gallucci, G. O., & Lee, S. J. (2022). An In-Vitro Evaluation of Articulation Accuracy for Digitally Milled Models vs. Conventional Gypsum Casts. Dentistry Journal, 10(1), 11. https://doi.org/10.3390/dj10010011