Hyperspectral Imaging Combined with Deep Learning to Detect Ischemic Necrosis in Small Intestinal Tissue

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
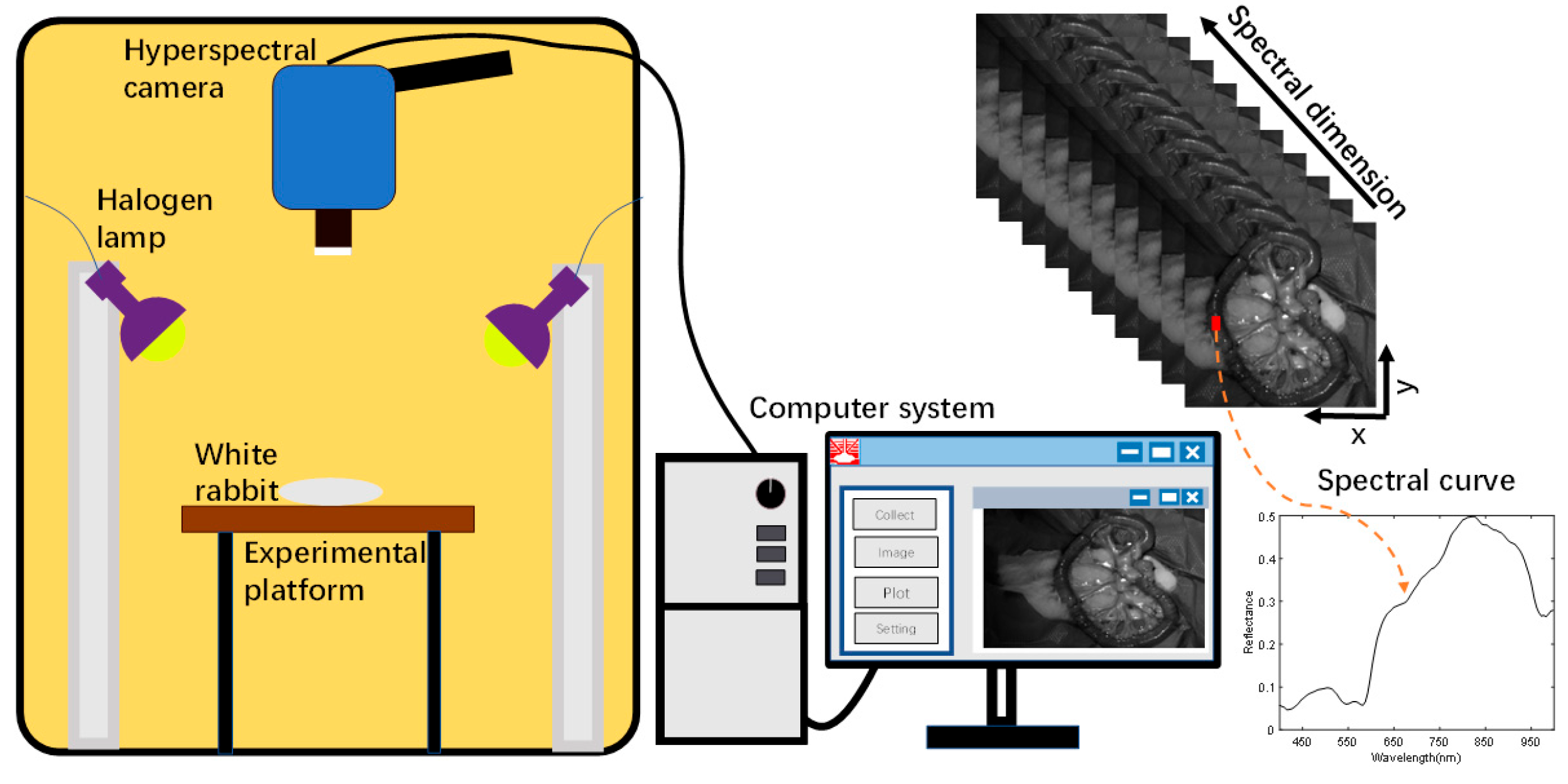
2.1. Small Intestine Tissue HSI Dataset
2.2. Preprocessing
2.3. Deep Learning
2.4. Experiment Description
2.5. Metrics
3. Results
3.1. Case1: 1D-CNN
3.2. Case2: 2D-CNN
3.3. Case3: 3D-CNN
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Emile, S.H. Predictive factors for intestinal transmural necrosis in patients with acute mesenteric ischemia. World J. Surg. 2018, 42, 2364–2372. [Google Scholar] [CrossRef]
- Luther, B.; Mamopoulos, A.; Lehmann, C.; Klar, E. The ongoing challenge of acute mesenteric ischemia. Visc. Med. 2018, 34, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Akbari, H.; Kosugi, Y.; Kojima, K.; Tanaka, N. Detection and analysis of the intestinal ischemia using visible and invisible hyperspectral imaging. IEEE Trans. Biomed. Eng. 2010, 57, 2011–2017. [Google Scholar] [CrossRef] [PubMed]
- Yasuhara, H. Acute mesenteric ischemia: The challenge of gastroenterology. Surg. Today 2005, 35, 185–195. [Google Scholar] [CrossRef]
- Sinha, D.; Kale, S.; Kundaragi, N.G.; Sharma, S. Mesenteric ischemia: A radiologic perspective. Abdom. Radiol. 2022, 47, 1514–1528. [Google Scholar] [CrossRef]
- Wyers, M.C. Acute mesenteric ischemia: Diagnostic approach and surgical treatment. Semin. Vasc. Surg. 2010, 23, 9–20. [Google Scholar] [CrossRef]
- Mehdorn, M.; Köhler, H.; Rabe, S.M.; Niebisch, S.; Lyros, O.; Chalopin, C.; Gockel, I.; Jansen-Winkeln, B. Hyperspectral imaging (HSI) in acute mesenteric ischemia to detect intestinal perfusion deficits. J. Surg. Res. 2020, 254, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Ambe, P.C.; Kang, K.; Papadakis, M.; Zirngibl, H. Can the preoperative serum lactate level predict the extent of bowel ischemia in patients presenting to the emergency department with acute mesenteric ischemia? Biomed. Res. Int. 2017, 2017, 8038796. [Google Scholar] [CrossRef]
- Wang, Y.; Tiusaba, L.; Jacobs, S.; Saruwatari, M.; Ning, B.; Levitt, M.; Sandler, A.D.; Nam, S.-H.; Kang, J.U.; Cha, J. Unsupervised and quantitative intestinal ischemia detection using conditional adversarial network in multimodal optical imaging. J. Med. Imaging 2022, 9, 064502. [Google Scholar] [CrossRef]
