Photostress Recovery Time after Flash-Lighting Is Increased in Myopic Eyes



Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Experimental System
2.3. Measurement Procedure
2.4. Graphical and Statistical Analysis
3. Results
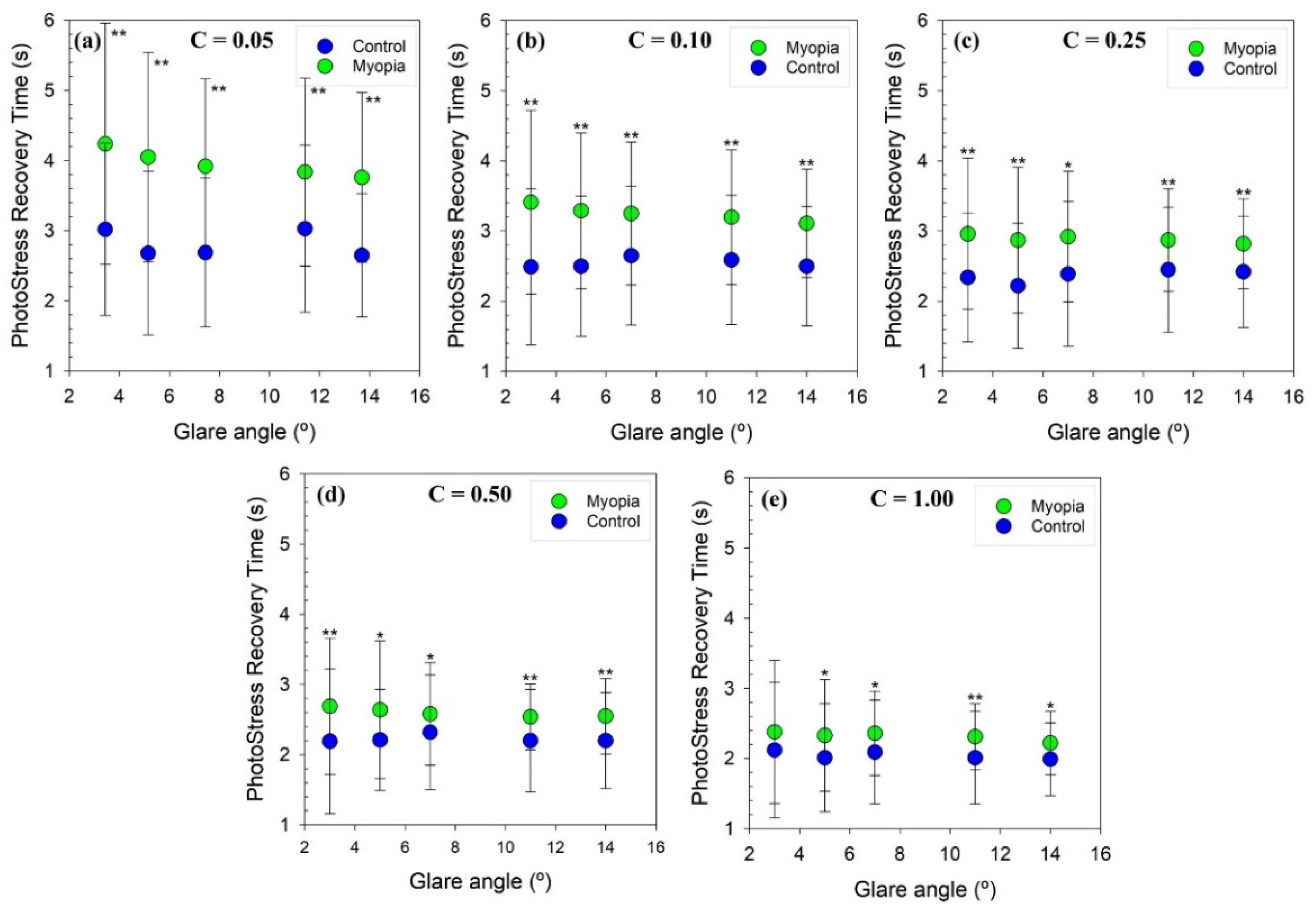
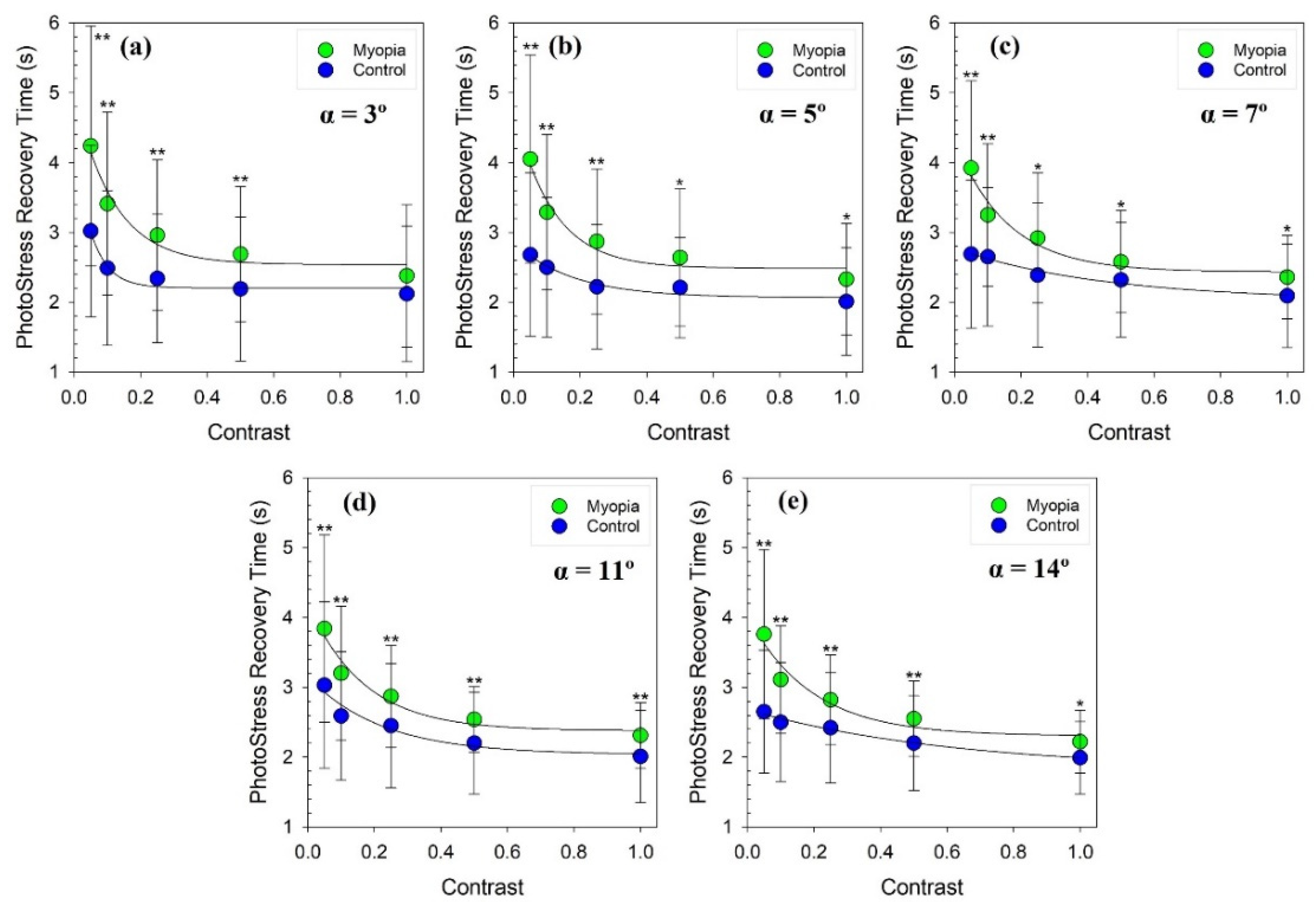
3.1. PSRT as a Function of the Stimuli Contrast and Glare Angle for Myopic and Emmetropic Groups
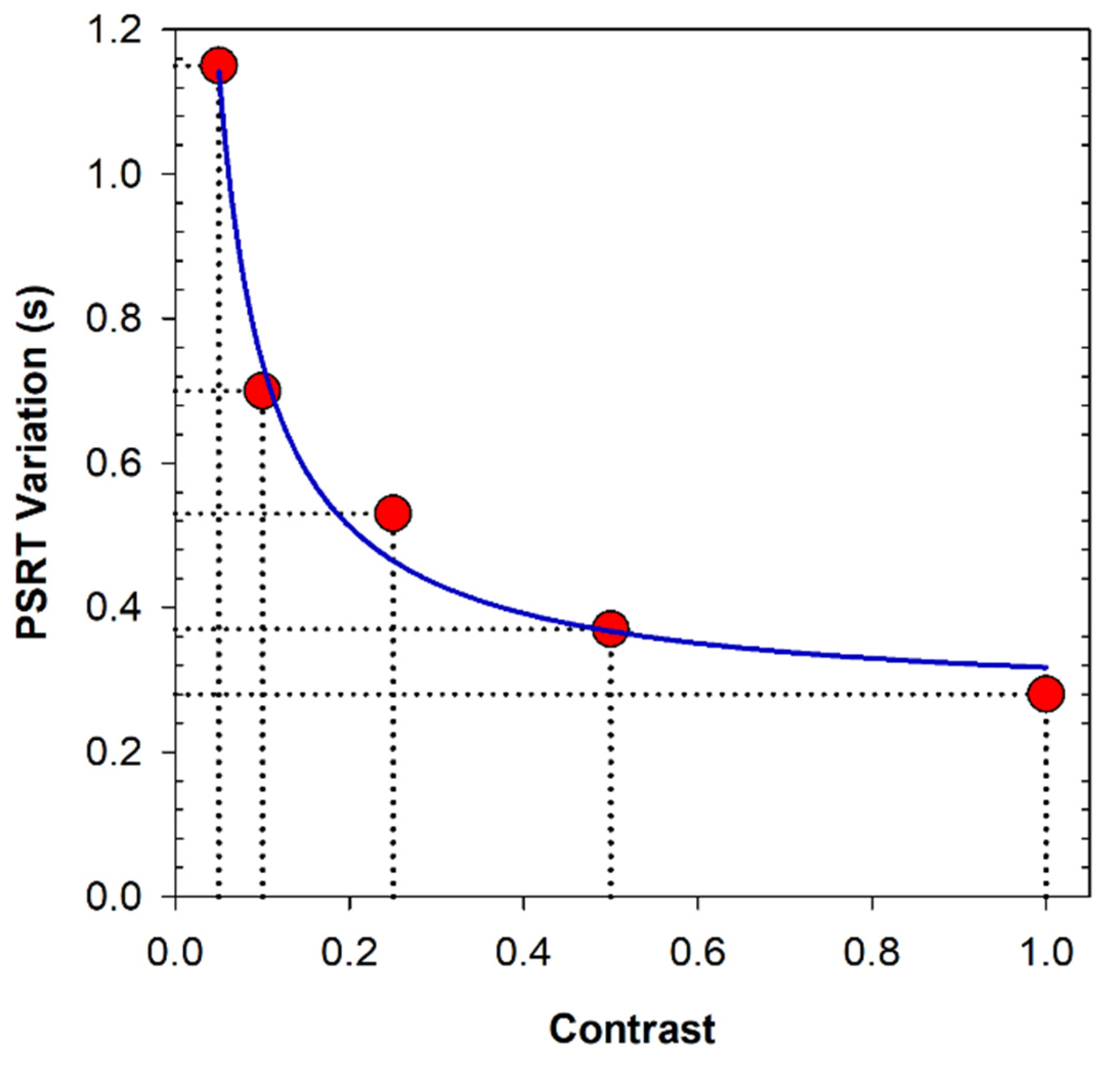
3.2. Myopia and Variation in PSRT
4. Discussion and Conclusions
4.1. Basics of Altered PSRT in Myopic Eyes
4.1.1. Factors Caused by a Different Retinal Exposure
4.1.2. Factors Caused by Different Visual Quality
4.2. PSRT Comparison with Other Studies
4.3. Limitations and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pan, C.W.; Ramamurthy, D.; Saw, S.M. Worldwide prevalence and risk factors for myopia. Ophthalmic Physiol. Opt. 2012, 32, 3–16. [Google Scholar] [CrossRef]
- Jonas, J.B.; Wang, Y.X.; Dong, L.; Guo, Y.; Panda-Jonas, S. Advances in myopia research anatomical findings in highly myopic eyes. Eye Vis. 2020, 7, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Heine, L. Beiträge zur Anatomie des myopischen Auges. Arch. Augenheilk 1899, 38, 277–290. [Google Scholar]
- Norman, R.E.; Flanagan, J.G.; Rausch, S.M.; Sigal, I.A.; Tertinegg, I.; Eilaghi, A.; Portnoy, S.; Sled, J.G.; Ethier, C.R. Dimensions of the human sclera: Thickness measurement and regional changes with axial length. Exp. Eye Res. 2010, 90, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Vurgese, S.; Panda-Jonas, S.; Jonas, J.B. Scleral thickness in human eyes. PLoS ONE 2012, 7, e29692. [Google Scholar] [CrossRef]
- Jonas, J.B.; Ohno-Matsui, K.; Holbach, L.; Panda-Jonas, S. Retinal pigment epithelium cell density in relationship to axial length in human eyes. Acta Ophthalmol. 2017, 95, e22–e28. [Google Scholar] [CrossRef]
- Coletta, N.J.; Watson, T. Effect of myopia on visual acuity measured with laser interference fringes. Vis. Res. 2006, 46, 636–651. [Google Scholar] [CrossRef]
- Strang, N.C.; Winn, B.; Bradley, A. The role of neural and optical factors in limiting visual resolution in myopia. Vis. Res. 1998, 38, 1713–1721. [Google Scholar] [CrossRef]
- Liou, S.-W.; Chiu, C.-J. Myopia and contrast sensitivity function. Curr. Eye Res. 2001, 22, 81–84. [Google Scholar] [CrossRef]
- Wolsley, C.J.; Saunders, K.J.; Silvestri, G.; Anderson, R.S. Investigation of changes in the myopic retina using multifocal electroretinograms, optical coherence tomography and peripheral resolution acuity. Vis. Res. 2008, 48, 1554–1561. [Google Scholar] [CrossRef]
- Choi, S.S.; Garner, L.F.; Enoch, J.M. The relationship between the Stiles-Crawford effect of the first kind (SCE-I) and myopia. Ophthalmic Physiol. Opt. 2003, 23, 465–472. [Google Scholar] [CrossRef] [PubMed]
- Stapley, V.; Anderson, R.S.; Saunders, K.J.; Mulholland, P.J. Altered spatial summation optimizes visual function in axial myopia. Sci. Rep. 2020, 10, 12179. [Google Scholar] [CrossRef]
- Lovasik, J.V. An electrophysiological investigation of the macular photostress test. Investig. Ophthalmol. Vis. Sci. 1983, 24, 437–441. [Google Scholar]
- Zabriskie, N.A.; Kardon, R.H. The pupil photostress test. Ophthalmology 1994, 101, 1122–1130. [Google Scholar] [CrossRef]
- Ito, Y.; Horiguchi, M.; Miyake, Y.; Awaya, S. Extrafoveal photostress recovery testing with a scanning laser ophthalmoscope. Jpn. J. Ophthalmol. 