- Lu, G.; Fei, B. Medical hyperspectral imaging: A review. J. Biomed. Opt. 2014, 19, 010901. [Google Scholar] [CrossRef] [PubMed]
- Jansen-Winkeln, B.; Holfert, N.; Köhler, H.; Moulla, Y.; Takoh, J.; Rabe, S.; Mehdorn, M.; Barberio, M.; Chalopin, C.; Neumuth, T. Determination of the transection margin during colorectal resection with hyperspectral imaging (HSI). Int. J. Color. Dis. 2019, 34, 731–739. [Google Scholar] [CrossRef]
- Jia, J.; Wang, Y.; Chen, J.; Guo, R.; Shu, R.; Wang, J. Status and application of advanced airborne hyperspectral imaging technology: A review. Infrared Phys. Technol. 2020, 104, 103115. [Google Scholar] [CrossRef]
- Saha, D.; Manickavasagan, A. Machine learning techniques for analysis of hyperspectral images to determine quality of food products: A review. Curr. Res. Food Sci. 2021, 4, 28–44. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Deng, L.; Liu, X.; Zhu, L. Application of UAV-based multi-angle hyperspectral remote sensing in fine vegetation classification. Remote Sens. 2019, 11, 2753. [Google Scholar] [CrossRef]
- Lugli, F.; Sciutto, G.; Oliveri, P.; Malegori, C.; Prati, S.; Gatti, L.; Silvestrini, S.; Romandini, M.; Catelli, E.; Casale, M. Near-infrared hyperspectral imaging (NIR-HSI) and normalized difference image (NDI) data processing: An advanced method to map collagen in archaeological bones. Talanta 2021, 226, 122126. [Google Scholar] [CrossRef] [PubMed]
- Ozdemir, A.; Polat, K. Deep learning applications for hyperspectral imaging: A systematic review. J. Inst. Electron. Comput. 2020, 2, 39–56. [Google Scholar] [CrossRef]
- Notarstefano, V.; Sabbatini, S.; Conti, C.; Pisani, M.; Astolfi, P.; Pro, C.; Rubini, C.; Vaccari, L.; Giorgini, E. Investigation of human pancreatic cancer tissues by Fourier Transform Infrared Hyperspectral Imaging. J. Biophoton. 2020, 13, e201960071. [Google Scholar] [CrossRef]
- Daukantas, P. Hyperspectral imaging meets biomedicine. Opt. Photonics News 2020, 31, 32–39. [Google Scholar] [CrossRef]
- Yoon, J. Hyperspectral imaging for clinical applications. Biochip J. 2022, 16, 1–12. [Google Scholar] [CrossRef]
- Promny, D.; Aich, J.; Püski, T.; Edo, A.M.; Reichert, B.; Billner, M. Evaluation of hyperspectral imaging as a modern aid in clinical assessment of burn wounds of the upper extremity. Burns 2022, 48, 615–622. [Google Scholar] [CrossRef]