1997, 41, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, H.; Davies, L.N.; Eperjesi, F. Reliability, normative data, and the effect of age-related macular disease on the Eger Macular Stressometer photostress recovery time. Ophthalmic Physiol. Opt. 2004, 24, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Collins, M.; Brown, B. Glare recovery and its relation to other clinical findings in age related maculopathy. Clin. Vis. Sci. 1989, 4, 155–163. [Google Scholar]
- Collins, M.; Brown, B. Glare recovery and age related maculopathy. Clin. Vis. Sci. 1989, 4, 145–153. [Google Scholar]
- Midena, E.; Degli Angeli, C.; Blarzino, M.C.; Valenti, M.; Segato, T. Macular function impairment in eyes with early age-related macular degeneration. Investig. Ophthalmol. Vis. Sci. 1997, 38, 469–477. [Google Scholar]
- Glaser, J.S.; Savino, P.J.; Sumers, K.D.; McDonald, S.A.; Knighton, R.W. The photostress recovery test in the clinical assessment of visual function. Am. J. Ophthalmol. 1977, 83, 255–260. [Google Scholar] [CrossRef]
- Wu, G.; Weiter, J.J.; Santos, S.; Ginsburg, L.; Villalobos, R. The macular photostress test in diabetic retinopathy and age-related macular degeneration. Arch. Ophthalmol. 1990, 108, 1556–1558. [Google Scholar] [CrossRef] [PubMed]
- Sherman, M.D.; Henkind, P. Photostress recovery in chronic open angle glaucoma. Br. J. Ophthal. 1988, 72, 641–645. [Google Scholar] [CrossRef] [PubMed]
- Baptista, A.M.G.; Sousa, R.; Rocha, F.A.S.Q.; Fernandes, P.S.; Macedo, A.F. The macular photostress test in diabetes, glaucoma, and cataract. Proc. SPIE 2013, 8785, 1740–1745. [Google Scholar]
- Boadi-Kusi, S.B.; Austin, E.; Abu Od, S.L.; Od, S.H.; Od, E.K.A.M. Disability glare and nighttime driving performance among commercial drivers in Ghana. J. Occup. Health 2021, 63, e12279. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, J.D.; Wallstrom, G.; Narayanan, D.; Welch, D.; Abelson, M.B. An Alternative Psychophysical Diagnostic Indicator of the Aging Eye. J. Ophthalmol. 2019, 2019, 2036192. [Google Scholar] [CrossRef]
- Hammond, B.R. Attenuating photostress and glare disability in pseudophakic patients through the addition of a short-wave absorbing filter. J. Ophthalmol. 2015, 2015, 60763. [Google Scholar] [CrossRef]
- Hammond, B.R.; Fletcher, L.M.; Roos, F.; Wittwer, J.; Schalch, W. A double-blind, placebo-controlled study on the effects of lutein and zeaxanthin on photostress recovery, glare disability, and chromatic contrast. Investig. Ophthalmol. Vis. Sci. 2014, 55, 8583–8589. [Google Scholar] [CrossRef]
- Margrain, T.H.; Thomson, D. Sources of variability in the clinical photostress test. Ophthalmic Physiol. Opt. 2002, 22, 61–67. [Google Scholar] [CrossRef]
- Mashige, K. Night vision and glare vision thresholds and recovery time in myopic and hyperopic eyes. S. Afr. Optom. 2010, 69, 132–139. [Google Scholar] [CrossRef]
- Avila, F.; Casado, P. Optical instrument for the study of time recovery from total disability glare vision. App. Opt. 2022, 61, 2438–2443. [Google Scholar] [CrossRef]
- Gomez-Ulla, F.; Louro, O.; Mosquera, M. Macular dazzling test on normal subjects. Br. J. Ophthalmol. 1986, 70, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Swan, E.; Schwiegerling, J.; Peyman, G.; Enikov, E. Photostress testing device for diagnosing retinal disease. Photonics 2014, 1, 211–219. [Google Scholar] [CrossRef]
- Foster, D.H. Chromatic function of the cone. In Encyclopedia of the Eye; Elsevier Ltd.: Amsterdam, The Netherlands, 2010; pp. 266–274. [Google Scholar]
- Loughman, J.; Ratzlaff, M.; Foerg, B.; Connell, P. Suitability and repeatability of a photostress recovery test device, the macular degeneration detector (MDD-2), for diabetes and diabetic retinopathy assessment. Retina 2014, 34, 1006–1013. [Google Scholar] [CrossRef]