- Sun, L.; Zhou, M.; Li, Q.; Hu, M.; Wen, Y.; Zhang, J.; Lu, Y.; Chu, J. Diagnosis of cholangiocarcinoma from microscopic hyperspectral pathological dataset by deep convolution neural networks. Methods 2022, 202, 22–30. [Google Scholar] [CrossRef]
- Wang, Q.; Wang, J.; Zhou, M.; Li, Q.; Wang, Y. Spectral-spatial feature-based neural network method for acute lymphoblastic leukemia cell identification via microscopic hyperspectral imaging technology. Biomed. Opt. Express 2017, 8, 3017–3028. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Du, J.; Zhang, Z.; Wang, Q. Tumor tissue classification based on micro-hyperspectral technology and deep learning. Biomed. Opt. Express 2019, 10, 6370–6389. [Google Scholar] [CrossRef] [PubMed]
- Jena, P.V.; Gravely, M.; Cupo, C.; Safaee, M.M.; Roxbury, D.; Heller, D.A. Hyperspectral counting of multiplexed nanoparticle emitters in single cells and organelles. ACS Nano 2022, 16, 3092–3104. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Tahiliani, S.; Neu-Baker, N.M.; Brenner, S.A. Hyperspectral microscopy as an analytical tool for nanomaterials. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2015, 7, 565–579. [Google Scholar] [CrossRef] [PubMed]
- Pham, Q.T.; Liou, N.-S. The development of on-line surface defect detection system for jujubes based on hyperspectral images. Comput. Electron. Agric. 2022, 194, 106743. [Google Scholar] [CrossRef]
- Sarker, I.H. Deep learning: A comprehensive overview on techniques, taxonomy, applications and research directions. SN Comput. Sci. 2021, 2, 420. [Google Scholar] [CrossRef]
- Hu, X.; Xie, C.; Fan, Z.; Duan, Q.; Zhang, D.; Jiang, L.; Wei, X.; Hong, D.; Li, G.; Zeng, X. Hyperspectral anomaly detection using deep learning: A review. Remote Sens. 2022, 14, 1973. [Google Scholar] [CrossRef]
- Zhang, L.; Huang, D.; Chen, X.; Zhu, L.; Chen, X.; Xie, Z.; Huang, G.; Gao, J.; Shi, W.; Cui, G. Visible near-infrared hyperspectral imaging and supervised classification for the detection of small intestinal necrosis tissue in vivo. Biomed. Opt. Express 2022, 13, 6061–6080. [Google Scholar] [CrossRef]
- Lu, G.; Little, J.V.; Wang, X.; Zhang, H.; Patel, M.R.; Griffith, C.C.; El-Deiry, M.W.; Chen, A.Y.; Fei, B. Detection of Head and Neck Cancer in Surgical Specimens Using Quantitative Hyperspectral ImagingHyperspectral Imaging for Head and Neck Cancer Detection. Clin. Cancer Res. 2017, 23, 5426–5436. [Google Scholar] [CrossRef]