- Natsikos, V.E.; Hart, J.C. Photostress recovery times in case of central serous retinopathy. J. Royal. Soc. Med. 1980, 73, 793–797. [Google Scholar] [CrossRef] [PubMed]
- Charman, W.N.; Radhakrishnan, H. Accommodation, pupil diameter and myopia. Ophthalmic Physiol. Opt. 2009, 29, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Linke, S.J.; Baviera, J.; Munzer, G.; Fricke, O.H.; Richard, G.; Katz, T. Mesopic pupil size in a refractive surgery population (13,959 eyes). Optom. Vis. Sci. 2012, 89, 1156–1164. [Google Scholar] [CrossRef]
- Cakmak, H.B.; Cagil, N.; Simavli, H.; Duzen, B.; Simsek, S. Refractive error may influence mesopic pupil size. Curr. Eye Res. 2010, 35, 130–136. [Google Scholar] [CrossRef]
- Mathur, A.; Gehrmann, J.; Atchison, D.A. Influences of luminance and accommodation stimuli on pupil size and pupil center location. Investig. Ophthalmol. Vis. Sci. 2014, 55, 2166–2172. [Google Scholar] [CrossRef]
- Pan, C.-W.; Qiu, Q.-X.; Qian, D.-J.; Hu, D.-N.; Li, J.; Saw, S.-M.; Zhong, H. Iris colour in relation to myopia among Chinese school-aged children. Ophthalmic Physiol. Opt. 2018, 38, 48–55. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Glare Condition | Glare Angle (°) | Max Illuminance (Lux) |
|---|---|---|
| 1 | 3 | 1246 |
| 2 | 5 | 2277 |
| 3 | 7 | 3027 |
| 4 | 11 | 4281 |
| 5 | 14 | 4511 |
| Glare Angle (°) | Contrast | C = 0.05 | C = 0.10 | C = 0.25 | C = 0.50 | C = 1.00 |
|---|---|---|---|---|---|---|
| 3 | Myopia | 4.24 ± 1.72 | 3.41 ± 1.31 | 2.96 ± 1.08 | 2.69 ± 0.97 | 2.38 ± 1.02 |
| Control | 3.02 ± 1.23 | 2.49 ± 1.11 | 2.34 ± 0.92 | 2.19 ± 1.03 | 2.12 ± 0.97 | |
| p value | <0.001 ** | <0.001 ** | 0.003 ** | 0.009 ** | 0.163 | |
| 5 | Myopia | 4.05 ± 1.49 | 3.29 ± 1.11 | 2.87 ± 1.04 | 2.64 ± 0.98 | 2.33 ± 0.80 |
| Control | 2.68 ± 1.17 | 2.50 ± 1.00 | 2.22 ± 0.89 | 2.21 ± 0.72 | 2.01 ± 0.77 | |
| p value | <0.001 ** | 0.002 ** | 0.004 ** | 0.033 * | 0.032 * | |
| 7 | Myopia | 3.92 ± 1.25 | 3.25 ± 1.02 | 2.92 ± 0.93 | 2.58 ± 0.73 | 2.36 ± 0.80 |
| Control | 2.69 ± 1.06 | 2.65 ± 0.99 | 2.39 ± 1.03 | 2.32 ± 0.82 | 2.09 ± 0.74 | |
| p value | <0.001 ** | 0.006 ** | 0.011 * | 0.050 * | 0.032 * | |
| 11 | Myopia | 3.84 ± 1.34 | 3.20 ± 0.96 | 2.87 ± 0.73 | 2.54 ± 0.47 | 2.31 ± 0.47 |
| Control | 3.03 ± 1.19 | 2.59 ± 0.92 | 2.45 ± 0.89 | 2.20 ± 0.73 | 2.01 ± 0.66 | |
| p value | 0.002 ** | 0.002 ** | 0.006 ** | 0.006 ** | 0.006 ** | |
| 14 | Myopia | 3.76 ± 1.21 | 3.11 ± 0.77 | 2.82 ± 0.64 | 2.55 ± 0.54 | 2.22 ± 0.45 |
| Control | 2.65 ± 0.88 | 2.50 ± 0.85 | 2.42 ± 0.79 | 2.20 ± 0.68 | 1.99 ± 0.52 | |
| p value | <0.001 ** | 0.002 ** | 0.010 ** | 0.006 ** | 0.013 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ávila, F.J.; Casado, P.; Ares, J. Photostress Recovery Time after Flash-Lighting Is Increased in Myopic Eyes. Photonics 2023, 10, 86. https://doi.org/10.3390/photonics10010086
Ávila FJ, Casado P, Ares J. Photostress Recovery Time after Flash-Lighting Is Increased in Myopic Eyes. Photonics. 2023; 10(1):86. https://doi.org/10.3390/photonics10010086
Chicago/Turabian StyleÁvila, Francisco J., Pilar Casado, and Jorge Ares. 2023. "Photostress Recovery Time after Flash-Lighting Is Increased in Myopic Eyes" Photonics 10, no. 1: 86. https://doi.org/10.3390/photonics10010086
APA StyleÁvila, F. J., Casado, P., & Ares, J. (2023). Photostress Recovery Time after Flash-Lighting Is Increased in Myopic Eyes. Photonics, 10(1), 86. https://doi.org/10.3390/photonics10010086