- Mũnoz-Marí, J.; Bovolo, F.; Gómez-Chova, L.; Bruzzone, L.; Camp-Valls, G. Semisupervised one-class support vector machines for classification of remote sensing data. IEEE Trans. Geosci. Remote Sens. 2010, 48, 3188–3197. [Google Scholar] [CrossRef]
- Zhang, L.; Huang, D.; Chen, X.; Zhu, L.; Xie, Z.; Chen, X.; Cui, G.; Zhou, Y.; Huang, G.; Shi, W. Discrimination between normal and necrotic small intestinal tissue using hyperspectral imaging and unsupervised classification. J. Biophoton. 2023, e202300020. [Google Scholar] [CrossRef]
- Ortega, S.; Halicek, M.; Fabelo, H.; Camacho, R.; Plaza, M.d.l.L.; Godtliebsen, F.; Callicó, G.M.; Fei, B. Hyperspectral imaging for the detection of glioblastoma tumor cells in H&E slides using convolutional neural networks. Sensors 2020, 20, 1911. [Google Scholar]
- Li, X.; Jiang, H.; Jiang, X.; Shi, M. Identification of geographical origin of Chinese chestnuts using hyperspectral imaging with 1D-CNN algorithm. Agriculture 2021, 11, 1274. [Google Scholar] [CrossRef]
- Hao, Q.; Pei, Y.; Zhou, R.; Sun, B.; Sun, J.; Li, S.; Kang, X. Fusing multiple deep models for in vivo human brain hyperspectral image classification to identify glioblastoma tumor. IEEE Trans. Instrum. Meas. 2021, 70, 1–14. [Google Scholar] [CrossRef]
- Fırat, H.; Asker, M.E.; Bayindir, M.İ.; Hanbay, D. Spatial-spectral classification of hyperspectral remote sensing images using 3D CNN based LeNet-5 architecture. Infrared Phys. Technol. 2022, 127, 104470. [Google Scholar] [CrossRef]
- Lu, G.; Wang, D.; Qin, X.; Halig, L.; Muller, S.; Zhang, H.; Chen, A.; Pogue, B.W.; Chen, Z.G.; Fei, B. Framework for hyperspectral image processing and quantification for cancer detection during animal tumor surgery. J. Biomed. Opt. 2015, 20, 126012. [Google Scholar] [CrossRef]
- Kumar, B.; Dikshit, O.; Gupta, A.; Singh, M.K. Feature extraction for hyperspectral image classification: A review. Int. J. Remote Sens. 2020, 41, 6248–6287. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample | Number of Pixels | ||
|---|---|---|---|
| Normal | Necrosis | Sum | |
| S1 | 10,397 | 10,821 | 21,728 |
| S2 | 11,635 | 10,806 | 22,441 |
| S3 | 5059 | 7531 | 12,590 |
| S4 | 5383 | 4563 | 9946 |
| S5 | 8493 | 8239 | 16,732 |
| S6 | 9859 | 11,487 | 21,346 |
| S7 | 8917 | 7622 | 16,539 |
| Total | 59,743 | 61,069 | 120,812 |
| Sample | OA (%) | Sensitivity (%) | Specificity (%) | Kappa (%) |
|---|---|---|---|---|
| S1 | 99.31 | 99.90 | 98.81 | 98.61 |
| S2 | 96.65 | 94.00 | 99.74 | 93.29 |
| S3 | 84.34 | 69.07 | 99.15 | 68.53 |
| S4 | 99.96 | 99.98 | 99.94 | 99.92 |
| S5 | 66.09 | 61.98 | 72.15 | 32.64 |
| S6 | 57.83 | 38.02 | 76.24 | 14.44 |
| S7 | 90.50 | 99.82 | 80.79 | 80.92 |
| Ave | 84.95 | 80.40 | 89.55 | 69.77 |
| Sample | OA (%) | Sensitivity (%) | Specificity (%) | Kappa (%) |
|---|---|---|---|---|
| S1 | 99.52 | 99.30 | 99.71 | 99.04 |
| S2 | 97.33 | 95.18 | 99.84 | 94.66 |
| S3 | 52.38 | 61.00 | 43.44 | 4.45 |
| S4 | 99.99 | 99.97 | 100.00 | 99.97 |
| S5 | 41.43 | 4.56 | 95.93 | 0.40 |
| S6 | 99.90 | 100.00 | 99.80 | 99.79 |
| S7 | 99.58 | 99.54 | 99.62 | 99.16 |
| Ave | 84.30 | 79.94 | 91.19 | 71.07 |
| Sample | OA (%) | Sensitivity (%) | Specificity (%) | Kappa (%) |
|---|---|---|---|---|
| S1 | 99.76 | 99.63 | 99.88 | 99.52 |
| S2 | 96.21 | 92.97 | 99.99 | 92.42 |
| S3 | 89.48 | 79.40 | 99.95 | 79.04 |
| S4 | 99.99 | 99.97 | 100.00 | 99.97 |
| S5 | 47.37 | 11.95 | 99.73 | 9.66 |
| S6 | 99.69 | 100.00 | 99.40 | 99.37 |
| S7 | 94.69 | 89.59 | 99.99 | 89.39 |
| Ave | 89.60 | 81.93 | 99.85 | 81.34 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, L.; Zhou, Y.; Huang, D.; Zhu, L.; Chen, X.; Xie, Z.; Cui, G.; Huang, G.; Ali, S.; Chen, X. Hyperspectral Imaging Combined with Deep Learning to Detect Ischemic Necrosis in Small Intestinal Tissue. Photonics 2023, 10, 708. https://doi.org/10.3390/photonics10070708
Zhang L, Zhou Y, Huang D, Zhu L, Chen X, Xie Z, Cui G, Huang G, Ali S, Chen X. Hyperspectral Imaging Combined with Deep Learning to Detect Ischemic Necrosis in Small Intestinal Tissue. Photonics. 2023; 10(7):708. https://doi.org/10.3390/photonics10070708
Chicago/Turabian StyleZhang, Lechao, Yao Zhou, Danfei Huang, Libin Zhu, Xiaoqing Chen, Zhonghao Xie, Guihua Cui, Guangzao Huang, Shujat Ali, and Xiaojing Chen. 2023. "Hyperspectral Imaging Combined with Deep Learning to Detect Ischemic Necrosis in Small Intestinal Tissue" Photonics 10, no. 7: 708. https://doi.org/10.3390/photonics10070708
APA StyleZhang, L., Zhou, Y., Huang, D., Zhu, L., Chen, X., Xie, Z., Cui, G., Huang, G., Ali, S., & Chen, X. (2023). Hyperspectral Imaging Combined with Deep Learning to Detect Ischemic Necrosis in Small Intestinal Tissue. Photonics, 10(7), 708. https://doi.org/10.3390/photonics10070708